- Published on
Emergency And Acute Medicine – Fibromyalgia
Basics Description
Fibromyalgia is a nonarticular, noninflammatory syndrome characterized by chronic, widespread musculoskeletal pain and heightened pain sensitivity to normally nonpainful stimuli (allodynia). It is more common in females and is associated with diffuse tenderness at multiple sites, fatigue, sleep disturbance, muscle stiffness, and cognitive difficulties involving attention and memory. Physical examination findings are often limited. Fibromyalgia is not a diagnosis of exclusion and may coexist with other rheumatologic or medical conditions.
Etiology
The underlying mechanism is believed to involve central pain processing abnormalities, with increased activity of pronociceptive pathways and reduced activity of antinociceptive pathways in the brain and spinal cord. Identified contributors include elevated substance P levels and decreased biogenic amines such as norepinephrine, serotonin, and dopamine. Reduced gray matter volume in certain brain regions has also been described. A genetic predisposition is suggested, with approximately one third of patients having an affected first-degree relative; candidate genes include those related to serotonin and dopamine pathways. Psychological factors are common, and many patients have comorbid psychiatric conditions. In susceptible individuals, fibromyalgia may be triggered by physical trauma, illness, inflammation, or chronic stress, with hypothalamic–pituitary–adrenal axis dysfunction often preceding symptom onset.
Diagnosis Signs And Symptoms
Patients report widespread pain involving both sides of the body, above and below the waist, and the axial skeleton, persisting for more than three months. Common associated symptoms include morning stiffness, generalized weakness, persistent fatigue not relieved by rest, sleep disturbance, muscle spasms, paresthesias, impaired concentration or memory, headaches, gastrointestinal discomfort relieved by bowel movements, pelvic or bladder discomfort, jaw or facial pain, and mood disturbances. Physical examination is typically unremarkable aside from tenderness at characteristic sites.
Essential Workup
History is the most important diagnostic tool. In the emergency department, evaluation is primarily focused on distinguishing chronic fibromyalgia pain from acute pain due to trauma, injury, or new medical conditions. If diagnostic confirmation is required, American College of Rheumatology criteria may be applied, including widespread pain for at least three months with either tender point assessment or use of the Widespread Pain Index (WPI) and Symptom Severity (SS) scale. Tender points are classically located at bilateral sites including the occiput, low cervical region, trapezius, supraspinatus, second rib, lateral epicondyle, gluteal region, greater trochanter, and medial knee fat pad.
Diagnosis Tests And Interpretation
Laboratory testing is not diagnostic and should be reserved for exclusion of alternative or acute conditions. Studies may include CBC, basic chemistries, ESR, muscle enzymes, thyroid function tests, and urinalysis when clinically indicated. Imaging and invasive procedures are not routinely useful and should only be performed to evaluate suspected alternative diagnoses.
Differential Diagnosis
Conditions to consider include myofascial pain syndrome, chronic fatigue syndrome, major depression, polymyalgia rheumatica, Lyme disease, hypothyroidism, collagen vascular diseases, electrolyte abnormalities, metabolic or drug-induced myopathies, osteomalacia, spondyloarthropathies, interstitial cystitis, and urinary tract infection.
Treatment
Emergency department management focuses on patient education, reassurance, and exclusion of acute pathology. Patients should be informed that fibromyalgia is chronic but not life-threatening, deforming, or associated with reduced life expectancy. Long-term management aims to reduce pain and improve function and requires outpatient follow-up. Pharmacologic therapy with central nervous system–acting agents is most effective, including gabapentin, pregabalin, tricyclic antidepressants, and serotonin–norepinephrine reuptake inhibitors. Opioids are not recommended and may worsen long-term pain. NSAIDs and corticosteroids have not demonstrated benefit. Local injections into tender points remain controversial due to lack of strong evidence.
Medication
Acetaminophen 650 mg PO q4h. Amitriptyline 25–50 mg PO at bedtime. Cyclobenzaprine 5–10 mg PO TID. Duloxetine 60 mg PO daily or BID. Gabapentin starting at 300 mg PO TID with gradual titration. Milnacipran starting at 12.5 mg daily and titrated to 50–100 mg PO BID. Pregabalin starting at 50 mg PO TID, titrated to a maximum of 450 mg/day. Tramadol may be used as an adjunct in selected patients.
Follow Up Disposition
Patients with uncomplicated fibromyalgia can be discharged with outpatient follow-up. Admission is reserved for those with serious underlying disease, intractable pain, immunocompromised status, or suicidal ideation.
Follow Up Recommendations
Patients should be referred to a primary care provider, rheumatologist, or pain specialist for ongoing management. Gradual aerobic exercise programs are encouraged, along with sleep hygiene measures such as regular sleep schedules and avoidance of caffeine in the evening. Stress management strategies and cognitive-behavioral therapy can provide sustained benefit.
Practical Takeaways And Frequent Missteps
Careful distinction between chronic fibromyalgia symptoms and new or acute pain is essential, as patients may still develop unrelated emergent conditions. Avoid unnecessary diagnostic testing once acute pathology has been excluded, and avoid opioid prescribing, which may worsen long-term outcomes.
Basics Description
Fibromyalgia is a nonarticular, noninflammatory syndrome characterized by chronic, widespread musculoskeletal pain and heightened pain sensitivity to normally nonpainful stimuli (allodynia). It is more common in females and is associated with diffuse tenderness at multiple sites, fatigue, sleep disturbance, muscle stiffness, and cognitive difficulties involving attention and memory. Physical examination findings are often limited. Fibromyalgia is not a diagnosis of exclusion and may coexist with other rheumatologic or medical conditions.
Etiology
The underlying mechanism is believed to involve central pain processing abnormalities, with increased activity of pronociceptive pathways and reduced activity of antinociceptive pathways in the brain and spinal cord. Identified contributors include elevated substance P levels and decreased biogenic amines such as norepinephrine, serotonin, and dopamine. Reduced gray matter volume in certain brain regions has also been described. A genetic predisposition is suggested, with approximately one third of patients having an affected first-degree relative; candidate genes include those related to serotonin and dopamine pathways. Psychological factors are common, and many patients have comorbid psychiatric conditions. In susceptible individuals, fibromyalgia may be triggered by physical trauma, illness, inflammation, or chronic stress, with hypothalamic–pituitary–adrenal axis dysfunction often preceding symptom onset.
Diagnosis Signs And Symptoms
Patients report widespread pain involving both sides of the body, above and below the waist, and the axial skeleton, persisting for more than three months. Common associated symptoms include morning stiffness, generalized weakness, persistent fatigue not relieved by rest, sleep disturbance, muscle spasms, paresthesias, impaired concentration or memory, headaches, gastrointestinal discomfort relieved by bowel movements, pelvic or bladder discomfort, jaw or facial pain, and mood disturbances. Physical examination is typically unremarkable aside from tenderness at characteristic sites.
Essential Workup
History is the most important diagnostic tool. In the emergency department, evaluation is primarily focused on distinguishing chronic fibromyalgia pain from acute pain due to trauma, injury, or new medical conditions. If diagnostic confirmation is required, American College of Rheumatology criteria may be applied, including widespread pain for at least three months with either tender point assessment or use of the Widespread Pain Index (WPI) and Symptom Severity (SS) scale. Tender points are classically located at bilateral sites including the occiput, low cervical region, trapezius, supraspinatus, second rib, lateral epicondyle, gluteal region, greater trochanter, and medial knee fat pad.
Diagnosis Tests And Interpretation
Laboratory testing is not diagnostic and should be reserved for exclusion of alternative or acute conditions. Studies may include CBC, basic chemistries, ESR, muscle enzymes, thyroid function tests, and urinalysis when clinically indicated. Imaging and invasive procedures are not routinely useful and should only be performed to evaluate suspected alternative diagnoses.
Differential Diagnosis
Conditions to consider include myofascial pain syndrome, chronic fatigue syndrome, major depression, polymyalgia rheumatica, Lyme disease, hypothyroidism, collagen vascular diseases, electrolyte abnormalities, metabolic or drug-induced myopathies, osteomalacia, spondyloarthropathies, interstitial cystitis, and urinary tract infection.
Treatment
Emergency department management focuses on patient education, reassurance, and exclusion of acute pathology. Patients should be informed that fibromyalgia is chronic but not life-threatening, deforming, or associated with reduced life expectancy. Long-term management aims to reduce pain and improve function and requires outpatient follow-up. Pharmacologic therapy with central nervous system–acting agents is most effective, including gabapentin, pregabalin, tricyclic antidepressants, and serotonin–norepinephrine reuptake inhibitors. Opioids are not recommended and may worsen long-term pain. NSAIDs and corticosteroids have not demonstrated benefit. Local injections into tender points remain controversial due to lack of strong evidence.
Medication
Acetaminophen 650 mg PO q4h. Amitriptyline 25–50 mg PO at bedtime. Cyclobenzaprine 5–10 mg PO TID. Duloxetine 60 mg PO daily or BID. Gabapentin starting at 300 mg PO TID with gradual titration. Milnacipran starting at 12.5 mg daily and titrated to 50–100 mg PO BID. Pregabalin starting at 50 mg PO TID, titrated to a maximum of 450 mg/day. Tramadol may be used as an adjunct in selected patients.
Follow Up Disposition
Patients with uncomplicated fibromyalgia can be discharged with outpatient follow-up. Admission is reserved for those with serious underlying disease, intractable pain, immunocompromised status, or suicidal ideation.
Follow Up Recommendations
Patients should be referred to a primary care provider, rheumatologist, or pain specialist for ongoing management. Gradual aerobic exercise programs are encouraged, along with sleep hygiene measures such as regular sleep schedules and avoidance of caffeine in the evening. Stress management strategies and cognitive-behavioral therapy can provide sustained benefit.
Practical Takeaways And Frequent Missteps
Careful distinction between chronic fibromyalgia symptoms and new or acute pain is essential, as patients may still develop unrelated emergent conditions. Avoid unnecessary diagnostic testing once acute pathology has been excluded, and avoid opioid prescribing, which may worsen long-term outcomes.

- Published on
Emergency And Acute Medicine – Pediatric Fever
Basics Description
Fever in children is defined as a rectal temperature of 38°C (100.4°F) or higher. Oral and tympanic temperatures are typically 0.6°C to 1°C lower than rectal measurements, and tympanic readings are unreliable in infants younger than six months. Axillary temperatures are generally inaccurate. Children who present afebrile but have a reliable history of documented fever should be considered febrile to the reported degree.
Etiology
Common causes of pediatric fever include bacteremia, viral illnesses often associated with exanthems, and localized infections. Vaccination against Haemophilus influenzae type B and Streptococcus pneumoniae has significantly reduced invasive disease caused by these organisms. Central nervous system causes include meningitis and encephalitis. Head and neck sources include otitis media, pharyngitis, cervical adenitis, sinusitis, mastoiditis, periorbital cellulitis, and deep neck space abscesses. Respiratory causes include croup, bronchiolitis, pneumonia, empyema, influenza, and epiglottitis. Additional etiologies include cardiac infections, urinary tract infections, gastrointestinal disease, osteomyelitis, septic arthritis, cellulitis, Kawasaki disease, neonatal herpes simplex virus infection, malignancy, drug reactions, heat-related illness, endocrine disorders, and inflammatory or autoimmune disease.
Diagnosis Signs And Symptoms
Clinical appearance is the most important factor in assessment. Airway, breathing, and circulation must be evaluated carefully, with special attention to hydration and perfusion. Toxic features include lethargy, poor feeding, delayed capillary refill, abnormal respirations, weak cry, hypotonia, and petechial or purpuric rash. Tachycardia and tachypnea may be the only early signs of serious illness. Fever increases heart rate by approximately ten beats per minute per degree Fahrenheit. Temperatures above 40°C are associated with increased bacteremia risk in children younger than twenty-four months, while temperatures above 42°C are more often noninfectious. Altered mental status may present as lethargy, irritability, or impaired interaction. Pneumonia should be suspected with tachypnea or hypoxia, and urinary tract infection should be considered in young females, uncircumcised males, and children with fever without a source. Febrile seizures may occur, and serious infection can be present even without fever. Antipyretics may improve clinical appearance without affecting underlying pathology, which can aid assessment. Approximately twenty percent of children will have fever without an identifiable source after initial evaluation.
Essential Workup
Oxygen saturation should be considered a mandatory vital sign. Resuscitation is initiated as needed. A focused history should include duration and pattern of fever, antipyretic use, immunization status, medical history, medications, birth history for infants younger than six months, exposures, feeding and elimination patterns, travel history, and review of systems. A thorough physical examination is performed to identify a source, and antipyretic therapy is initiated.
Diagnosis Tests And Interpretation
Laboratory evaluation may include a complete blood count with differential and urinalysis with culture in all male infants younger than six months, uncircumcised males younger than twelve months, and females younger than two years, using catheterized or suprapubic specimens. Blood cultures are obtained when bacteremia is suspected. Cerebrospinal fluid analysis is required for toxic children and neonates and considered selectively in older infants. Stool studies are indicated when bacterial diarrhea is suspected. Inflammatory markers such as C-reactive protein, erythrocyte sedimentation rate, and procalcitonin may provide supportive information. Chest radiography is indicated for tachypnea, hypoxia, or respiratory findings, with additional imaging guided by suspected source.
Treatment
Prehospital care focuses on stabilization and early antipyretic administration. Initial emergency department management prioritizes treatment of life-threatening conditions. Antipyretics are administered, while evaporative cooling has a limited role. Toxic-appearing children require immediate sepsis evaluation and empiric antibiotics. Neonates younger than twenty-eight days require full sepsis workup and admission with empiric antimicrobial therapy. Infants aged twenty-nine to ninety days are managed based on risk stratification, with selective laboratory evaluation, antibiotic use, and close follow-up. Children three months to three years of age are evaluated selectively, with focused testing based on clinical findings. Immunocompromised children, those with petechiae or purpura, sickle cell disease, malignancy, indwelling devices, or incomplete immunizations require aggressive evaluation and management.
Follow Up Disposition
Admission is required for toxic patients, neonates with fever, higher-risk infants who do not meet low-risk criteria, immunocompromised children, and those with unreliable follow-up. Discharge may be considered for well-appearing infants meeting low-risk criteria and older children who are nontoxic with reliable caregivers and follow-up. Clear return precautions and re-evaluation within twenty-four to forty-eight hours are essential.
Follow Up Recommendations
Children discharged with fever require close follow-up with a primary care provider and explicit instructions for return if symptoms worsen or new signs develop.
Key Clinical Insights And Common Errors
Fever is the most frequent presenting complaint in pediatric patients and may indicate life-threatening disease. Neonates require empiric treatment until serious infection is excluded. Older children may appear well despite significant illness, making subtle findings such as tachycardia, tachypnea, or altered mental status critically important. Inadequate follow-up and failure to recognize early signs of serious infection are common sources of error.

- Published on
Emergency And Acute Medicine – Adult Fever
Basics Description
Fever is an elevation of core body temperature caused by an increase in the hypothalamic thermoregulatory set point. Prostaglandin E2 synthesis within the anterior hypothalamus mediates this process and is the primary target of antipyretic therapy. Normal core temperature is regulated around 37°C with circadian variation, typically lowest in the early morning and highest in the late afternoon. Fever must be distinguished from hyperthermia, in which temperature elevation occurs despite a normal hypothalamic set point, and from hyperpyrexia, defined as extreme temperatures above 41.5°C, often associated with central nervous system injury. Endogenous pyrogens such as interleukins and tumor necrosis factor, as well as exogenous pyrogens including bacterial endotoxins, raise the thermoregulatory set point. Patients receiving anticytokine agents or glucocorticoids may exhibit a blunted febrile response. Fever of unknown origin is defined as a temperature above 38.3°C for more than three weeks without an established diagnosis after appropriate evaluation.
Etiology
Fever may result from infectious processes involving the central nervous system, respiratory tract, gastrointestinal tract, genitourinary system, skin, soft tissue, bone, vascular structures, or cardiac endocardium. Noninfectious causes include neoplastic disease, drug reactions, toxidromes, hypersensitivity reactions, systemic inflammatory and rheumatologic disorders, endocrine abnormalities such as hyperthyroidism or pheochromocytoma, withdrawal syndromes, and miscellaneous conditions including pulmonary embolism and hemolytic anemia. Common causes of fever of unknown origin include occult infections such as tuberculosis or abscesses, malignancies such as lymphoma or renal cell carcinoma, and inflammatory disorders.
Diagnosis Signs And Symptoms
Patients may report chills, rigors, weight loss, or night sweats, which can suggest bacteremia, malignancy, or chronic infection. Certain fever patterns provide diagnostic clues, including relapsing, remittent, intermittent, or double quotidian fevers. High-risk features include immunosuppression, anticytokine therapy, incomplete vaccination status, intravenous drug use, pregnancy, recent chemotherapy, recent travel, and splenectomy. Physical examination should focus on accurate core temperature measurement, assessment for diaphoresis, heart rate response relative to temperature, mental status changes, muscle rigidity or clonus, and skin findings such as rash or petechiae. Signs of endocrine disease, including goiter or exophthalmos, should also be assessed.
Essential Workup
Rectal temperature measurement provides the most accurate assessment of core temperature. A thorough history and physical examination guide the need for further diagnostic testing, including evaluation of recent infections, travel, medication use, occupational exposures, animal or tick contact, and immunization history.
Diagnosis Tests And Interpretation
Laboratory evaluation may include a complete blood count to assess for neutropenia, leukocytosis, or atypical lymphocytosis. Serum lactate is useful for identifying sepsis and guiding resuscitation. Urinalysis, urine culture, and blood cultures should be obtained in systemically ill patients or those at risk for bacteremia. Additional testing such as malaria smears, stool studies, heterophile antibody testing, or inflammatory markers may be indicated based on clinical context. Imaging studies such as chest radiography are useful in patients with respiratory findings or unclear fever sources, while advanced imaging is reserved for suspected deep or focal infections.
Treatment
Prehospital care focuses on monitoring and stabilization in unstable patients. Initial emergency department management prioritizes airway, breathing, and circulation in critically ill individuals. Early administration of broad-spectrum antibiotics is indicated in patients with suspected sepsis, neutropenia, or other high-risk features. Antipyretics such as acetaminophen or nonsteroidal anti-inflammatory drugs may be administered for comfort. Empiric antimicrobial therapy should be tailored to patient risk factors, including coverage for neutropenic, asplenic, or immunocompromised patients. External cooling measures are rarely required.
Follow Up Disposition
Patients with unstable vital signs or severe illness require hospital or intensive care admission. High-risk populations, including neutropenic, immunocompromised, asplenic, elderly, or intravenous drug–using patients, warrant a lower threshold for admission even in the absence of a clear source. Stable, immunocompetent patients with an identified benign source or suspected viral illness may be discharged with appropriate follow-up. Referral is guided by the suspected underlying etiology.
Key Clinical Insights And Common Errors
Early identification of sepsis using lactate screening and prompt initiation of broad-spectrum antibiotics are critical. Clinicians should maintain a broad differential diagnosis and carefully evaluate immunosuppressed, elderly, and high-risk patients, as fever may be the only manifestation of serious disease. Failure to recognize atypical presentations or delayed treatment in vulnerable populations can lead to significant morbidity and mortality.

- Published on
Emergency And Acute Medicine – Femur Fracture
Overview And Classification
Femoral fractures are classified by location, fracture geometry, degree of comminution, and soft tissue involvement. Fractures may involve the proximal third including the subtrochanteric region, the midshaft, or the distal metaphyseal–diaphyseal junction. Fracture geometry includes spiral, transverse, oblique, or segmental patterns and may be open or closed. Two commonly used classification systems are the AO/OTA system and the Winquist and Hansen classification, which categorizes fractures by the degree of comminution and stability. Grade I fractures involve minimal cortical loss and are lengthwise and rotationally stable, while Grade IV fractures demonstrate circumferential cortical loss and are unstable in all planes.
Etiology And Risk Factors
Femoral fractures typically result from high-energy trauma and are most commonly seen in young adults involved in motor vehicle collisions, gunshot wounds, or high-impact falls. Spiral fractures may occur with falls from height. Pathologic fractures should be considered when fractures occur after minor mechanisms, and stress fractures may result from repetitive activity. Complications include hemorrhage, compartment syndrome, fat embolism, and acute respiratory distress syndrome. In older adults, atypical femur fractures have been associated with bisphosphonate use. In children younger than three years, a significant proportion of femoral fractures result from nonaccidental trauma, and spiral fractures are particularly concerning.
Clinical Presentation
Patients typically present with severe thigh pain, deformity, swelling, shortening of the limb, and inability to move the hip or knee. Femur fractures frequently occur as part of multisystem trauma and may be associated with injuries to the chest, abdomen, pelvis, hip, or knee. Physical examination may reveal hypotension due to hemorrhage into the thigh, which can hold several units of blood. Distal neurovascular compromise or compartment syndrome may also be present.
Essential Evaluation
Initial evaluation includes radiographic imaging and careful assessment of distal pulses, sensation, motor function, and compartment firmness. Doppler evaluation or angiography may be required if pulses are diminished or asymmetric. Associated injuries should be sought in all patients with high-energy mechanisms. In children with suspected nonaccidental trauma, a skeletal survey or bone scan is indicated.
Diagnostic Studies And Interpretation
Laboratory studies include a complete blood count and type and cross-match due to the risk of significant blood loss. Imaging should include an anteroposterior pelvis, true lateral hip view, anteroposterior and lateral views of the femur, and a complete knee series. Chest radiography and additional imaging should follow trauma protocols as indicated.
Management And Initial Stabilization
Prehospital care includes immobilization of the extremity and use of a traction splint when appropriate to reduce pain and tamponade bleeding. Traction is contraindicated in fractures near the knee, ipsilateral hip fractures or dislocations, pelvic fractures, or lower leg fractures. Open fractures should not be reduced in the field and must be covered with sterile dressings. Patients require close monitoring for hemorrhagic shock.
Emergency Department Treatment
Airway, chest, and abdominal injuries take priority. Pain control should be provided with parenteral analgesia or femoral nerve block, particularly in pediatric or polytrauma patients. Orthopedic consultation is required for all femur fractures and is emergent when neurovascular compromise is present. Open fractures require immediate operative irrigation and debridement. Antibiotic therapy is indicated for open fractures, typically with cefazolin or clindamycin in patients with allergies, with additional coverage for extensive contamination. Skeletal traction should be applied if operative fixation is delayed. Vascular injury requires immediate angiography or surgical exploration.
Disposition And Follow Up
All femur fractures require hospital admission except in rare circumstances involving nonambulatory patients or pathologic fractures managed nonoperatively in consultation with orthopedics. Any suspicion of nonaccidental trauma mandates admission and further evaluation. Follow-up care is determined by the orthopedic surgeon based on fracture type and clinical course.
Key Clinical Insights And Common Errors
Femoral fractures result from high-energy trauma, and clinicians must maintain a high index of suspicion for associated life-threatening injuries. Neurovascular status should be carefully documented on arrival and reassessed frequently. In pediatric patients, femoral fractures do not always require operative management, but nonaccidental trauma must always be considered and evaluated appropriately.
Overview And Classification
Femoral fractures are classified by location, fracture geometry, degree of comminution, and soft tissue involvement. Fractures may involve the proximal third including the subtrochanteric region, the midshaft, or the distal metaphyseal–diaphyseal junction. Fracture geometry includes spiral, transverse, oblique, or segmental patterns and may be open or closed. Two commonly used classification systems are the AO/OTA system and the Winquist and Hansen classification, which categorizes fractures by the degree of comminution and stability. Grade I fractures involve minimal cortical loss and are lengthwise and rotationally stable, while Grade IV fractures demonstrate circumferential cortical loss and are unstable in all planes.
Etiology And Risk Factors
Femoral fractures typically result from high-energy trauma and are most commonly seen in young adults involved in motor vehicle collisions, gunshot wounds, or high-impact falls. Spiral fractures may occur with falls from height. Pathologic fractures should be considered when fractures occur after minor mechanisms, and stress fractures may result from repetitive activity. Complications include hemorrhage, compartment syndrome, fat embolism, and acute respiratory distress syndrome. In older adults, atypical femur fractures have been associated with bisphosphonate use. In children younger than three years, a significant proportion of femoral fractures result from nonaccidental trauma, and spiral fractures are particularly concerning.
Clinical Presentation
Patients typically present with severe thigh pain, deformity, swelling, shortening of the limb, and inability to move the hip or knee. Femur fractures frequently occur as part of multisystem trauma and may be associated with injuries to the chest, abdomen, pelvis, hip, or knee. Physical examination may reveal hypotension due to hemorrhage into the thigh, which can hold several units of blood. Distal neurovascular compromise or compartment syndrome may also be present.
Essential Evaluation
Initial evaluation includes radiographic imaging and careful assessment of distal pulses, sensation, motor function, and compartment firmness. Doppler evaluation or angiography may be required if pulses are diminished or asymmetric. Associated injuries should be sought in all patients with high-energy mechanisms. In children with suspected nonaccidental trauma, a skeletal survey or bone scan is indicated.
Diagnostic Studies And Interpretation
Laboratory studies include a complete blood count and type and cross-match due to the risk of significant blood loss. Imaging should include an anteroposterior pelvis, true lateral hip view, anteroposterior and lateral views of the femur, and a complete knee series. Chest radiography and additional imaging should follow trauma protocols as indicated.
Management And Initial Stabilization
Prehospital care includes immobilization of the extremity and use of a traction splint when appropriate to reduce pain and tamponade bleeding. Traction is contraindicated in fractures near the knee, ipsilateral hip fractures or dislocations, pelvic fractures, or lower leg fractures. Open fractures should not be reduced in the field and must be covered with sterile dressings. Patients require close monitoring for hemorrhagic shock.
Emergency Department Treatment
Airway, chest, and abdominal injuries take priority. Pain control should be provided with parenteral analgesia or femoral nerve block, particularly in pediatric or polytrauma patients. Orthopedic consultation is required for all femur fractures and is emergent when neurovascular compromise is present. Open fractures require immediate operative irrigation and debridement. Antibiotic therapy is indicated for open fractures, typically with cefazolin or clindamycin in patients with allergies, with additional coverage for extensive contamination. Skeletal traction should be applied if operative fixation is delayed. Vascular injury requires immediate angiography or surgical exploration.
Disposition And Follow Up
All femur fractures require hospital admission except in rare circumstances involving nonambulatory patients or pathologic fractures managed nonoperatively in consultation with orthopedics. Any suspicion of nonaccidental trauma mandates admission and further evaluation. Follow-up care is determined by the orthopedic surgeon based on fracture type and clinical course.
Key Clinical Insights And Common Errors
Femoral fractures result from high-energy trauma, and clinicians must maintain a high index of suspicion for associated life-threatening injuries. Neurovascular status should be carefully documented on arrival and reassessed frequently. In pediatric patients, femoral fractures do not always require operative management, but nonaccidental trauma must always be considered and evaluated appropriately.


- Published on
Emergency And Acute Medicine – Feeding Tube Complications
Overview And Definitions
Feeding tube complications include mechanical, infectious, gastrointestinal, and metabolic problems associated with nasoenteric tubes, percutaneous endoscopic gastrostomy (PEG) tubes, gastrostomy tubes, and jejunostomy tubes. Accidental or intentional extubation occurs more frequently with nasoenteric tubes. Occlusion is common with small-diameter tubes due to inadequate flushing, pill fragments, or incompatibility between medications and enteral formula. Proper assessment must exclude tube malposition, fracture, or dislodgement.
Etiology And Pathophysiology
Peristomal wound infections are associated with malnutrition, local irritation, poor wound care, stomal leakage, immunosuppression, diabetes mellitus, obesity, and excessive traction on the tube, which delays maturation of the gastrocutaneous tract. Stomal leakage may result from distal obstruction, dysmotility, high gastric residuals, or excessive tube movement. Aspiration pneumonia occurs in patients with impaired airway protective reflexes, delayed gastric emptying, bowel obstruction, gastroparesis, or gastroesophageal reflux, which is more common with large nasoenteric tubes. Diarrhea may result from antibiotics, promotility agents, infection with Clostridium difficile or other organisms, or high-osmolar formulas. Feeding intolerance is often due to rapid delivery, high-osmolar formulas, lactose or fat intolerance, low serum albumin, or gastrointestinal motility dysfunction. Rare but serious complications include abdominal wall hematoma, fistula formation, perforation, pressure ulcers, gastrointestinal bleeding, gastric outlet obstruction, buried bumper syndrome, and bowel volvulus around a PEG tube. Pediatric patients are at increased risk for aspiration due to immature lower esophageal sphincter function and delayed gastric emptying.
Clinical Presentation
Extubation presents with visible tube removal or absence from the expected position. Occlusion is suspected when liquids cannot be flushed through the tube. Tube migration may cause dumping syndrome, ischemia, intussusception, or distal obstruction. Peristomal infections present with cellulitis, abscess, or necrotizing soft tissue infection. Stomal leakage manifests as leakage of feeds or gastric contents around the stoma. Aspiration pneumonia presents with cough, dyspnea, hypoxia, fever, or food particles in pulmonary secretions. Misplacement of nasoenteric tubes into the pulmonary tree may cause pneumothorax, hydrothorax, pleural effusion, bronchopleural fistula, or pneumonia. Diarrhea presents with frequent loose stools and dehydration, while feeding intolerance is suggested by persistently high gastric residuals and increased aspiration risk.
Essential Evaluation
The tube site and external markings should be carefully inspected to assess position and integrity. Suspected tube migration requires confirmation with water-soluble contrast radiography to determine intraluminal position.
Diagnostic Studies And Interpretation
Laboratory evaluation for peristomal infection includes complete blood count and blood cultures in systemically ill patients. Aspiration pneumonia evaluation includes pulse oximetry or arterial blood gas analysis, complete blood count, electrolytes, renal function testing, glucose, and blood or sputum cultures. Diarrhea may require stool studies including white blood cells, culture, and C. difficile toxin testing. Serial complete blood counts are indicated for gastrointestinal bleeding. Imaging includes chest radiography to assess tube position and aspiration pneumonia, and contrast radiography for suspected migration. Endoscopy may be required to evaluate tube displacement.
Management And Initial Therapy
Initial management focuses on airway, breathing, and circulation, with intravenous fluid resuscitation for dehydration or sepsis. If a feeding tube has been accidentally removed, the tube should accompany the patient to facilitate replacement.
Emergency Department Treatment
Nasoenteric tubes may be replaced in the emergency department with radiographic confirmation prior to use. PEG and gastrojejunal tubes require 4–6 weeks for tract maturation. Tubes in place longer than four weeks may be replaced in the emergency department, often using a Foley catheter of equivalent size, with confirmation by water-soluble contrast imaging and secure external fixation. Tubes placed fewer than four weeks prior should not be replaced in the emergency department due to risk of intraperitoneal placement and peritonitis. Early dislodgement of surgical gastrostomy or jejunostomy tubes within the first three days requires emergent surgical consultation and antibiotic coverage. Occluded tubes may be managed with gentle irrigation using saline, water, carbonated beverages, or pancreatic enzymes; failed irrigation necessitates tube replacement. Tube migration may be managed by external repositioning if tolerated; persistent obstruction or peritonitis requires admission and specialty consultation. Peristomal infections are treated with local wound care and antibiotics, with surgical consultation for severe cases. Stomal leakage is managed by reducing infusion rate, optimizing nutrition, relieving tube tension, and using prokinetic agents; larger tubes should not be placed. Aspiration pneumonia requires cessation of feeds, oxygen therapy, antibiotics, and airway protection when indicated. Diarrhea management includes treating the underlying cause, correcting fluid and electrolyte abnormalities, adjusting formula composition, and using antimotility agents when appropriate.
Disposition And Follow Up
Admission is indicated for early tube dislodgement, significant peristomal infection, aspiration pneumonia, dehydration-related diarrhea, gastrointestinal bleeding, or peritonitis. Discharge may be considered after successful tube replacement and stabilization. Gastroenterology or surgical consultation is required when tube replacement cannot be safely performed in the emergency department. Ongoing follow-up with primary care or gastroenterology is recommended for recurrent complications.
Key Clinical Insights And Common Errors
Radiographic confirmation of feeding tube placement is essential before use. Newly placed PEG, gastrostomy, or jejunostomy tubes should not be replaced in the emergency department due to high risk of tract disruption and peritonitis. Failure to recognize tube migration, buried bumper syndrome, or aspiration risk can result in serious morbidity, particularly in pediatric patients.
Overview And Definitions
Feeding tube complications include mechanical, infectious, gastrointestinal, and metabolic problems associated with nasoenteric tubes, percutaneous endoscopic gastrostomy (PEG) tubes, gastrostomy tubes, and jejunostomy tubes. Accidental or intentional extubation occurs more frequently with nasoenteric tubes. Occlusion is common with small-diameter tubes due to inadequate flushing, pill fragments, or incompatibility between medications and enteral formula. Proper assessment must exclude tube malposition, fracture, or dislodgement.
Etiology And Pathophysiology
Peristomal wound infections are associated with malnutrition, local irritation, poor wound care, stomal leakage, immunosuppression, diabetes mellitus, obesity, and excessive traction on the tube, which delays maturation of the gastrocutaneous tract. Stomal leakage may result from distal obstruction, dysmotility, high gastric residuals, or excessive tube movement. Aspiration pneumonia occurs in patients with impaired airway protective reflexes, delayed gastric emptying, bowel obstruction, gastroparesis, or gastroesophageal reflux, which is more common with large nasoenteric tubes. Diarrhea may result from antibiotics, promotility agents, infection with Clostridium difficile or other organisms, or high-osmolar formulas. Feeding intolerance is often due to rapid delivery, high-osmolar formulas, lactose or fat intolerance, low serum albumin, or gastrointestinal motility dysfunction. Rare but serious complications include abdominal wall hematoma, fistula formation, perforation, pressure ulcers, gastrointestinal bleeding, gastric outlet obstruction, buried bumper syndrome, and bowel volvulus around a PEG tube. Pediatric patients are at increased risk for aspiration due to immature lower esophageal sphincter function and delayed gastric emptying.
Clinical Presentation
Extubation presents with visible tube removal or absence from the expected position. Occlusion is suspected when liquids cannot be flushed through the tube. Tube migration may cause dumping syndrome, ischemia, intussusception, or distal obstruction. Peristomal infections present with cellulitis, abscess, or necrotizing soft tissue infection. Stomal leakage manifests as leakage of feeds or gastric contents around the stoma. Aspiration pneumonia presents with cough, dyspnea, hypoxia, fever, or food particles in pulmonary secretions. Misplacement of nasoenteric tubes into the pulmonary tree may cause pneumothorax, hydrothorax, pleural effusion, bronchopleural fistula, or pneumonia. Diarrhea presents with frequent loose stools and dehydration, while feeding intolerance is suggested by persistently high gastric residuals and increased aspiration risk.
Essential Evaluation
The tube site and external markings should be carefully inspected to assess position and integrity. Suspected tube migration requires confirmation with water-soluble contrast radiography to determine intraluminal position.
Diagnostic Studies And Interpretation
Laboratory evaluation for peristomal infection includes complete blood count and blood cultures in systemically ill patients. Aspiration pneumonia evaluation includes pulse oximetry or arterial blood gas analysis, complete blood count, electrolytes, renal function testing, glucose, and blood or sputum cultures. Diarrhea may require stool studies including white blood cells, culture, and C. difficile toxin testing. Serial complete blood counts are indicated for gastrointestinal bleeding. Imaging includes chest radiography to assess tube position and aspiration pneumonia, and contrast radiography for suspected migration. Endoscopy may be required to evaluate tube displacement.
Management And Initial Therapy
Initial management focuses on airway, breathing, and circulation, with intravenous fluid resuscitation for dehydration or sepsis. If a feeding tube has been accidentally removed, the tube should accompany the patient to facilitate replacement.
Emergency Department Treatment
Nasoenteric tubes may be replaced in the emergency department with radiographic confirmation prior to use. PEG and gastrojejunal tubes require 4–6 weeks for tract maturation. Tubes in place longer than four weeks may be replaced in the emergency department, often using a Foley catheter of equivalent size, with confirmation by water-soluble contrast imaging and secure external fixation. Tubes placed fewer than four weeks prior should not be replaced in the emergency department due to risk of intraperitoneal placement and peritonitis. Early dislodgement of surgical gastrostomy or jejunostomy tubes within the first three days requires emergent surgical consultation and antibiotic coverage. Occluded tubes may be managed with gentle irrigation using saline, water, carbonated beverages, or pancreatic enzymes; failed irrigation necessitates tube replacement. Tube migration may be managed by external repositioning if tolerated; persistent obstruction or peritonitis requires admission and specialty consultation. Peristomal infections are treated with local wound care and antibiotics, with surgical consultation for severe cases. Stomal leakage is managed by reducing infusion rate, optimizing nutrition, relieving tube tension, and using prokinetic agents; larger tubes should not be placed. Aspiration pneumonia requires cessation of feeds, oxygen therapy, antibiotics, and airway protection when indicated. Diarrhea management includes treating the underlying cause, correcting fluid and electrolyte abnormalities, adjusting formula composition, and using antimotility agents when appropriate.
Disposition And Follow Up
Admission is indicated for early tube dislodgement, significant peristomal infection, aspiration pneumonia, dehydration-related diarrhea, gastrointestinal bleeding, or peritonitis. Discharge may be considered after successful tube replacement and stabilization. Gastroenterology or surgical consultation is required when tube replacement cannot be safely performed in the emergency department. Ongoing follow-up with primary care or gastroenterology is recommended for recurrent complications.
Key Clinical Insights And Common Errors
Radiographic confirmation of feeding tube placement is essential before use. Newly placed PEG, gastrostomy, or jejunostomy tubes should not be replaced in the emergency department due to high risk of tract disruption and peritonitis. Failure to recognize tube migration, buried bumper syndrome, or aspiration risk can result in serious morbidity, particularly in pediatric patients.
- Published on
Emergency And Acute Medicine – Feeding Problems, Pediatric
Overview And Definitions
Feeding problems may involve one or more components of feeding, including oral intake initiation, swallowing, or gastrointestinal ingestion and absorption. Acute feeding difficulties may reflect systemic illness such as infection or bowel obstruction, whereas chronic feeding problems often result from neuromuscular, cardiovascular, behavioral, or social factors. Minor feeding difficulties occur in up to half of otherwise healthy children, while more severe feeding disorders are common in premature infants and children with chronic medical conditions.
Etiology And Pathophysiology
Feeding problems often arise from overlapping etiologies. Structural abnormalities may involve the naso-oropharynx, larynx, trachea, or esophagus, including cleft lip or palate, choanal atresia, micrognathia, macroglossia, tonsillar hypertrophy, laryngeal clefts, tracheomalacia, esophageal strictures, webs, vascular rings, masses, or foreign bodies. Neurologic conditions include cerebral palsy, neuromuscular disorders, mitochondrial disease, Arnold–Chiari malformation, myasthenia gravis, brainstem injury, autism spectrum disorder, infant botulism, and prematurity. Immune-mediated disorders include food allergy, eosinophilic esophagitis, and celiac disease. Cardiac disease may cause feeding intolerance due to fatigue or increased metabolic demand, both before and after corrective surgery. Metabolic disorders such as hypothyroidism and inborn errors of metabolism may impair feeding. Acute illnesses including sepsis, pharyngitis, intussusception, malrotation, or abusive head trauma may present with feeding refusal. Behavioral and environmental factors include dysfunctional caregiver–child interaction, selective eating, rumination, feeding-related anxiety, neglect, depression, and poverty.
Clinical Presentation
Common presentations include caregiver concern regarding feeding behavior, poor weight gain or failure to thrive, and recurrent or chronic respiratory illness. Aspiration is frequently silent in infants and may present as recurrent pneumonia or wheezing.
History And Physical Examination
History should address onset and duration of feeding problems, meal length, food refusal or oral aversion, independent feeding ability, vomiting or gagging, diarrhea or rectal bleeding, respiratory symptoms, irritability or lethargy during feeds, and feeding frequency and volume appropriate for age. Feeding times consistently longer than 30 minutes are concerning. Physical examination includes vital signs and pulse oximetry, growth measurements plotted on standardized growth curves, and assessment of nutritional status. Severe cases may show emaciation, weakness, or apathy. Examination should focus on affect and social responsiveness, dysmorphic features, ENT abnormalities, cardiovascular and pulmonary status, abdominal findings, neurologic tone and coordination, and skin signs of malnutrition or allergy. Direct observation of feeding is essential, assessing oral motor function, pacing, airway sounds, gagging, coughing, emesis, respiratory distress, fatigue, irritability, and feeding duration.
Essential Evaluation
A well-appearing, hydrated child with normal examination findings and adequate recent weight gain may not require emergency department testing beyond ensuring appropriate follow-up. Children with distress, dehydration, respiratory compromise, or poor growth require further evaluation.
Diagnostic Studies And Interpretation
Initial laboratory evaluation in children with failure to thrive or malnutrition may include complete blood count, urinalysis, electrolytes, BUN, glucose, ESR or CRP, thyroid function tests, liver function tests, total protein, and albumin. Blood, urine, and cerebrospinal fluid cultures are indicated if infection is suspected. Metabolic testing may include serum ammonia and urine organic acids. Imaging may include chest radiograph for cardiopulmonary disease, ECG for suspected cardiac pathology, and ultrasound or advanced imaging as indicated. Videofluoroscopic or fiberoptic swallowing studies may be required. MRI is indicated when brainstem or spinal pathology is suspected. Multidisciplinary evaluation involving speech therapy, pediatrics, and otolaryngology is often necessary.
Differential Diagnosis
Feeding disorders represent a final common pathway for numerous conditions. Prolonged feeding with fatigue suggests cardiac disease. Recurrent pneumonias suggest chronic aspiration. Stridor during feeds raises concern for airway anomalies. Poor suck–swallow–breathing coordination suggests nasal obstruction or choanal atresia. Vomiting, diarrhea, abdominal pain, or colic may indicate allergy or gastroesophageal reflux.
Management And Initial Therapy
Initial management includes assessment of airway, breathing, circulation, hydration status, and glucose. Cardiopulmonary and fluid resuscitation are provided as needed. Hypoglycemia should be promptly identified and treated. Certain inborn errors of metabolism may cause severe hypoglycemia with feeding interruption and require immediate intravenous dextrose. Bilious vomiting in infants raises concern for malrotation with volvulus and mandates emergent surgical consultation.
Emergency Department Treatment
Dehydration should be treated with oral rehydration when feasible or intravenous fluids when oral intake is not tolerated. Ondansetron may be used for acute vomiting in appropriate patients. Respiratory distress should be addressed, including nasal suctioning prior to feeding in young infants with upper respiratory symptoms. Oxygen and additional respiratory support should be provided as needed. Infection should be treated promptly, recognizing that severely malnourished children may have blunted physiologic responses to sepsis.
Disposition And Follow Up
Admission is indicated for suspected systemic infection, inability to maintain hydration, sustained hypoxia during feeding, significant failure to thrive—particularly in infants younger than three months—decompensated cardiopulmonary disease, symptomatic anemia or endocrine dysfunction, or concerns regarding caregiver capacity. Discharge may be considered when the child demonstrates adequate oral intake, weight stability or gain, reliable caregiving, and assured follow-up. Referral should be tailored to the underlying etiology, with multidisciplinary care often required for complex or chronic feeding disorders. Nonoral nutritional support may be necessary when oral feeding is insufficient.
Key Clinical Insights And Common Errors
Effective feeding requires coordinated interaction among physiologic, developmental, and environmental factors, and disruption of one component often affects others. Acute-onset feeding problems are more likely to have a single identifiable cause such as infection or obstruction, whereas chronic feeding difficulties are often multifactorial. Simple interventions such as aggressive nasal suctioning before feeding may resolve symptoms in infants with upper respiratory congestion. Swallowing disorders and aspiration are frequently occult. Feeding difficulties may persist behaviorally even after correction of the underlying medical condition, particularly when early negative feeding experiences have occurred.
- Published on
Emergency And Acute Medicine – Fatigue
Overview And Definitions
Fatigue is a subjective sensation of overwhelming, persistent exhaustion with reduced capacity for physical and mental activity that is not relieved by rest. It may occur with or without objective abnormalities on physical examination. Fatigue is a frequent complaint among patients both with and without systemic disease, making evaluation challenging in emergency practice.
Etiology And Pathophysiology
The precise mechanisms underlying fatigue are not fully understood. Common contributing categories include hematologic disorders such as anemia and leukemia; endocrine conditions including thyroid disease, adrenal insufficiency, diabetes, and pregnancy; malignancy with paraneoplastic syndromes; psychiatric illness including depression, emotional distress, eating disorders, substance use, and withdrawal; sleep disorders such as insomnia and sleep apnea; cardiac and pulmonary disease; acute and chronic infections; rheumatologic and autoimmune disorders; nutritional deficiencies and electrolyte abnormalities; physical deconditioning; medication effects; and chronic fatigue syndrome. Chronic fatigue syndrome is defined by severe fatigue lasting longer than six months, not explained by medical or psychiatric disease, accompanied by four or more symptoms including headache, arthralgias, sleep disturbance, lymphadenopathy, postexertional malaise, myalgias, impaired concentration or memory, and sore throat.
Clinical Presentation
Fatigue is characterized by persistent tiredness or exhaustion that interferes with daily activities and does not resolve with sleep. While no physical findings are specific, associated signs may suggest an underlying etiology.
History And Physical Examination
History should focus on onset, duration, and progression of fatigue, associated symptoms such as fever, night sweats, dyspnea, weakness, weight changes, and sleep patterns, as well as past medical, surgical, psychiatric, and social history including substance use and recent stressors. Medication review and a full review of systems are essential. Physical examination should be comprehensive and directed toward identifying an underlying cause. Vital signs may reveal infection or metabolic disturbance. HEENT exam may show icterus, pallor, or pupillary abnormalities. Thyroid enlargement or tenderness may suggest dysfunction. Cardiac murmurs or S3 gallop raise concern for heart failure. Pulmonary findings may indicate acute or chronic lung disease. Abdominal masses or tenderness warrant further investigation. Skin findings such as rash, dehydration, or hyperpigmentation may indicate systemic disease. Neurologic examination should assess for focal deficits or true weakness. Musculoskeletal and vascular access sites should be inspected for infection or electrolyte-related complications.
Essential Evaluation
Because fatigue is subjective, evaluation is guided by clinical suspicion based on history and examination, with the goal of identifying reversible or serious underlying conditions.
Diagnostic Studies And Interpretation
Laboratory testing should be selective and include complete blood count to screen for anemia or malignancy, serum glucose to identify hypo- or hyperglycemia, pregnancy testing when appropriate, electrolytes with renal function, thyroid-stimulating hormone to evaluate for hypothyroidism, and urine drug screening when substance use is suspected. Imaging and specialized testing are reserved for abnormalities identified during initial evaluation.
Differential Diagnosis
The differential diagnosis includes infectious etiologies such as bacteremia, pneumonia, viral syndromes, EBV, CMV, HIV, and HHV-6; immunologic and connective tissue diseases; neoplastic disorders; metabolic abnormalities; hematologic disease; endocrine dysfunction; neurologic disorders; cardiovascular disease; pulmonary pathology; gastrointestinal and hepatic disease; autonomic dysfunction; lifestyle-related factors; psychiatric illness; medication effects; and dehydration.
Management And Initial Therapy
Initial management includes assessment of airway, breathing, and circulation, supplemental oxygen for hypoxia, and intravenous fluids for dehydration. Emergency department treatment is directed at identifying and correcting the underlying cause, including treatment of infection, correction of metabolic or hematologic abnormalities, recognition of neurologic or psychiatric emergencies, discontinuation of offending medications, and initiation of appropriate referrals. In many cases no definitive cause is identified, and reassurance with close outpatient follow-up is appropriate. Patients should be counseled on sleep hygiene, nutrition, physical activity, and routine care.
Disposition And Follow Up
Admission is indicated for patients with serious underlying disease requiring inpatient treatment, inability to care for themselves, or failure to thrive as an outpatient. Discharge is appropriate when serious conditions have been excluded, the patient is stable, and reliable follow-up is arranged. Referral should be made to appropriate specialists when an etiology is identified, or to primary care when evaluation is incomplete or ongoing.
Key Clinical Insights And Common Errors
Fatigue is a symptom rather than a diagnosis and requires careful history and physical examination. Absence of abnormal findings does not exclude serious disease. Elderly patients, children, intoxicated individuals, and those with impaired communication may present with fatigue as the only sign of life-threatening illness. Failure to recognize high-risk features or unreliable histories is a common cause of missed diagnoses.
Overview And Definitions
Fatigue is a subjective sensation of overwhelming, persistent exhaustion with reduced capacity for physical and mental activity that is not relieved by rest. It may occur with or without objective abnormalities on physical examination. Fatigue is a frequent complaint among patients both with and without systemic disease, making evaluation challenging in emergency practice.
Etiology And Pathophysiology
The precise mechanisms underlying fatigue are not fully understood. Common contributing categories include hematologic disorders such as anemia and leukemia; endocrine conditions including thyroid disease, adrenal insufficiency, diabetes, and pregnancy; malignancy with paraneoplastic syndromes; psychiatric illness including depression, emotional distress, eating disorders, substance use, and withdrawal; sleep disorders such as insomnia and sleep apnea; cardiac and pulmonary disease; acute and chronic infections; rheumatologic and autoimmune disorders; nutritional deficiencies and electrolyte abnormalities; physical deconditioning; medication effects; and chronic fatigue syndrome. Chronic fatigue syndrome is defined by severe fatigue lasting longer than six months, not explained by medical or psychiatric disease, accompanied by four or more symptoms including headache, arthralgias, sleep disturbance, lymphadenopathy, postexertional malaise, myalgias, impaired concentration or memory, and sore throat.
Clinical Presentation
Fatigue is characterized by persistent tiredness or exhaustion that interferes with daily activities and does not resolve with sleep. While no physical findings are specific, associated signs may suggest an underlying etiology.
History And Physical Examination
History should focus on onset, duration, and progression of fatigue, associated symptoms such as fever, night sweats, dyspnea, weakness, weight changes, and sleep patterns, as well as past medical, surgical, psychiatric, and social history including substance use and recent stressors. Medication review and a full review of systems are essential. Physical examination should be comprehensive and directed toward identifying an underlying cause. Vital signs may reveal infection or metabolic disturbance. HEENT exam may show icterus, pallor, or pupillary abnormalities. Thyroid enlargement or tenderness may suggest dysfunction. Cardiac murmurs or S3 gallop raise concern for heart failure. Pulmonary findings may indicate acute or chronic lung disease. Abdominal masses or tenderness warrant further investigation. Skin findings such as rash, dehydration, or hyperpigmentation may indicate systemic disease. Neurologic examination should assess for focal deficits or true weakness. Musculoskeletal and vascular access sites should be inspected for infection or electrolyte-related complications.
Essential Evaluation
Because fatigue is subjective, evaluation is guided by clinical suspicion based on history and examination, with the goal of identifying reversible or serious underlying conditions.
Diagnostic Studies And Interpretation
Laboratory testing should be selective and include complete blood count to screen for anemia or malignancy, serum glucose to identify hypo- or hyperglycemia, pregnancy testing when appropriate, electrolytes with renal function, thyroid-stimulating hormone to evaluate for hypothyroidism, and urine drug screening when substance use is suspected. Imaging and specialized testing are reserved for abnormalities identified during initial evaluation.
Differential Diagnosis
The differential diagnosis includes infectious etiologies such as bacteremia, pneumonia, viral syndromes, EBV, CMV, HIV, and HHV-6; immunologic and connective tissue diseases; neoplastic disorders; metabolic abnormalities; hematologic disease; endocrine dysfunction; neurologic disorders; cardiovascular disease; pulmonary pathology; gastrointestinal and hepatic disease; autonomic dysfunction; lifestyle-related factors; psychiatric illness; medication effects; and dehydration.
Management And Initial Therapy
Initial management includes assessment of airway, breathing, and circulation, supplemental oxygen for hypoxia, and intravenous fluids for dehydration. Emergency department treatment is directed at identifying and correcting the underlying cause, including treatment of infection, correction of metabolic or hematologic abnormalities, recognition of neurologic or psychiatric emergencies, discontinuation of offending medications, and initiation of appropriate referrals. In many cases no definitive cause is identified, and reassurance with close outpatient follow-up is appropriate. Patients should be counseled on sleep hygiene, nutrition, physical activity, and routine care.
Disposition And Follow Up
Admission is indicated for patients with serious underlying disease requiring inpatient treatment, inability to care for themselves, or failure to thrive as an outpatient. Discharge is appropriate when serious conditions have been excluded, the patient is stable, and reliable follow-up is arranged. Referral should be made to appropriate specialists when an etiology is identified, or to primary care when evaluation is incomplete or ongoing.
Key Clinical Insights And Common Errors
Fatigue is a symptom rather than a diagnosis and requires careful history and physical examination. Absence of abnormal findings does not exclude serious disease. Elderly patients, children, intoxicated individuals, and those with impaired communication may present with fatigue as the only sign of life-threatening illness. Failure to recognize high-risk features or unreliable histories is a common cause of missed diagnoses.

- Published on
Emergency And Acute Medicine – Failure To Thrive
Overview And Definitions
Failure to thrive (FTT) is not a single diagnosis but a descriptive term encompassing a spectrum of conditions characterized by inadequate physical growth, most often identified before two years of age. It is broadly categorized into organic causes, in which an underlying medical condition is present, and nonorganic causes, where no identifiable medical etiology exists. Although FTT occurs across all socioeconomic groups, poverty significantly increases risk. Early-life FTT, particularly in the first few months, may lead to long-term growth impairment as well as behavioral and developmental consequences.
Etiology And Pathophysiology
Failure to thrive results from one or more fundamental mechanisms including insufficient caloric intake, impaired caloric absorption or malabsorption, or excessive caloric expenditure. These mechanisms are frequently secondary to chronic medical conditions but may also arise from psychosocial or environmental factors.
Clinical Presentation
There is no universally accepted definition of failure to thrive. Common criteria include weight below two standard deviations for age and sex, adjusted for prematurity, or a downward crossing of two major percentile lines on standardized growth charts. A change in growth velocity affecting one or more parameters is typical. Weight is usually affected first, followed by length or height, and finally head circumference in cases of prolonged caloric deficiency. Isolated linear growth failure often suggests endocrine disease, while impaired head circumference growth points toward a primary neurologic condition. Physical manifestations may include muscle wasting, loss of subcutaneous fat, alopecia, dermatitis, chronic illness states such as marasmus or kwashiorkor, endocrinologic abnormalities, developmental delay, and increased susceptibility to infection.
History And Physical Examination
A detailed feeding history is essential, including breast-feeding practices, formula type and preparation, feeding frequency, volume, and introduction of solids. Associated vomiting, urine and stool output, and blood in stool should be assessed. Prenatal and birth history should include maternal illness, substance exposure, gestational age, birth weight, and congenital anomalies. Developmental progress, temperament, and psychosocial context including family support, stressors, maternal depression, and possible abuse or neglect must be evaluated. Physical examination requires accurate measurement and plotting of weight, length or height, and head circumference on appropriate growth charts, ideally with multiple prior data points. Examination should assess for dysmorphic features, signs of cardiac, pulmonary, gastrointestinal, or neurologic disease, and indicators of maltreatment.
Essential Evaluation
Evaluation centers on a thorough history and physical examination, accurate growth chart analysis, direct observation of feeding, and assessment of caregiver–child interaction. Initial laboratory testing may include complete blood count, inflammatory markers, electrolytes, urinalysis and culture, and lead level when indicated.
Diagnostic Studies And Interpretation
Laboratory evaluation may reveal anemia, infection, malignancy, metabolic derangements, renal disease, endocrine disorders, or lead toxicity. Review of newborn screening results is often informative. Additional testing may include blood gas analysis, HIV testing, stool studies, imaging such as chest radiography, bone age assessment, and targeted diagnostic procedures including pH probe studies, sweat chloride testing, or tuberculin skin testing based on clinical suspicion.
Differential Diagnosis
Organic causes include gastrointestinal disorders such as malabsorption, celiac disease, cystic fibrosis, inflammatory bowel disease, anatomic obstruction, gastroesophageal reflux, and nutritional deficiencies; cardiac disease; chronic pulmonary disease; hematologic or oncologic conditions; renal disease; neurologic disorders; immunodeficiency; endocrine abnormalities; infectious etiologies; genetic syndromes; and toxic exposures. Nonorganic causes include feeding technique errors, inadequate food availability, psychosocial stressors, caregiver mental illness or substance use, parent–child interaction disorders, neglect, and fabricated illness by proxy.
Management And Initial Therapy
Initial management includes assessment for hypoglycemia and dehydration with prompt correction when present. A supportive, nonjudgmental approach is essential. Emergency department care focuses on identifying FTT, excluding urgent organic pathology, engaging social services when appropriate, and providing feeding support including lactation consultation.
Disposition And Follow Up
Hospital admission is indicated for children with significant organic disease, severe malnutrition, dehydration, electrolyte imbalance, suspected abuse or neglect, or when observation of feeding and caregiver interaction is required. Infants younger than three to six months warrant a lower threshold for admission due to neurodevelopmental vulnerability. Discharge is appropriate when close outpatient follow-up is assured and growth monitoring can be reliably maintained. Referral to appropriate subspecialists should be arranged based on the suspected etiology.
Key Clinical Insights And Common Errors
Failure to thrive is a descriptive finding rather than a diagnosis and often reflects an underlying medical or psychosocial issue. Weight loss typically precedes declines in length and head circumference. Normal laboratory results do not exclude serious nonorganic causes. Abrupt changes in growth trajectory should raise concern for organic disease. Early recognition and intervention are critical to prevent long-term developmental sequelae, and clinicians must remain vigilant for neglect or abuse while maintaining a supportive and unbiased approach.
Overview And Definitions
Failure to thrive (FTT) is not a single diagnosis but a descriptive term encompassing a spectrum of conditions characterized by inadequate physical growth, most often identified before two years of age. It is broadly categorized into organic causes, in which an underlying medical condition is present, and nonorganic causes, where no identifiable medical etiology exists. Although FTT occurs across all socioeconomic groups, poverty significantly increases risk. Early-life FTT, particularly in the first few months, may lead to long-term growth impairment as well as behavioral and developmental consequences.
Etiology And Pathophysiology
Failure to thrive results from one or more fundamental mechanisms including insufficient caloric intake, impaired caloric absorption or malabsorption, or excessive caloric expenditure. These mechanisms are frequently secondary to chronic medical conditions but may also arise from psychosocial or environmental factors.
Clinical Presentation
There is no universally accepted definition of failure to thrive. Common criteria include weight below two standard deviations for age and sex, adjusted for prematurity, or a downward crossing of two major percentile lines on standardized growth charts. A change in growth velocity affecting one or more parameters is typical. Weight is usually affected first, followed by length or height, and finally head circumference in cases of prolonged caloric deficiency. Isolated linear growth failure often suggests endocrine disease, while impaired head circumference growth points toward a primary neurologic condition. Physical manifestations may include muscle wasting, loss of subcutaneous fat, alopecia, dermatitis, chronic illness states such as marasmus or kwashiorkor, endocrinologic abnormalities, developmental delay, and increased susceptibility to infection.
History And Physical Examination
A detailed feeding history is essential, including breast-feeding practices, formula type and preparation, feeding frequency, volume, and introduction of solids. Associated vomiting, urine and stool output, and blood in stool should be assessed. Prenatal and birth history should include maternal illness, substance exposure, gestational age, birth weight, and congenital anomalies. Developmental progress, temperament, and psychosocial context including family support, stressors, maternal depression, and possible abuse or neglect must be evaluated. Physical examination requires accurate measurement and plotting of weight, length or height, and head circumference on appropriate growth charts, ideally with multiple prior data points. Examination should assess for dysmorphic features, signs of cardiac, pulmonary, gastrointestinal, or neurologic disease, and indicators of maltreatment.
Essential Evaluation
Evaluation centers on a thorough history and physical examination, accurate growth chart analysis, direct observation of feeding, and assessment of caregiver–child interaction. Initial laboratory testing may include complete blood count, inflammatory markers, electrolytes, urinalysis and culture, and lead level when indicated.
Diagnostic Studies And Interpretation
Laboratory evaluation may reveal anemia, infection, malignancy, metabolic derangements, renal disease, endocrine disorders, or lead toxicity. Review of newborn screening results is often informative. Additional testing may include blood gas analysis, HIV testing, stool studies, imaging such as chest radiography, bone age assessment, and targeted diagnostic procedures including pH probe studies, sweat chloride testing, or tuberculin skin testing based on clinical suspicion.
Differential Diagnosis
Organic causes include gastrointestinal disorders such as malabsorption, celiac disease, cystic fibrosis, inflammatory bowel disease, anatomic obstruction, gastroesophageal reflux, and nutritional deficiencies; cardiac disease; chronic pulmonary disease; hematologic or oncologic conditions; renal disease; neurologic disorders; immunodeficiency; endocrine abnormalities; infectious etiologies; genetic syndromes; and toxic exposures. Nonorganic causes include feeding technique errors, inadequate food availability, psychosocial stressors, caregiver mental illness or substance use, parent–child interaction disorders, neglect, and fabricated illness by proxy.
Management And Initial Therapy
Initial management includes assessment for hypoglycemia and dehydration with prompt correction when present. A supportive, nonjudgmental approach is essential. Emergency department care focuses on identifying FTT, excluding urgent organic pathology, engaging social services when appropriate, and providing feeding support including lactation consultation.
Disposition And Follow Up
Hospital admission is indicated for children with significant organic disease, severe malnutrition, dehydration, electrolyte imbalance, suspected abuse or neglect, or when observation of feeding and caregiver interaction is required. Infants younger than three to six months warrant a lower threshold for admission due to neurodevelopmental vulnerability. Discharge is appropriate when close outpatient follow-up is assured and growth monitoring can be reliably maintained. Referral to appropriate subspecialists should be arranged based on the suspected etiology.
Key Clinical Insights And Common Errors
Failure to thrive is a descriptive finding rather than a diagnosis and often reflects an underlying medical or psychosocial issue. Weight loss typically precedes declines in length and head circumference. Normal laboratory results do not exclude serious nonorganic causes. Abrupt changes in growth trajectory should raise concern for organic disease. Early recognition and intervention are critical to prevent long-term developmental sequelae, and clinicians must remain vigilant for neglect or abuse while maintaining a supportive and unbiased approach.

- Published on
Emergency And Acute Medicine – Facial Fractures
Overview And Definitions
Facial fractures result from blunt trauma most commonly caused by motor vehicle collisions, assaults, or falls. These injuries frequently involve multiple facial bones and are often associated with damage to adjacent structures including the eyes, teeth, mandible, cervical spine, and brain. Open fractures are common, and facial trauma may be the initial indicator of more severe systemic injury. In women and children, clinicians should maintain a high index of suspicion for physical assault or domestic violence.
Etiology And Mechanisms Of Injury
Facial fractures are categorized based on the anatomic structures involved. Le Fort fractures represent classic maxillary fracture patterns. Le Fort I fractures involve a horizontal separation of the maxilla above the teeth. Le Fort II fractures are pyramidal in shape, extending through the nasal bridge, maxilla, and infraorbital rims. Le Fort III fractures result in craniofacial disjunction with complete separation of the midface from the cranial base. Some patients may sustain asymmetric or mixed Le Fort patterns.
Other common fractures include zygomatic arch fractures, which may involve the orbit and maxilla, frontal sinus fractures that may be complicated by cerebrospinal fluid leaks, and orbital fractures, particularly blow-out fractures of the orbital floor that are frequently associated with ocular injury.
Special Populations
In older adults, facial fractures most commonly result from falls, with the zygoma being the most frequently fractured bone. These patients are at increased risk for concomitant cervical spine and intracranial injuries. In children, facial fractures are uncommon before the age of six; when present, nonaccidental trauma must be considered. Pediatric facial fractures are often associated with severe head injury, and orbital fractures are the most common non-nasal facial fracture in this population.
Clinical Presentation
Patients typically present with facial pain, swelling, ecchymosis, deformity, epistaxis, facial numbness, and malocclusion. Cerebrospinal fluid rhinorrhea, raccoon eyes, and facial anesthesia may indicate more severe injury. A septal hematoma appears as a bluish, fluctuant swelling of the nasal septum and represents a true emergency due to the risk of cartilage necrosis.
Physical Examination
Initial assessment must prioritize airway patency. A thorough facial examination includes palpation for tenderness, step-offs, crepitus, and deformity. Evaluation of dental occlusion, nasal inspection for septal hematoma or cerebrospinal fluid leak, and detailed sensory testing of the face are essential. A comprehensive eye examination including visual acuity, pupillary response, extraocular movements, and funduscopic evaluation is mandatory. Le Fort fractures can be assessed by stabilizing the nasal bridge while gently mobilizing the maxilla to detect midface instability.
Diagnostic Evaluation
After airway stabilization, radiologic evaluation is required for all suspected facial fractures. Computed tomography of the facial bones with multiplanar reconstruction is the imaging modality of choice and allows detailed assessment of fracture patterns and associated injuries. Plain radiographs are generally insufficient and should not be relied upon when CT imaging is available.
Differential Diagnosis
Conditions that may mimic or coexist with facial fractures include nasal fractures, isolated zygomatic fractures, mandibular fractures, frontal sinus injuries, skull base fractures, orbital soft tissue injuries, and facial contusions or lacerations without underlying bony injury.
Management Principles
Airway control takes precedence in all patients with facial trauma. Rapid-sequence intubation is preferred when airway protection is required, while nasotracheal intubation is contraindicated in most facial fractures. Surgical airway access may be necessary if standard intubation fails. Cervical spine immobilization must be maintained until injury is excluded.
Antibiotics are indicated for open fractures and cerebrospinal fluid leaks, and tetanus prophylaxis should be updated. Septal hematomas must be drained promptly in the emergency department. Pain control is achieved with parenteral analgesics. Consultation with otolaryngology, plastic surgery, oral surgery, or neurosurgery is required depending on fracture complexity.
Disposition And Follow Up
Patients with airway compromise, significant associated trauma, Le Fort II or III fractures, cerebrospinal fluid leaks, posterior table frontal sinus fractures, or most open fractures require admission. Stable patients with closed, nondisplaced fractures and no associated injuries may be discharged with close specialist follow-up within 24 to 36 hours. Septal hematomas require re-evaluation within 24 hours after drainage.
Clinical Pearls And Pitfalls
Facial fractures may appear dramatic but should never distract from airway management and evaluation for life-threatening injuries. Nasotracheal intubation should be avoided. Ocular injuries are common and must be actively sought. Always examine for a septal hematoma. Missing teeth must be accounted for, and aspiration should be excluded with chest imaging when indicated.
Overview And Definitions
Facial fractures result from blunt trauma most commonly caused by motor vehicle collisions, assaults, or falls. These injuries frequently involve multiple facial bones and are often associated with damage to adjacent structures including the eyes, teeth, mandible, cervical spine, and brain. Open fractures are common, and facial trauma may be the initial indicator of more severe systemic injury. In women and children, clinicians should maintain a high index of suspicion for physical assault or domestic violence.
Etiology And Mechanisms Of Injury
Facial fractures are categorized based on the anatomic structures involved. Le Fort fractures represent classic maxillary fracture patterns. Le Fort I fractures involve a horizontal separation of the maxilla above the teeth. Le Fort II fractures are pyramidal in shape, extending through the nasal bridge, maxilla, and infraorbital rims. Le Fort III fractures result in craniofacial disjunction with complete separation of the midface from the cranial base. Some patients may sustain asymmetric or mixed Le Fort patterns.
Other common fractures include zygomatic arch fractures, which may involve the orbit and maxilla, frontal sinus fractures that may be complicated by cerebrospinal fluid leaks, and orbital fractures, particularly blow-out fractures of the orbital floor that are frequently associated with ocular injury.
Special Populations
In older adults, facial fractures most commonly result from falls, with the zygoma being the most frequently fractured bone. These patients are at increased risk for concomitant cervical spine and intracranial injuries. In children, facial fractures are uncommon before the age of six; when present, nonaccidental trauma must be considered. Pediatric facial fractures are often associated with severe head injury, and orbital fractures are the most common non-nasal facial fracture in this population.
Clinical Presentation
Patients typically present with facial pain, swelling, ecchymosis, deformity, epistaxis, facial numbness, and malocclusion. Cerebrospinal fluid rhinorrhea, raccoon eyes, and facial anesthesia may indicate more severe injury. A septal hematoma appears as a bluish, fluctuant swelling of the nasal septum and represents a true emergency due to the risk of cartilage necrosis.
Physical Examination
Initial assessment must prioritize airway patency. A thorough facial examination includes palpation for tenderness, step-offs, crepitus, and deformity. Evaluation of dental occlusion, nasal inspection for septal hematoma or cerebrospinal fluid leak, and detailed sensory testing of the face are essential. A comprehensive eye examination including visual acuity, pupillary response, extraocular movements, and funduscopic evaluation is mandatory. Le Fort fractures can be assessed by stabilizing the nasal bridge while gently mobilizing the maxilla to detect midface instability.
Diagnostic Evaluation
After airway stabilization, radiologic evaluation is required for all suspected facial fractures. Computed tomography of the facial bones with multiplanar reconstruction is the imaging modality of choice and allows detailed assessment of fracture patterns and associated injuries. Plain radiographs are generally insufficient and should not be relied upon when CT imaging is available.
Differential Diagnosis
Conditions that may mimic or coexist with facial fractures include nasal fractures, isolated zygomatic fractures, mandibular fractures, frontal sinus injuries, skull base fractures, orbital soft tissue injuries, and facial contusions or lacerations without underlying bony injury.
Management Principles
Airway control takes precedence in all patients with facial trauma. Rapid-sequence intubation is preferred when airway protection is required, while nasotracheal intubation is contraindicated in most facial fractures. Surgical airway access may be necessary if standard intubation fails. Cervical spine immobilization must be maintained until injury is excluded.
Antibiotics are indicated for open fractures and cerebrospinal fluid leaks, and tetanus prophylaxis should be updated. Septal hematomas must be drained promptly in the emergency department. Pain control is achieved with parenteral analgesics. Consultation with otolaryngology, plastic surgery, oral surgery, or neurosurgery is required depending on fracture complexity.
Disposition And Follow Up
Patients with airway compromise, significant associated trauma, Le Fort II or III fractures, cerebrospinal fluid leaks, posterior table frontal sinus fractures, or most open fractures require admission. Stable patients with closed, nondisplaced fractures and no associated injuries may be discharged with close specialist follow-up within 24 to 36 hours. Septal hematomas require re-evaluation within 24 hours after drainage.
Clinical Pearls And Pitfalls
Facial fractures may appear dramatic but should never distract from airway management and evaluation for life-threatening injuries. Nasotracheal intubation should be avoided. Ocular injuries are common and must be actively sought. Always examine for a septal hematoma. Missing teeth must be accounted for, and aspiration should be excluded with chest imaging when indicated.
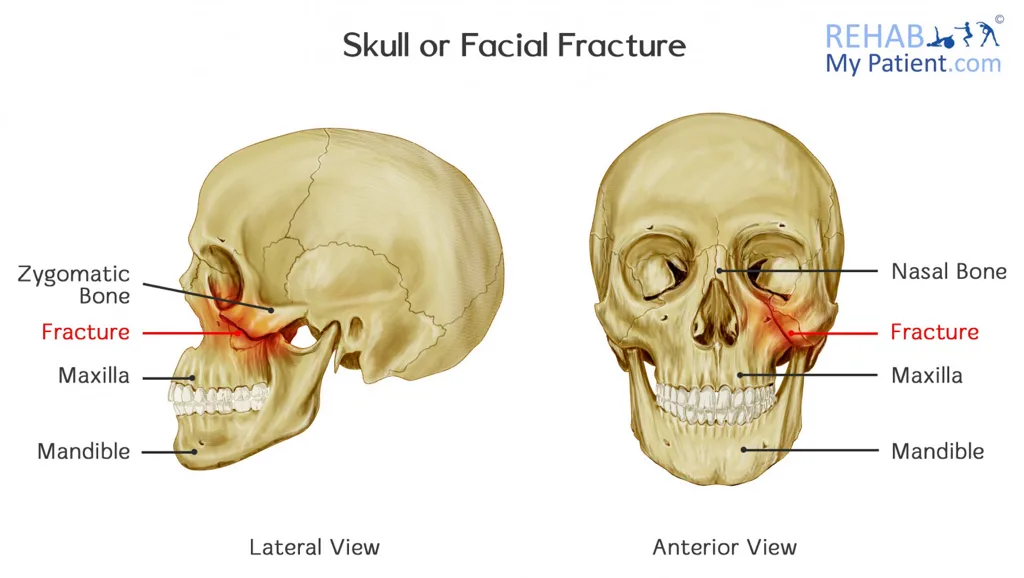
- Published on
Emergency And Acute Medicine - Extremity Trauma, Penetrating
Condition overview
Penetrating extremity trauma refers to injuries in which an object breaches the skin and underlying tissues of an arm or leg. These injuries range from minor puncture wounds to severe limb-threatening trauma involving vascular, neurologic, musculoskeletal, or compartment compromise.
Mechanisms of injury
Common mechanisms include stab or puncture wounds, gunshot wounds, lacerations, animal or human bites, and high-pressure injection injuries. High-muzzle-velocity gunshot wounds are particularly destructive, as the shock wave may cause extensive tissue damage beyond the visible wound tract, often with more damage at the exit wound than the entry site.
Clinical presentation
Findings may include entry and exit wounds, lacerations, or punctures. Vascular injury should be suspected with decreased or absent distal pulses, ischemic changes, expanding hematoma, or a bruit or thrill over the injury; the presence of a distal pulse does not exclude proximal vascular damage. Neurologic injury may present with paresthesias, weakness, or loss of sensation distal to the wound. Musculoskeletal injury may manifest as deformity, joint effusion, ligamentous laxity, or limited range of motion. Compartment syndrome is suggested by severe, constant pain, pain with passive stretch, compartment tenderness, weakness, and sensory deficits, with pallor and pulselessness being late findings.
History and examination priorities
Key historical elements include the mechanism and timing of injury, circumstances such as assault or self-harm, and comorbid conditions including diabetes, immunosuppression, peripheral vascular disease, valvular heart disease, or asplenia. Examination should document wound location, size, depth, and shape, and assess for exit wounds. Distal pulses should be compared bilaterally by palpation and Doppler. Capillary refill, motor and sensory function, joint stability, and signs of compartment syndrome must be evaluated. The wound should be carefully inspected for foreign bodies.
Diagnostic evaluation
The physical examination guides further testing. Acute wound cultures are not routinely indicated. Plain radiographs with at least anteroposterior and lateral views are used to detect fractures or radiopaque foreign bodies. Ultrasound, fluoroscopy, or CT may help identify radiolucent foreign bodies. When vascular injury is suspected and immediate surgery is not required, arteriography may be indicated.
Management principles
Prehospital care focuses on hemorrhage control with direct pressure, limb elevation, pain control, neurovascular assessment, and stabilization of impaled objects in place. In the emergency department, airway and hemodynamic stabilization take priority. The wound should be fully exposed, constricting items removed, and bleeding controlled with direct pressure; blind clamping and prolonged tourniquet use are discouraged. After a full neurologic exam, pain control is provided. Visible debris and devitalized tissue are removed, with copious high-pressure saline irrigation as the cornerstone of wound care. Tetanus prophylaxis is essential.
Stab and gunshot wounds should receive a single dose of cefazolin in the emergency department. Extremities should be immobilized when vascular injury, fracture, tendon injury, or joint violation is suspected. Loss of distal pulse or signs of ischemia mandate emergent surgical consultation without delay for imaging. Clean lacerations seen within 6–8 hours may be closed primarily; puncture wounds and gunshot wounds should not be closed primarily, with delayed primary closure considered for contaminated or older wounds.
Special considerations
Plantar puncture wounds require careful inspection and removal of foreign material; aggressive probing or irrigation may worsen contamination. Prophylactic antibiotics are generally not recommended unless the patient is diabetic, immunocompromised, or the wound is highly contaminated or delayed in presentation. High-pressure injection injuries of the hand require immediate orthopedic evaluation, as surface wounds may underestimate deep tissue involvement. Small inert foreign bodies, including bullets, may be left in place if not near vital structures, whereas organic material should always be removed.
Disposition and follow-up
Admission and emergent surgical consultation are required for suspected vascular injury, compartment syndrome, joint penetration, high-velocity gunshot wounds, or contaminated wounds in high-risk patients. Stable patients without indications for surgery may be discharged after appropriate wound care with instructions for elevation, wound hygiene, and close follow-up within 24–48 hours.
Key clinical lessons
A normal distal pulse does not exclude significant vascular injury. High-pressure hand injuries and plantar puncture wounds are commonly underestimated. Failure of a puncture wound infection to improve with antibiotics should prompt concern for a retained foreign body.
Condition overview
Penetrating extremity trauma refers to injuries in which an object breaches the skin and underlying tissues of an arm or leg. These injuries range from minor puncture wounds to severe limb-threatening trauma involving vascular, neurologic, musculoskeletal, or compartment compromise.
Mechanisms of injury
Common mechanisms include stab or puncture wounds, gunshot wounds, lacerations, animal or human bites, and high-pressure injection injuries. High-muzzle-velocity gunshot wounds are particularly destructive, as the shock wave may cause extensive tissue damage beyond the visible wound tract, often with more damage at the exit wound than the entry site.
Clinical presentation
Findings may include entry and exit wounds, lacerations, or punctures. Vascular injury should be suspected with decreased or absent distal pulses, ischemic changes, expanding hematoma, or a bruit or thrill over the injury; the presence of a distal pulse does not exclude proximal vascular damage. Neurologic injury may present with paresthesias, weakness, or loss of sensation distal to the wound. Musculoskeletal injury may manifest as deformity, joint effusion, ligamentous laxity, or limited range of motion. Compartment syndrome is suggested by severe, constant pain, pain with passive stretch, compartment tenderness, weakness, and sensory deficits, with pallor and pulselessness being late findings.
History and examination priorities
Key historical elements include the mechanism and timing of injury, circumstances such as assault or self-harm, and comorbid conditions including diabetes, immunosuppression, peripheral vascular disease, valvular heart disease, or asplenia. Examination should document wound location, size, depth, and shape, and assess for exit wounds. Distal pulses should be compared bilaterally by palpation and Doppler. Capillary refill, motor and sensory function, joint stability, and signs of compartment syndrome must be evaluated. The wound should be carefully inspected for foreign bodies.
Diagnostic evaluation
The physical examination guides further testing. Acute wound cultures are not routinely indicated. Plain radiographs with at least anteroposterior and lateral views are used to detect fractures or radiopaque foreign bodies. Ultrasound, fluoroscopy, or CT may help identify radiolucent foreign bodies. When vascular injury is suspected and immediate surgery is not required, arteriography may be indicated.
Management principles
Prehospital care focuses on hemorrhage control with direct pressure, limb elevation, pain control, neurovascular assessment, and stabilization of impaled objects in place. In the emergency department, airway and hemodynamic stabilization take priority. The wound should be fully exposed, constricting items removed, and bleeding controlled with direct pressure; blind clamping and prolonged tourniquet use are discouraged. After a full neurologic exam, pain control is provided. Visible debris and devitalized tissue are removed, with copious high-pressure saline irrigation as the cornerstone of wound care. Tetanus prophylaxis is essential.
Stab and gunshot wounds should receive a single dose of cefazolin in the emergency department. Extremities should be immobilized when vascular injury, fracture, tendon injury, or joint violation is suspected. Loss of distal pulse or signs of ischemia mandate emergent surgical consultation without delay for imaging. Clean lacerations seen within 6–8 hours may be closed primarily; puncture wounds and gunshot wounds should not be closed primarily, with delayed primary closure considered for contaminated or older wounds.
Special considerations
Plantar puncture wounds require careful inspection and removal of foreign material; aggressive probing or irrigation may worsen contamination. Prophylactic antibiotics are generally not recommended unless the patient is diabetic, immunocompromised, or the wound is highly contaminated or delayed in presentation. High-pressure injection injuries of the hand require immediate orthopedic evaluation, as surface wounds may underestimate deep tissue involvement. Small inert foreign bodies, including bullets, may be left in place if not near vital structures, whereas organic material should always be removed.
Disposition and follow-up
Admission and emergent surgical consultation are required for suspected vascular injury, compartment syndrome, joint penetration, high-velocity gunshot wounds, or contaminated wounds in high-risk patients. Stable patients without indications for surgery may be discharged after appropriate wound care with instructions for elevation, wound hygiene, and close follow-up within 24–48 hours.
Key clinical lessons
A normal distal pulse does not exclude significant vascular injury. High-pressure hand injuries and plantar puncture wounds are commonly underestimated. Failure of a puncture wound infection to improve with antibiotics should prompt concern for a retained foreign body.