- Published on
Emergency And Acute Medicine - External Ear Chondritis And Abscess
Condition overview
This condition involves inflammation and/or infection of the auricular cartilage of the pinna. Because the cartilage of the external ear has minimal subcutaneous tissue, limited blood supply, and is exposed, it is particularly vulnerable to injury and infection. Chondritis often develops as a delayed complication after trauma or burns, sometimes appearing after the ear seems to have healed. Inadequate or delayed treatment can lead to cartilage avascular necrosis and permanent deformity of the pinna, ranging from a cauliflower-like ear to near-total loss of the external ear with possible narrowing of the auditory canal.
Underlying causes
Damage to the auricular cartilage may result from chemical or thermal burns, frostbite, auricular hematomas, blunt or penetrating trauma, human or insect bites, deep abrasions, otitis externa, and high ear piercings—especially when performed with poor technique, hygiene, or aftercare. Common causative organisms include Pseudomonas aeruginosa, Staphylococcus species, and Proteus species.
Clinical presentation
Symptoms often begin with a dull ache that progressively worsens. Fever and chills may occur in more advanced cases. Patients frequently report a history of ear trauma or recent ear piercing. On examination, the pinna is painful with marked tenderness, erythema, and warmth. Swelling leads to loss of normal auricular contours, typically sparing the lobule. The auriculocephalic angle may increase. As infection progresses, fluctuance can develop, followed by skin breakdown and purulent drainage.
Diagnostic approach
The diagnosis is primarily clinical, based on characteristic physical findings and a compatible history. Laboratory testing is reserved for patients with systemic signs of infection and may include a complete blood count and blood cultures. When drainage is performed for abscess or advanced chondritis, local cultures should be obtained to guide antibiotic therapy.
Conditions to consider
Important alternatives include allergic reactions, mastoiditis, dermatitis, and auricular hematoma.
Management principles
Early prevention and treatment are critical to avoid permanent deformity. Pressure to the injured ear should be avoided. Eschars and crusts should not be aggressively debrided. The ear should be gently cleansed twice daily with antibacterial soap and water, thoroughly dried, and treated with topical antibiotics if the skin barrier is disrupted. Hair should be kept away from the affected ear. Mild, early infections limited to the lobule may be treated with oral antibiotics. Established chondritis or abscess formation requires parenteral antibiotics and prompt surgical drainage.
Pharmacologic therapy
Antibiotic regimens must include coverage for Pseudomonas. Oral options for mild cases include ciprofloxacin, cephalexin, or dicloxacillin, adjusted for age and weight in pediatric patients. Severe infections require intravenous antibiotics. Topical antibiotics are indicated when there is a break in the skin.
Disposition and follow-up
Admission is indicated for patients with significant edema, erythema, marked tenderness, systemic toxicity, fever, chills, or immunocompromise. Stable patients without systemic signs may be discharged with close otolaryngology follow-up. ENT consultation is recommended for all cases of chondritis, abscess, or cartilage necrosis, and early surgical drainage is essential when abscess is present.
Key clinical lessons
Prompt and aggressive early management is essential to prevent severe and permanent ear deformity. Antibiotic therapy should always include reliable antipseudomonal coverage.
Condition overview
This condition involves inflammation and/or infection of the auricular cartilage of the pinna. Because the cartilage of the external ear has minimal subcutaneous tissue, limited blood supply, and is exposed, it is particularly vulnerable to injury and infection. Chondritis often develops as a delayed complication after trauma or burns, sometimes appearing after the ear seems to have healed. Inadequate or delayed treatment can lead to cartilage avascular necrosis and permanent deformity of the pinna, ranging from a cauliflower-like ear to near-total loss of the external ear with possible narrowing of the auditory canal.
Underlying causes
Damage to the auricular cartilage may result from chemical or thermal burns, frostbite, auricular hematomas, blunt or penetrating trauma, human or insect bites, deep abrasions, otitis externa, and high ear piercings—especially when performed with poor technique, hygiene, or aftercare. Common causative organisms include Pseudomonas aeruginosa, Staphylococcus species, and Proteus species.
Clinical presentation
Symptoms often begin with a dull ache that progressively worsens. Fever and chills may occur in more advanced cases. Patients frequently report a history of ear trauma or recent ear piercing. On examination, the pinna is painful with marked tenderness, erythema, and warmth. Swelling leads to loss of normal auricular contours, typically sparing the lobule. The auriculocephalic angle may increase. As infection progresses, fluctuance can develop, followed by skin breakdown and purulent drainage.
Diagnostic approach
The diagnosis is primarily clinical, based on characteristic physical findings and a compatible history. Laboratory testing is reserved for patients with systemic signs of infection and may include a complete blood count and blood cultures. When drainage is performed for abscess or advanced chondritis, local cultures should be obtained to guide antibiotic therapy.
Conditions to consider
Important alternatives include allergic reactions, mastoiditis, dermatitis, and auricular hematoma.
Management principles
Early prevention and treatment are critical to avoid permanent deformity. Pressure to the injured ear should be avoided. Eschars and crusts should not be aggressively debrided. The ear should be gently cleansed twice daily with antibacterial soap and water, thoroughly dried, and treated with topical antibiotics if the skin barrier is disrupted. Hair should be kept away from the affected ear. Mild, early infections limited to the lobule may be treated with oral antibiotics. Established chondritis or abscess formation requires parenteral antibiotics and prompt surgical drainage.
Pharmacologic therapy
Antibiotic regimens must include coverage for Pseudomonas. Oral options for mild cases include ciprofloxacin, cephalexin, or dicloxacillin, adjusted for age and weight in pediatric patients. Severe infections require intravenous antibiotics. Topical antibiotics are indicated when there is a break in the skin.
Disposition and follow-up
Admission is indicated for patients with significant edema, erythema, marked tenderness, systemic toxicity, fever, chills, or immunocompromise. Stable patients without systemic signs may be discharged with close otolaryngology follow-up. ENT consultation is recommended for all cases of chondritis, abscess, or cartilage necrosis, and early surgical drainage is essential when abscess is present.
Key clinical lessons
Prompt and aggressive early management is essential to prevent severe and permanent ear deformity. Antibiotic therapy should always include reliable antipseudomonal coverage.


- Published on
Emergency And Acute Medicine - Ethylene glycol poisoning
Basic description
Peak serum concentration occurs in 1–4 hr. The half-life is 2.5–4.5 hr, and less than 20% is excreted unchanged by the kidneys.
Ethylene glycol is metabolized by hepatic alcohol dehydrogenase and aldehyde dehydrogenase to acidic metabolites that ultimately form oxalic acid. Aldehyde and acid metabolites are directly toxic to the CNS, heart, and kidneys.
Etiology
Exposure is typically from ethylene-glycol–containing products such as antifreeze and certain solvents. The minimum reported lethal dose is approximately 30 mL of 100% ethylene glycol.
Diagnosis – signs and symptoms
Cardiovascular: tachycardia, bradycardia, dysrhythmias, hypertension, hypotension.
Cns: inebriation, irritability, ataxia, obtundation, coma, cerebral edema, seizures; may also have peripheral nervous system findings including cranial nerve abnormalities.
Gi: nausea, vomiting, abdominal pain.
Pulmonary: tachypnea, hyperventilation, Kussmaul respirations, pulmonary edema.
Renal: crystalluria and acute renal failure.
Three overlapping stages may be seen:
History
Intentional or unintentional ingestion may be reported. Consider this diagnosis even without a clear history when there is an unexplained high anion gap metabolic acidosis and/or an elevated, unexplained osmol gap.
Physical examination
Tachypnea and altered mental status are common.
Essential workup
Obtain a complete ingestion history. Draw the following simultaneously:
Diagnosis tests and interpretation
Calculate the anion gap: (Na⁺) − (Cl⁻ + HCO₃⁻); normal is approximately 8–12.
Calculate the osmol gap: measured osmolality − calculated osmolarity; an increased gap is generally >10.
Calculated osmolarity: 2(Na⁺) + glucose/18 + BUN/2.8 + ethanol (mg/dL)/4.6.
The osmol gap is most useful early after ingestion (and may be larger with concurrent ethanol ingestion, with less severe acidosis). A normal osmol gap does not exclude ethylene glycol poisoning, especially with late presentation when metabolites drive an anion gap acidosis.
Urinalysis may show envelope-shaped calcium oxalate crystals (specific but insensitive). Absence of crystals does not rule out exposure.
Wood lamp inspection of urine or gastric contents may show fluorescein from antifreeze, but this is insensitive and nonspecific.
Differential diagnosis
Elevated osmol gap: methanol, ethanol, isopropyl alcohol, mannitol/glycerin/propylene glycol/sorbitol, acetone/ammonia, propylene glycol.
Elevated anion gap metabolic acidosis: alcoholic ketoacidosis, toxic asphyxiants (e.g., cyanide/CO/H₂S), acetaminophen-related causes, antiretrovirals (NRTIs), toluene, metformin, uremia, DKA, iron/INH, lactic acidosis, salicylates, starvation ketosis, methanol, ethylene glycol.
Treatment
Prehospital care
Bring containers of suspected substances. Monitor airway and mental status. For dermal exposure, remove contaminated clothing/jewelry and irrigate with soap and water.
Initial stabilization and therapy
ABCs. Provide supplemental oxygen, cardiac monitoring, and IV access with 0.9% saline. For altered mental status, check glucose and consider dextrose, naloxone, and thiamine as appropriate.
Emergency department treatment and procedures
Pregnancy considerations
Fomepizole is class C in pregnancy. Ethanol is not recommended.
Pediatric considerations
Ethanol can cause significant CNS depression and hypoglycemia in children.
Medication
Activated charcoal: 1 g/kg PO.
Dextrose: D50W 25 g IV (peds: D25W 2–4 mL/kg).
Ethanol: oral (via NG) or IV 10% ethanol in D5W per dosing protocols; adjust during hemodialysis.
Fomepizole: 15 mg/kg IV load over 30 min, then 10 mg/kg q12h ×4 doses, then 15 mg/kg q12h until level <25 mg />L; dose adjustments required during hemodialysis.
Magnesium: 25–50 mg/kg IV once (max 2 g).
Naloxone: 2 mg IV/IM (peds: 0.1 mg/kg).
Pyridoxine: 100 mg daily for 2 days.
Sodium bicarbonate: 1–2 mEq/kg IV in D5W.
Thiamine: 100 mg daily for 2 days (peds: 50 mg).
Follow-up and disposition
Admission criteria
Admit all patients with significant suspected or confirmed ethylene glycol ingestion, even if initially asymptomatic. ICU admission is indicated for serious illness, metabolic acidosis, or renal failure. Transfer if fomepizole or hemodialysis is indicated but not available.
Discharge criteria
An asymptomatic patient with isolated exposure may be discharged only if ethylene glycol concentration is undetectable and there is no metabolic acidosis.
Follow-up recommendations
Psychiatric evaluation is indicated after intentional ingestion.
Clinical pearls and common pitfalls
An osmol gap <10 does not exclude ethylene glycol poisoning. treat early with fomepizole when the diagnosis is on table and confirm serum levels available. presentations may show only an osmol gap, while late anion gap. do use absence of urinary crystals or lack fluorescence under a wood lamp to rule out exposure. if confirmation, antidote availability, 24 /> hemodialysis capability is uncertain, transfer to a facility that has all of these resources.
Basic description
Peak serum concentration occurs in 1–4 hr. The half-life is 2.5–4.5 hr, and less than 20% is excreted unchanged by the kidneys.
Ethylene glycol is metabolized by hepatic alcohol dehydrogenase and aldehyde dehydrogenase to acidic metabolites that ultimately form oxalic acid. Aldehyde and acid metabolites are directly toxic to the CNS, heart, and kidneys.
Etiology
Exposure is typically from ethylene-glycol–containing products such as antifreeze and certain solvents. The minimum reported lethal dose is approximately 30 mL of 100% ethylene glycol.
Diagnosis – signs and symptoms
Cardiovascular: tachycardia, bradycardia, dysrhythmias, hypertension, hypotension.
Cns: inebriation, irritability, ataxia, obtundation, coma, cerebral edema, seizures; may also have peripheral nervous system findings including cranial nerve abnormalities.
Gi: nausea, vomiting, abdominal pain.
Pulmonary: tachypnea, hyperventilation, Kussmaul respirations, pulmonary edema.
Renal: crystalluria and acute renal failure.
Three overlapping stages may be seen:
- First stage (1–12 hr): CNS depression, GI symptoms, worsening acidosis, coma, seizures, cerebral edema, tetany or myoclonus from hypocalcemia.
- Second stage (12–36 hr): cardiopulmonary manifestations; many deaths occur in this period.
- Third stage (36–72 hr): oliguria, flank pain, acute renal failure.
History
Intentional or unintentional ingestion may be reported. Consider this diagnosis even without a clear history when there is an unexplained high anion gap metabolic acidosis and/or an elevated, unexplained osmol gap.
Physical examination
Tachypnea and altered mental status are common.
Essential workup
Obtain a complete ingestion history. Draw the following simultaneously:
- Arterial blood gas
- Serum ethylene glycol, methanol, isopropyl alcohol, and ethanol concentrations
- Electrolytes, BUN/creatinine, glucose
- Measured serum osmolality (freezing point depression)
- Serum calcium, phosphorus, magnesium
Diagnosis tests and interpretation
Calculate the anion gap: (Na⁺) − (Cl⁻ + HCO₃⁻); normal is approximately 8–12.
Calculate the osmol gap: measured osmolality − calculated osmolarity; an increased gap is generally >10.
Calculated osmolarity: 2(Na⁺) + glucose/18 + BUN/2.8 + ethanol (mg/dL)/4.6.
The osmol gap is most useful early after ingestion (and may be larger with concurrent ethanol ingestion, with less severe acidosis). A normal osmol gap does not exclude ethylene glycol poisoning, especially with late presentation when metabolites drive an anion gap acidosis.
Urinalysis may show envelope-shaped calcium oxalate crystals (specific but insensitive). Absence of crystals does not rule out exposure.
Wood lamp inspection of urine or gastric contents may show fluorescein from antifreeze, but this is insensitive and nonspecific.
Differential diagnosis
Elevated osmol gap: methanol, ethanol, isopropyl alcohol, mannitol/glycerin/propylene glycol/sorbitol, acetone/ammonia, propylene glycol.
Elevated anion gap metabolic acidosis: alcoholic ketoacidosis, toxic asphyxiants (e.g., cyanide/CO/H₂S), acetaminophen-related causes, antiretrovirals (NRTIs), toluene, metformin, uremia, DKA, iron/INH, lactic acidosis, salicylates, starvation ketosis, methanol, ethylene glycol.
Treatment
Prehospital care
Bring containers of suspected substances. Monitor airway and mental status. For dermal exposure, remove contaminated clothing/jewelry and irrigate with soap and water.
Initial stabilization and therapy
ABCs. Provide supplemental oxygen, cardiac monitoring, and IV access with 0.9% saline. For altered mental status, check glucose and consider dextrose, naloxone, and thiamine as appropriate.
Emergency department treatment and procedures
- Limit absorption: gastric lavage may be considered only in select cases (<1 hr since ingestion, coma, or reported large ingestion). activated charcoal may be given for coingestants but adsorbs ethylene glycol poorly.< />pan>
- Block toxic metabolism: initiate fomepizole promptly when a potentially toxic ingestion is suspected (intentional ingestion, more than a “sip,” or unexplained osmol gap and/or anion gap acidosis with concerning presentation). Do not wait for confirmatory levels if suspicion is high.
- Alternative antidote: ethanol is second-line if fomepizole is unavailable, targeting a serum ethanol level of 100–150 mg/dL, and continuing until ethylene glycol level is ~25 mg/dL.
- Adjunct cofactors: thiamine, pyridoxine, and magnesium may be given to support metabolism toward less toxic pathways (human outcome data are limited).
- Hemodialysis: use to accelerate clearance of ethylene glycol and metabolites. Consider for severe acidosis, persistent metabolic derangements, renal insufficiency, pulmonary edema, cerebral edema, or ethylene glycol concentration >25 mg/dL; continue until level approaches 25 mg/dL and acidosis resolves.
- Correct complications: ensure urine output with IV fluids. Use sodium bicarbonate for severe acidemia (commonly when pH <7.1) to maintain ph in the normal range. monitor and replace calcium as needed because oxalate formation can lower serum calcium.< />pan>
Pregnancy considerations
Fomepizole is class C in pregnancy. Ethanol is not recommended.
Pediatric considerations
Ethanol can cause significant CNS depression and hypoglycemia in children.
Medication
Activated charcoal: 1 g/kg PO.
Dextrose: D50W 25 g IV (peds: D25W 2–4 mL/kg).
Ethanol: oral (via NG) or IV 10% ethanol in D5W per dosing protocols; adjust during hemodialysis.
Fomepizole: 15 mg/kg IV load over 30 min, then 10 mg/kg q12h ×4 doses, then 15 mg/kg q12h until level <25 mg />L; dose adjustments required during hemodialysis.
Magnesium: 25–50 mg/kg IV once (max 2 g).
Naloxone: 2 mg IV/IM (peds: 0.1 mg/kg).
Pyridoxine: 100 mg daily for 2 days.
Sodium bicarbonate: 1–2 mEq/kg IV in D5W.
Thiamine: 100 mg daily for 2 days (peds: 50 mg).
Follow-up and disposition
Admission criteria
Admit all patients with significant suspected or confirmed ethylene glycol ingestion, even if initially asymptomatic. ICU admission is indicated for serious illness, metabolic acidosis, or renal failure. Transfer if fomepizole or hemodialysis is indicated but not available.
Discharge criteria
An asymptomatic patient with isolated exposure may be discharged only if ethylene glycol concentration is undetectable and there is no metabolic acidosis.
Follow-up recommendations
Psychiatric evaluation is indicated after intentional ingestion.
Clinical pearls and common pitfalls
An osmol gap <10 does not exclude ethylene glycol poisoning. treat early with fomepizole when the diagnosis is on table and confirm serum levels available. presentations may show only an osmol gap, while late anion gap. do use absence of urinary crystals or lack fluorescence under a wood lamp to rule out exposure. if confirmation, antidote availability, 24 /> hemodialysis capability is uncertain, transfer to a facility that has all of these resources.

- Published on
Emergency And Acute Medicine - Esophageal trauma
Basic description
The adult esophagus is approximately 25–30 cm in length and lies in close proximity to the mediastinum, with potential access to the pleural space. It begins at the hypopharynx posterior to the larynx at the level of the cricoid cartilage. On either side are the piriform recesses, which are common sites for foreign body lodgment.
Physiologic narrowing occurs at the cricopharyngeal muscle (upper esophageal sphincter), at the crossover of the left mainstem bronchus and aortic arch, and at the gastroesophageal junction (lower esophageal sphincter). Additional narrowing may occur in areas of disease such as malignancy, webs, or Schatzki rings.
The upper third of the esophagus consists of striated muscle and initiates swallowing. The middle third contains both striated and smooth muscle, and the distal third is composed entirely of smooth muscle. Although relatively fixed, the esophagus may be displaced by adjacent structures such as goiter, enlarged atria, or mediastinal masses.
Etiology
Esophageal trauma may result from external or internal forces.
External mechanisms include penetrating injuries such as stab or missile wounds, direct perforation from foreign bodies, pressure necrosis, chemical or radiation injury, and iatrogenic trauma from instrumentation. Blunt trauma, most commonly from motor vehicle collisions, may also cause injury.
Internal mechanisms include caustic ingestions, infections, medication-induced injury, swallowed foreign bodies, iatrogenic causes, and barotrauma.
Caustic ingestions include alkali substances, which cause liquefaction necrosis and deep tissue penetration, and acids, which cause coagulation necrosis and thermal injury. Chlorine bleach typically causes mucosal edema and superficial erythema.
Infectious causes include viral infections such as CMV, HPV, and HSV, and fungal infections in immunocompromised patients.
Medication-related injury has been reported with agents such as alendronate, doxycycline, NSAIDs, and mycophenolate mofetil.
Swallowed foreign bodies include food bolus impaction, coins, bones, pins, and button batteries. Meat impaction is the most common type in adults, particularly among prisoners, psychiatric patients, intoxicated individuals, and edentulous patients.
Iatrogenic injury accounts for more than half of cases, most commonly due to endoscopy, nasogastric tube placement, or nasotracheal intubation.
Increased intraluminal pressure from vomiting or retching may result in Mallory–Weiss tears, which are mucosal lacerations with bleeding, or Boerhaave syndrome, which is a spontaneous full-thickness rupture of the distal esophagus.
Pediatric considerations
Foreign body ingestion accounts for most cases of esophageal trauma in children, particularly in those aged 18–48 months. Perforations are most often iatrogenic. Caustic ingestions are more common in children younger than five years. Button batteries lodged in the esophagus require urgent removal due to their highly alkaline nature. Single-use laundry detergent packets are an increasingly common hazard.
Diagnosis – signs and symptoms
Common symptoms include dysphagia, odynophagia, chest pain that may be pleuritic and severe, hoarseness, and dyspnea.
Tears or perforations may present with bleeding or hematemesis.
Foreign body ingestion may cause drooling, choking, gagging, vomiting, stridor, wheezing, or inability to tolerate oral intake.
Caustic ingestion may produce oral pain, abdominal pain, vomiting, and drooling.
History
Key historical elements include the type, amount, and timing of ingestions; history of prolonged vomiting; sudden inability to swallow after eating; foreign body sensation; penetrating trauma; or prior cancer therapy.
Physical examination
Findings suggestive of perforation include subcutaneous emphysema at the base of the neck, a Hamman crunch due to mediastinal air, signs of shock, septicemia, or peritonitis.
Penetrating trauma may be associated with injuries to the trachea, neck, chest, or abdomen.
Caustic ingestions may cause airway edema with stridor and visible oral burns.
Essential workup
A high index of suspicion and early diagnosis are critical. Mortality for esophageal perforation is less than 5% if repaired within 24 hours but increases dramatically with delayed diagnosis. Early endoscopy is indicated for caustic ingestions. Chest and lateral neck radiographs are part of the initial evaluation.
Diagnosis tests and interpretation
Laboratory studies may include complete blood count, type and crossmatch for significant bleeding, coagulation studies, electrolytes for prolonged vomiting or retained foreign body, and arterial blood gas analysis in acid ingestions.
Imaging includes chest radiography to assess for pneumomediastinum, pneumothorax, widened mediastinum, or pleural effusion. Lateral cervical spine radiographs may reveal retropharyngeal air or fluid.
Esophagram is useful for suspected perforation, with water-soluble contrast preferred initially. Endoscopy is indicated for suspected perforation, caustic injury, or foreign body removal. CT with dilute oral contrast may aid in identifying perforation and associated complications.
Differential diagnosis
Pulmonary causes include tracheal injury and pneumothorax. Cardiovascular causes include myocardial infarction and aortic dissection. Other esophageal conditions include strictures, neoplasm, Schatzki ring, diverticula, achalasia, esophageal spasm, gastroesophageal reflux, and medication-induced esophagitis.
Treatment
Prehospital care
Chest pain should be presumed cardiac until proven otherwise. Airway protection, suctioning of secretions, intravenous fluids for hypotension or bleeding, and analgesia are indicated. Neutralizing agents and large volumes of oral fluids should be avoided in caustic ingestions.
Initial stabilization and therapy
Airway management and resuscitation are priorities. Establish intravenous access, initiate monitoring, and consider early intubation for penetrating neck or chest injuries.
Emergency department treatment and procedures
Most foreign bodies pass spontaneously, but endoscopic removal is required in a significant minority. Pharmacologic measures such as glucagon, nitroglycerin, or benzodiazepines may be attempted for food impaction. Gastroenterology consultation is indicated if these measures fail.
Caustic ingestions require avoidance of emesis and lavage, cautious dilution with milk, and early endoscopy for prognostication. Corticosteroids are not recommended.
Partial-thickness tears generally heal spontaneously. Full-thickness perforations require surgical consultation, broad-spectrum intravenous antibiotics, and possible operative repair.
Medication
For food impaction, glucagon, nitroglycerin, or diazepam may be used selectively.
For perforation, broad-spectrum intravenous antibiotics such as cefoxitin with gentamicin are indicated. Steroids are not indicated in caustic injury.
Follow-up and disposition
Admission criteria
Indications for admission include caustic ingestion, sharp foreign bodies, airway compromise, penetrating neck or chest trauma, evidence of sepsis or mediastinitis, esophageal perforation, significant bleeding, and inability to tolerate oral intake.
Discharge criteria
Patients may be discharged if bleeding from a partial-thickness tear is self-limited or if a foreign body or food bolus has passed beyond the lower esophageal sphincter without complications.
Clinical pearls and common pitfalls
Time to diagnosis and definitive therapy is the most important predictor of outcome, with intervention within 24 hours significantly reducing mortality. Cervical injuries have better outcomes than thoracic or abdominal injuries. Spontaneous perforation carries the highest mortality, followed by iatrogenic and then traumatic causes.
Basic description
The adult esophagus is approximately 25–30 cm in length and lies in close proximity to the mediastinum, with potential access to the pleural space. It begins at the hypopharynx posterior to the larynx at the level of the cricoid cartilage. On either side are the piriform recesses, which are common sites for foreign body lodgment.
Physiologic narrowing occurs at the cricopharyngeal muscle (upper esophageal sphincter), at the crossover of the left mainstem bronchus and aortic arch, and at the gastroesophageal junction (lower esophageal sphincter). Additional narrowing may occur in areas of disease such as malignancy, webs, or Schatzki rings.
The upper third of the esophagus consists of striated muscle and initiates swallowing. The middle third contains both striated and smooth muscle, and the distal third is composed entirely of smooth muscle. Although relatively fixed, the esophagus may be displaced by adjacent structures such as goiter, enlarged atria, or mediastinal masses.
Etiology
Esophageal trauma may result from external or internal forces.
External mechanisms include penetrating injuries such as stab or missile wounds, direct perforation from foreign bodies, pressure necrosis, chemical or radiation injury, and iatrogenic trauma from instrumentation. Blunt trauma, most commonly from motor vehicle collisions, may also cause injury.
Internal mechanisms include caustic ingestions, infections, medication-induced injury, swallowed foreign bodies, iatrogenic causes, and barotrauma.
Caustic ingestions include alkali substances, which cause liquefaction necrosis and deep tissue penetration, and acids, which cause coagulation necrosis and thermal injury. Chlorine bleach typically causes mucosal edema and superficial erythema.
Infectious causes include viral infections such as CMV, HPV, and HSV, and fungal infections in immunocompromised patients.
Medication-related injury has been reported with agents such as alendronate, doxycycline, NSAIDs, and mycophenolate mofetil.
Swallowed foreign bodies include food bolus impaction, coins, bones, pins, and button batteries. Meat impaction is the most common type in adults, particularly among prisoners, psychiatric patients, intoxicated individuals, and edentulous patients.
Iatrogenic injury accounts for more than half of cases, most commonly due to endoscopy, nasogastric tube placement, or nasotracheal intubation.
Increased intraluminal pressure from vomiting or retching may result in Mallory–Weiss tears, which are mucosal lacerations with bleeding, or Boerhaave syndrome, which is a spontaneous full-thickness rupture of the distal esophagus.
Pediatric considerations
Foreign body ingestion accounts for most cases of esophageal trauma in children, particularly in those aged 18–48 months. Perforations are most often iatrogenic. Caustic ingestions are more common in children younger than five years. Button batteries lodged in the esophagus require urgent removal due to their highly alkaline nature. Single-use laundry detergent packets are an increasingly common hazard.
Diagnosis – signs and symptoms
Common symptoms include dysphagia, odynophagia, chest pain that may be pleuritic and severe, hoarseness, and dyspnea.
Tears or perforations may present with bleeding or hematemesis.
Foreign body ingestion may cause drooling, choking, gagging, vomiting, stridor, wheezing, or inability to tolerate oral intake.
Caustic ingestion may produce oral pain, abdominal pain, vomiting, and drooling.
History
Key historical elements include the type, amount, and timing of ingestions; history of prolonged vomiting; sudden inability to swallow after eating; foreign body sensation; penetrating trauma; or prior cancer therapy.
Physical examination
Findings suggestive of perforation include subcutaneous emphysema at the base of the neck, a Hamman crunch due to mediastinal air, signs of shock, septicemia, or peritonitis.
Penetrating trauma may be associated with injuries to the trachea, neck, chest, or abdomen.
Caustic ingestions may cause airway edema with stridor and visible oral burns.
Essential workup
A high index of suspicion and early diagnosis are critical. Mortality for esophageal perforation is less than 5% if repaired within 24 hours but increases dramatically with delayed diagnosis. Early endoscopy is indicated for caustic ingestions. Chest and lateral neck radiographs are part of the initial evaluation.
Diagnosis tests and interpretation
Laboratory studies may include complete blood count, type and crossmatch for significant bleeding, coagulation studies, electrolytes for prolonged vomiting or retained foreign body, and arterial blood gas analysis in acid ingestions.
Imaging includes chest radiography to assess for pneumomediastinum, pneumothorax, widened mediastinum, or pleural effusion. Lateral cervical spine radiographs may reveal retropharyngeal air or fluid.
Esophagram is useful for suspected perforation, with water-soluble contrast preferred initially. Endoscopy is indicated for suspected perforation, caustic injury, or foreign body removal. CT with dilute oral contrast may aid in identifying perforation and associated complications.
Differential diagnosis
Pulmonary causes include tracheal injury and pneumothorax. Cardiovascular causes include myocardial infarction and aortic dissection. Other esophageal conditions include strictures, neoplasm, Schatzki ring, diverticula, achalasia, esophageal spasm, gastroesophageal reflux, and medication-induced esophagitis.
Treatment
Prehospital care
Chest pain should be presumed cardiac until proven otherwise. Airway protection, suctioning of secretions, intravenous fluids for hypotension or bleeding, and analgesia are indicated. Neutralizing agents and large volumes of oral fluids should be avoided in caustic ingestions.
Initial stabilization and therapy
Airway management and resuscitation are priorities. Establish intravenous access, initiate monitoring, and consider early intubation for penetrating neck or chest injuries.
Emergency department treatment and procedures
Most foreign bodies pass spontaneously, but endoscopic removal is required in a significant minority. Pharmacologic measures such as glucagon, nitroglycerin, or benzodiazepines may be attempted for food impaction. Gastroenterology consultation is indicated if these measures fail.
Caustic ingestions require avoidance of emesis and lavage, cautious dilution with milk, and early endoscopy for prognostication. Corticosteroids are not recommended.
Partial-thickness tears generally heal spontaneously. Full-thickness perforations require surgical consultation, broad-spectrum intravenous antibiotics, and possible operative repair.
Medication
For food impaction, glucagon, nitroglycerin, or diazepam may be used selectively.
For perforation, broad-spectrum intravenous antibiotics such as cefoxitin with gentamicin are indicated. Steroids are not indicated in caustic injury.
Follow-up and disposition
Admission criteria
Indications for admission include caustic ingestion, sharp foreign bodies, airway compromise, penetrating neck or chest trauma, evidence of sepsis or mediastinitis, esophageal perforation, significant bleeding, and inability to tolerate oral intake.
Discharge criteria
Patients may be discharged if bleeding from a partial-thickness tear is self-limited or if a foreign body or food bolus has passed beyond the lower esophageal sphincter without complications.
Clinical pearls and common pitfalls
Time to diagnosis and definitive therapy is the most important predictor of outcome, with intervention within 24 hours significantly reducing mortality. Cervical injuries have better outcomes than thoracic or abdominal injuries. Spontaneous perforation carries the highest mortality, followed by iatrogenic and then traumatic causes.

- Published on
Emergency And Acute Medicine - Esophageal trauma
Basic description
The adult esophagus is approximately 25–30 cm in length and lies in close proximity to the mediastinum, with potential access to the pleural space. It begins at the hypopharynx posterior to the larynx at the level of the cricoid cartilage. On either side are the piriform recesses, which are common sites for foreign body lodgment.
Physiologic narrowing occurs at the cricopharyngeal muscle (upper esophageal sphincter), at the crossover of the left mainstem bronchus and aortic arch, and at the gastroesophageal junction (lower esophageal sphincter). Additional narrowing may occur in areas of disease such as malignancy, webs, or Schatzki rings.
The upper third of the esophagus consists of striated muscle and initiates swallowing. The middle third contains both striated and smooth muscle, and the distal third is composed entirely of smooth muscle. Although relatively fixed, the esophagus may be displaced by adjacent structures such as goiter, enlarged atria, or mediastinal masses.
Etiology
Esophageal trauma may result from external or internal forces.
External mechanisms include penetrating injuries such as stab or missile wounds, direct perforation from foreign bodies, pressure necrosis, chemical or radiation injury, and iatrogenic trauma from instrumentation. Blunt trauma, most commonly from motor vehicle collisions, may also cause injury.
Internal mechanisms include caustic ingestions, infections, medication-induced injury, swallowed foreign bodies, iatrogenic causes, and barotrauma.
Caustic ingestions include alkali substances, which cause liquefaction necrosis and deep tissue penetration, and acids, which cause coagulation necrosis and thermal injury. Chlorine bleach typically causes mucosal edema and superficial erythema.
Infectious causes include viral infections such as CMV, HPV, and HSV, and fungal infections in immunocompromised patients.
Medication-related injury has been reported with agents such as alendronate, doxycycline, NSAIDs, and mycophenolate mofetil.
Swallowed foreign bodies include food bolus impaction, coins, bones, pins, and button batteries. Meat impaction is the most common type in adults, particularly among prisoners, psychiatric patients, intoxicated individuals, and edentulous patients.
Iatrogenic injury accounts for more than half of cases, most commonly due to endoscopy, nasogastric tube placement, or nasotracheal intubation.
Increased intraluminal pressure from vomiting or retching may result in Mallory–Weiss tears, which are mucosal lacerations with bleeding, or Boerhaave syndrome, which is a spontaneous full-thickness rupture of the distal esophagus.
Pediatric considerations
Foreign body ingestion accounts for most cases of esophageal trauma in children, particularly in those aged 18–48 months. Perforations are most often iatrogenic. Caustic ingestions are more common in children younger than five years. Button batteries lodged in the esophagus require urgent removal due to their highly alkaline nature. Single-use laundry detergent packets are an increasingly common hazard.
Diagnosis – signs and symptoms
Common symptoms include dysphagia, odynophagia, chest pain that may be pleuritic and severe, hoarseness, and dyspnea.
Tears or perforations may present with bleeding or hematemesis.
Foreign body ingestion may cause drooling, choking, gagging, vomiting, stridor, wheezing, or inability to tolerate oral intake.
Caustic ingestion may produce oral pain, abdominal pain, vomiting, and drooling.
History
Key historical elements include the type, amount, and timing of ingestions; history of prolonged vomiting; sudden inability to swallow after eating; foreign body sensation; penetrating trauma; or prior cancer therapy.
Physical examination
Findings suggestive of perforation include subcutaneous emphysema at the base of the neck, a Hamman crunch due to mediastinal air, signs of shock, septicemia, or peritonitis.
Penetrating trauma may be associated with injuries to the trachea, neck, chest, or abdomen.
Caustic ingestions may cause airway edema with stridor and visible oral burns.
Essential workup
A high index of suspicion and early diagnosis are critical. Mortality for esophageal perforation is less than 5% if repaired within 24 hours but increases dramatically with delayed diagnosis. Early endoscopy is indicated for caustic ingestions. Chest and lateral neck radiographs are part of the initial evaluation.
Diagnosis tests and interpretation
Laboratory studies may include complete blood count, type and crossmatch for significant bleeding, coagulation studies, electrolytes for prolonged vomiting or retained foreign body, and arterial blood gas analysis in acid ingestions.
Imaging includes chest radiography to assess for pneumomediastinum, pneumothorax, widened mediastinum, or pleural effusion. Lateral cervical spine radiographs may reveal retropharyngeal air or fluid.
Esophagram is useful for suspected perforation, with water-soluble contrast preferred initially. Endoscopy is indicated for suspected perforation, caustic injury, or foreign body removal. CT with dilute oral contrast may aid in identifying perforation and associated complications.
Differential diagnosis
Pulmonary causes include tracheal injury and pneumothorax. Cardiovascular causes include myocardial infarction and aortic dissection. Other esophageal conditions include strictures, neoplasm, Schatzki ring, diverticula, achalasia, esophageal spasm, gastroesophageal reflux, and medication-induced esophagitis.
Treatment
Prehospital care
Chest pain should be presumed cardiac until proven otherwise. Airway protection, suctioning of secretions, intravenous fluids for hypotension or bleeding, and analgesia are indicated. Neutralizing agents and large volumes of oral fluids should be avoided in caustic ingestions.
Initial stabilization and therapy
Airway management and resuscitation are priorities. Establish intravenous access, initiate monitoring, and consider early intubation for penetrating neck or chest injuries.
Emergency department treatment and procedures
Most foreign bodies pass spontaneously, but endoscopic removal is required in a significant minority. Pharmacologic measures such as glucagon, nitroglycerin, or benzodiazepines may be attempted for food impaction. Gastroenterology consultation is indicated if these measures fail.
Caustic ingestions require avoidance of emesis and lavage, cautious dilution with milk, and early endoscopy for prognostication. Corticosteroids are not recommended.
Partial-thickness tears generally heal spontaneously. Full-thickness perforations require surgical consultation, broad-spectrum intravenous antibiotics, and possible operative repair.
Medication
For food impaction, glucagon, nitroglycerin, or diazepam may be used selectively.
For perforation, broad-spectrum intravenous antibiotics such as cefoxitin with gentamicin are indicated. Steroids are not indicated in caustic injury.
Follow-up and disposition
Admission criteria
Indications for admission include caustic ingestion, sharp foreign bodies, airway compromise, penetrating neck or chest trauma, evidence of sepsis or mediastinitis, esophageal perforation, significant bleeding, and inability to tolerate oral intake.
Discharge criteria
Patients may be discharged if bleeding from a partial-thickness tear is self-limited or if a foreign body or food bolus has passed beyond the lower esophageal sphincter without complications.
Clinical pearls and common pitfalls
Time to diagnosis and definitive therapy is the most important predictor of outcome, with intervention within 24 hours significantly reducing mortality. Cervical injuries have better outcomes than thoracic or abdominal injuries. Spontaneous perforation carries the highest mortality, followed by iatrogenic and then traumatic causes.
Basic description
The adult esophagus is approximately 25–30 cm in length and lies in close proximity to the mediastinum, with potential access to the pleural space. It begins at the hypopharynx posterior to the larynx at the level of the cricoid cartilage. On either side are the piriform recesses, which are common sites for foreign body lodgment.
Physiologic narrowing occurs at the cricopharyngeal muscle (upper esophageal sphincter), at the crossover of the left mainstem bronchus and aortic arch, and at the gastroesophageal junction (lower esophageal sphincter). Additional narrowing may occur in areas of disease such as malignancy, webs, or Schatzki rings.
The upper third of the esophagus consists of striated muscle and initiates swallowing. The middle third contains both striated and smooth muscle, and the distal third is composed entirely of smooth muscle. Although relatively fixed, the esophagus may be displaced by adjacent structures such as goiter, enlarged atria, or mediastinal masses.
Etiology
Esophageal trauma may result from external or internal forces.
External mechanisms include penetrating injuries such as stab or missile wounds, direct perforation from foreign bodies, pressure necrosis, chemical or radiation injury, and iatrogenic trauma from instrumentation. Blunt trauma, most commonly from motor vehicle collisions, may also cause injury.
Internal mechanisms include caustic ingestions, infections, medication-induced injury, swallowed foreign bodies, iatrogenic causes, and barotrauma.
Caustic ingestions include alkali substances, which cause liquefaction necrosis and deep tissue penetration, and acids, which cause coagulation necrosis and thermal injury. Chlorine bleach typically causes mucosal edema and superficial erythema.
Infectious causes include viral infections such as CMV, HPV, and HSV, and fungal infections in immunocompromised patients.
Medication-related injury has been reported with agents such as alendronate, doxycycline, NSAIDs, and mycophenolate mofetil.
Swallowed foreign bodies include food bolus impaction, coins, bones, pins, and button batteries. Meat impaction is the most common type in adults, particularly among prisoners, psychiatric patients, intoxicated individuals, and edentulous patients.
Iatrogenic injury accounts for more than half of cases, most commonly due to endoscopy, nasogastric tube placement, or nasotracheal intubation.
Increased intraluminal pressure from vomiting or retching may result in Mallory–Weiss tears, which are mucosal lacerations with bleeding, or Boerhaave syndrome, which is a spontaneous full-thickness rupture of the distal esophagus.
Pediatric considerations
Foreign body ingestion accounts for most cases of esophageal trauma in children, particularly in those aged 18–48 months. Perforations are most often iatrogenic. Caustic ingestions are more common in children younger than five years. Button batteries lodged in the esophagus require urgent removal due to their highly alkaline nature. Single-use laundry detergent packets are an increasingly common hazard.
Diagnosis – signs and symptoms
Common symptoms include dysphagia, odynophagia, chest pain that may be pleuritic and severe, hoarseness, and dyspnea.
Tears or perforations may present with bleeding or hematemesis.
Foreign body ingestion may cause drooling, choking, gagging, vomiting, stridor, wheezing, or inability to tolerate oral intake.
Caustic ingestion may produce oral pain, abdominal pain, vomiting, and drooling.
History
Key historical elements include the type, amount, and timing of ingestions; history of prolonged vomiting; sudden inability to swallow after eating; foreign body sensation; penetrating trauma; or prior cancer therapy.
Physical examination
Findings suggestive of perforation include subcutaneous emphysema at the base of the neck, a Hamman crunch due to mediastinal air, signs of shock, septicemia, or peritonitis.
Penetrating trauma may be associated with injuries to the trachea, neck, chest, or abdomen.
Caustic ingestions may cause airway edema with stridor and visible oral burns.
Essential workup
A high index of suspicion and early diagnosis are critical. Mortality for esophageal perforation is less than 5% if repaired within 24 hours but increases dramatically with delayed diagnosis. Early endoscopy is indicated for caustic ingestions. Chest and lateral neck radiographs are part of the initial evaluation.
Diagnosis tests and interpretation
Laboratory studies may include complete blood count, type and crossmatch for significant bleeding, coagulation studies, electrolytes for prolonged vomiting or retained foreign body, and arterial blood gas analysis in acid ingestions.
Imaging includes chest radiography to assess for pneumomediastinum, pneumothorax, widened mediastinum, or pleural effusion. Lateral cervical spine radiographs may reveal retropharyngeal air or fluid.
Esophagram is useful for suspected perforation, with water-soluble contrast preferred initially. Endoscopy is indicated for suspected perforation, caustic injury, or foreign body removal. CT with dilute oral contrast may aid in identifying perforation and associated complications.
Differential diagnosis
Pulmonary causes include tracheal injury and pneumothorax. Cardiovascular causes include myocardial infarction and aortic dissection. Other esophageal conditions include strictures, neoplasm, Schatzki ring, diverticula, achalasia, esophageal spasm, gastroesophageal reflux, and medication-induced esophagitis.
Treatment
Prehospital care
Chest pain should be presumed cardiac until proven otherwise. Airway protection, suctioning of secretions, intravenous fluids for hypotension or bleeding, and analgesia are indicated. Neutralizing agents and large volumes of oral fluids should be avoided in caustic ingestions.
Initial stabilization and therapy
Airway management and resuscitation are priorities. Establish intravenous access, initiate monitoring, and consider early intubation for penetrating neck or chest injuries.
Emergency department treatment and procedures
Most foreign bodies pass spontaneously, but endoscopic removal is required in a significant minority. Pharmacologic measures such as glucagon, nitroglycerin, or benzodiazepines may be attempted for food impaction. Gastroenterology consultation is indicated if these measures fail.
Caustic ingestions require avoidance of emesis and lavage, cautious dilution with milk, and early endoscopy for prognostication. Corticosteroids are not recommended.
Partial-thickness tears generally heal spontaneously. Full-thickness perforations require surgical consultation, broad-spectrum intravenous antibiotics, and possible operative repair.
Medication
For food impaction, glucagon, nitroglycerin, or diazepam may be used selectively.
For perforation, broad-spectrum intravenous antibiotics such as cefoxitin with gentamicin are indicated. Steroids are not indicated in caustic injury.
Follow-up and disposition
Admission criteria
Indications for admission include caustic ingestion, sharp foreign bodies, airway compromise, penetrating neck or chest trauma, evidence of sepsis or mediastinitis, esophageal perforation, significant bleeding, and inability to tolerate oral intake.
Discharge criteria
Patients may be discharged if bleeding from a partial-thickness tear is self-limited or if a foreign body or food bolus has passed beyond the lower esophageal sphincter without complications.
Clinical pearls and common pitfalls
Time to diagnosis and definitive therapy is the most important predictor of outcome, with intervention within 24 hours significantly reducing mortality. Cervical injuries have better outcomes than thoracic or abdominal injuries. Spontaneous perforation carries the highest mortality, followed by iatrogenic and then traumatic causes.

- Published on
Emergency And Acute Medicine - Erythema multiforme
Basic description
Erythema multiforme is a rash caused by a hypersensitivity reaction that may occur in response to medications, infections, or other illnesses.
Erythema multiforme minor is characterized by typical target lesions and edematous papules, usually distributed peripherally. It is a benign, self-limited condition and is generally not associated with serious acute illness.
Erythema multiforme major, also referred to as bullous erythema multiforme, presents with similar target lesions and edematous papules in a peripheral distribution but includes involvement of one or more mucous membranes with less than 10% total body surface area epidermal detachment.
It is important to differentiate erythema multiforme from Stevens–Johnson syndrome, which also involves less than 10% total body surface area epidermal detachment but typically presents with more widespread blistering over the trunk and face and prominent mucosal involvement, and from toxic epidermal necrolysis, which involves more than 30% total body surface area detachment.
Erythema multiforme is now considered a distinct entity separate from Stevens–Johnson syndrome and toxic epidermal necrolysis. It most commonly affects children and young adults, with more than half of cases occurring in patients younger than 20 years. Males are affected more often than females.
Etiology
Erythema multiforme is a hypersensitivity reaction, likely related to a transient autoimmune defect. Herpes simplex virus is the most common precipitating factor, accounting for more than 70% of cases. Other causes include idiopathic disease, medications such as penicillins, sulfa-based drugs, phenytoin, barbiturates, and NSAIDs, vaccines including diphtheria–tetanus, hepatitis B, and smallpox, as well as malignancy and infections such as HIV, cytomegalovirus, hepatitis C, and Mycoplasma infections.
Diagnosis – signs and symptoms
Patients may have a mild prodrome with low-grade fever or malaise, although systemic symptoms are infrequent. A history of antecedent herpes simplex infection within three weeks is common. The condition is usually not associated with severe systemic illness.
Physical examination
The characteristic rash consists of symmetric dull red macules and papules that evolve into round, well-demarcated target lesions with central clearing. There is no epidermal necrosis in erythema multiforme minor. The term “multiforme” reflects the presence of lesions at various stages of evolution simultaneously.
Lesions are typically distributed on the extremities, especially the dorsal hands and feet, extensor surfaces, elbows, and knees, and erythema multiforme is one of the few rashes that may involve the palms and soles. The rash often spreads from the extremities toward the trunk.
Mucosal involvement, when present, usually consists of minor blistering or erosions affecting a single mucosal surface, most commonly the lips or oral cavity. The duration of illness is usually one to four weeks, although recurrent or chronic cases may occur.
Essential workup
Evaluation consists of a complete history and physical examination, with particular attention to skin findings, recent infections, medication exposure, and genitourinary involvement.
Diagnosis tests and interpretation
No specific laboratory tests or imaging studies are required. Skin biopsy, when performed, shows a mononuclear cell infiltrate around superficial dermal blood vessels without leukocytoclastic vasculitis or epidermal keratinocyte necrosis. Biopsy is not necessary in most cases.
Differential diagnosis
Systemic lupus erythematosus, fixed drug eruption, pityriasis rosea, secondary syphilis, erythema migrans, urticaria, viral exanthem, vasculitis, Stevens–Johnson syndrome, and toxic epidermal necrolysis.
Treatment
Prehospital care
Erythema multiforme is not contagious and does not require isolation or postexposure prophylaxis.
Initial stabilization and therapy
The condition is generally benign and self-limited and does not require acute stabilization.
Emergency department treatment and procedures
Management focuses on identifying and removing the underlying cause when possible. Treatment is primarily symptomatic and includes cool compresses and antipruritic measures.
Medication
Antiviral therapy may be considered in acute herpes-associated erythema multiforme if initiated within 48 hours of onset, although it may not significantly alter the clinical course. Acyclovir may be used for prevention of recurrent disease.
Antipruritic agents such as cetirizine, diphenhydramine, or hydroxyzine can be used for symptomatic relief.
Topical corticosteroids of low to medium potency are first-line therapy for skin lesions, with low-potency agents reserved for the face or intertriginous areas.
Oral corticosteroids are reserved for severe mucosal disease. Topical anesthetic mouth rinses may be used for painful oral lesions.
Follow-up and disposition
Admission criteria
Admission is rarely required and is generally limited to patients unable to tolerate oral intake due to severe mucosal involvement or those requiring hospitalization for another concurrent condition.
Discharge criteria
Most patients can be safely discharged, as erythema multiforme is typically a benign and self-limited disorder.
Issues for referral
Referral to dermatology is recommended if the diagnosis is uncertain or if the rash is atypical or severe. Immediate ophthalmology referral is required for any ocular involvement.
Follow-up recommendations
Patients should follow up with a primary care physician within one week to assess progression or resolution of the rash and to evaluate for underlying triggers such as infection, medications, or malignancy. Dermatology follow-up within one week is appropriate if diagnostic uncertainty remains.
Clinical pearls and common pitfalls
Severe systemic illness should prompt consideration of alternative diagnoses such as Stevens–Johnson syndrome or toxic epidermal necrolysis. Most patients with erythema multiforme have an underlying herpes simplex infection. Secondary syphilis may produce similar lesions on the palms and soles. Reassurance is important, as erythema multiforme is usually benign and self-limited.
Basic description
Erythema multiforme is a rash caused by a hypersensitivity reaction that may occur in response to medications, infections, or other illnesses.
Erythema multiforme minor is characterized by typical target lesions and edematous papules, usually distributed peripherally. It is a benign, self-limited condition and is generally not associated with serious acute illness.
Erythema multiforme major, also referred to as bullous erythema multiforme, presents with similar target lesions and edematous papules in a peripheral distribution but includes involvement of one or more mucous membranes with less than 10% total body surface area epidermal detachment.
It is important to differentiate erythema multiforme from Stevens–Johnson syndrome, which also involves less than 10% total body surface area epidermal detachment but typically presents with more widespread blistering over the trunk and face and prominent mucosal involvement, and from toxic epidermal necrolysis, which involves more than 30% total body surface area detachment.
Erythema multiforme is now considered a distinct entity separate from Stevens–Johnson syndrome and toxic epidermal necrolysis. It most commonly affects children and young adults, with more than half of cases occurring in patients younger than 20 years. Males are affected more often than females.
Etiology
Erythema multiforme is a hypersensitivity reaction, likely related to a transient autoimmune defect. Herpes simplex virus is the most common precipitating factor, accounting for more than 70% of cases. Other causes include idiopathic disease, medications such as penicillins, sulfa-based drugs, phenytoin, barbiturates, and NSAIDs, vaccines including diphtheria–tetanus, hepatitis B, and smallpox, as well as malignancy and infections such as HIV, cytomegalovirus, hepatitis C, and Mycoplasma infections.
Diagnosis – signs and symptoms
Patients may have a mild prodrome with low-grade fever or malaise, although systemic symptoms are infrequent. A history of antecedent herpes simplex infection within three weeks is common. The condition is usually not associated with severe systemic illness.
Physical examination
The characteristic rash consists of symmetric dull red macules and papules that evolve into round, well-demarcated target lesions with central clearing. There is no epidermal necrosis in erythema multiforme minor. The term “multiforme” reflects the presence of lesions at various stages of evolution simultaneously.
Lesions are typically distributed on the extremities, especially the dorsal hands and feet, extensor surfaces, elbows, and knees, and erythema multiforme is one of the few rashes that may involve the palms and soles. The rash often spreads from the extremities toward the trunk.
Mucosal involvement, when present, usually consists of minor blistering or erosions affecting a single mucosal surface, most commonly the lips or oral cavity. The duration of illness is usually one to four weeks, although recurrent or chronic cases may occur.
Essential workup
Evaluation consists of a complete history and physical examination, with particular attention to skin findings, recent infections, medication exposure, and genitourinary involvement.
Diagnosis tests and interpretation
No specific laboratory tests or imaging studies are required. Skin biopsy, when performed, shows a mononuclear cell infiltrate around superficial dermal blood vessels without leukocytoclastic vasculitis or epidermal keratinocyte necrosis. Biopsy is not necessary in most cases.
Differential diagnosis
Systemic lupus erythematosus, fixed drug eruption, pityriasis rosea, secondary syphilis, erythema migrans, urticaria, viral exanthem, vasculitis, Stevens–Johnson syndrome, and toxic epidermal necrolysis.
Treatment
Prehospital care
Erythema multiforme is not contagious and does not require isolation or postexposure prophylaxis.
Initial stabilization and therapy
The condition is generally benign and self-limited and does not require acute stabilization.
Emergency department treatment and procedures
Management focuses on identifying and removing the underlying cause when possible. Treatment is primarily symptomatic and includes cool compresses and antipruritic measures.
Medication
Antiviral therapy may be considered in acute herpes-associated erythema multiforme if initiated within 48 hours of onset, although it may not significantly alter the clinical course. Acyclovir may be used for prevention of recurrent disease.
Antipruritic agents such as cetirizine, diphenhydramine, or hydroxyzine can be used for symptomatic relief.
Topical corticosteroids of low to medium potency are first-line therapy for skin lesions, with low-potency agents reserved for the face or intertriginous areas.
Oral corticosteroids are reserved for severe mucosal disease. Topical anesthetic mouth rinses may be used for painful oral lesions.
Follow-up and disposition
Admission criteria
Admission is rarely required and is generally limited to patients unable to tolerate oral intake due to severe mucosal involvement or those requiring hospitalization for another concurrent condition.
Discharge criteria
Most patients can be safely discharged, as erythema multiforme is typically a benign and self-limited disorder.
Issues for referral
Referral to dermatology is recommended if the diagnosis is uncertain or if the rash is atypical or severe. Immediate ophthalmology referral is required for any ocular involvement.
Follow-up recommendations
Patients should follow up with a primary care physician within one week to assess progression or resolution of the rash and to evaluate for underlying triggers such as infection, medications, or malignancy. Dermatology follow-up within one week is appropriate if diagnostic uncertainty remains.
Clinical pearls and common pitfalls
Severe systemic illness should prompt consideration of alternative diagnoses such as Stevens–Johnson syndrome or toxic epidermal necrolysis. Most patients with erythema multiforme have an underlying herpes simplex infection. Secondary syphilis may produce similar lesions on the palms and soles. Reassurance is important, as erythema multiforme is usually benign and self-limited.

- Published on
Emergency And Acute Medicine – Foreign Body in the ear
Basics Description
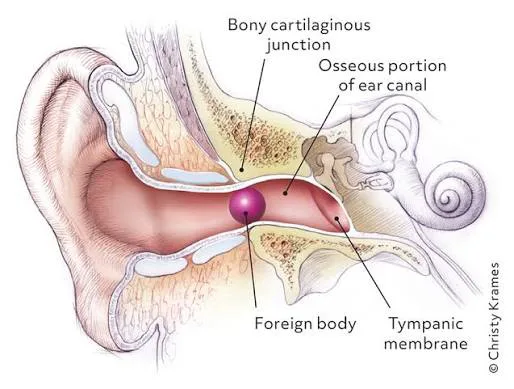
Foreign bodies lodged in the external auditory canal are common, particularly in children younger than 8 years. The canal is a cartilaginous and bony passage lined with highly sensitive periosteum, making removal painful; small children may require procedural sedation or general anesthesia. Foreign bodies often lodge at the junction of the cartilaginous and bony canal or at the isthmus. The canal is innervated by the facial, glossopharyngeal, and vagus nerves.
Inanimate objects often present late because children may delay reporting. The right ear is more commonly involved due to right-handedness. Predisposing factors include cerumen impaction, pica, and psychiatric illness.
Complications include canal laceration, tympanic membrane perforation (often iatrogenic), otitis externa, temporomandibular joint erosion, parapharyngeal abscess, mastoiditis, meningitis, and brain abscess. Button batteries are particularly dangerous due to electrical injury and pressure necrosis, often causing rapid tissue destruction.
Etiology
Children commonly insert beads, stones, paper, seeds, popcorn kernels, beans, toys, and button batteries. Adults more often present with cotton-swab tips, earplugs, insects (cockroaches most common in the US), or concealed illicit drugs.
Diagnosis Signs And Symptoms
Symptoms include unilateral ear pain, fullness, decreased hearing, crying in infants, buzzing or movement sensation with live insects, nausea, dizziness, ipsilateral tearing, itching, bleeding, or purulent discharge.
History should include prior removal attempts and possible trauma.
Physical examination requires careful otoscopy before and after removal to identify the object type, assess swelling risk, evaluate for otitis externa, retained fragments, or tympanic membrane perforation. A bilateral ear exam and inspection of nostrils are essential, especially in children and psychiatric patients. Concerning findings such as vertigo, nystagmus, hearing loss, facial nerve weakness, or severe pain warrant ENT consultation.
Essential Workup
A careful otoscopic examination is the cornerstone. Identify the foreign body and minimize patient discomfort before attempting removal.
Diagnosis Tests And Interpretation
Laboratory studies are not indicated. CT imaging is reserved for suspected infectious, erosive, or intracranial complications. Otomicroscopy may assist when standard techniques fail.
Differential Diagnosis
Cerumen impaction, otitis externa, canal hematoma, granuloma, trauma, tympanic membrane perforation, residual inflammation after self-removal, and tumors.
Treatment
Prehospital care for suspected live insects includes instillation of warm lidocaine or mineral oil to immobilize the insect; field removal attempts are discouraged.
In the emergency department, ensure adequate lighting, proper head immobilization, and analgesia. Lidocaine (1–2%) may be instilled topically or injected into the canal walls. Procedural sedation is recommended for children or uncooperative adults and should be used early to prevent traumatic repeated attempts.
Removal techniques depend on object type: irrigation for non–button battery objects; forceps, hooks, suction, Fogarty catheter, or cyanoacrylate glue for selected cases; acetone for Styrofoam or adhesive materials. Vegetable matter should not be irrigated. Button batteries must never be irrigated and require urgent removal. Live insects should be killed first with lidocaine, alcohol, or mineral oil before extraction. Sharp objects and complicated cases require ENT referral.
Medication
Analgesia or sedation may include fentanyl, ketamine, or midazolam. Topical antibiotic-steroid drops are indicated if canal abrasion or infection is suspected. Oral antibiotics are reserved for tympanic membrane perforation or secondary infection.
Follow Up Disposition
Admission is required for button batteries that cannot be removed.
Discharge is appropriate once the foreign body is removed or if a nonhazardous object cannot be safely removed in the ED.
ENT referral is indicated for failed removal, complications, immunocompromised patients, or significant trauma.
Follow Up Recommendations
Advise patients not to insert objects into the ear. Provide short-term analgesia after traumatic removal. Treat otitis externa with topical antimicrobials. Avoid water submersion if trauma or infection is present and arrange ENT follow-up when indicated.
Key Practice Insights And Avoidable Errors
Early use of procedural sedation improves success and reduces complications. Never irrigate an ear containing a button battery, as this can rapidly worsen tissue necrosis.
Basics Description
Foreign bodies lodged in the external auditory canal are common, particularly in children younger than 8 years. The canal is a cartilaginous and bony passage lined with highly sensitive periosteum, making removal painful; small children may require procedural sedation or general anesthesia. Foreign bodies often lodge at the junction of the cartilaginous and bony canal or at the isthmus. The canal is innervated by the facial, glossopharyngeal, and vagus nerves.
Inanimate objects often present late because children may delay reporting. The right ear is more commonly involved due to right-handedness. Predisposing factors include cerumen impaction, pica, and psychiatric illness.
Complications include canal laceration, tympanic membrane perforation (often iatrogenic), otitis externa, temporomandibular joint erosion, parapharyngeal abscess, mastoiditis, meningitis, and brain abscess. Button batteries are particularly dangerous due to electrical injury and pressure necrosis, often causing rapid tissue destruction.
Etiology
Children commonly insert beads, stones, paper, seeds, popcorn kernels, beans, toys, and button batteries. Adults more often present with cotton-swab tips, earplugs, insects (cockroaches most common in the US), or concealed illicit drugs.
Diagnosis Signs And Symptoms
Symptoms include unilateral ear pain, fullness, decreased hearing, crying in infants, buzzing or movement sensation with live insects, nausea, dizziness, ipsilateral tearing, itching, bleeding, or purulent discharge.
History should include prior removal attempts and possible trauma.
Physical examination requires careful otoscopy before and after removal to identify the object type, assess swelling risk, evaluate for otitis externa, retained fragments, or tympanic membrane perforation. A bilateral ear exam and inspection of nostrils are essential, especially in children and psychiatric patients. Concerning findings such as vertigo, nystagmus, hearing loss, facial nerve weakness, or severe pain warrant ENT consultation.
Essential Workup
A careful otoscopic examination is the cornerstone. Identify the foreign body and minimize patient discomfort before attempting removal.
Diagnosis Tests And Interpretation
Laboratory studies are not indicated. CT imaging is reserved for suspected infectious, erosive, or intracranial complications. Otomicroscopy may assist when standard techniques fail.
Differential Diagnosis
Cerumen impaction, otitis externa, canal hematoma, granuloma, trauma, tympanic membrane perforation, residual inflammation after self-removal, and tumors.
Treatment
Prehospital care for suspected live insects includes instillation of warm lidocaine or mineral oil to immobilize the insect; field removal attempts are discouraged.
In the emergency department, ensure adequate lighting, proper head immobilization, and analgesia. Lidocaine (1–2%) may be instilled topically or injected into the canal walls. Procedural sedation is recommended for children or uncooperative adults and should be used early to prevent traumatic repeated attempts.
Removal techniques depend on object type: irrigation for non–button battery objects; forceps, hooks, suction, Fogarty catheter, or cyanoacrylate glue for selected cases; acetone for Styrofoam or adhesive materials. Vegetable matter should not be irrigated. Button batteries must never be irrigated and require urgent removal. Live insects should be killed first with lidocaine, alcohol, or mineral oil before extraction. Sharp objects and complicated cases require ENT referral.
Medication
Analgesia or sedation may include fentanyl, ketamine, or midazolam. Topical antibiotic-steroid drops are indicated if canal abrasion or infection is suspected. Oral antibiotics are reserved for tympanic membrane perforation or secondary infection.
Follow Up Disposition
Admission is required for button batteries that cannot be removed.
Discharge is appropriate once the foreign body is removed or if a nonhazardous object cannot be safely removed in the ED.
ENT referral is indicated for failed removal, complications, immunocompromised patients, or significant trauma.
Follow Up Recommendations
Advise patients not to insert objects into the ear. Provide short-term analgesia after traumatic removal. Treat otitis externa with topical antimicrobials. Avoid water submersion if trauma or infection is present and arrange ENT follow-up when indicated.
Key Practice Insights And Avoidable Errors
Early use of procedural sedation improves success and reduces complications. Never irrigate an ear containing a button battery, as this can rapidly worsen tissue necrosis.
- Published on
Emergency And Acute Medicine – Shaft and Distal Forearm Fractures
Basics Description
Forearm shaft fractures may involve one or both bones and are frequently displaced due to muscular contraction. These injuries may be associated with joint dislocations, including Galeazzi fractures, which involve a distal radius fracture with distal radioulnar joint dislocation, and Monteggia fractures, which involve a proximal ulna fracture with radial head dislocation.
Distal forearm fractures include several classic patterns. Colles fractures result from hyperextension with dorsal displacement of the distal radius fragment and are often associated with ulnar styloid injury. Smith fractures occur with hyperflexion and result in volar displacement. Barton fractures are intra-articular fractures of the dorsal rim of the distal radius and may involve carpal dislocation. Hutchinson fractures involve the radial styloid.
In children, shaft fractures commonly present as torus fractures, greenstick fractures, or plastic deformities. Distal fractures in pediatric patients frequently involve Salter–Harris growth plate injuries.
Etiology
Common mechanisms include direct blows to the forearm, longitudinal compression such as falls on an outstretched hand, horizontal force, and excessive pronation, supination, hyperextension, or hyperflexion.
Diagnosis Signs And Symptoms
Patients typically present with pain, deformity, swelling, and limited function. History should include mechanism of injury, hand dominance, occupational or repetitive stress factors, and prior bone disease or fractures.
Physical examination focuses on deformity, tenderness, crepitus, edema, ecchymosis, joint effusions at the elbow or wrist, abnormal mobility, and careful assessment of neurovascular status. Findings concerning for compartment syndrome require urgent attention.
Essential Workup
Suspected forearm fractures require anteroposterior and lateral radiographs that include the wrist, forearm, and elbow to evaluate joints above and below the injury.
Diagnosis Tests And Interpretation
Imaging may include CT for complex or intra-articular fractures. Compartment pressure measurement is indicated when compartment syndrome is suspected. Laboratory studies are generally reserved for preoperative evaluation.
Differential Diagnosis
Consider muscle or ligament injury, elbow or wrist dislocations, contusions or hematomas, infection, tumors, osteomyelitis, vascular or neurologic injury, arthritis, and in children, normal growth plates or nutrient vessels that may mimic fractures.
Treatment
Prehospital care includes elevation, splinting, and immobilization of the elbow and wrist. Open fractures should be covered with sterile dressings and not reduced in the field.
In the emergency department, nondisplaced shaft fractures are treated with long-arm splinting and orthopedic referral. Displaced shaft fractures often require orthopedic consultation and operative fixation.
Nondisplaced distal fractures are managed with sugar-tong or anteroposterior splints and referral. Simple Colles or Smith fractures may be reduced in the emergency department and splinted, while complicated patterns require orthopedic consultation. Barton and Hutchinson fractures are splinted and referred, with operative management as needed.
Open fractures require antibiotics, tetanus prophylaxis, splinting, and immediate orthopedic consultation. Any fracture associated with neurovascular compromise or compartment syndrome requires urgent specialist evaluation.
In pediatric patients, minimally angulated torus or greenstick fractures may be splinted and referred, while plastic deformities and Salter–Harris fractures require orthopedic consultation.
Medication
Pain control is achieved with acetaminophen, NSAIDs, or opioids as appropriate. Open fractures require parenteral antibiotics such as first-generation cephalosporins, with additional coverage for contaminated wounds. Tetanus prophylaxis should be updated as indicated.
Follow Up Disposition
Admission is required for open fractures, compartment syndrome, neurovascular compromise, fractures requiring immediate surgery, or suspected nonaccidental trauma.
Discharge is appropriate after adequate reduction and immobilization, confirmation of intact neurovascular status, effective pain control, and ensured orthopedic follow-up with clear splint and cast care instructions.
Clinical Insights And Common Pitfalls
Always evaluate for a second fracture or associated joint dislocation. Reassess neurovascular status frequently and maintain a high index of suspicion for evolving compartment syndrome.
Basics Description
Forearm shaft fractures may involve one or both bones and are frequently displaced due to muscular contraction. These injuries may be associated with joint dislocations, including Galeazzi fractures, which involve a distal radius fracture with distal radioulnar joint dislocation, and Monteggia fractures, which involve a proximal ulna fracture with radial head dislocation.
Distal forearm fractures include several classic patterns. Colles fractures result from hyperextension with dorsal displacement of the distal radius fragment and are often associated with ulnar styloid injury. Smith fractures occur with hyperflexion and result in volar displacement. Barton fractures are intra-articular fractures of the dorsal rim of the distal radius and may involve carpal dislocation. Hutchinson fractures involve the radial styloid.
In children, shaft fractures commonly present as torus fractures, greenstick fractures, or plastic deformities. Distal fractures in pediatric patients frequently involve Salter–Harris growth plate injuries.
Etiology
Common mechanisms include direct blows to the forearm, longitudinal compression such as falls on an outstretched hand, horizontal force, and excessive pronation, supination, hyperextension, or hyperflexion.
Diagnosis Signs And Symptoms
Patients typically present with pain, deformity, swelling, and limited function. History should include mechanism of injury, hand dominance, occupational or repetitive stress factors, and prior bone disease or fractures.
Physical examination focuses on deformity, tenderness, crepitus, edema, ecchymosis, joint effusions at the elbow or wrist, abnormal mobility, and careful assessment of neurovascular status. Findings concerning for compartment syndrome require urgent attention.
Essential Workup
Suspected forearm fractures require anteroposterior and lateral radiographs that include the wrist, forearm, and elbow to evaluate joints above and below the injury.
Diagnosis Tests And Interpretation
Imaging may include CT for complex or intra-articular fractures. Compartment pressure measurement is indicated when compartment syndrome is suspected. Laboratory studies are generally reserved for preoperative evaluation.
Differential Diagnosis
Consider muscle or ligament injury, elbow or wrist dislocations, contusions or hematomas, infection, tumors, osteomyelitis, vascular or neurologic injury, arthritis, and in children, normal growth plates or nutrient vessels that may mimic fractures.
Treatment
Prehospital care includes elevation, splinting, and immobilization of the elbow and wrist. Open fractures should be covered with sterile dressings and not reduced in the field.
In the emergency department, nondisplaced shaft fractures are treated with long-arm splinting and orthopedic referral. Displaced shaft fractures often require orthopedic consultation and operative fixation.
Nondisplaced distal fractures are managed with sugar-tong or anteroposterior splints and referral. Simple Colles or Smith fractures may be reduced in the emergency department and splinted, while complicated patterns require orthopedic consultation. Barton and Hutchinson fractures are splinted and referred, with operative management as needed.
Open fractures require antibiotics, tetanus prophylaxis, splinting, and immediate orthopedic consultation. Any fracture associated with neurovascular compromise or compartment syndrome requires urgent specialist evaluation.
In pediatric patients, minimally angulated torus or greenstick fractures may be splinted and referred, while plastic deformities and Salter–Harris fractures require orthopedic consultation.
Medication
Pain control is achieved with acetaminophen, NSAIDs, or opioids as appropriate. Open fractures require parenteral antibiotics such as first-generation cephalosporins, with additional coverage for contaminated wounds. Tetanus prophylaxis should be updated as indicated.
Follow Up Disposition
Admission is required for open fractures, compartment syndrome, neurovascular compromise, fractures requiring immediate surgery, or suspected nonaccidental trauma.
Discharge is appropriate after adequate reduction and immobilization, confirmation of intact neurovascular status, effective pain control, and ensured orthopedic follow-up with clear splint and cast care instructions.
Clinical Insights And Common Pitfalls
Always evaluate for a second fracture or associated joint dislocation. Reassess neurovascular status frequently and maintain a high index of suspicion for evolving compartment syndrome.


- Published on
Emergency And Acute Medicine - Edema
Core overview
Edema is the visible accumulation of fluid within the interstitial (extravascular) space caused by disruption of normal hydrostatic and oncotic pressure balance. Mechanisms include increased venous or capillary hydrostatic pressure, reduced plasma oncotic pressure, increased interstitial oncotic pressure, increased capillary permeability, impaired lymphatic drainage, or a combination of these factors. Edema may be generalized, as seen in conditions such as heart failure or nephrotic syndrome, or localized, as in deep vein thrombosis. Elevated venous pressure or reduced oncotic pressure typically produces pitting edema, whereas leakage of protein-rich fluid results in nonpitting edema. Some conditions, such as idiopathic (cyclic) edema, do not clearly follow Starling forces and are often worsened by heat, occur more commonly in women, and are not consistently linked to the menstrual cycle.
Etiology and contributing causes
Generalized edema is most commonly associated with heart failure, cor pulmonale, cardiomyopathies, constrictive pericarditis, pulmonary hypertension related to sleep apnea or COPD, acute glomerulonephritis, renal failure, cirrhosis, nephrotic syndrome, protein-losing enteropathy, malnutrition, pregnancy, myxedema, and idiopathic edema. Numerous medications can contribute, often through salt and water retention, including corticosteroids, estrogens, NSAIDs, antihypertensives (particularly vasodilators), lithium, cyclosporine, insulin, thiazolidinediones, growth hormone, interleukin-2, MAO inhibitors, pramipexole, docetaxel, and minoxidil, as well as abrupt withdrawal of diuretics.
Localized edema may result from deep vein thrombosis, venous insufficiency, thrombophlebitis, chronic lymphatic obstruction, cellulitis, Baker cysts, vasculitis, angioedema, trauma, burns, radiation injury, surgery disrupting lymphatics, malignancy, filariasis, or neurologic conditions such as hemiplegia and reflex sympathetic dystrophy.
Clinical presentation and symptoms
Patients often report rapid weight gain, localized discomfort, swelling, and tenderness. Pitting edema suggests increased hydrostatic pressure or decreased oncotic pressure, while nonpitting edema implies protein-rich fluid accumulation. In generalized edema (anasarca), swelling is most evident in dependent areas such as the feet, sacrum, and lower extremities, and may involve facial or periorbital tissues, particularly in the morning.
Associated findings depend on the underlying cause. Cardiac causes may present with dyspnea, orthopnea, paroxysmal nocturnal dyspnea, jugular venous distention, rales, or an S3 gallop. Renal disease may cause anorexia, periorbital puffiness, frothy urine, oliguria, dark urine, hematuria, and hypertension. Hepatic disease may be accompanied by jaundice, spider angiomas, palmar erythema, gynecomastia, testicular atrophy, and ascites. Myxedema produces nonpitting pretibial edema, dry waxy skin, fatigue, cold intolerance, constipation, weight gain, and delayed reflex relaxation. Idiopathic edema often fluctuates diurnally. Localized edema may be associated with erythema, warmth, fever, pruritus, hives, trauma, or signs of venous disease such as skin discoloration and ulceration.
Special pregnancy considerations
Edema is common during pregnancy due to hormonally mediated fluid retention. Dependent edema is typical in late pregnancy from impaired venous return. Swelling of the hands and face should raise concern for preeclampsia. Diuretics are generally contraindicated.
Essential evaluation approach
Diagnostic testing should be guided by the suspected underlying cause based on history and physical examination.
Diagnostic testing and interpretation
When a cardiac cause is suspected, B-type natriuretic peptide testing, ECG, and chest radiography are useful. Suspected deep vein thrombosis may be evaluated with d-dimer testing in low-risk patients and confirmed with duplex ultrasonography or venography. Renal evaluation includes serum electrolytes, BUN, creatinine, urinalysis, urine protein assessment, and lipid studies. Hepatic causes warrant liver function tests, serum albumin, and coagulation studies. Thyroid function testing is indicated when myxedema is suspected. Abdominal or pelvic CT imaging is considered if malignancy is a concern.
Conditions to differentiate from
Important alternative diagnoses include cellulitis, contact dermatitis, diffuse subcutaneous infiltrative disorders, lymphedema, and obesity.
Initial stabilization and emergency management
Management focuses on treating the underlying cause. Diuretics are commonly used for generalized edema but are rarely required emergently and may be harmful in certain conditions such as cirrhosis with ascites, where rapid fluid shifts can precipitate hepatorenal syndrome.
Pharmacologic options
Common agents include loop diuretics such as furosemide, thiazide diuretics, potassium-sparing diuretics such as spironolactone or amiloride, and adjunctive medications tailored to the underlying condition.
Disposition and follow-up planning
Admission decisions depend on the etiology and severity of illness. Indications include cardiopulmonary compromise, hypoxia, inability to ambulate safely, or lack of adequate home support. Stable patients may be discharged with instructions to reduce sodium intake, elevate affected limbs, and use compression stockings when appropriate.
Referral considerations
Patients over 45 years of age with chronic edema or features suggesting cardiopulmonary disease require outpatient cardiac evaluation. Pulmonary hypertension of unclear cause warrants referral for sleep apnea evaluation. A negative initial ultrasound in a high-risk patient for DVT necessitates repeat imaging within 5–7 days.
Ongoing care recommendations
Chronic edema should be managed in coordination with primary care for continued evaluation and treatment adjustment.
Key clinical insights and common errors
Always classify edema as generalized or localized and as pitting or nonpitting. Pitting edema reflects protein-poor fluid accumulation from increased hydrostatic pressure or reduced oncotic pressure, whereas nonpitting edema reflects protein-rich fluid from lymphatic obstruction or increased permeability. Bilateral or generalized edema suggests systemic disease, while acute unilateral leg swelling mandates evaluation for deep vein thrombosis. In pregnancy, edema involving the face or hands should prompt consideration of preeclampsia.
Core overview
Edema is the visible accumulation of fluid within the interstitial (extravascular) space caused by disruption of normal hydrostatic and oncotic pressure balance. Mechanisms include increased venous or capillary hydrostatic pressure, reduced plasma oncotic pressure, increased interstitial oncotic pressure, increased capillary permeability, impaired lymphatic drainage, or a combination of these factors. Edema may be generalized, as seen in conditions such as heart failure or nephrotic syndrome, or localized, as in deep vein thrombosis. Elevated venous pressure or reduced oncotic pressure typically produces pitting edema, whereas leakage of protein-rich fluid results in nonpitting edema. Some conditions, such as idiopathic (cyclic) edema, do not clearly follow Starling forces and are often worsened by heat, occur more commonly in women, and are not consistently linked to the menstrual cycle.
Etiology and contributing causes
Generalized edema is most commonly associated with heart failure, cor pulmonale, cardiomyopathies, constrictive pericarditis, pulmonary hypertension related to sleep apnea or COPD, acute glomerulonephritis, renal failure, cirrhosis, nephrotic syndrome, protein-losing enteropathy, malnutrition, pregnancy, myxedema, and idiopathic edema. Numerous medications can contribute, often through salt and water retention, including corticosteroids, estrogens, NSAIDs, antihypertensives (particularly vasodilators), lithium, cyclosporine, insulin, thiazolidinediones, growth hormone, interleukin-2, MAO inhibitors, pramipexole, docetaxel, and minoxidil, as well as abrupt withdrawal of diuretics.
Localized edema may result from deep vein thrombosis, venous insufficiency, thrombophlebitis, chronic lymphatic obstruction, cellulitis, Baker cysts, vasculitis, angioedema, trauma, burns, radiation injury, surgery disrupting lymphatics, malignancy, filariasis, or neurologic conditions such as hemiplegia and reflex sympathetic dystrophy.
Clinical presentation and symptoms
Patients often report rapid weight gain, localized discomfort, swelling, and tenderness. Pitting edema suggests increased hydrostatic pressure or decreased oncotic pressure, while nonpitting edema implies protein-rich fluid accumulation. In generalized edema (anasarca), swelling is most evident in dependent areas such as the feet, sacrum, and lower extremities, and may involve facial or periorbital tissues, particularly in the morning.
Associated findings depend on the underlying cause. Cardiac causes may present with dyspnea, orthopnea, paroxysmal nocturnal dyspnea, jugular venous distention, rales, or an S3 gallop. Renal disease may cause anorexia, periorbital puffiness, frothy urine, oliguria, dark urine, hematuria, and hypertension. Hepatic disease may be accompanied by jaundice, spider angiomas, palmar erythema, gynecomastia, testicular atrophy, and ascites. Myxedema produces nonpitting pretibial edema, dry waxy skin, fatigue, cold intolerance, constipation, weight gain, and delayed reflex relaxation. Idiopathic edema often fluctuates diurnally. Localized edema may be associated with erythema, warmth, fever, pruritus, hives, trauma, or signs of venous disease such as skin discoloration and ulceration.
Special pregnancy considerations
Edema is common during pregnancy due to hormonally mediated fluid retention. Dependent edema is typical in late pregnancy from impaired venous return. Swelling of the hands and face should raise concern for preeclampsia. Diuretics are generally contraindicated.
Essential evaluation approach
Diagnostic testing should be guided by the suspected underlying cause based on history and physical examination.
Diagnostic testing and interpretation
When a cardiac cause is suspected, B-type natriuretic peptide testing, ECG, and chest radiography are useful. Suspected deep vein thrombosis may be evaluated with d-dimer testing in low-risk patients and confirmed with duplex ultrasonography or venography. Renal evaluation includes serum electrolytes, BUN, creatinine, urinalysis, urine protein assessment, and lipid studies. Hepatic causes warrant liver function tests, serum albumin, and coagulation studies. Thyroid function testing is indicated when myxedema is suspected. Abdominal or pelvic CT imaging is considered if malignancy is a concern.
Conditions to differentiate from
Important alternative diagnoses include cellulitis, contact dermatitis, diffuse subcutaneous infiltrative disorders, lymphedema, and obesity.
Initial stabilization and emergency management
Management focuses on treating the underlying cause. Diuretics are commonly used for generalized edema but are rarely required emergently and may be harmful in certain conditions such as cirrhosis with ascites, where rapid fluid shifts can precipitate hepatorenal syndrome.
Pharmacologic options
Common agents include loop diuretics such as furosemide, thiazide diuretics, potassium-sparing diuretics such as spironolactone or amiloride, and adjunctive medications tailored to the underlying condition.
Disposition and follow-up planning
Admission decisions depend on the etiology and severity of illness. Indications include cardiopulmonary compromise, hypoxia, inability to ambulate safely, or lack of adequate home support. Stable patients may be discharged with instructions to reduce sodium intake, elevate affected limbs, and use compression stockings when appropriate.
Referral considerations
Patients over 45 years of age with chronic edema or features suggesting cardiopulmonary disease require outpatient cardiac evaluation. Pulmonary hypertension of unclear cause warrants referral for sleep apnea evaluation. A negative initial ultrasound in a high-risk patient for DVT necessitates repeat imaging within 5–7 days.
Ongoing care recommendations
Chronic edema should be managed in coordination with primary care for continued evaluation and treatment adjustment.
Key clinical insights and common errors
Always classify edema as generalized or localized and as pitting or nonpitting. Pitting edema reflects protein-poor fluid accumulation from increased hydrostatic pressure or reduced oncotic pressure, whereas nonpitting edema reflects protein-rich fluid from lymphatic obstruction or increased permeability. Bilateral or generalized edema suggests systemic disease, while acute unilateral leg swelling mandates evaluation for deep vein thrombosis. In pregnancy, edema involving the face or hands should prompt consideration of preeclampsia.

- Published on
Emergency And Acute Medicine - Eczema / Atopic Dermatitis
Core Overview
Atopic dermatitis is the most frequent cause of eczema, and the terms are commonly used interchangeably. It is strongly associated with other atopic conditions, including asthma and allergic rhinitis. The term eczema refers to spongiosis, a process in which microscopic vesicles form within the epidermis and subsequently rupture, producing erythema, edema, crusting, and oozing. Intense pruritus is a hallmark feature. Repeated rubbing and scratching lead to skin breakdown with weeping and crust formation, while chronic disease results in epidermal hyperplasia and hyperkeratosis. Approximately 90% of patients are colonized with Staphylococcus aureus, predisposing them to recurrent secondary infections.
Predisposing Factors
Genetic susceptibility plays a major role, particularly a family history of atopic disease such as asthma or allergic rhinitis. Mutations in the filaggrin protein, a key component of the epidermal barrier, are strongly associated with disease development.
Underlying Mechanism
Atopic dermatitis arises from impaired epidermal barrier function, allowing allergens and irritants to penetrate the skin and trigger immune-mediated inflammation.
Clinical Features
Patients typically report a pruritic rash and a personal or family history of atopy. Diagnostic criteria emphasize pruritus plus additional features such as flexural involvement, history of asthma or allergic rhinitis, chronically dry skin, onset before two years of age, and visible flexural dermatitis. Other commonly reported findings include recurrent skin infections, itching with sweating, intolerance to wool or lipid solvents, and symptom exacerbation during periods of stress.
Physical Examination Findings
Dermatitis is commonly located in areas of friction or movement, including flexural surfaces, hands, and feet. Skin findings reflect barrier disruption with dryness, weeping, oozing, and crusting, along with inflammatory changes such as maculopapular erythema and edema. Chronic scratching leads to excoriations, fissuring, lichenification, and hyperkeratosis. Additional characteristic signs may include ichthyosis, palmar hyperlinearity, keratosis pilaris, hand or foot dermatitis, nipple involvement, cheilitis, Dennie–Morgan infraorbital folds, periocular darkening, facial pallor or erythema, pityriasis alba, perifollicular accentuation, and white dermographism or delayed blanching.
Special Pediatric Considerations
Most cases begin early in life, with approximately 70% presenting within the first five years. Only a small proportion begin in adulthood. A significant percentage of affected children later develop asthma or allergic rhinitis. In infants, lesions classically involve the face, scalp, and extensor surfaces.
Essential Evaluation
Diagnosis is primarily clinical and based on history and physical examination.
Diagnostic Testing Considerations
Laboratory studies are generally unnecessary in the emergency setting. Although IgE levels are often elevated, routine testing is not required. Specialized testing such as allergen-specific IgE assays or patch testing is typically reserved for outpatient evaluation, particularly when allergic contact dermatitis is suspected.
Conditions To Differentiate From
Important alternative diagnoses include seborrheic dermatitis, lichen simplex chronicus, allergic or irritant contact dermatitis, psoriasis, dyshidrotic eczema, ichthyosis, and scabies.
Emergency Department Management
Mild disease or involvement of the head and neck is treated with low-potency topical corticosteroids such as hydrocortisone and regular emollient application. Moderate to severe disease affecting the trunk or extremities may require mid- to high-potency topical corticosteroids. Severe head and neck involvement is best managed with topical calcineurin inhibitors such as tacrolimus or pimecrolimus. First-generation antihistamines may be used to reduce pruritus, though their efficacy is limited. Supportive measures include avoiding excessive bathing, using tepid water and mild soaps, and applying emollients frequently. Suspected bacterial superinfection should prompt treatment with appropriate antibiotics, with consideration for methicillin-resistant Staphylococcus aureus.
Pharmacologic Options
Emollients such as petrolatum-based ointments are foundational therapy. Topical corticosteroids are selected based on disease severity and location. Calcineurin inhibitors are useful alternatives for sensitive areas such as the face. Antihistamines may aid symptom control. Antibiotics are indicated when secondary infection is present.
Disposition And Referral Planning
Patients with refractory or severe disease should be referred for dermatology follow-up.
Ongoing Care Guidance
Patients should be counseled regarding potential adverse effects of therapy. Prolonged use of high-potency topical corticosteroids can lead to skin atrophy. Calcineurin inhibitors may cause transient stinging during initial use, and long-term safety considerations should be discussed.
Key Clinical Insights And Common Errors
Always consider secondary bacterial infection, as colonization with S. aureus is common. Use topical calcineurin inhibitors preferentially for moderate to severe disease of the face and neck. Lotions may worsen dryness due to low lipid content; thick creams or ointments are preferred. Avoid using medium- or high-potency topical corticosteroids on the face or eyelids to prevent complications.
Core Overview
Atopic dermatitis is the most frequent cause of eczema, and the terms are commonly used interchangeably. It is strongly associated with other atopic conditions, including asthma and allergic rhinitis. The term eczema refers to spongiosis, a process in which microscopic vesicles form within the epidermis and subsequently rupture, producing erythema, edema, crusting, and oozing. Intense pruritus is a hallmark feature. Repeated rubbing and scratching lead to skin breakdown with weeping and crust formation, while chronic disease results in epidermal hyperplasia and hyperkeratosis. Approximately 90% of patients are colonized with Staphylococcus aureus, predisposing them to recurrent secondary infections.
Predisposing Factors
Genetic susceptibility plays a major role, particularly a family history of atopic disease such as asthma or allergic rhinitis. Mutations in the filaggrin protein, a key component of the epidermal barrier, are strongly associated with disease development.
Underlying Mechanism
Atopic dermatitis arises from impaired epidermal barrier function, allowing allergens and irritants to penetrate the skin and trigger immune-mediated inflammation.
Clinical Features
Patients typically report a pruritic rash and a personal or family history of atopy. Diagnostic criteria emphasize pruritus plus additional features such as flexural involvement, history of asthma or allergic rhinitis, chronically dry skin, onset before two years of age, and visible flexural dermatitis. Other commonly reported findings include recurrent skin infections, itching with sweating, intolerance to wool or lipid solvents, and symptom exacerbation during periods of stress.
Physical Examination Findings
Dermatitis is commonly located in areas of friction or movement, including flexural surfaces, hands, and feet. Skin findings reflect barrier disruption with dryness, weeping, oozing, and crusting, along with inflammatory changes such as maculopapular erythema and edema. Chronic scratching leads to excoriations, fissuring, lichenification, and hyperkeratosis. Additional characteristic signs may include ichthyosis, palmar hyperlinearity, keratosis pilaris, hand or foot dermatitis, nipple involvement, cheilitis, Dennie–Morgan infraorbital folds, periocular darkening, facial pallor or erythema, pityriasis alba, perifollicular accentuation, and white dermographism or delayed blanching.
Special Pediatric Considerations
Most cases begin early in life, with approximately 70% presenting within the first five years. Only a small proportion begin in adulthood. A significant percentage of affected children later develop asthma or allergic rhinitis. In infants, lesions classically involve the face, scalp, and extensor surfaces.
Essential Evaluation
Diagnosis is primarily clinical and based on history and physical examination.
Diagnostic Testing Considerations
Laboratory studies are generally unnecessary in the emergency setting. Although IgE levels are often elevated, routine testing is not required. Specialized testing such as allergen-specific IgE assays or patch testing is typically reserved for outpatient evaluation, particularly when allergic contact dermatitis is suspected.
Conditions To Differentiate From
Important alternative diagnoses include seborrheic dermatitis, lichen simplex chronicus, allergic or irritant contact dermatitis, psoriasis, dyshidrotic eczema, ichthyosis, and scabies.
Emergency Department Management
Mild disease or involvement of the head and neck is treated with low-potency topical corticosteroids such as hydrocortisone and regular emollient application. Moderate to severe disease affecting the trunk or extremities may require mid- to high-potency topical corticosteroids. Severe head and neck involvement is best managed with topical calcineurin inhibitors such as tacrolimus or pimecrolimus. First-generation antihistamines may be used to reduce pruritus, though their efficacy is limited. Supportive measures include avoiding excessive bathing, using tepid water and mild soaps, and applying emollients frequently. Suspected bacterial superinfection should prompt treatment with appropriate antibiotics, with consideration for methicillin-resistant Staphylococcus aureus.
Pharmacologic Options
Emollients such as petrolatum-based ointments are foundational therapy. Topical corticosteroids are selected based on disease severity and location. Calcineurin inhibitors are useful alternatives for sensitive areas such as the face. Antihistamines may aid symptom control. Antibiotics are indicated when secondary infection is present.
Disposition And Referral Planning
Patients with refractory or severe disease should be referred for dermatology follow-up.
Ongoing Care Guidance
Patients should be counseled regarding potential adverse effects of therapy. Prolonged use of high-potency topical corticosteroids can lead to skin atrophy. Calcineurin inhibitors may cause transient stinging during initial use, and long-term safety considerations should be discussed.
Key Clinical Insights And Common Errors
Always consider secondary bacterial infection, as colonization with S. aureus is common. Use topical calcineurin inhibitors preferentially for moderate to severe disease of the face and neck. Lotions may worsen dryness due to low lipid content; thick creams or ointments are preferred. Avoid using medium- or high-potency topical corticosteroids on the face or eyelids to prevent complications.

- Published on
Emergency And Acute Medicine - Ectopic Pregnancy
Core Overview
Ectopic pregnancy occurs when a fertilized ovum implants outside the uterine cavity, most commonly within the fallopian tube, accounting for approximately 93–97% of cases. Less common sites include abdominal and peritoneal locations, which are associated with higher morbidity due to diagnostic difficulty and increased bleeding risk. Ectopic pregnancy occurs in about 2–2.6% of all pregnancies and is responsible for roughly 6% of maternal deaths, making it the leading cause of pregnancy-related mortality in the first trimester. Despite this, approximately 60% of women with a prior ectopic pregnancy are able to achieve a subsequent normal intrauterine pregnancy.
Predisposing Factors And Causes
Risk factors include maternal age over 35 years, African American race, prior fallopian tube damage from pelvic inflammatory disease, previous tubal surgery or ectopic pregnancy, intrauterine device use (with 25–50% of pregnancies occurring with an IUD being ectopic), diethylstilbestrol exposure, in vitro fertilization, and current tobacco use. Importantly, more than half of affected women have no identifiable risk factors.
Clinical Manifestations
The classic triad of amenorrhea, vaginal bleeding, and abdominal pain is present in only a minority of patients. Amenorrhea occurs in most cases, abdominal pain—often unilateral—is very common, and abnormal vaginal bleeding is frequent. Some patients report symptoms of early pregnancy, while others may present with orthostatic hypotension, dizziness, or syncope. Physical findings may include abdominal tenderness, adnexal tenderness or mass, and cervical motion tenderness.
Focused History And Examination
History should address the last menstrual period, gestational and parity history, bleeding characteristics, pain location and severity, prior pelvic surgery or ectopic pregnancy, IUD use, and fertility treatments. Examination should assess for peritoneal signs and include a pelvic examination evaluating uterine size, adnexal masses or tenderness, cervical motion tenderness, and whether the cervical os is open or closed.
Essential Initial Evaluation
All women of reproductive age presenting with abdominal pain or vaginal bleeding must undergo pregnancy testing, regardless of contraception history or prior sterilization. A positive test requires quantitative serum β-hCG measurement. In unstable patients, establish two large-bore IV lines, obtain type and cross-match with hemoglobin and hematocrit, perform bedside ultrasound if available, and urgently consult obstetrics/gynecology. In stable patients, obtain hemoglobin and hematocrit, blood type and Rh status, and transvaginal ultrasound.
Diagnostic Studies And Interpretation
Urine pregnancy tests typically detect β-hCG levels of 25–50 mIU/L, while serum testing detects levels as low as 25 mIU/L. In normal early pregnancy, β-hCG levels double approximately every 48 hours; slower rises suggest ectopic pregnancy. Transvaginal ultrasound can identify a gestational sac at around 5 weeks and cardiac activity by approximately 6.5 weeks. The absence of an intrauterine pregnancy when β-hCG exceeds the discriminatory zone (generally 1,500–3,000 mIU/mL) strongly suggests ectopic pregnancy. Complex adnexal masses with pelvic free fluid are highly predictive when present. Culdocentesis may be considered if ultrasound is unavailable.
Alternative Diagnoses To Consider
Differential diagnoses include spontaneous or threatened abortion, cervicitis, trauma, ruptured ovarian or corpus luteum cyst, ovarian torsion, urinary tract infection, nephrolithiasis, appendicitis, pelvic inflammatory disease, and heterotopic pregnancy, particularly in patients undergoing fertility treatments.
Prehospital And Early Management Considerations
Any woman of childbearing age presenting in shock should be presumed to have a ruptured ectopic pregnancy until proven otherwise. Early recognition and rapid transport are critical.
Stabilization Priorities
Unstable patients require airway management, aggressive resuscitation with oxygen and IV fluids, blood transfusion as needed, immediate gynecology consultation, and urgent operative management. Stable patients with confirmed ectopic pregnancy require gynecologic evaluation to determine suitability for medical versus surgical treatment. Patients with pregnancy of unknown location require close follow-up and serial β-hCG testing.
Emergency Department Interventions
Methotrexate therapy may be considered in reliable, stable patients with unruptured ectopic pregnancies, small ectopic size, and lower β-hCG levels, under obstetric supervision. Contraindications include breastfeeding, immunodeficiency, hematologic disorders, significant anemia, hepatic or renal dysfunction, peptic ulcer disease, active pulmonary disease, and alcoholism. Serial β-hCG monitoring is mandatory, and patients must be counseled regarding expected side effects and warning signs of rupture.
Pharmacologic Therapy
Methotrexate is typically administered as a single dose of 50 mg/m² intramuscularly or intravenously, with repeat dosing guided by β-hCG response. Rh-negative women should receive Rho(D) immune globulin based on gestational age.
Disposition And Monitoring Decisions
Admission is required for hemodynamically unstable patients and those with confirmed ectopic pregnancy who cannot ensure close follow-up. Outpatient management may be appropriate for stable, reliable patients with coordinated obstetric follow-up. Clear return precautions must be provided, including instructions to seek immediate care for worsening abdominal pain, increased bleeding, dizziness, or syncope.
Follow-Up Planning
All patients with positive pregnancy tests and no confirmed intrauterine pregnancy must have close obstetric follow-up with serial β-hCG testing and repeat ultrasound as indicated.
Key Clinical Insights And Common Errors
Always obtain a pregnancy test in women of childbearing age. Combine quantitative β-hCG testing with transvaginal ultrasound in any pregnant patient with abdominal pain or vaginal bleeding. Maintain awareness of heterotopic pregnancy, especially after assisted reproduction. Ensure reliable follow-up and clear return precautions for any patient discharged during evaluation for ectopic pregnancy.
Core Overview
Ectopic pregnancy occurs when a fertilized ovum implants outside the uterine cavity, most commonly within the fallopian tube, accounting for approximately 93–97% of cases. Less common sites include abdominal and peritoneal locations, which are associated with higher morbidity due to diagnostic difficulty and increased bleeding risk. Ectopic pregnancy occurs in about 2–2.6% of all pregnancies and is responsible for roughly 6% of maternal deaths, making it the leading cause of pregnancy-related mortality in the first trimester. Despite this, approximately 60% of women with a prior ectopic pregnancy are able to achieve a subsequent normal intrauterine pregnancy.
Predisposing Factors And Causes
Risk factors include maternal age over 35 years, African American race, prior fallopian tube damage from pelvic inflammatory disease, previous tubal surgery or ectopic pregnancy, intrauterine device use (with 25–50% of pregnancies occurring with an IUD being ectopic), diethylstilbestrol exposure, in vitro fertilization, and current tobacco use. Importantly, more than half of affected women have no identifiable risk factors.
Clinical Manifestations
The classic triad of amenorrhea, vaginal bleeding, and abdominal pain is present in only a minority of patients. Amenorrhea occurs in most cases, abdominal pain—often unilateral—is very common, and abnormal vaginal bleeding is frequent. Some patients report symptoms of early pregnancy, while others may present with orthostatic hypotension, dizziness, or syncope. Physical findings may include abdominal tenderness, adnexal tenderness or mass, and cervical motion tenderness.
Focused History And Examination
History should address the last menstrual period, gestational and parity history, bleeding characteristics, pain location and severity, prior pelvic surgery or ectopic pregnancy, IUD use, and fertility treatments. Examination should assess for peritoneal signs and include a pelvic examination evaluating uterine size, adnexal masses or tenderness, cervical motion tenderness, and whether the cervical os is open or closed.
Essential Initial Evaluation
All women of reproductive age presenting with abdominal pain or vaginal bleeding must undergo pregnancy testing, regardless of contraception history or prior sterilization. A positive test requires quantitative serum β-hCG measurement. In unstable patients, establish two large-bore IV lines, obtain type and cross-match with hemoglobin and hematocrit, perform bedside ultrasound if available, and urgently consult obstetrics/gynecology. In stable patients, obtain hemoglobin and hematocrit, blood type and Rh status, and transvaginal ultrasound.
Diagnostic Studies And Interpretation
Urine pregnancy tests typically detect β-hCG levels of 25–50 mIU/L, while serum testing detects levels as low as 25 mIU/L. In normal early pregnancy, β-hCG levels double approximately every 48 hours; slower rises suggest ectopic pregnancy. Transvaginal ultrasound can identify a gestational sac at around 5 weeks and cardiac activity by approximately 6.5 weeks. The absence of an intrauterine pregnancy when β-hCG exceeds the discriminatory zone (generally 1,500–3,000 mIU/mL) strongly suggests ectopic pregnancy. Complex adnexal masses with pelvic free fluid are highly predictive when present. Culdocentesis may be considered if ultrasound is unavailable.
Alternative Diagnoses To Consider
Differential diagnoses include spontaneous or threatened abortion, cervicitis, trauma, ruptured ovarian or corpus luteum cyst, ovarian torsion, urinary tract infection, nephrolithiasis, appendicitis, pelvic inflammatory disease, and heterotopic pregnancy, particularly in patients undergoing fertility treatments.
Prehospital And Early Management Considerations
Any woman of childbearing age presenting in shock should be presumed to have a ruptured ectopic pregnancy until proven otherwise. Early recognition and rapid transport are critical.
Stabilization Priorities
Unstable patients require airway management, aggressive resuscitation with oxygen and IV fluids, blood transfusion as needed, immediate gynecology consultation, and urgent operative management. Stable patients with confirmed ectopic pregnancy require gynecologic evaluation to determine suitability for medical versus surgical treatment. Patients with pregnancy of unknown location require close follow-up and serial β-hCG testing.
Emergency Department Interventions
Methotrexate therapy may be considered in reliable, stable patients with unruptured ectopic pregnancies, small ectopic size, and lower β-hCG levels, under obstetric supervision. Contraindications include breastfeeding, immunodeficiency, hematologic disorders, significant anemia, hepatic or renal dysfunction, peptic ulcer disease, active pulmonary disease, and alcoholism. Serial β-hCG monitoring is mandatory, and patients must be counseled regarding expected side effects and warning signs of rupture.
Pharmacologic Therapy
Methotrexate is typically administered as a single dose of 50 mg/m² intramuscularly or intravenously, with repeat dosing guided by β-hCG response. Rh-negative women should receive Rho(D) immune globulin based on gestational age.
Disposition And Monitoring Decisions
Admission is required for hemodynamically unstable patients and those with confirmed ectopic pregnancy who cannot ensure close follow-up. Outpatient management may be appropriate for stable, reliable patients with coordinated obstetric follow-up. Clear return precautions must be provided, including instructions to seek immediate care for worsening abdominal pain, increased bleeding, dizziness, or syncope.
Follow-Up Planning
All patients with positive pregnancy tests and no confirmed intrauterine pregnancy must have close obstetric follow-up with serial β-hCG testing and repeat ultrasound as indicated.
Key Clinical Insights And Common Errors
Always obtain a pregnancy test in women of childbearing age. Combine quantitative β-hCG testing with transvaginal ultrasound in any pregnant patient with abdominal pain or vaginal bleeding. Maintain awareness of heterotopic pregnancy, especially after assisted reproduction. Ensure reliable follow-up and clear return precautions for any patient discharged during evaluation for ectopic pregnancy.


