- Published on
Emergency and Acute Medicine – Carbon Monoxide Poisoning
Foundational Overview
Carbon monoxide is a colorless, odorless, and nonirritating gas that causes toxicity by binding hemoglobin to form carboxyhemoglobin, thereby reducing oxygen-carrying capacity. It also acts as a direct cellular toxin and interferes with intracellular oxygen utilization, leading to tissue hypoxia despite normal arterial oxygen tension.
Mechanisms And Sources
Carbon monoxide exposure may be endogenous at low levels from normal metabolism but is most often due to incomplete combustion of carbon-based fuels. Common sources include internal combustion engines, furnaces, fireplaces, heaters, indoor grills, accidental fires, and tobacco smoke. Methylene chloride, found in paint removers and furniture strippers, is metabolized in vivo to carbon monoxide, with delayed peak carboxyhemoglobin levels due to prolonged half-life.
Clinical Presentation
Symptoms are often nonspecific and may vary by organ system. Neurologic manifestations include headache, dizziness, ataxia, confusion, syncope, seizures, and coma. Gastrointestinal symptoms include nausea and vomiting. Cardiovascular findings may include chest pain and palpitations, while respiratory symptoms include dyspnea. Visual disturbances such as decreased acuity may occur.
Examination Findings
Neurologic examination may reveal acute encephalopathy, seizures, or coma. Cardiovascular findings include tachycardia, dysrhythmias, premature ventricular contractions, and myocardial ischemia or infarction. Respiratory findings include tachypnea and noncardiogenic pulmonary edema. Additional findings may include retinal hemorrhage, respiratory alkalosis, rhabdomyolysis, and lactic acidosis.
Initial Evaluation Strategy
A high index of suspicion is critical, as symptoms may be mild or vague. History should assess for similar symptoms in household members, malfunctioning heating systems, use of space heaters or ovens for heat, and illness in pets. Arterial blood gas typically shows normal PaO₂ with low measured oxygen saturation and may reveal metabolic acidosis in severe cases. Carboxyhemoglobin levels should be measured early but may underestimate severity if time has elapsed since exposure; normal levels are 0–3%, up to 10% in smokers.
Diagnostic Interpretation
Pulse oximetry is unreliable because it cannot differentiate oxyhemoglobin from carboxyhemoglobin and may appear falsely normal. Laboratory studies may reveal metabolic acidosis with elevated anion gap. Cardiac enzymes should be obtained when ischemia is suspected, and pregnancy testing is indicated when relevant. ECG may show dysrhythmias or nonspecific ST-T changes. Chest radiography may demonstrate pulmonary edema, and head CT may show bilateral globus pallidus lesions in unclear cases.
Conditions To Exclude
Alternative diagnoses include viral syndromes, meningitis or encephalitis, intracranial hemorrhage, gastroenteritis, migraine or tension headache, ethanol intoxication, sedative–hypnotic overdose, cyanide poisoning, salicylate toxicity, and toxic alcohol exposure.
Prehospital Care
Immediate administration of 100% oxygen is essential.
Early Emergency Management
Initial priorities include airway, breathing, and circulation, establishment of IV access, continuous cardiac monitoring, and delivery of 100% oxygen.
Definitive Emergency Treatment
Administer 100% normobaric oxygen via face mask or endotracheal tube until carboxyhemoglobin levels fall below 10%. The half-life of carboxyhemoglobin is approximately 300 minutes in room air, 90 minutes with 100% oxygen, and 20 minutes at 3 atmospheres in hyperbaric conditions. Hyperbaric oxygen therapy may reduce delayed neurologic sequelae and significantly shortens carboxyhemoglobin half-life, though its use remains controversial. Potential complications include barotrauma, pneumothorax, seizures, decompression sickness, and pulmonary edema. Consultation with a hyperbaric specialist is advised for altered mental status, focal neurologic deficits, seizures, cardiovascular instability, persistent metabolic acidosis, carboxyhemoglobin levels above 25%, or pregnancy with levels above 10%.
Pregnancy-Specific Considerations
Fetal hemoglobin has a higher affinity for carbon monoxide, resulting in fetal carboxyhemoglobin levels that exceed maternal levels by 10–15% and delayed fetal clearance, increasing risk of fetal hypoxia.
Disposition Planning
Admission is warranted for persistent symptoms after four hours of oxygen therapy, myocardial ischemia, seizures, syncope, metabolic acidosis, or hemodynamic instability. Discharge may be considered if the patient is asymptomatic after four hours of observation and none of the above criteria are present, with psychiatric clearance when exposure was intentional.
Follow-Up Guidance
Local fire authorities should be notified in cases of residential exposure to ensure environmental safety.
Key Clinical Insights
Carbon monoxide poisoning should be suspected in patients presenting with headache during heater use or when multiple individuals in the same environment develop similar symptoms. Early administration of 100% oxygen is critical, and timely transfer for hyperbaric therapy should be considered when indicated.
Foundational Overview
Carbon monoxide is a colorless, odorless, and nonirritating gas that causes toxicity by binding hemoglobin to form carboxyhemoglobin, thereby reducing oxygen-carrying capacity. It also acts as a direct cellular toxin and interferes with intracellular oxygen utilization, leading to tissue hypoxia despite normal arterial oxygen tension.
Mechanisms And Sources
Carbon monoxide exposure may be endogenous at low levels from normal metabolism but is most often due to incomplete combustion of carbon-based fuels. Common sources include internal combustion engines, furnaces, fireplaces, heaters, indoor grills, accidental fires, and tobacco smoke. Methylene chloride, found in paint removers and furniture strippers, is metabolized in vivo to carbon monoxide, with delayed peak carboxyhemoglobin levels due to prolonged half-life.
Clinical Presentation
Symptoms are often nonspecific and may vary by organ system. Neurologic manifestations include headache, dizziness, ataxia, confusion, syncope, seizures, and coma. Gastrointestinal symptoms include nausea and vomiting. Cardiovascular findings may include chest pain and palpitations, while respiratory symptoms include dyspnea. Visual disturbances such as decreased acuity may occur.
Examination Findings
Neurologic examination may reveal acute encephalopathy, seizures, or coma. Cardiovascular findings include tachycardia, dysrhythmias, premature ventricular contractions, and myocardial ischemia or infarction. Respiratory findings include tachypnea and noncardiogenic pulmonary edema. Additional findings may include retinal hemorrhage, respiratory alkalosis, rhabdomyolysis, and lactic acidosis.
Initial Evaluation Strategy
A high index of suspicion is critical, as symptoms may be mild or vague. History should assess for similar symptoms in household members, malfunctioning heating systems, use of space heaters or ovens for heat, and illness in pets. Arterial blood gas typically shows normal PaO₂ with low measured oxygen saturation and may reveal metabolic acidosis in severe cases. Carboxyhemoglobin levels should be measured early but may underestimate severity if time has elapsed since exposure; normal levels are 0–3%, up to 10% in smokers.
Diagnostic Interpretation
Pulse oximetry is unreliable because it cannot differentiate oxyhemoglobin from carboxyhemoglobin and may appear falsely normal. Laboratory studies may reveal metabolic acidosis with elevated anion gap. Cardiac enzymes should be obtained when ischemia is suspected, and pregnancy testing is indicated when relevant. ECG may show dysrhythmias or nonspecific ST-T changes. Chest radiography may demonstrate pulmonary edema, and head CT may show bilateral globus pallidus lesions in unclear cases.
Conditions To Exclude
Alternative diagnoses include viral syndromes, meningitis or encephalitis, intracranial hemorrhage, gastroenteritis, migraine or tension headache, ethanol intoxication, sedative–hypnotic overdose, cyanide poisoning, salicylate toxicity, and toxic alcohol exposure.
Prehospital Care
Immediate administration of 100% oxygen is essential.
Early Emergency Management
Initial priorities include airway, breathing, and circulation, establishment of IV access, continuous cardiac monitoring, and delivery of 100% oxygen.
Definitive Emergency Treatment
Administer 100% normobaric oxygen via face mask or endotracheal tube until carboxyhemoglobin levels fall below 10%. The half-life of carboxyhemoglobin is approximately 300 minutes in room air, 90 minutes with 100% oxygen, and 20 minutes at 3 atmospheres in hyperbaric conditions. Hyperbaric oxygen therapy may reduce delayed neurologic sequelae and significantly shortens carboxyhemoglobin half-life, though its use remains controversial. Potential complications include barotrauma, pneumothorax, seizures, decompression sickness, and pulmonary edema. Consultation with a hyperbaric specialist is advised for altered mental status, focal neurologic deficits, seizures, cardiovascular instability, persistent metabolic acidosis, carboxyhemoglobin levels above 25%, or pregnancy with levels above 10%.
Pregnancy-Specific Considerations
Fetal hemoglobin has a higher affinity for carbon monoxide, resulting in fetal carboxyhemoglobin levels that exceed maternal levels by 10–15% and delayed fetal clearance, increasing risk of fetal hypoxia.
Disposition Planning
Admission is warranted for persistent symptoms after four hours of oxygen therapy, myocardial ischemia, seizures, syncope, metabolic acidosis, or hemodynamic instability. Discharge may be considered if the patient is asymptomatic after four hours of observation and none of the above criteria are present, with psychiatric clearance when exposure was intentional.
Follow-Up Guidance
Local fire authorities should be notified in cases of residential exposure to ensure environmental safety.
Key Clinical Insights
Carbon monoxide poisoning should be suspected in patients presenting with headache during heater use or when multiple individuals in the same environment develop similar symptoms. Early administration of 100% oxygen is critical, and timely transfer for hyperbaric therapy should be considered when indicated.
- Published on
Emergency and Acute Medicine – Carbamazepine Poisoning
Overview And Clinical Context
Carbamazepine is an anticonvulsant used for seizure disorders, chronic neuropathic pain, migraine prophylaxis, and mood stabilization. Toxicity most commonly results from intentional overdose but may also occur with accidental ingestion, supratherapeutic dosing, or drug–drug interactions. Extended-release formulations are associated with delayed and unpredictable absorption. The drug blocks voltage-gated sodium channels and has anticholinergic properties similar to phenytoin and tricyclic antidepressants, leading primarily to neurologic toxicity, with cardiotoxicity typically seen only in massive overdoses.
Pathophysiology And Toxic Mechanisms
Excessive sodium channel blockade impairs neuronal conduction and decreases synaptic transmission. Carbamazepine is metabolized hepatically to an active epoxide metabolite that contributes significantly to toxicity but is not routinely measured, explaining the poor correlation between serum levels and clinical severity. Erratic gastrointestinal absorption and enterohepatic recirculation result in fluctuating serum concentrations and delayed recurrence of symptoms.
Clinical Manifestations
Neurologic findings predominate and include dizziness, drowsiness, ataxia, nystagmus, agitation, hallucinations, coma, and seizures. Respiratory depression and aspiration pneumonia may occur in severe cases. Cardiovascular effects include hypotension and conduction abnormalities, particularly in elderly patients or massive ingestions. Sinus tachycardia or bradycardia may be present, with ECG findings of PR, QRS, and QTc prolongation and nonspecific T-wave changes. Anticholinergic features include mydriasis, flushing, urinary retention, and decreased bowel sounds, while neuromuscular findings may include tremor, slurred speech, myoclonus, and choreiform movements.
Initial Assessment Priorities
All symptomatic patients require continuous cardiac monitoring. Serum carbamazepine levels should be obtained, recognizing therapeutic concentrations of 6–12 μg/mL and that levels above 25–40 μg/mL are associated with severe toxicity. Because serum levels may not reflect CNS exposure, serial measurements are often required. Electrocardiography is essential to assess conduction delays, and serum acetaminophen levels should be obtained in suspected intentional ingestions to evaluate for coingestants.
Supporting Diagnostic Studies
Laboratory findings may include leukopenia or leukocytosis, hyponatremia, hypokalemia, hyperglycemia, and mild transaminase elevations. Arterial blood gas analysis may show respiratory acidosis in severe poisoning. Urinalysis may demonstrate glucosuria or ketonuria. Chest radiography is indicated when aspiration pneumonia or pulmonary edema is suspected.
Diagnostic Alternatives To Consider
The differential diagnosis includes alcohol, benzodiazepines, opioids, lithium, barbiturates, anticholinergics, and phenothiazines. Seizure etiologies include alcohol withdrawal, isoniazid, camphor, sympathomimetics, and tricyclic antidepressants. Abnormal movements may be caused by antihistamines, cocaine, phenytoin, caffeine, neuroleptics, or levodopa.
Early Stabilization Measures
Ipecac is contraindicated. Initial management follows airway, breathing, and circulation principles with early airway protection for respiratory depression. Supplemental oxygen, intravenous access, isotonic fluid resuscitation for hypotension, and continuous cardiac monitoring are required. Naloxone, thiamine, and glucose should be considered in patients with altered mental status.
Emergency Department Management
Activated charcoal is recommended if presentation is early and bowel sounds are present, with sorbitol used only in the initial dose. Multidose activated charcoal may reduce toxicity by interrupting enterohepatic circulation and is indicated in moderate to severe cases. Hemoperfusion or hemodialysis removes limited drug amounts and is reserved for clinical deterioration despite supportive care. Respiratory failure requires intubation and ventilatory support. Hypotension should be treated with isotonic crystalloid boluses followed by norepinephrine if refractory. Seizures are treated with benzodiazepines, with diazepam as first-line therapy, and phenobarbital if refractory. Phenytoin is ineffective. Sodium bicarbonate is indicated for significant QRS prolongation. Psychiatric consultation is mandatory after intentional ingestion.
Disposition And Follow-Up Planning
Patients with seizures, dysrhythmias, persistent altered mental status, or intentional overdose require admission and monitoring for at least 24 hours due to delayed toxicity and serum level rebound. Asymptomatic patients may be discharged after six hours of observation if mental status and ECG are normal and psychiatric clearance is obtained when indicated.
High-Yield Clinical Takeaways
Carbamazepine levels commonly rebound, requiring serial monitoring. Clinical toxicity correlates poorly with serum concentrations. Multidose activated charcoal is frequently necessary. Paradoxical seizures may occur and should be treated with benzodiazepines. Continuous cardiac monitoring is essential due to delayed conduction abnormalities.
.
Overview And Clinical Context
Carbamazepine is an anticonvulsant used for seizure disorders, chronic neuropathic pain, migraine prophylaxis, and mood stabilization. Toxicity most commonly results from intentional overdose but may also occur with accidental ingestion, supratherapeutic dosing, or drug–drug interactions. Extended-release formulations are associated with delayed and unpredictable absorption. The drug blocks voltage-gated sodium channels and has anticholinergic properties similar to phenytoin and tricyclic antidepressants, leading primarily to neurologic toxicity, with cardiotoxicity typically seen only in massive overdoses.
Pathophysiology And Toxic Mechanisms
Excessive sodium channel blockade impairs neuronal conduction and decreases synaptic transmission. Carbamazepine is metabolized hepatically to an active epoxide metabolite that contributes significantly to toxicity but is not routinely measured, explaining the poor correlation between serum levels and clinical severity. Erratic gastrointestinal absorption and enterohepatic recirculation result in fluctuating serum concentrations and delayed recurrence of symptoms.
Clinical Manifestations
Neurologic findings predominate and include dizziness, drowsiness, ataxia, nystagmus, agitation, hallucinations, coma, and seizures. Respiratory depression and aspiration pneumonia may occur in severe cases. Cardiovascular effects include hypotension and conduction abnormalities, particularly in elderly patients or massive ingestions. Sinus tachycardia or bradycardia may be present, with ECG findings of PR, QRS, and QTc prolongation and nonspecific T-wave changes. Anticholinergic features include mydriasis, flushing, urinary retention, and decreased bowel sounds, while neuromuscular findings may include tremor, slurred speech, myoclonus, and choreiform movements.
Initial Assessment Priorities
All symptomatic patients require continuous cardiac monitoring. Serum carbamazepine levels should be obtained, recognizing therapeutic concentrations of 6–12 μg/mL and that levels above 25–40 μg/mL are associated with severe toxicity. Because serum levels may not reflect CNS exposure, serial measurements are often required. Electrocardiography is essential to assess conduction delays, and serum acetaminophen levels should be obtained in suspected intentional ingestions to evaluate for coingestants.
Supporting Diagnostic Studies
Laboratory findings may include leukopenia or leukocytosis, hyponatremia, hypokalemia, hyperglycemia, and mild transaminase elevations. Arterial blood gas analysis may show respiratory acidosis in severe poisoning. Urinalysis may demonstrate glucosuria or ketonuria. Chest radiography is indicated when aspiration pneumonia or pulmonary edema is suspected.
Diagnostic Alternatives To Consider
The differential diagnosis includes alcohol, benzodiazepines, opioids, lithium, barbiturates, anticholinergics, and phenothiazines. Seizure etiologies include alcohol withdrawal, isoniazid, camphor, sympathomimetics, and tricyclic antidepressants. Abnormal movements may be caused by antihistamines, cocaine, phenytoin, caffeine, neuroleptics, or levodopa.
Early Stabilization Measures
Ipecac is contraindicated. Initial management follows airway, breathing, and circulation principles with early airway protection for respiratory depression. Supplemental oxygen, intravenous access, isotonic fluid resuscitation for hypotension, and continuous cardiac monitoring are required. Naloxone, thiamine, and glucose should be considered in patients with altered mental status.
Emergency Department Management
Activated charcoal is recommended if presentation is early and bowel sounds are present, with sorbitol used only in the initial dose. Multidose activated charcoal may reduce toxicity by interrupting enterohepatic circulation and is indicated in moderate to severe cases. Hemoperfusion or hemodialysis removes limited drug amounts and is reserved for clinical deterioration despite supportive care. Respiratory failure requires intubation and ventilatory support. Hypotension should be treated with isotonic crystalloid boluses followed by norepinephrine if refractory. Seizures are treated with benzodiazepines, with diazepam as first-line therapy, and phenobarbital if refractory. Phenytoin is ineffective. Sodium bicarbonate is indicated for significant QRS prolongation. Psychiatric consultation is mandatory after intentional ingestion.
Disposition And Follow-Up Planning
Patients with seizures, dysrhythmias, persistent altered mental status, or intentional overdose require admission and monitoring for at least 24 hours due to delayed toxicity and serum level rebound. Asymptomatic patients may be discharged after six hours of observation if mental status and ECG are normal and psychiatric clearance is obtained when indicated.
High-Yield Clinical Takeaways
Carbamazepine levels commonly rebound, requiring serial monitoring. Clinical toxicity correlates poorly with serum concentrations. Multidose activated charcoal is frequently necessary. Paradoxical seizures may occur and should be treated with benzodiazepines. Continuous cardiac monitoring is essential due to delayed conduction abnormalities.
.

- Published on
Emergency and Acute Medicine – Oral Candidiasis
Overview and Definitions
Oral candidiasis is an infection of the oral mucosa caused by species of Candida. Although Candida albicans accounts for up to 80% of cases, other species such as Candida glabrata and Candida tropicalis may be involved, particularly in immunocompromised patients. Candida organisms are part of the normal oral flora in approximately 60% of healthy individuals.
Clinical variants include pseudomembranous candidiasis (thrush), acute and chronic atrophic candidiasis, angular cheilitis, and hyperplastic candidiasis. The condition is more common in neonates, the elderly, and immunocompromised individuals. In otherwise healthy patients, oral candidiasis typically follows a benign, localized course. In immunocompromised patients, infections are more likely to be recurrent, caused by non-albicans species, and may represent an early manifestation of HIV infection. Although usually localized, certain populations are at risk for progression to systemic infection.
Etiology and Pathophysiology
Oral candidiasis most commonly results from overgrowth of Candida albicans due to alterations in the intraoral environment. Medication-induced changes are frequent, particularly with antimicrobial use, inhaled or systemic corticosteroids, chemotherapy, and immunosuppressive agents. Impaired immune function significantly increases susceptibility.
Reduced salivary flow also predisposes to infection and may occur with anticholinergic or psychotropic medications, Sjögren disease, or head and neck radiation. Denture use and orthodontic appliances are common contributing factors and account for a large proportion of chronic atrophic candidiasis cases. Disruption of the epithelial barrier, endocrinopathies such as diabetes or hypothyroidism, and mechanical trauma may also contribute.
In infants, immune immaturity and lack of established oral flora predispose to thrush. In the elderly, denture use and age-related changes increase colonization, and angular cheilitis is more common due to facial wrinkling.
Diagnosis
Signs and Symptoms
Pseudomembranous candidiasis presents with painless, white, adherent plaques that can be scraped off to reveal an erythematous base. Lesions may become confluent and curdlike and may be associated with anorexia or dysphagia.
Acute atrophic candidiasis presents as erythematous mucosa with a burning sensation, typically involving the palate or tongue, which may appear bright red. Chronic atrophic candidiasis, also known as denture stomatitis, causes irritation and erythema beneath dentures. Angular cheilitis presents as cracking, erythema, or pain at the corners of the mouth and is often complicated by bacterial superinfection. Hyperplastic candidiasis manifests as chronic, adherent plaques or ulcers, usually on the lateral tongue or buccal mucosa, and carries a risk of malignant transformation, especially in tobacco users.
Essential Workup
In otherwise healthy infants, minimal evaluation is required and diagnosis is usually clinical. In adults or older children without clear risk factors, evaluation for underlying immunodeficiency or diabetes should be considered. Systemic infection should be excluded in high-risk patients.
Diagnostic Tests and Interpretation
Diagnosis is most often clinical. Laboratory testing may include CBC and serum glucose in patients with suspected systemic disease. Fungal staining or culture may reveal branching hyphae or pseudohyphae and is recommended in refractory cases or high-risk patients such as those with HIV, neutropenia, or transplant history.
Differential Diagnosis
Hairy leukoplakia, lichen planus, squamous cell carcinoma, and adherent food or milk residue.
Management
Emergency Department Management
Supportive care includes IV fluids if dehydration is present and topical analgesia for pain control. “Magic mouthwash,” consisting of viscous lidocaine, antacid, and diphenhydramine, may provide symptomatic relief. Topical antifungal therapy is first-line treatment, while systemic therapy is reserved for severe, recurrent, or refractory disease.
Patient education regarding oral hygiene is essential, including rinsing the mouth after inhaled steroid use and proper denture care.
Medications
First-line therapy includes topical antifungals such as nystatin oral suspension, nystatin pastilles, or clotrimazole troches administered for 7–14 days. Second-line therapy includes systemic azoles such as fluconazole or itraconazole for patients who fail topical therapy or have severe disease. Amphotericin B is preferred during pregnancy when systemic therapy is required.
Disposition and Follow-Up
Patients may be discharged if hydration and oral intake are adequate. Admission is indicated for inability to tolerate oral intake, newly diagnosed immunocompromised states, or evidence of systemic infection. Persistent or unexplained oral candidiasis warrants further evaluation for immunodeficiency.
Clinical Pearls and Pitfalls
Failure to recognize underlying immunodeficiency can delay diagnosis of serious systemic illness. Persistent oral lesions should prompt evaluation for alternative diagnoses, including squamous cell carcinoma.
- Published on
Emergency and Acute Medicine – Cervical Adenitis
Overview
Cervical adenitis is an acute bacterial infection of a cervical lymph node, most often arising after a preceding bacterial infection of the head or neck. It is primarily a pediatric condition but is increasingly recognized in adults, particularly those who are immunocompromised (HIV, malignancy, transplant recipients). Any cervical node may be involved, though more than 80% of pediatric cases affect the submandibular or deep cervical nodes, commonly the jugulodigastric node just below the mandibular angle. Cervical lymph nodes serve as the final common drainage pathway for the head and neck. Initial lymphadenopathy reflects hyperplasia and lymphocytic infiltration; progression to lymphadenitis occurs when bacteria proliferate within the lymphatic system, leading to neutrophil activation, pus formation, abscess development, and a clinically warm, tender, erythematous, swollen node.
Causative Factors
Approximately 70% of cases are due to group A β-hemolytic Streptococcus, 20% to Staphylococcus aureus, and about 10% to viral or other bacterial causes. Community-acquired MRSA infections are increasingly common, particularly in children, who have high colonization and invasive disease rates. Mycobacterial causes include tuberculosis (scrofula), typically a chronic posterior cervical lymphadenitis with strongly positive PPD and nonsurgical management, and atypical mycobacteria such as Mycobacterium avium complex, which usually presents as chronic submandibular or anterior cervical lymphadenitis and is treated surgically. Bartonella henselae causes catscratch disease, a subacute lymphadenitis with minimal systemic symptoms that usually resolves spontaneously over 4–6 weeks. Anaerobes should be considered with dental or gingival infections. Rare pathogens include gram-negative bacilli, Yersinia pestis, group B Streptococcus, Francisella tularensis, alpha-streptococcus, and Bacillus anthracis.
In neonates, group B Streptococcus and S. aureus predominate. Group B streptococcal cellulitis–adenitis syndrome presents in infants 3–7 weeks old with fever, submandibular or facial cellulitis, ipsilateral otitis media, and a high rate of bacteremia. Viral infections often cause bilateral adenopathy. In older adults, malignancy should be considered, particularly with hard, fixed, nontender nodes and absence of systemic infection signs.
Clinical Presentation
Patients typically present with a unilateral, enlarged, tender cervical lymph node with overlying warmth and erythema. The node is initially firm and may become fluctuant as suppuration develops. Fever may be present, along with malaise, and irritability in infants and children. A concurrent head or neck infection is common, including pharyngitis, tonsillitis, peritonsillar abscess, otitis media or externa, dental infection, impetigo, or scalp infection.
History and Examination
Key history includes timing of onset, associated fever, weight loss or rash, exposure or travel history, and comorbidities or birth history in infants. Physical examination requires a complete head and neck assessment with attention to airway patency and overall clinical appearance.
Evaluation Strategy
Cervical adenitis is primarily a clinical diagnosis. Identification of a primary head or neck infection source is essential. If no local source is found, tuberculosis exposure should be considered and systemic or viral illness evaluated. Laboratory studies are unnecessary when a clear, treatable source is identified. Blood cultures are reserved for toxic-appearing patients, and full sepsis evaluation is required in neonates. When etiology is unclear, adjunct testing such as CBC with differential, Monospot, throat cultures, and targeted serologies (EBV, CMV, toxoplasmosis) may be useful. Imaging with chest radiograph, lateral neck film, or Panorex can help identify occult sources or deep space infection; chest radiograph may screen for tuberculosis. Ultrasound can distinguish cystic from solid lesions and detect deep abscesses, while CT or MRI helps delineate deep space infections or congenital masses. Fluctuant nodes should undergo needle aspiration for Gram stain, acid-fast stain, and aerobic, anaerobic, mycobacterial, and fungal cultures, except when tuberculosis is suspected, due to risk of sinus tract formation.
Alternative Diagnoses
Consider reactive lymphadenopathy from viral infections (adenovirus, rhinovirus, enterovirus, EBV, HSV, VZV, CMV), mumps, rubella, rubeola, Kawasaki disease, Kikuchi disease, PFAPA syndrome, toxoplasmosis, congenital cysts (branchial cleft, thyroglossal duct cyst, cystic hygroma), malignancy (leukemia, lymphoma, rhabdomyosarcoma, thyroid carcinoma), and systemic inflammatory diseases such as lupus or sarcoidosis.
Management Principles
Airway monitoring is essential if significant neck swelling is present. Treatment targets the underlying source of infection, with empiric coverage for group A Streptococcus and S. aureus; MRSA coverage should be considered if there is poor response to standard therapy. All fluctuant nodes require aspiration. Oral agents such as cephalexin, cefadroxil, or amoxicillin–clavulanate are commonly effective. Clindamycin or amoxicillin–clavulanate is preferred when dental or anaerobic sources are suspected. CA-MRSA may be treated with clindamycin or TMP-SMX, recognizing increasing resistance; toxic patients may require IV vancomycin or linezolid. Antibiotic therapy should continue for at least 10 days. Adjunctive measures include warm compresses and analgesia.
Disposition and Follow-Up
Admission is indicated for neonates, airway compromise, toxic appearance, immunocompromised patients, inability to tolerate oral intake, or failure of outpatient therapy. Most patients can be discharged on oral antibiotics with mandatory re-evaluation in 48–72 hours. Patients should return immediately for worsening symptoms, abscess formation, voice changes, dyspnea, or systemic illness. Referral to ENT or dentistry is based on the infection source, and concerning features for malignancy or congenital anomalies warrant specialist evaluation.
Clinical Insights
Cervical adenitis is a clinical diagnosis most often caused by group A Streptococcus or Staphylococcus aureus. Unilateral, warm, tender, erythematous lymphadenopathy is characteristic. Consider group B Streptococcus in young infants and MRSA in cases not improving with standard therapy. Disposition decisions should be guided by overall clinical status rather than node size alone.
Overview
Cervical adenitis is an acute bacterial infection of a cervical lymph node, most often arising after a preceding bacterial infection of the head or neck. It is primarily a pediatric condition but is increasingly recognized in adults, particularly those who are immunocompromised (HIV, malignancy, transplant recipients). Any cervical node may be involved, though more than 80% of pediatric cases affect the submandibular or deep cervical nodes, commonly the jugulodigastric node just below the mandibular angle. Cervical lymph nodes serve as the final common drainage pathway for the head and neck. Initial lymphadenopathy reflects hyperplasia and lymphocytic infiltration; progression to lymphadenitis occurs when bacteria proliferate within the lymphatic system, leading to neutrophil activation, pus formation, abscess development, and a clinically warm, tender, erythematous, swollen node.
Causative Factors
Approximately 70% of cases are due to group A β-hemolytic Streptococcus, 20% to Staphylococcus aureus, and about 10% to viral or other bacterial causes. Community-acquired MRSA infections are increasingly common, particularly in children, who have high colonization and invasive disease rates. Mycobacterial causes include tuberculosis (scrofula), typically a chronic posterior cervical lymphadenitis with strongly positive PPD and nonsurgical management, and atypical mycobacteria such as Mycobacterium avium complex, which usually presents as chronic submandibular or anterior cervical lymphadenitis and is treated surgically. Bartonella henselae causes catscratch disease, a subacute lymphadenitis with minimal systemic symptoms that usually resolves spontaneously over 4–6 weeks. Anaerobes should be considered with dental or gingival infections. Rare pathogens include gram-negative bacilli, Yersinia pestis, group B Streptococcus, Francisella tularensis, alpha-streptococcus, and Bacillus anthracis.
In neonates, group B Streptococcus and S. aureus predominate. Group B streptococcal cellulitis–adenitis syndrome presents in infants 3–7 weeks old with fever, submandibular or facial cellulitis, ipsilateral otitis media, and a high rate of bacteremia. Viral infections often cause bilateral adenopathy. In older adults, malignancy should be considered, particularly with hard, fixed, nontender nodes and absence of systemic infection signs.
Clinical Presentation
Patients typically present with a unilateral, enlarged, tender cervical lymph node with overlying warmth and erythema. The node is initially firm and may become fluctuant as suppuration develops. Fever may be present, along with malaise, and irritability in infants and children. A concurrent head or neck infection is common, including pharyngitis, tonsillitis, peritonsillar abscess, otitis media or externa, dental infection, impetigo, or scalp infection.
History and Examination
Key history includes timing of onset, associated fever, weight loss or rash, exposure or travel history, and comorbidities or birth history in infants. Physical examination requires a complete head and neck assessment with attention to airway patency and overall clinical appearance.
Evaluation Strategy
Cervical adenitis is primarily a clinical diagnosis. Identification of a primary head or neck infection source is essential. If no local source is found, tuberculosis exposure should be considered and systemic or viral illness evaluated. Laboratory studies are unnecessary when a clear, treatable source is identified. Blood cultures are reserved for toxic-appearing patients, and full sepsis evaluation is required in neonates. When etiology is unclear, adjunct testing such as CBC with differential, Monospot, throat cultures, and targeted serologies (EBV, CMV, toxoplasmosis) may be useful. Imaging with chest radiograph, lateral neck film, or Panorex can help identify occult sources or deep space infection; chest radiograph may screen for tuberculosis. Ultrasound can distinguish cystic from solid lesions and detect deep abscesses, while CT or MRI helps delineate deep space infections or congenital masses. Fluctuant nodes should undergo needle aspiration for Gram stain, acid-fast stain, and aerobic, anaerobic, mycobacterial, and fungal cultures, except when tuberculosis is suspected, due to risk of sinus tract formation.
Alternative Diagnoses
Consider reactive lymphadenopathy from viral infections (adenovirus, rhinovirus, enterovirus, EBV, HSV, VZV, CMV), mumps, rubella, rubeola, Kawasaki disease, Kikuchi disease, PFAPA syndrome, toxoplasmosis, congenital cysts (branchial cleft, thyroglossal duct cyst, cystic hygroma), malignancy (leukemia, lymphoma, rhabdomyosarcoma, thyroid carcinoma), and systemic inflammatory diseases such as lupus or sarcoidosis.
Management Principles
Airway monitoring is essential if significant neck swelling is present. Treatment targets the underlying source of infection, with empiric coverage for group A Streptococcus and S. aureus; MRSA coverage should be considered if there is poor response to standard therapy. All fluctuant nodes require aspiration. Oral agents such as cephalexin, cefadroxil, or amoxicillin–clavulanate are commonly effective. Clindamycin or amoxicillin–clavulanate is preferred when dental or anaerobic sources are suspected. CA-MRSA may be treated with clindamycin or TMP-SMX, recognizing increasing resistance; toxic patients may require IV vancomycin or linezolid. Antibiotic therapy should continue for at least 10 days. Adjunctive measures include warm compresses and analgesia.
Disposition and Follow-Up
Admission is indicated for neonates, airway compromise, toxic appearance, immunocompromised patients, inability to tolerate oral intake, or failure of outpatient therapy. Most patients can be discharged on oral antibiotics with mandatory re-evaluation in 48–72 hours. Patients should return immediately for worsening symptoms, abscess formation, voice changes, dyspnea, or systemic illness. Referral to ENT or dentistry is based on the infection source, and concerning features for malignancy or congenital anomalies warrant specialist evaluation.
Clinical Insights
Cervical adenitis is a clinical diagnosis most often caused by group A Streptococcus or Staphylococcus aureus. Unilateral, warm, tender, erythematous lymphadenopathy is characteristic. Consider group B Streptococcus in young infants and MRSA in cases not improving with standard therapy. Disposition decisions should be guided by overall clinical status rather than node size alone.
- Published on
Emergency and Acute Medicine - Cerebrovascular Accident (Stroke)
Overview
A cerebrovascular accident (CVA) results from interruption of blood flow to a specific brain region. Clinical deficits correspond to the vascular territory involved. Onset may be abrupt and complete or stepwise and fluctuating. Stroke accounts for ~1 in 18 deaths in the United States, with ~610,000 new cases annually.
Predisposing Factors
Hypertension, diabetes mellitus, smoking, coronary artery disease, cardiac dysrhythmias, peripheral vascular disease, oral contraceptive use, polycythemia vera, sickle cell disease, antithrombin III deficiency, protein C or S deficiency.
Pathologic Mechanisms
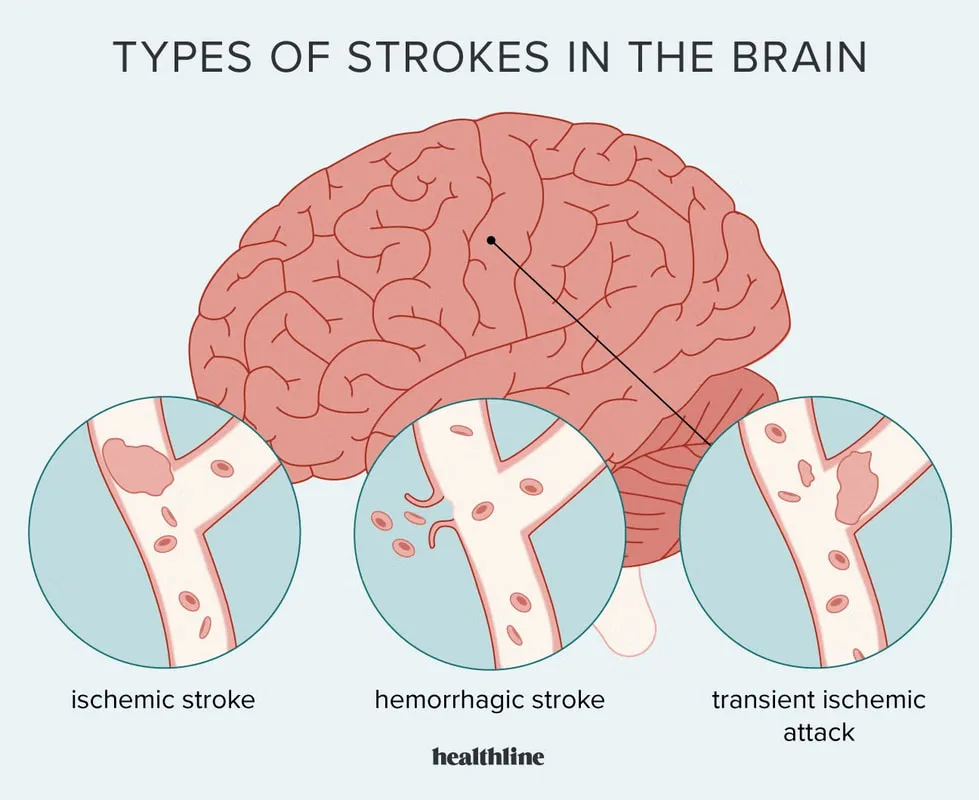
Ischemic stroke includes thrombotic, embolic, dissection-related, or hypoperfusion etiologies. Thrombotic stroke most often results from clot formation at an ulcerated atherosclerotic plaque or from sludging states (sickle cell disease, polycythemia vera, protein C deficiency). Embolic stroke arises from cardiac mural thrombi (atrial fibrillation, mitral stenosis, cardiomyopathy, CHF, MI), prosthetic or abnormal valves, carotid or aortic arch plaques, atrial myxoma, or ventricular aneurysm thrombi. Arterial dissection may involve carotid arteries or be associated with arteritis (giant cell, Takayasu) or fibromuscular dysplasia. Global ischemic stroke results from systemic hypotension due to sepsis, hemorrhage, or shock. Hemorrhagic stroke includes intracerebral and subarachnoid hemorrhage.
Pediatrics: Usually secondary to underlying disease (sickle cell disease, leukemia, infection, blood dyscrasia); younger children often present with seizures or altered mental status.
Clinical Features
History focuses on exact time of onset or last known normal, trauma or surgery, medications, confusion, headache, vertigo, and focal neurologic deficits.
General exam may show Cheyne–Stokes respirations, apnea, hypertension, dysrhythmias, or murmurs.
Anterior cerebral artery involvement causes contralateral leg-predominant weakness and sensory loss, apraxia, confusion, and impaired judgment.
Middle cerebral artery involvement causes contralateral face and arm weakness, hemisensory loss, homonymous hemianopsia, aphasia or dysarthria, and agnosia.
Posterior cerebral artery involvement causes cortical blindness, visual agnosia, memory impairment, altered mental status, third-nerve palsy, or hemiballismus.
Vertebrobasilar strokes cause vertigo, diplopia, nystagmus, visual field defects, and crossed cranial nerve and motor deficits; basilar artery occlusion may lead to quadriplegia, locked-in syndrome, or coma.
Watershed infarcts produce proximal limb weakness with sparing of face, hands, and feet.
Initial Evaluation Priorities
Perform a focused neurologic examination and calculate the NIH Stroke Scale when possible. Obtain emergent noncontrast head CT to differentiate ischemic from hemorrhagic stroke; early CT may be normal within 24–48 hours. Goals include CT completion within 25 minutes, interpretation within 45 minutes, and thrombolytic administration within 60 minutes if indicated. If CT is negative but subarachnoid hemorrhage is suspected, perform lumbar puncture. Obtain ECG, oxygen saturation, and rapid blood glucose.
Diagnostic Studies
Laboratory tests include CBC, electrolytes, renal and liver function, PT/PTT, urinalysis, and ESR when indicated. Additional studies may include cardiac enzymes, pregnancy test, toxicology screen, alcohol level, ABG, and blood cultures. Imaging may include MRI for early ischemia, chest radiograph, and carotid ultrasound. ECG evaluates for arrhythmia; lumbar puncture is required if CT is nondiagnostic and SAH remains suspected.
Key Differentials
Intracranial hemorrhage, hypoglycemia, seizure with Todd paralysis, conversion disorder, transient global amnesia, encephalitis or meningitis, peripheral neuropathy, intracranial abscess, migraine, air embolism, TIA, metabolic encephalopathy, neoplasm, vasculitis, multiple sclerosis, compressive myelopathy, vestibulitis, medication or toxin effects.
Prehospital Considerations
Patients may have impaired movement or communication. Field neurologic assessment should include level of consciousness, GCS, speech, facial symmetry, gait, and motor deficits. Fingerstick glucose is essential.
Stabilization Measures
Ensure airway protection; provide supplemental oxygen at 2–4 L/min. Intubation may be required for airway control or ICP management. For altered mental status, administer naloxone and thiamine and correct hypoglycemia.
Emergency Department Management
Treat severe hypertension only if SBP >220 mm Hg or DBP >120 mm Hg, or if required for comorbid conditions; initial target is <180 />10 mm Hg. Control seizures with benzodiazepines followed by fosphenytoin or phenytoin. Maintain euvolemia and normothermia.
Thrombolysis: For ischemic stroke only, administer IV alteplase within 4.5 hours of symptom onset if criteria are met. Avoid antiplatelet and anticoagulant therapy for 24 hours post-tPA.
Contraindications: Prior intracranial hemorrhage, recent stroke or head trauma (<3 months), major surgery (<14 days), uncontrolled hypertension, bleeding diathesis, recent mi, inr>1.7, platelets <100,000, intracranial neoplasm, seizure at onset, rapidly improving symptoms, pregnancy, recent internal bleeding, glucose <50 mg />L, age <18 years.< />pan>
3-4.5 hour exclusions: Age >80, oral anticoagulant use, NIHSS >25 or >1/3 MCA involvement, prior stroke plus diabetes.
Manage cerebral edema with head elevation, controlled ventilation (PaCO₂ 35–40 mm Hg), mannitol, and neurosurgical consultation when indicated. Selected patients may undergo intra-arterial thrombolysis or mechanical thrombectomy.
Medications
First line: Alteplase 0.9 mg/kg IV (max 90 mg), aspirin 81–325 mg PO/PR, labetalol IV bolus and infusion.
Second line: Clopidogrel, diazepam, enalapril, hydralazine, mannitol, nicardipine, nitroprusside, trimethaphan.
Pediatrics: Heparin or LMWH often used; pediatric stroke consultation available via 1-800-NOCLOTS.
Disposition
All acute strokes require hospital admission. ICU admission is indicated for depressed consciousness, hemodynamic instability, serious arrhythmias, elevated ICP, or tPA administration.
Discharge may be considered for completed strokes days to weeks old in patients who are functionally independent or have reliable support.
Follow-Up Care
Neurology consultation, primary care follow-up, and rehabilitation services including speech and occupational therapy.
Clinical Pearls
Document prehospital observations carefully. Accurate symptom onset time is critical for thrombolysis eligibility. Avoid rapid BP reduction to prevent cerebral hypoperfusion. Door-to-needle time goal is under 60 minutes.
Overview
A cerebrovascular accident (CVA) results from interruption of blood flow to a specific brain region. Clinical deficits correspond to the vascular territory involved. Onset may be abrupt and complete or stepwise and fluctuating. Stroke accounts for ~1 in 18 deaths in the United States, with ~610,000 new cases annually.
Predisposing Factors
Hypertension, diabetes mellitus, smoking, coronary artery disease, cardiac dysrhythmias, peripheral vascular disease, oral contraceptive use, polycythemia vera, sickle cell disease, antithrombin III deficiency, protein C or S deficiency.
Pathologic Mechanisms
Ischemic stroke includes thrombotic, embolic, dissection-related, or hypoperfusion etiologies. Thrombotic stroke most often results from clot formation at an ulcerated atherosclerotic plaque or from sludging states (sickle cell disease, polycythemia vera, protein C deficiency). Embolic stroke arises from cardiac mural thrombi (atrial fibrillation, mitral stenosis, cardiomyopathy, CHF, MI), prosthetic or abnormal valves, carotid or aortic arch plaques, atrial myxoma, or ventricular aneurysm thrombi. Arterial dissection may involve carotid arteries or be associated with arteritis (giant cell, Takayasu) or fibromuscular dysplasia. Global ischemic stroke results from systemic hypotension due to sepsis, hemorrhage, or shock. Hemorrhagic stroke includes intracerebral and subarachnoid hemorrhage.
Pediatrics: Usually secondary to underlying disease (sickle cell disease, leukemia, infection, blood dyscrasia); younger children often present with seizures or altered mental status.
Clinical Features
History focuses on exact time of onset or last known normal, trauma or surgery, medications, confusion, headache, vertigo, and focal neurologic deficits.
General exam may show Cheyne–Stokes respirations, apnea, hypertension, dysrhythmias, or murmurs.
Anterior cerebral artery involvement causes contralateral leg-predominant weakness and sensory loss, apraxia, confusion, and impaired judgment.
Middle cerebral artery involvement causes contralateral face and arm weakness, hemisensory loss, homonymous hemianopsia, aphasia or dysarthria, and agnosia.
Posterior cerebral artery involvement causes cortical blindness, visual agnosia, memory impairment, altered mental status, third-nerve palsy, or hemiballismus.
Vertebrobasilar strokes cause vertigo, diplopia, nystagmus, visual field defects, and crossed cranial nerve and motor deficits; basilar artery occlusion may lead to quadriplegia, locked-in syndrome, or coma.
Watershed infarcts produce proximal limb weakness with sparing of face, hands, and feet.
Initial Evaluation Priorities
Perform a focused neurologic examination and calculate the NIH Stroke Scale when possible. Obtain emergent noncontrast head CT to differentiate ischemic from hemorrhagic stroke; early CT may be normal within 24–48 hours. Goals include CT completion within 25 minutes, interpretation within 45 minutes, and thrombolytic administration within 60 minutes if indicated. If CT is negative but subarachnoid hemorrhage is suspected, perform lumbar puncture. Obtain ECG, oxygen saturation, and rapid blood glucose.
Diagnostic Studies
Laboratory tests include CBC, electrolytes, renal and liver function, PT/PTT, urinalysis, and ESR when indicated. Additional studies may include cardiac enzymes, pregnancy test, toxicology screen, alcohol level, ABG, and blood cultures. Imaging may include MRI for early ischemia, chest radiograph, and carotid ultrasound. ECG evaluates for arrhythmia; lumbar puncture is required if CT is nondiagnostic and SAH remains suspected.
Key Differentials
Intracranial hemorrhage, hypoglycemia, seizure with Todd paralysis, conversion disorder, transient global amnesia, encephalitis or meningitis, peripheral neuropathy, intracranial abscess, migraine, air embolism, TIA, metabolic encephalopathy, neoplasm, vasculitis, multiple sclerosis, compressive myelopathy, vestibulitis, medication or toxin effects.
Prehospital Considerations
Patients may have impaired movement or communication. Field neurologic assessment should include level of consciousness, GCS, speech, facial symmetry, gait, and motor deficits. Fingerstick glucose is essential.
Stabilization Measures
Ensure airway protection; provide supplemental oxygen at 2–4 L/min. Intubation may be required for airway control or ICP management. For altered mental status, administer naloxone and thiamine and correct hypoglycemia.
Emergency Department Management
Treat severe hypertension only if SBP >220 mm Hg or DBP >120 mm Hg, or if required for comorbid conditions; initial target is <180 />10 mm Hg. Control seizures with benzodiazepines followed by fosphenytoin or phenytoin. Maintain euvolemia and normothermia.
Thrombolysis: For ischemic stroke only, administer IV alteplase within 4.5 hours of symptom onset if criteria are met. Avoid antiplatelet and anticoagulant therapy for 24 hours post-tPA.
Contraindications: Prior intracranial hemorrhage, recent stroke or head trauma (<3 months), major surgery (<14 days), uncontrolled hypertension, bleeding diathesis, recent mi, inr>1.7, platelets <100,000, intracranial neoplasm, seizure at onset, rapidly improving symptoms, pregnancy, recent internal bleeding, glucose <50 mg />L, age <18 years.< />pan>
3-4.5 hour exclusions: Age >80, oral anticoagulant use, NIHSS >25 or >1/3 MCA involvement, prior stroke plus diabetes.
Manage cerebral edema with head elevation, controlled ventilation (PaCO₂ 35–40 mm Hg), mannitol, and neurosurgical consultation when indicated. Selected patients may undergo intra-arterial thrombolysis or mechanical thrombectomy.
Medications
First line: Alteplase 0.9 mg/kg IV (max 90 mg), aspirin 81–325 mg PO/PR, labetalol IV bolus and infusion.
Second line: Clopidogrel, diazepam, enalapril, hydralazine, mannitol, nicardipine, nitroprusside, trimethaphan.
Pediatrics: Heparin or LMWH often used; pediatric stroke consultation available via 1-800-NOCLOTS.
Disposition
All acute strokes require hospital admission. ICU admission is indicated for depressed consciousness, hemodynamic instability, serious arrhythmias, elevated ICP, or tPA administration.
Discharge may be considered for completed strokes days to weeks old in patients who are functionally independent or have reliable support.
Follow-Up Care
Neurology consultation, primary care follow-up, and rehabilitation services including speech and occupational therapy.
Clinical Pearls
Document prehospital observations carefully. Accurate symptom onset time is critical for thrombolysis eligibility. Avoid rapid BP reduction to prevent cerebral hypoperfusion. Door-to-needle time goal is under 60 minutes.
- Published on
Emergency and Acute Medicine – Cerebral Aneurysm
Core Overview
A cerebral aneurysm is a focal dilation or outpouching of a cerebral artery wall. It occurs in approximately 5–10% of the population. Rupture of saccular aneurysms accounts for 5–15% of all strokes. Distribution of ruptured aneurysms includes the anterior communicating artery (≈40%), internal carotid artery (≈30%), middle cerebral artery (≈20%), and vertebrobasilar system (≈5–10%).
Underlying Causes and Associations
Most cerebral aneurysms are saccular (berry) aneurysms, representing about 90% of cases. They develop at arterial bifurcations and weak points in vessel walls and increase in incidence with age. Multiple aneurysms occur in 20–30% of patients. Higher prevalence is seen with polycystic kidney disease, cerebral AVMs, connective tissue disorders (Ehlers–Danlos, Marfan), fibromuscular dysplasia, moyamoya syndrome, coarctation of the aorta, sickle cell disease, neurofibromatosis, and inflammatory or genetic disorders. Fusiform or dolichoectatic aneurysms account for about 7% and are more common in peripheral vessels. Mycotic aneurysms occur in roughly 10% of patients with bacterial endocarditis. Traumatic and neoplastic aneurysms are less common. A first-degree relative with an aneurysm nearly doubles lifetime risk. In children, aneurysms are rare but often large and located in the posterior circulation.
Clinical Presentation
Most aneurysms are asymptomatic until rupture. Sentinel headaches occur in 30–60% of patients and may precede rupture. Rupture leads to subarachnoid hemorrhage, typically presenting with a sudden, severe “thunderclap” headache described as the worst headache of life, often without focal deficits. Nuchal rigidity is common due to blood in the CSF. Seizures, syncope, or altered mental status may occur. Compression of adjacent structures can cause focal neurologic signs. ACA aneurysms may affect optic pathways, causing visual field deficits. Internal carotid–posterior communicating artery aneurysms often compress the oculomotor nerve, producing ptosis, diplopia, and a fixed dilated pupil. Cortical aneurysms may cause hemiparesis, aphasia, visual disturbances, or seizures.
Essential Evaluation
A complete neurologic examination is critical. Emergent noncontrast head CT detects 90–95% of subarachnoid hemorrhages. If CT is negative but suspicion remains high, lumbar puncture with CSF analysis is required.
Diagnostic Studies
Laboratory testing includes CBC, coagulation studies, electrolytes, renal and liver function tests, and arterial blood gas as indicated. Imaging includes chest radiography for pulmonary edema. Four-vessel cerebral angiography remains the diagnostic gold standard. CTA and MRA can identify aneurysms larger than 3 mm. Transcranial Doppler ultrasound is useful for monitoring vasospasm. Lumbar puncture is indicated when CT is normal but aneurysmal rupture is suspected.
Key Differentials
Consider arteriovenous malformation, intracranial hemorrhage (subdural, epidural, intracerebral), thromboembolic stroke, meningitis, encephalitis, migraine, optic neuritis, acute glaucoma, hypertensive encephalopathy, metabolic disturbances, sinusitis, and temporal arteritis.
Prehospital Priorities
Field neurologic assessment is valuable, including level of consciousness, speech, motor deficits, gait, and facial symmetry. Patients with suspected subarachnoid hemorrhage may require emergent airway protection and rapid transport to a facility with CT and ICU capabilities.
Initial Stabilization
Secure airway, breathing, and circulation. Provide supplemental oxygen and continuous cardiac and pulse oximetry monitoring. Rapid-sequence intubation may be necessary. Check blood glucose immediately in altered patients and correct hypoglycemia. Reverse anticoagulation when indicated. Control nausea and vomiting to prevent spikes in intracranial pressure. Treat seizures acutely with IV benzodiazepines and antiepileptics; routine seizure prophylaxis is not recommended.
Emergency Department Management
Early goals include prevention of rebleeding, vasospasm, and hydrocephalus. Management follows subarachnoid hemorrhage protocols. Early neurosurgical involvement is essential. Ventriculostomy may be required for intracranial pressure control and can reduce systemic hypertension.
Definitive Intervention
Timing of angiography and repair remains debated, though early intervention is favored to reduce rebleeding and vasospasm. Pediatric aneurysms carry a high hemorrhage risk and should be repaired early.
Pharmacologic Therapy
Blood pressure control is essential, commonly with labetalol or nicardipine. Nimodipine is used orally or via nasogastric tube to reduce vasospasm risk and should never be given intravenously. Antiemetics and stool softeners help prevent increases in intracranial pressure. Antiepileptics are used for active seizures.
Disposition and Follow-Up
All patients with aneurysmal subarachnoid hemorrhage require ICU admission. Symptomatic unruptured aneurysms warrant admission and urgent neurosurgical consultation due to high rupture risk. Incidentally discovered, asymptomatic aneurysms may be discharged with close neurosurgical follow-up. Annual rupture risk is approximately 1–2%, with treatment thresholds often considered in the 4–8 mm range.
Clinical Pearls and Pitfalls
A normal CT does not exclude subarachnoid hemorrhage—lumbar puncture is essential when suspicion persists. Vasospasm typically develops around day 3 after bleeding or surgery. Nimodipine reduces vasospasm-related morbidity but must never be administered intravenously. Avoid nitroprusside and nitroglycerin, as they can increase cerebral blood volume and intracranial pressure.
Core Overview
A cerebral aneurysm is a focal dilation or outpouching of a cerebral artery wall. It occurs in approximately 5–10% of the population. Rupture of saccular aneurysms accounts for 5–15% of all strokes. Distribution of ruptured aneurysms includes the anterior communicating artery (≈40%), internal carotid artery (≈30%), middle cerebral artery (≈20%), and vertebrobasilar system (≈5–10%).
Underlying Causes and Associations
Most cerebral aneurysms are saccular (berry) aneurysms, representing about 90% of cases. They develop at arterial bifurcations and weak points in vessel walls and increase in incidence with age. Multiple aneurysms occur in 20–30% of patients. Higher prevalence is seen with polycystic kidney disease, cerebral AVMs, connective tissue disorders (Ehlers–Danlos, Marfan), fibromuscular dysplasia, moyamoya syndrome, coarctation of the aorta, sickle cell disease, neurofibromatosis, and inflammatory or genetic disorders. Fusiform or dolichoectatic aneurysms account for about 7% and are more common in peripheral vessels. Mycotic aneurysms occur in roughly 10% of patients with bacterial endocarditis. Traumatic and neoplastic aneurysms are less common. A first-degree relative with an aneurysm nearly doubles lifetime risk. In children, aneurysms are rare but often large and located in the posterior circulation.
Clinical Presentation
Most aneurysms are asymptomatic until rupture. Sentinel headaches occur in 30–60% of patients and may precede rupture. Rupture leads to subarachnoid hemorrhage, typically presenting with a sudden, severe “thunderclap” headache described as the worst headache of life, often without focal deficits. Nuchal rigidity is common due to blood in the CSF. Seizures, syncope, or altered mental status may occur. Compression of adjacent structures can cause focal neurologic signs. ACA aneurysms may affect optic pathways, causing visual field deficits. Internal carotid–posterior communicating artery aneurysms often compress the oculomotor nerve, producing ptosis, diplopia, and a fixed dilated pupil. Cortical aneurysms may cause hemiparesis, aphasia, visual disturbances, or seizures.
Essential Evaluation
A complete neurologic examination is critical. Emergent noncontrast head CT detects 90–95% of subarachnoid hemorrhages. If CT is negative but suspicion remains high, lumbar puncture with CSF analysis is required.
Diagnostic Studies
Laboratory testing includes CBC, coagulation studies, electrolytes, renal and liver function tests, and arterial blood gas as indicated. Imaging includes chest radiography for pulmonary edema. Four-vessel cerebral angiography remains the diagnostic gold standard. CTA and MRA can identify aneurysms larger than 3 mm. Transcranial Doppler ultrasound is useful for monitoring vasospasm. Lumbar puncture is indicated when CT is normal but aneurysmal rupture is suspected.
Key Differentials
Consider arteriovenous malformation, intracranial hemorrhage (subdural, epidural, intracerebral), thromboembolic stroke, meningitis, encephalitis, migraine, optic neuritis, acute glaucoma, hypertensive encephalopathy, metabolic disturbances, sinusitis, and temporal arteritis.
Prehospital Priorities
Field neurologic assessment is valuable, including level of consciousness, speech, motor deficits, gait, and facial symmetry. Patients with suspected subarachnoid hemorrhage may require emergent airway protection and rapid transport to a facility with CT and ICU capabilities.
Initial Stabilization
Secure airway, breathing, and circulation. Provide supplemental oxygen and continuous cardiac and pulse oximetry monitoring. Rapid-sequence intubation may be necessary. Check blood glucose immediately in altered patients and correct hypoglycemia. Reverse anticoagulation when indicated. Control nausea and vomiting to prevent spikes in intracranial pressure. Treat seizures acutely with IV benzodiazepines and antiepileptics; routine seizure prophylaxis is not recommended.
Emergency Department Management
Early goals include prevention of rebleeding, vasospasm, and hydrocephalus. Management follows subarachnoid hemorrhage protocols. Early neurosurgical involvement is essential. Ventriculostomy may be required for intracranial pressure control and can reduce systemic hypertension.
Definitive Intervention
Timing of angiography and repair remains debated, though early intervention is favored to reduce rebleeding and vasospasm. Pediatric aneurysms carry a high hemorrhage risk and should be repaired early.
Pharmacologic Therapy
Blood pressure control is essential, commonly with labetalol or nicardipine. Nimodipine is used orally or via nasogastric tube to reduce vasospasm risk and should never be given intravenously. Antiemetics and stool softeners help prevent increases in intracranial pressure. Antiepileptics are used for active seizures.
Disposition and Follow-Up
All patients with aneurysmal subarachnoid hemorrhage require ICU admission. Symptomatic unruptured aneurysms warrant admission and urgent neurosurgical consultation due to high rupture risk. Incidentally discovered, asymptomatic aneurysms may be discharged with close neurosurgical follow-up. Annual rupture risk is approximately 1–2%, with treatment thresholds often considered in the 4–8 mm range.
Clinical Pearls and Pitfalls
A normal CT does not exclude subarachnoid hemorrhage—lumbar puncture is essential when suspicion persists. Vasospasm typically develops around day 3 after bleeding or surgery. Nimodipine reduces vasospasm-related morbidity but must never be administered intravenously. Avoid nitroprusside and nitroglycerin, as they can increase cerebral blood volume and intracranial pressure.

- Published on
Emergency and Acute Medicine – Central Retinal Vein Occlusion
Overview
Central retinal vein occlusion (CRVO) is characterized by decreased visual acuity due to venous outflow obstruction of the retina. Vision loss is typically acute, unilateral, and painless. The condition results from impaired venous drainage leading to retinal hemorrhage, edema, and ischemia.
Pathophysiologic Types
Ischemic CRVO accounts for approximately 20–25% of cases and represents complete venous obstruction. Blocked venous return causes capillary backflow, extensive hemorrhage, macular edema, and retinal ischemia. Thrombosis is promoted by limited space at the lamina cribrosa, slow blood flow, vessel wall changes, adjacent arteriosclerotic arterial compression, and increased blood viscosity.
Nonischemic CRVO represents partial or incomplete occlusion and is generally milder with better visual prognosis.
Clinical Features
Patients present with acute, painless, unilateral loss of vision. In nonischemic CRVO, vision loss may be intermittent or incomplete. Visual acuity is often severely reduced, commonly worse than 20/200. An afferent pupillary defect may be present. Fundoscopic examination reveals dilated and tortuous retinal veins, widespread retinal hemorrhages involving all four quadrants in central involvement, optic disc edema, and cotton wool spots. Extensive hemorrhage produces the classic “blood and thunder” appearance.
Essential Assessment
Measure blood pressure. Perform visual acuity testing, visual field assessment, fundoscopy, and tonometry. Normal intraocular pressure ranges from 10–21 mm Hg.
Diagnostic Evaluation
Laboratory studies include CBC, PT/PTT, ESR, ANA, and serum protein electrophoresis to assess for systemic or hyperviscosity conditions. Fluorescein angiography, performed by ophthalmology, differentiates ischemic from nonischemic CRVO by identifying areas of capillary nonperfusion. Gonioscopy is used to evaluate for iris or angle neovascularization.
Differential Considerations
Amaurosis fugax or TIA, cavernous sinus thrombosis, diabetic or hypertensive retinopathy, hyperviscosity syndromes (sickle cell disease, polycythemia, leukemia, multiple myeloma), ocular ischemia syndrome, papilledema, retinal artery occlusion, retinal detachment, temporal arteritis, vitreous hemorrhage, severe anemia with thrombocytopenia, and functional vision loss.
Initial Management Principles
There are no prehospital eye-specific interventions. In the ED, address elevated intraocular pressure if present and manage underlying systemic conditions. The cornerstone of management is early recognition and urgent ophthalmologic referral.
Emergency Department Management
No therapy has proven definitive benefit in the ED setting. In consultation with ophthalmology, attempted therapies may include aspirin, anti-inflammatory agents, systemic corticosteroids, systemic anticoagulation, fibrinolytics (controversial), or laser chorioretinal anastomosis.
Definitive and Ophthalmologic Therapies
Ophthalmologists may use intravitreal corticosteroids such as triamcinolone or antivascular endothelial growth factor agents such as bevacizumab. Panretinal photocoagulation is often performed if neovascularization develops.
Disposition and Follow-Up
Admission depends on ophthalmologic assessment and need for intervention. Patients may be discharged if immediate ophthalmology follow-up is ensured. If ophthalmologic care is unavailable, initiate management of associated conditions and transfer to a facility with specialty services. Long-term follow-up is essential, particularly for ischemic CRVO, to detect neovascularization and secondary glaucoma. Patients require full medical evaluation for underlying vascular disease and comorbidity management.
Clinical Insights and Pitfalls
Elevated intraocular pressure from edema or neovascularization can worsen ischemia and lead to permanent vision loss if untreated. Bilateral CRVO or CRVO in young patients should prompt evaluation for hyperviscosity syndromes and systemic disease.
Overview
Central retinal vein occlusion (CRVO) is characterized by decreased visual acuity due to venous outflow obstruction of the retina. Vision loss is typically acute, unilateral, and painless. The condition results from impaired venous drainage leading to retinal hemorrhage, edema, and ischemia.
Pathophysiologic Types
Ischemic CRVO accounts for approximately 20–25% of cases and represents complete venous obstruction. Blocked venous return causes capillary backflow, extensive hemorrhage, macular edema, and retinal ischemia. Thrombosis is promoted by limited space at the lamina cribrosa, slow blood flow, vessel wall changes, adjacent arteriosclerotic arterial compression, and increased blood viscosity.
Nonischemic CRVO represents partial or incomplete occlusion and is generally milder with better visual prognosis.
Clinical Features
Patients present with acute, painless, unilateral loss of vision. In nonischemic CRVO, vision loss may be intermittent or incomplete. Visual acuity is often severely reduced, commonly worse than 20/200. An afferent pupillary defect may be present. Fundoscopic examination reveals dilated and tortuous retinal veins, widespread retinal hemorrhages involving all four quadrants in central involvement, optic disc edema, and cotton wool spots. Extensive hemorrhage produces the classic “blood and thunder” appearance.
Essential Assessment
Measure blood pressure. Perform visual acuity testing, visual field assessment, fundoscopy, and tonometry. Normal intraocular pressure ranges from 10–21 mm Hg.
Diagnostic Evaluation
Laboratory studies include CBC, PT/PTT, ESR, ANA, and serum protein electrophoresis to assess for systemic or hyperviscosity conditions. Fluorescein angiography, performed by ophthalmology, differentiates ischemic from nonischemic CRVO by identifying areas of capillary nonperfusion. Gonioscopy is used to evaluate for iris or angle neovascularization.
Differential Considerations
Amaurosis fugax or TIA, cavernous sinus thrombosis, diabetic or hypertensive retinopathy, hyperviscosity syndromes (sickle cell disease, polycythemia, leukemia, multiple myeloma), ocular ischemia syndrome, papilledema, retinal artery occlusion, retinal detachment, temporal arteritis, vitreous hemorrhage, severe anemia with thrombocytopenia, and functional vision loss.
Initial Management Principles
There are no prehospital eye-specific interventions. In the ED, address elevated intraocular pressure if present and manage underlying systemic conditions. The cornerstone of management is early recognition and urgent ophthalmologic referral.
Emergency Department Management
No therapy has proven definitive benefit in the ED setting. In consultation with ophthalmology, attempted therapies may include aspirin, anti-inflammatory agents, systemic corticosteroids, systemic anticoagulation, fibrinolytics (controversial), or laser chorioretinal anastomosis.
Definitive and Ophthalmologic Therapies
Ophthalmologists may use intravitreal corticosteroids such as triamcinolone or antivascular endothelial growth factor agents such as bevacizumab. Panretinal photocoagulation is often performed if neovascularization develops.
Disposition and Follow-Up
Admission depends on ophthalmologic assessment and need for intervention. Patients may be discharged if immediate ophthalmology follow-up is ensured. If ophthalmologic care is unavailable, initiate management of associated conditions and transfer to a facility with specialty services. Long-term follow-up is essential, particularly for ischemic CRVO, to detect neovascularization and secondary glaucoma. Patients require full medical evaluation for underlying vascular disease and comorbidity management.
Clinical Insights and Pitfalls
Elevated intraocular pressure from edema or neovascularization can worsen ischemia and lead to permanent vision loss if untreated. Bilateral CRVO or CRVO in young patients should prompt evaluation for hyperviscosity syndromes and systemic disease.
- Published on
Emergency and Acute Medicine – Central Retinal Artery Occlusion
Overview
Central retinal artery occlusion (CRAO) is an obstruction of the central retinal artery resulting in sudden, painless, monocular vision loss. It typically affects adults aged 50–70 years and is often described as a “stroke of the eye.” The ophthalmic artery is the first branch of the carotid artery. Risk factors include hypertension, atherosclerosis, carotid artery disease, valvular heart disease, coronary artery disease, vasculitis, lupus, sickle cell disease, and trauma. Incidence is approximately 1–10 per 100,000. Irreversible retinal injury can occur within 90 minutes.
Causative Mechanisms
Embolic causes are most common and include cholesterol or platelet emboli from carotid atherosclerosis, carotid stenosis, valvular heart disease, atrial myxoma, or arterial dissection. Thrombotic causes result from rupture of an atherosclerotic plaque or hypercoagulable states such as sickle cell disease. Inflammatory causes include giant cell arteritis, lupus, and systemic vasculitis. Arterial spasm may be migraine-related. Reduced ocular perfusion may occur with severe hypotension, acute angle-closure glaucoma, or retrobulbar hemorrhage.
Clinical Presentation
Patients present with sudden, painless, unilateral vision loss. Some report prior transient episodes of visual loss lasting seconds to minutes (amaurosis fugax). Visual acuity is markedly reduced. An afferent pupillary defect is usually present. Fundoscopy may reveal emboli within retinal vessels appearing as yellow-white glistening plaques, ischemic retinal edema within 15–20 minutes, and a classic cherry-red spot at the fovea. Retinal arteries may appear empty or show segmented “box-carring.” Within 1–2 hours, the infarcted retina becomes opaque. Partial visual field deficits suggest branch retinal artery involvement.
Essential Evaluation
Immediate assessment includes visual acuity, visual fields, fundoscopic examination, intraocular pressure measurement, and urgent ophthalmology consultation.
Diagnostic Studies
Laboratory evaluation targets underlying causes and includes CBC with platelets, PT/PTT, electrolytes, renal function, glucose, ESR and CRP (especially in patients >55 years for giant cell arteritis), ANA, RF, RPR, hemoglobin electrophoresis, and serum protein electrophoresis. Imaging focuses on embolic sources and includes carotid Doppler ultrasound and echocardiography. Fluorescein angiography or electroretinography may confirm diagnosis.
Differential Considerations
Acute angle-closure glaucoma, central retinal vein occlusion, giant cell arteritis, optic neuritis, and retinal detachment.
Emergency Management Principles
This is a true ophthalmologic emergency. Treatment must begin immediately to attempt retinal salvage. Goals include embolus displacement or dissolution, vasodilation to improve retinal perfusion, and reduction of intraocular pressure to enhance the perfusion gradient.
Emergency Department Interventions
Initiate immediate ocular (global) massage with the patient supine: apply firm pressure on the closed eyelid for 15 seconds, release for 15 seconds, and repeat for five cycles. Administer 100% oxygen via nonrebreather mask and consider hyperbaric oxygen if within 24 hours of onset. Carbogen inhalation may be used if available. Reduce intraocular pressure with IV acetazolamide and topical timolol. Administer aspirin and IV heparin to prevent clot propagation. Obtain emergent ophthalmology consultation for possible anterior chamber paracentesis and consideration of intra-arterial fibrinolysis. If inflammatory arteritis is suspected, begin high-dose systemic corticosteroids immediately.
Medications
First-line options include acetazolamide 500 mg IV or PO, timolol maleate 0.5% ophthalmic drops, IV heparin (80 U/kg bolus then 18 U/kg/hr infusion), and carbogen inhalation. Second-line or adjunctive therapies include aspirin 325 mg PO, methylprednisolone 250 mg IV for suspected arteritis, mannitol, and sublingual nitroglycerin.
Disposition and Follow-Up
Most acute cases require admission for urgent evaluation of embolic, thrombotic, or inflammatory sources. Chronic or remote occlusions without active disease may be evaluated outpatient. All suspected cases require immediate ophthalmology involvement. Carotid imaging is recommended in most patients.
Clinical Insights and Pitfalls
Transient monocular vision loss (amaurosis fugax) is a warning sign for CRAO and systemic stroke and requires urgent evaluation. CRAO is a medical and ophthalmologic emergency with a very narrow therapeutic window. Thorough documentation of visual acuity and fundoscopic findings is essential.
Overview
Central retinal artery occlusion (CRAO) is an obstruction of the central retinal artery resulting in sudden, painless, monocular vision loss. It typically affects adults aged 50–70 years and is often described as a “stroke of the eye.” The ophthalmic artery is the first branch of the carotid artery. Risk factors include hypertension, atherosclerosis, carotid artery disease, valvular heart disease, coronary artery disease, vasculitis, lupus, sickle cell disease, and trauma. Incidence is approximately 1–10 per 100,000. Irreversible retinal injury can occur within 90 minutes.
Causative Mechanisms
Embolic causes are most common and include cholesterol or platelet emboli from carotid atherosclerosis, carotid stenosis, valvular heart disease, atrial myxoma, or arterial dissection. Thrombotic causes result from rupture of an atherosclerotic plaque or hypercoagulable states such as sickle cell disease. Inflammatory causes include giant cell arteritis, lupus, and systemic vasculitis. Arterial spasm may be migraine-related. Reduced ocular perfusion may occur with severe hypotension, acute angle-closure glaucoma, or retrobulbar hemorrhage.
Clinical Presentation
Patients present with sudden, painless, unilateral vision loss. Some report prior transient episodes of visual loss lasting seconds to minutes (amaurosis fugax). Visual acuity is markedly reduced. An afferent pupillary defect is usually present. Fundoscopy may reveal emboli within retinal vessels appearing as yellow-white glistening plaques, ischemic retinal edema within 15–20 minutes, and a classic cherry-red spot at the fovea. Retinal arteries may appear empty or show segmented “box-carring.” Within 1–2 hours, the infarcted retina becomes opaque. Partial visual field deficits suggest branch retinal artery involvement.
Essential Evaluation
Immediate assessment includes visual acuity, visual fields, fundoscopic examination, intraocular pressure measurement, and urgent ophthalmology consultation.
Diagnostic Studies
Laboratory evaluation targets underlying causes and includes CBC with platelets, PT/PTT, electrolytes, renal function, glucose, ESR and CRP (especially in patients >55 years for giant cell arteritis), ANA, RF, RPR, hemoglobin electrophoresis, and serum protein electrophoresis. Imaging focuses on embolic sources and includes carotid Doppler ultrasound and echocardiography. Fluorescein angiography or electroretinography may confirm diagnosis.
Differential Considerations
Acute angle-closure glaucoma, central retinal vein occlusion, giant cell arteritis, optic neuritis, and retinal detachment.
Emergency Management Principles
This is a true ophthalmologic emergency. Treatment must begin immediately to attempt retinal salvage. Goals include embolus displacement or dissolution, vasodilation to improve retinal perfusion, and reduction of intraocular pressure to enhance the perfusion gradient.
Emergency Department Interventions
Initiate immediate ocular (global) massage with the patient supine: apply firm pressure on the closed eyelid for 15 seconds, release for 15 seconds, and repeat for five cycles. Administer 100% oxygen via nonrebreather mask and consider hyperbaric oxygen if within 24 hours of onset. Carbogen inhalation may be used if available. Reduce intraocular pressure with IV acetazolamide and topical timolol. Administer aspirin and IV heparin to prevent clot propagation. Obtain emergent ophthalmology consultation for possible anterior chamber paracentesis and consideration of intra-arterial fibrinolysis. If inflammatory arteritis is suspected, begin high-dose systemic corticosteroids immediately.
Medications
First-line options include acetazolamide 500 mg IV or PO, timolol maleate 0.5% ophthalmic drops, IV heparin (80 U/kg bolus then 18 U/kg/hr infusion), and carbogen inhalation. Second-line or adjunctive therapies include aspirin 325 mg PO, methylprednisolone 250 mg IV for suspected arteritis, mannitol, and sublingual nitroglycerin.
Disposition and Follow-Up
Most acute cases require admission for urgent evaluation of embolic, thrombotic, or inflammatory sources. Chronic or remote occlusions without active disease may be evaluated outpatient. All suspected cases require immediate ophthalmology involvement. Carotid imaging is recommended in most patients.
Clinical Insights and Pitfalls
Transient monocular vision loss (amaurosis fugax) is a warning sign for CRAO and systemic stroke and requires urgent evaluation. CRAO is a medical and ophthalmologic emergency with a very narrow therapeutic window. Thorough documentation of visual acuity and fundoscopic findings is essential.

- Published on
Emergency and Acute Medicine – Cellulitis
Core Concepts
Cellulitis is an acute, spreading infection of the skin and subcutaneous tissues with erythema, warmth, pain, tenderness, and progressive expansion. Extension into deeper layers may evolve into necrotizing soft-tissue infection. Predisposing factors include lymphedema, tinea pedis, open wounds, pre-existing lesions such as furuncles, prior trauma or surgery, retained foreign body, vascular or immune compromise, and injection drug use.
Likely Causes
Uncomplicated cellulitis is most often due to group A streptococci or Staphylococcus aureus, including community-associated MRSA (CA-MRSA). CA-MRSA risk is higher with prior MRSA infection, close contact with MRSA cases, daycare exposure, children, soldiers, incarcerated persons, contact-sport athletes, IV drug users, and men who have sex with men; CA-MRSA prevalence is high enough that empiric coverage is often appropriate, especially in nonresponding cases. Hospital-acquired MRSA is associated with recent hospitalization or long-term care, surgery, vascular devices, dialysis, recent antibiotic exposure, and injection drug use and is resistant to many antibiotics. After lymphatic disruption, nongroup A β-hemolytic streptococci (groups C, B, G) are more common. Diabetic cellulitis may be polymicrobial with streptococci, S. aureus, gram-negatives, and anaerobes, especially with ulcers. Special patterns include periorbital cellulitis (staph and strep), buccal cellulitis (historically Hib, plus anaerobic oral flora with intraoral lacerations or dental abscess), and less common exposures such as Pasteurella (cat/dog bites), Eikenella (human bites), Pseudomonas (hot-tub folliculitis; puncture wounds), Aeromonas (freshwater), Vibrio (seawater/raw seafood), Erysipelothrix (raw fish/meat handlers), clostridia, and anthrax. Pediatric patterns include facial cellulitis (strep pneumo and Hib—declining with vaccination), perianal cellulitis (group A strep), and neonatal cases (group B strep).
Clinical Features
Typical findings include pain, warmth, erythema, edema/induration, fever/chills, tender regional nodes, lymphangitis, and sometimes superficial vesicles. A concurrent subcutaneous abscess can coexist, and a deep abscess should be suspected if there is treatment failure. Buccal/odontogenic cellulitis may progress with fever, neck swelling, dysphagia, and deep-space spread. Pediatric facial cellulitis can be rapidly progressive, usually unilateral with URTI symptoms, and carries risk of cavernous sinus thrombosis and optic nerve injury. Perianal cellulitis presents with pruritic erythema extending outward from the anus, pain with defecation, and sometimes blood-streaked stools. Bedside clues: staphylococcal infection tends to have focal pustule/abscess with fluctuance or drainage and a slower course, while streptococcal infection often has sharper borders, lymphangitis, lymphedema association, and may include nausea from toxin effects.
Key Assessment
Cellulitis is primarily a clinical diagnosis; the exam should look for a portal of entry or deeper infection and assess for airway risk in deep facial/neck involvement.
Testing Strategy
Routine WBC is usually unnecessary. Aspirate/punch biopsy for Gram stain and culture is most useful in treatment failures and in admitted patients to identify resistant organisms such as MRSA. Blood cultures are typically negative in uncomplicated disease but may help in lymphedema-associated infections, buccal or periorbital cellulitis, water-exposure cases, or systemic symptoms with fever/chills. Plain radiographs can detect foreign bodies, subcutaneous gas, or suggest abscess; early osteomyelitis is not reliably seen. Ultrasound helps identify abscess when exam is equivocal and may show “cobblestoning” of the subcutaneous tissue in cellulitis. CT/MRI can help evaluate for necrotizing fasciitis.
Conditions to Differentiate
Important alternatives include necrotizing fasciitis, lymphangitis/lymphadenitis, thrombophlebitis or DVT, insect bite/allergy, gout/pseudogout, ruptured Baker cyst, herpetic whitlow, neoplasm, phytophotodermatitis, erythema migrans, and for facial disease, angioedema, conjunctivitis, or contusion. Pediatric perianal differentials include Candida intertrigo, psoriasis, pinworms, abuse, behavioral causes, and inflammatory bowel disease.
Emergency Management
Airway compromise is a concern with deep facial or neck extension. General approach: account for local resistance patterns and include CA-MRSA coverage when appropriate (notably uncomplicated cellulitis in many settings, periorbital disease, and diabetics). Typical outpatient duration is 7–10 days, with cool compresses, analgesia, elevation, and treatment of tinea pedis when present.
Antibiotic Approach by Scenario
Simple cellulitis outpatient: oral cephalexin plus TMP-SMX for CA-MRSA coverage; alternatives for β-lactam include dicloxacillin, macrolide, or levofloxacin; alternatives to TMP-SMX include clindamycin or doxycycline. Inpatient: IV nafcillin (or equivalent) plus IV vancomycin. Post-lymphatic disruption cellulitis: treat like simple cellulitis. Diabetic cellulitis outpatient: amoxicillin/clavulanate plus TMP-SMX or clindamycin; inpatient: IV ampicillin/sulbactam or imipenem-cilastatin plus IV vancomycin. Adult periorbital cellulitis outpatient: dicloxacillin or azithromycin plus TMP-SMX; inpatient: IV vancomycin. Adult buccal cellulitis outpatient: amoxicillin/clavulanate; inpatient: IV ceftriaxone; odontogenic cases require drainage and anaerobe coverage such as clindamycin. Pediatric facial cellulitis: IV ceftriaxone. Perianal cellulitis: oral penicillin VK outpatient or IV penicillin G inpatient. Bite wounds: amoxicillin/clavulanate. Foot puncture wounds: ciprofloxacin or IV ceftazidime. MRSA: hospital-acquired—IV vancomycin or linezolid; CA-MRSA—TMP-SMX, clindamycin, or doxycycline orally, and vancomycin or clindamycin IV.
Medication Options
Common regimens include amoxicillin/clavulanate, ampicillin/sulbactam, azithromycin, ceftazidime, ceftriaxone, cephalexin, ciprofloxacin, clindamycin, dicloxacillin, doxycycline, imipenem-cilastatin, levofloxacin, linezolid, nafcillin, penicillin VK, aqueous penicillin G, TMP-SMX, and vancomycin with pediatric adjustments and therapeutic monitoring where appropriate.
Disposition Criteria
Admit patients who appear toxic, have tissue necrosis, immunosuppression, significant comorbid illness, inability to tolerate oral meds, unreliable follow-up, or high-risk anatomy. Discharge is reasonable for mild infection in a nontoxic patient who can take oral therapy, has no immunosuppression or major comorbidities, no hand/face involvement, and has reliable follow-up within 24–48 hours.
Follow-Up Guidance
Reassess within 24–48 hours, sooner if fever worsens, lymphangitis develops, or erythema expands. Mark the edge of erythema prior to discharge to track progression.
Clinical Traps
Strep and staph remain the most common causes, and CA-MRSA is common enough that empiric coverage is often required. Clinicians are not reliably accurate at identifying MRSA by appearance alone. Deep abscess can be mistaken for cellulitis; use clinical suspicion and ultrasound to avoid missed abscess.
Core Concepts
Cellulitis is an acute, spreading infection of the skin and subcutaneous tissues with erythema, warmth, pain, tenderness, and progressive expansion. Extension into deeper layers may evolve into necrotizing soft-tissue infection. Predisposing factors include lymphedema, tinea pedis, open wounds, pre-existing lesions such as furuncles, prior trauma or surgery, retained foreign body, vascular or immune compromise, and injection drug use.
Likely Causes
Uncomplicated cellulitis is most often due to group A streptococci or Staphylococcus aureus, including community-associated MRSA (CA-MRSA). CA-MRSA risk is higher with prior MRSA infection, close contact with MRSA cases, daycare exposure, children, soldiers, incarcerated persons, contact-sport athletes, IV drug users, and men who have sex with men; CA-MRSA prevalence is high enough that empiric coverage is often appropriate, especially in nonresponding cases. Hospital-acquired MRSA is associated with recent hospitalization or long-term care, surgery, vascular devices, dialysis, recent antibiotic exposure, and injection drug use and is resistant to many antibiotics. After lymphatic disruption, nongroup A β-hemolytic streptococci (groups C, B, G) are more common. Diabetic cellulitis may be polymicrobial with streptococci, S. aureus, gram-negatives, and anaerobes, especially with ulcers. Special patterns include periorbital cellulitis (staph and strep), buccal cellulitis (historically Hib, plus anaerobic oral flora with intraoral lacerations or dental abscess), and less common exposures such as Pasteurella (cat/dog bites), Eikenella (human bites), Pseudomonas (hot-tub folliculitis; puncture wounds), Aeromonas (freshwater), Vibrio (seawater/raw seafood), Erysipelothrix (raw fish/meat handlers), clostridia, and anthrax. Pediatric patterns include facial cellulitis (strep pneumo and Hib—declining with vaccination), perianal cellulitis (group A strep), and neonatal cases (group B strep).
Clinical Features
Typical findings include pain, warmth, erythema, edema/induration, fever/chills, tender regional nodes, lymphangitis, and sometimes superficial vesicles. A concurrent subcutaneous abscess can coexist, and a deep abscess should be suspected if there is treatment failure. Buccal/odontogenic cellulitis may progress with fever, neck swelling, dysphagia, and deep-space spread. Pediatric facial cellulitis can be rapidly progressive, usually unilateral with URTI symptoms, and carries risk of cavernous sinus thrombosis and optic nerve injury. Perianal cellulitis presents with pruritic erythema extending outward from the anus, pain with defecation, and sometimes blood-streaked stools. Bedside clues: staphylococcal infection tends to have focal pustule/abscess with fluctuance or drainage and a slower course, while streptococcal infection often has sharper borders, lymphangitis, lymphedema association, and may include nausea from toxin effects.
Key Assessment
Cellulitis is primarily a clinical diagnosis; the exam should look for a portal of entry or deeper infection and assess for airway risk in deep facial/neck involvement.
Testing Strategy
Routine WBC is usually unnecessary. Aspirate/punch biopsy for Gram stain and culture is most useful in treatment failures and in admitted patients to identify resistant organisms such as MRSA. Blood cultures are typically negative in uncomplicated disease but may help in lymphedema-associated infections, buccal or periorbital cellulitis, water-exposure cases, or systemic symptoms with fever/chills. Plain radiographs can detect foreign bodies, subcutaneous gas, or suggest abscess; early osteomyelitis is not reliably seen. Ultrasound helps identify abscess when exam is equivocal and may show “cobblestoning” of the subcutaneous tissue in cellulitis. CT/MRI can help evaluate for necrotizing fasciitis.
Conditions to Differentiate
Important alternatives include necrotizing fasciitis, lymphangitis/lymphadenitis, thrombophlebitis or DVT, insect bite/allergy, gout/pseudogout, ruptured Baker cyst, herpetic whitlow, neoplasm, phytophotodermatitis, erythema migrans, and for facial disease, angioedema, conjunctivitis, or contusion. Pediatric perianal differentials include Candida intertrigo, psoriasis, pinworms, abuse, behavioral causes, and inflammatory bowel disease.
Emergency Management
Airway compromise is a concern with deep facial or neck extension. General approach: account for local resistance patterns and include CA-MRSA coverage when appropriate (notably uncomplicated cellulitis in many settings, periorbital disease, and diabetics). Typical outpatient duration is 7–10 days, with cool compresses, analgesia, elevation, and treatment of tinea pedis when present.
Antibiotic Approach by Scenario
Simple cellulitis outpatient: oral cephalexin plus TMP-SMX for CA-MRSA coverage; alternatives for β-lactam include dicloxacillin, macrolide, or levofloxacin; alternatives to TMP-SMX include clindamycin or doxycycline. Inpatient: IV nafcillin (or equivalent) plus IV vancomycin. Post-lymphatic disruption cellulitis: treat like simple cellulitis. Diabetic cellulitis outpatient: amoxicillin/clavulanate plus TMP-SMX or clindamycin; inpatient: IV ampicillin/sulbactam or imipenem-cilastatin plus IV vancomycin. Adult periorbital cellulitis outpatient: dicloxacillin or azithromycin plus TMP-SMX; inpatient: IV vancomycin. Adult buccal cellulitis outpatient: amoxicillin/clavulanate; inpatient: IV ceftriaxone; odontogenic cases require drainage and anaerobe coverage such as clindamycin. Pediatric facial cellulitis: IV ceftriaxone. Perianal cellulitis: oral penicillin VK outpatient or IV penicillin G inpatient. Bite wounds: amoxicillin/clavulanate. Foot puncture wounds: ciprofloxacin or IV ceftazidime. MRSA: hospital-acquired—IV vancomycin or linezolid; CA-MRSA—TMP-SMX, clindamycin, or doxycycline orally, and vancomycin or clindamycin IV.
Medication Options
Common regimens include amoxicillin/clavulanate, ampicillin/sulbactam, azithromycin, ceftazidime, ceftriaxone, cephalexin, ciprofloxacin, clindamycin, dicloxacillin, doxycycline, imipenem-cilastatin, levofloxacin, linezolid, nafcillin, penicillin VK, aqueous penicillin G, TMP-SMX, and vancomycin with pediatric adjustments and therapeutic monitoring where appropriate.
Disposition Criteria
Admit patients who appear toxic, have tissue necrosis, immunosuppression, significant comorbid illness, inability to tolerate oral meds, unreliable follow-up, or high-risk anatomy. Discharge is reasonable for mild infection in a nontoxic patient who can take oral therapy, has no immunosuppression or major comorbidities, no hand/face involvement, and has reliable follow-up within 24–48 hours.
Follow-Up Guidance
Reassess within 24–48 hours, sooner if fever worsens, lymphangitis develops, or erythema expands. Mark the edge of erythema prior to discharge to track progression.
Clinical Traps
Strep and staph remain the most common causes, and CA-MRSA is common enough that empiric coverage is often required. Clinicians are not reliably accurate at identifying MRSA by appearance alone. Deep abscess can be mistaken for cellulitis; use clinical suspicion and ultrasound to avoid missed abscess.
- Published on
Emergency and Acute Medicine – Cavernous Sinus Thrombosis
Overview
Cavernous sinus thrombosis is thrombosis within a major intracranial venous drainage pathway and is most often infectious in origin. Infection commonly spreads from facial, odontogenic, or paranasal sinus sources, with hematogenous or contiguous extension. Less frequently, thrombosis occurs in the setting of hypercoagulable states. The cavernous sinus lies superolateral to the sphenoid sinus and surrounds the sella; cranial nerves III, IV, V1, and V2 course within its lateral wall, while cranial nerve VI and the internal carotid artery run medially. Although the cavernous sinus is most often involved, the transverse and superior sagittal sinuses may also be affected.
Pathophysiologic Mechanisms
Infection spreads hematogenously from facial, otic, or neck sources or directly from infected sinus cavities, most commonly sphenoid and ethmoid sinuses. Bacterial proliferation triggers inflammation and coagulation, leading to venous thrombosis. Resulting venous congestion affects adjacent neurovascular structures, producing ophthalmoplegia from involvement of cranial nerves III, IV, or VI, pupillary abnormalities from cranial nerve III dysfunction, and sensory deficits of the forehead or cheek from cranial nerves V1 and V2.
Causative Factors
Septic thrombosis is most common, with Staphylococcus aureus responsible for approximately 70% of cases; Streptococcus pneumoniae, gram-negative organisms, and anaerobes are also implicated. Fungal causes such as Aspergillus and Rhizopus are less frequent. Aseptic causes include granulomatous disease such as tuberculosis, inflammatory disorders, mass effect from skull-base tumors or aneurysms, and hypercoagulable states.
Clinical Presentation
Headache is present in the majority of patients, often accompanied by fever, ocular or retrobulbar pain, facial swelling, visual disturbances, facial dysesthesia, and lethargy or altered mental status. Early physical findings include periorbital edema and chemosis with retinal venous congestion, followed by ptosis, proptosis, and ophthalmoplegia. Cranial nerve deficits are common, particularly lateral gaze palsy from cranial nerve VI involvement and sensory changes in V1 or V2 distributions. Advanced disease may present with meningismus, seizures, coma, or septic shock.
Risk-Oriented History
High-risk features include recent facial trauma, ENT or neurosurgical procedures, manipulation of central facial furuncles, diabetes, or immunocompromised states such as HIV infection, chronic steroid use, or malignancy. Pediatric patients may present with nonspecific symptoms including fever, vomiting, lethargy, or signs of increased intracranial pressure, particularly following otitis or pharyngitis; neonatal cases are especially challenging to diagnose.
Initial Clinical Assessment
Diagnosis is primarily clinical, suggested by venous congestion, ocular findings, unilateral symptoms that rapidly progress to bilateral involvement, and overall toxic appearance. Laboratory studies are supportive but nonspecific, and early imaging findings may be subtle.
Diagnostic Evaluation
Laboratory testing may show leukocytosis, bandemia, and elevated ESR or D-dimer, but lacks sensitivity and specificity. Cerebrospinal fluid analysis may demonstrate parameningeal inflammation or meningitis. Noncontrast CT imaging can be normal early but may later show increased density, filling defects with contrast, dilation of the superior ophthalmic vein, intracranial hemorrhage, or signs of raised intracranial pressure. MRI with MR venography is the diagnostic modality of choice, allowing direct visualization of thrombus and venous structures at all stages of disease.
Alternative Diagnoses
Consider meningitis or encephalitis, intracranial abscess, orbital or periorbital cellulitis, carotid artery aneurysm or fistula, pseudotumor cerebri, acute angle-closure glaucoma, intracranial hemorrhage, and Tolosa–Hunt syndrome.
Emergency Stabilization
Patients may be critically ill and unstable. Immediate assessment and stabilization of airway, breathing, and circulation are essential, with early intubation for airway protection when mental status is impaired and aggressive fluid resuscitation for hemodynamic instability.
Definitive Emergency Management
Initiate broad-spectrum intravenous antibiotics promptly to cover gram-positive organisms including MRSA, gram-negative organisms, and anaerobes, typically using vancomycin or nafcillin combined with a third-generation cephalosporin and metronidazole or clindamycin when indicated. Anticoagulation with heparin may limit clot propagation and improve outcomes, though its use remains controversial and requires exclusion of intracranial hemorrhage prior to initiation. Endovascular thrombolysis may be considered in refractory, severe cases. Systemic corticosteroids may be beneficial in selected patients, particularly with pituitary involvement or inflammatory etiologies. Surgical consultation is required for drainage of the primary infectious source, such as sinus or dental abscesses, and intracranial pressure should be managed aggressively when elevated.
Disposition and Follow-Up
All patients with cavernous sinus thrombosis require hospital admission to a monitored setting, often the intensive care unit. Neurology and neurosurgical consultation are mandatory, and discharge from the emergency department is not appropriate.
Complications and Clinical Cautions
Potential complications include permanent visual impairment, persistent cranial nerve palsies, meningitis, intracranial abscess, seizures, pituitary necrosis with endocrine insufficiency, septic emboli, sepsis, and shock. Mortality remains significant. Maintain a high index of suspicion in patients with recent ENT infections, refractory headache, ocular findings, or hypercoagulable risk factors, as early CT imaging may be misleadingly normal and MRI/MRV should be pursued promptly.
Overview
Cavernous sinus thrombosis is thrombosis within a major intracranial venous drainage pathway and is most often infectious in origin. Infection commonly spreads from facial, odontogenic, or paranasal sinus sources, with hematogenous or contiguous extension. Less frequently, thrombosis occurs in the setting of hypercoagulable states. The cavernous sinus lies superolateral to the sphenoid sinus and surrounds the sella; cranial nerves III, IV, V1, and V2 course within its lateral wall, while cranial nerve VI and the internal carotid artery run medially. Although the cavernous sinus is most often involved, the transverse and superior sagittal sinuses may also be affected.
Pathophysiologic Mechanisms
Infection spreads hematogenously from facial, otic, or neck sources or directly from infected sinus cavities, most commonly sphenoid and ethmoid sinuses. Bacterial proliferation triggers inflammation and coagulation, leading to venous thrombosis. Resulting venous congestion affects adjacent neurovascular structures, producing ophthalmoplegia from involvement of cranial nerves III, IV, or VI, pupillary abnormalities from cranial nerve III dysfunction, and sensory deficits of the forehead or cheek from cranial nerves V1 and V2.
Causative Factors
Septic thrombosis is most common, with Staphylococcus aureus responsible for approximately 70% of cases; Streptococcus pneumoniae, gram-negative organisms, and anaerobes are also implicated. Fungal causes such as Aspergillus and Rhizopus are less frequent. Aseptic causes include granulomatous disease such as tuberculosis, inflammatory disorders, mass effect from skull-base tumors or aneurysms, and hypercoagulable states.
Clinical Presentation
Headache is present in the majority of patients, often accompanied by fever, ocular or retrobulbar pain, facial swelling, visual disturbances, facial dysesthesia, and lethargy or altered mental status. Early physical findings include periorbital edema and chemosis with retinal venous congestion, followed by ptosis, proptosis, and ophthalmoplegia. Cranial nerve deficits are common, particularly lateral gaze palsy from cranial nerve VI involvement and sensory changes in V1 or V2 distributions. Advanced disease may present with meningismus, seizures, coma, or septic shock.
Risk-Oriented History
High-risk features include recent facial trauma, ENT or neurosurgical procedures, manipulation of central facial furuncles, diabetes, or immunocompromised states such as HIV infection, chronic steroid use, or malignancy. Pediatric patients may present with nonspecific symptoms including fever, vomiting, lethargy, or signs of increased intracranial pressure, particularly following otitis or pharyngitis; neonatal cases are especially challenging to diagnose.
Initial Clinical Assessment
Diagnosis is primarily clinical, suggested by venous congestion, ocular findings, unilateral symptoms that rapidly progress to bilateral involvement, and overall toxic appearance. Laboratory studies are supportive but nonspecific, and early imaging findings may be subtle.
Diagnostic Evaluation
Laboratory testing may show leukocytosis, bandemia, and elevated ESR or D-dimer, but lacks sensitivity and specificity. Cerebrospinal fluid analysis may demonstrate parameningeal inflammation or meningitis. Noncontrast CT imaging can be normal early but may later show increased density, filling defects with contrast, dilation of the superior ophthalmic vein, intracranial hemorrhage, or signs of raised intracranial pressure. MRI with MR venography is the diagnostic modality of choice, allowing direct visualization of thrombus and venous structures at all stages of disease.
Alternative Diagnoses
Consider meningitis or encephalitis, intracranial abscess, orbital or periorbital cellulitis, carotid artery aneurysm or fistula, pseudotumor cerebri, acute angle-closure glaucoma, intracranial hemorrhage, and Tolosa–Hunt syndrome.
Emergency Stabilization
Patients may be critically ill and unstable. Immediate assessment and stabilization of airway, breathing, and circulation are essential, with early intubation for airway protection when mental status is impaired and aggressive fluid resuscitation for hemodynamic instability.
Definitive Emergency Management
Initiate broad-spectrum intravenous antibiotics promptly to cover gram-positive organisms including MRSA, gram-negative organisms, and anaerobes, typically using vancomycin or nafcillin combined with a third-generation cephalosporin and metronidazole or clindamycin when indicated. Anticoagulation with heparin may limit clot propagation and improve outcomes, though its use remains controversial and requires exclusion of intracranial hemorrhage prior to initiation. Endovascular thrombolysis may be considered in refractory, severe cases. Systemic corticosteroids may be beneficial in selected patients, particularly with pituitary involvement or inflammatory etiologies. Surgical consultation is required for drainage of the primary infectious source, such as sinus or dental abscesses, and intracranial pressure should be managed aggressively when elevated.
Disposition and Follow-Up
All patients with cavernous sinus thrombosis require hospital admission to a monitored setting, often the intensive care unit. Neurology and neurosurgical consultation are mandatory, and discharge from the emergency department is not appropriate.
Complications and Clinical Cautions
Potential complications include permanent visual impairment, persistent cranial nerve palsies, meningitis, intracranial abscess, seizures, pituitary necrosis with endocrine insufficiency, septic emboli, sepsis, and shock. Mortality remains significant. Maintain a high index of suspicion in patients with recent ENT infections, refractory headache, ocular findings, or hypercoagulable risk factors, as early CT imaging may be misleadingly normal and MRI/MRV should be pursued promptly.