- Published on
Emergency And Acute Medicine – Chronic Obstructive Pulmonary Disease
Overview And Disease Process
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death in the United States and affects approximately 10% of the population, including nearly half of long-term smokers. It is characterized by persistent airflow limitation resulting from a combination of emphysema, chronic bronchitis, and components of reactive airway disease. Emphysema involves irreversible alveolar destruction with loss of elastic recoil, while chronic bronchitis is defined by airway inflammation without alveolar damage. Reactive airway disease contributes reversible bronchospasm, mucus plugging, and mucosal edema. Patients frequently have comorbid hypertension, diabetes, heart failure, and cardiovascular disease. Recurrent exacerbations are associated with increased mortality, faster decline in lung function, poorer quality of life, and higher rates of hospitalization.
Risk Factors And Causes
Cigarette smoking is the primary cause, with COPD developing in approximately 15% of smokers. Additional risk factors include air pollution, airway hyperresponsiveness, genetic conditions such as α1-antitrypsin deficiency, and possible autoimmune mechanisms. Acute exacerbations are most commonly triggered by infections. Viral infections account for more than half of exacerbations, particularly rhinovirus and respiratory syncytial virus. Bacterial pathogens are isolated in 40–60% of cases, most often Haemophilus influenzae, Moraxella catarrhalis, and Streptococcus pneumoniae. Exacerbations are more likely when dyspnea worsens, sputum volume increases, and sputum becomes purulent. Environmental pollutants, reduced immunity, and seasonal variation—especially winter months—also contribute.
Clinical Presentation
Patients commonly report progressive dyspnea on exertion, chronic cough, sputum production, wheezing, fatigue, and sometimes orthopnea. In advanced cases, altered mental status may occur due to carbon dioxide retention. Physical examination may reveal wheezing, prolonged expiratory phase, decreased air movement, use of accessory muscles, barrel chest, cyanosis, jugular venous distension, peripheral edema, and cardiac gallops. Severe disease may lead to carbon dioxide narcosis with confusion or somnolence.
Diagnostic Evaluation
Laboratory studies may show secondary polycythemia from chronic hypoxemia or leukocytosis during infectious exacerbations. Arterial blood gas analysis often demonstrates hypercapnia with or without acidosis and impaired oxygenation. β-natriuretic peptide testing may help differentiate COPD exacerbation from heart failure. Chest radiography is used to identify pneumonia, pneumothorax, heart failure, or lobar collapse, while computed tomography is reserved for suspected pulmonary embolism or further disease characterization. Pulse oximetry, electrocardiography, pulmonary function testing, and echocardiography are useful adjuncts depending on clinical context.
Differential Diagnosis
Conditions that may mimic or coexist with a COPD exacerbation include pneumothorax, pneumonia, congestive heart failure, pulmonary embolism, asthma, upper airway obstruction, restrictive lung disease, acute respiratory distress syndrome, pleural effusion, acute coronary syndrome, pericardial effusion, and metabolic derangements.
Early And Emergency Management
Initial prehospital and emergency care focuses on supplemental oxygen and rapid bronchodilation. Oxygen should not be withheld due to fear of carbon dioxide retention; instead, patients should be closely monitored. In the emergency department, oxygen therapy is titrated to maintain oxygen saturation above 90–92%, with careful observation for hypoventilation. Noninvasive positive pressure ventilation is the preferred method of ventilatory support for hypercapnic respiratory failure and can often prevent intubation. Endotracheal intubation is reserved for patients with clinical fatigue, worsening mental status, inability to tolerate therapy, or ineffective ventilation.
Definitive Treatment
Management includes continuous cardiac and oxygen monitoring, inhaled short-acting β-agonists and anticholinergics, and systemic corticosteroids to reduce airway inflammation and relapse risk. Antibiotics are indicated when fever, increased sputum production, or worsening dyspnea suggests bacterial infection, with macrolides offering potential additional anti-inflammatory benefit. Ventilator strategies should allow sufficient expiratory time to minimize air trapping, accepting permissive hypercapnia when necessary.
Disposition And Follow-Up
Intensive care admission is required for patients needing intubation, those with severe acidosis, refractory hypoxemia, carbon dioxide narcosis, or significant comorbid cardiac or pulmonary disease. Hospital admission is appropriate for patients with pneumonia, lobar collapse, increased work of breathing, or failure to improve with emergency treatment. Discharge may be considered for mild exacerbations that resolve in the emergency department with stable oxygen saturation above 92%. Long-term management includes smoking cessation, vaccination against influenza and pneumococcus, trigger avoidance, and consideration of specialist referral for advanced therapies such as lung volume reduction surgery.
Clinical Pearls And Pitfalls
Noninvasive positive pressure ventilation is the therapy of choice when optimal medical treatment is insufficient. Patients with COPD are at increased risk for cardiovascular disease, diabetes, and hypertension, emphasizing the importance of preventive care. Routine immunization and early recognition of exacerbations are essential to improving outcomes.
Overview And Disease Process
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death in the United States and affects approximately 10% of the population, including nearly half of long-term smokers. It is characterized by persistent airflow limitation resulting from a combination of emphysema, chronic bronchitis, and components of reactive airway disease. Emphysema involves irreversible alveolar destruction with loss of elastic recoil, while chronic bronchitis is defined by airway inflammation without alveolar damage. Reactive airway disease contributes reversible bronchospasm, mucus plugging, and mucosal edema. Patients frequently have comorbid hypertension, diabetes, heart failure, and cardiovascular disease. Recurrent exacerbations are associated with increased mortality, faster decline in lung function, poorer quality of life, and higher rates of hospitalization.
Risk Factors And Causes
Cigarette smoking is the primary cause, with COPD developing in approximately 15% of smokers. Additional risk factors include air pollution, airway hyperresponsiveness, genetic conditions such as α1-antitrypsin deficiency, and possible autoimmune mechanisms. Acute exacerbations are most commonly triggered by infections. Viral infections account for more than half of exacerbations, particularly rhinovirus and respiratory syncytial virus. Bacterial pathogens are isolated in 40–60% of cases, most often Haemophilus influenzae, Moraxella catarrhalis, and Streptococcus pneumoniae. Exacerbations are more likely when dyspnea worsens, sputum volume increases, and sputum becomes purulent. Environmental pollutants, reduced immunity, and seasonal variation—especially winter months—also contribute.
Clinical Presentation
Patients commonly report progressive dyspnea on exertion, chronic cough, sputum production, wheezing, fatigue, and sometimes orthopnea. In advanced cases, altered mental status may occur due to carbon dioxide retention. Physical examination may reveal wheezing, prolonged expiratory phase, decreased air movement, use of accessory muscles, barrel chest, cyanosis, jugular venous distension, peripheral edema, and cardiac gallops. Severe disease may lead to carbon dioxide narcosis with confusion or somnolence.
Diagnostic Evaluation
Laboratory studies may show secondary polycythemia from chronic hypoxemia or leukocytosis during infectious exacerbations. Arterial blood gas analysis often demonstrates hypercapnia with or without acidosis and impaired oxygenation. β-natriuretic peptide testing may help differentiate COPD exacerbation from heart failure. Chest radiography is used to identify pneumonia, pneumothorax, heart failure, or lobar collapse, while computed tomography is reserved for suspected pulmonary embolism or further disease characterization. Pulse oximetry, electrocardiography, pulmonary function testing, and echocardiography are useful adjuncts depending on clinical context.
Differential Diagnosis
Conditions that may mimic or coexist with a COPD exacerbation include pneumothorax, pneumonia, congestive heart failure, pulmonary embolism, asthma, upper airway obstruction, restrictive lung disease, acute respiratory distress syndrome, pleural effusion, acute coronary syndrome, pericardial effusion, and metabolic derangements.
Early And Emergency Management
Initial prehospital and emergency care focuses on supplemental oxygen and rapid bronchodilation. Oxygen should not be withheld due to fear of carbon dioxide retention; instead, patients should be closely monitored. In the emergency department, oxygen therapy is titrated to maintain oxygen saturation above 90–92%, with careful observation for hypoventilation. Noninvasive positive pressure ventilation is the preferred method of ventilatory support for hypercapnic respiratory failure and can often prevent intubation. Endotracheal intubation is reserved for patients with clinical fatigue, worsening mental status, inability to tolerate therapy, or ineffective ventilation.
Definitive Treatment
Management includes continuous cardiac and oxygen monitoring, inhaled short-acting β-agonists and anticholinergics, and systemic corticosteroids to reduce airway inflammation and relapse risk. Antibiotics are indicated when fever, increased sputum production, or worsening dyspnea suggests bacterial infection, with macrolides offering potential additional anti-inflammatory benefit. Ventilator strategies should allow sufficient expiratory time to minimize air trapping, accepting permissive hypercapnia when necessary.
Disposition And Follow-Up
Intensive care admission is required for patients needing intubation, those with severe acidosis, refractory hypoxemia, carbon dioxide narcosis, or significant comorbid cardiac or pulmonary disease. Hospital admission is appropriate for patients with pneumonia, lobar collapse, increased work of breathing, or failure to improve with emergency treatment. Discharge may be considered for mild exacerbations that resolve in the emergency department with stable oxygen saturation above 92%. Long-term management includes smoking cessation, vaccination against influenza and pneumococcus, trigger avoidance, and consideration of specialist referral for advanced therapies such as lung volume reduction surgery.
Clinical Pearls And Pitfalls
Noninvasive positive pressure ventilation is the therapy of choice when optimal medical treatment is insufficient. Patients with COPD are at increased risk for cardiovascular disease, diabetes, and hypertension, emphasizing the importance of preventive care. Routine immunization and early recognition of exacerbations are essential to improving outcomes.

- Published on
Emergency and Acute Medicine – Cholelithiasis
Overview and mechanism
Cholelithiasis refers to the presence of gallstones that become symptomatic when they obstruct the cystic duct or common bile duct, disrupting normal bile flow and triggering gallbladder spasm. This produces the characteristic pain of biliary colic. A related functional disorder, biliary dyskinesia, causes identical symptoms despite the absence of stones. When stones migrate into the common bile duct (choledocholithiasis), pain may be more prolonged and is often accompanied by abnormal liver function tests and bilirubin elevation, with risk of complications such as cholangitis or pancreatitis.
Causes and risk factors
Most gallstones are cholesterol stones, which develop when bile becomes supersaturated with cholesterol. Pigment stones account for about one fifth of cases and consist mainly of calcium bilirubinate; they are commonly associated with hemolytic disorders that increase unconjugated bilirubin levels. The incidence of gallstones rises with age and is higher in females, with additional risk factors including obesity, pregnancy, rapid weight loss, Hispanic ethnicity, and medications that promote biliary stasis such as oral contraceptives or ceftriaxone. In children, gallstones are rare and are usually linked to hemolytic anemias such as sickle cell disease or hereditary spherocytosis. Biliary sludge, a nonstone crystalline material, may also cause biliary colic and is associated with pregnancy, rapid weight loss, certain medications, and organ transplantation. Chronic obstruction with calcium deposition can lead to a porcelain gallbladder, a condition associated with an increased risk of gallbladder carcinoma.
Clinical presentation
Patients typically describe dull, aching epigastric or right upper quadrant pain that develops gradually over several minutes, persists for 30 minutes to several hours, and then resolves. The pain often radiates to the right scapula, shoulder, or thoracic spine and is frequently triggered by a large or fatty meal. Associated symptoms include anorexia, nausea, and vomiting. Patients are usually afebrile; the presence of fever or chills suggests a complication such as cholecystitis or cholangitis.
Examination findings
On examination, there is tenderness to deep palpation in the right upper quadrant without rebound or guarding. A Murphy sign may be present during an active episode of biliary colic but should resolve once the pain subsides.
Initial evaluation
Assessment includes exclusion of cardiac causes when appropriate, along with basic laboratory testing such as a complete blood count, liver function tests, pancreatic enzymes, urinalysis, and pregnancy testing when indicated. These tests help distinguish uncomplicated biliary colic from complications involving infection, obstruction, or pancreatitis.
Diagnostic studies
Laboratory studies are often normal in uncomplicated cholelithiasis. Leukocytosis or significant liver enzyme abnormalities suggest cholecystitis, cholangitis, or common bile duct obstruction. Ultrasound is the imaging modality of choice, with high sensitivity and specificity for gallstones and the ability to assess bile duct dilation and gallbladder wall changes. Hepatobiliary scintigraphy is useful when cholecystitis is suspected but ultrasound findings are equivocal, though it does not directly visualize stones. Computed tomography is less sensitive for gallstones but may identify complications or alternative diagnoses.
Differential considerations
Conditions that can mimic biliary colic include myocardial infarction, abdominal aortic aneurysm, acute cholecystitis, cholangitis, pancreatitis, renal colic, peptic ulcer disease, pneumonia involving the right lower lobe, hepatitis, and other intra-abdominal emergencies.
Early management
Initial treatment focuses on supportive care. Intravenous access and fluids are provided for patients with vomiting or dehydration, and oral intake is withheld during acute symptoms. Pain control is essential, often with parenteral nonsteroidal anti-inflammatory drugs or opioids combined with antiemetics once the diagnosis is reasonably secure.
Emergency department care
Hydration, analgesia, and antiemetics form the mainstay of treatment for uncomplicated biliary colic. Anticholinergic agents have not demonstrated benefit. Ongoing reassessment is required to ensure symptoms resolve and that no complications develop.
Disposition and follow-up
Patients should be admitted and receive surgical or gastroenterology consultation if there is evidence of cholecystitis, cholangitis, common bile duct obstruction, or gallstone pancreatitis. Discharge may be considered when pain has fully resolved, laboratory and imaging studies show no complications, and the patient can tolerate oral intake. All patients with symptomatic gallstones require referral for surgical evaluation, and those with choledocholithiasis need gastroenterology follow-up.
Clinical pearls
Gallstones detected incidentally on imaging may not be the cause of abdominal pain, so alternative diagnoses must always be considered. Ultrasound is the most accurate initial test for gallstones, while hepatobiliary scintigraphy is particularly useful for diagnosing cystic duct obstruction and acute cholecystitis. Computed tomography may miss non-radiopaque stones and should not be relied upon alone for diagnosis.
Overview and mechanism
Cholelithiasis refers to the presence of gallstones that become symptomatic when they obstruct the cystic duct or common bile duct, disrupting normal bile flow and triggering gallbladder spasm. This produces the characteristic pain of biliary colic. A related functional disorder, biliary dyskinesia, causes identical symptoms despite the absence of stones. When stones migrate into the common bile duct (choledocholithiasis), pain may be more prolonged and is often accompanied by abnormal liver function tests and bilirubin elevation, with risk of complications such as cholangitis or pancreatitis.
Causes and risk factors
Most gallstones are cholesterol stones, which develop when bile becomes supersaturated with cholesterol. Pigment stones account for about one fifth of cases and consist mainly of calcium bilirubinate; they are commonly associated with hemolytic disorders that increase unconjugated bilirubin levels. The incidence of gallstones rises with age and is higher in females, with additional risk factors including obesity, pregnancy, rapid weight loss, Hispanic ethnicity, and medications that promote biliary stasis such as oral contraceptives or ceftriaxone. In children, gallstones are rare and are usually linked to hemolytic anemias such as sickle cell disease or hereditary spherocytosis. Biliary sludge, a nonstone crystalline material, may also cause biliary colic and is associated with pregnancy, rapid weight loss, certain medications, and organ transplantation. Chronic obstruction with calcium deposition can lead to a porcelain gallbladder, a condition associated with an increased risk of gallbladder carcinoma.
Clinical presentation
Patients typically describe dull, aching epigastric or right upper quadrant pain that develops gradually over several minutes, persists for 30 minutes to several hours, and then resolves. The pain often radiates to the right scapula, shoulder, or thoracic spine and is frequently triggered by a large or fatty meal. Associated symptoms include anorexia, nausea, and vomiting. Patients are usually afebrile; the presence of fever or chills suggests a complication such as cholecystitis or cholangitis.
Examination findings
On examination, there is tenderness to deep palpation in the right upper quadrant without rebound or guarding. A Murphy sign may be present during an active episode of biliary colic but should resolve once the pain subsides.
Initial evaluation
Assessment includes exclusion of cardiac causes when appropriate, along with basic laboratory testing such as a complete blood count, liver function tests, pancreatic enzymes, urinalysis, and pregnancy testing when indicated. These tests help distinguish uncomplicated biliary colic from complications involving infection, obstruction, or pancreatitis.
Diagnostic studies
Laboratory studies are often normal in uncomplicated cholelithiasis. Leukocytosis or significant liver enzyme abnormalities suggest cholecystitis, cholangitis, or common bile duct obstruction. Ultrasound is the imaging modality of choice, with high sensitivity and specificity for gallstones and the ability to assess bile duct dilation and gallbladder wall changes. Hepatobiliary scintigraphy is useful when cholecystitis is suspected but ultrasound findings are equivocal, though it does not directly visualize stones. Computed tomography is less sensitive for gallstones but may identify complications or alternative diagnoses.
Differential considerations
Conditions that can mimic biliary colic include myocardial infarction, abdominal aortic aneurysm, acute cholecystitis, cholangitis, pancreatitis, renal colic, peptic ulcer disease, pneumonia involving the right lower lobe, hepatitis, and other intra-abdominal emergencies.
Early management
Initial treatment focuses on supportive care. Intravenous access and fluids are provided for patients with vomiting or dehydration, and oral intake is withheld during acute symptoms. Pain control is essential, often with parenteral nonsteroidal anti-inflammatory drugs or opioids combined with antiemetics once the diagnosis is reasonably secure.
Emergency department care
Hydration, analgesia, and antiemetics form the mainstay of treatment for uncomplicated biliary colic. Anticholinergic agents have not demonstrated benefit. Ongoing reassessment is required to ensure symptoms resolve and that no complications develop.
Disposition and follow-up
Patients should be admitted and receive surgical or gastroenterology consultation if there is evidence of cholecystitis, cholangitis, common bile duct obstruction, or gallstone pancreatitis. Discharge may be considered when pain has fully resolved, laboratory and imaging studies show no complications, and the patient can tolerate oral intake. All patients with symptomatic gallstones require referral for surgical evaluation, and those with choledocholithiasis need gastroenterology follow-up.
Clinical pearls
Gallstones detected incidentally on imaging may not be the cause of abdominal pain, so alternative diagnoses must always be considered. Ultrasound is the most accurate initial test for gallstones, while hepatobiliary scintigraphy is particularly useful for diagnosing cystic duct obstruction and acute cholecystitis. Computed tomography may miss non-radiopaque stones and should not be relied upon alone for diagnosis.
- Published on
Emergency and acute medicine – acute cholecystitis
Definition and pathogenesis
Acute cholecystitis refers to inflammation of the gallbladder, most often resulting from obstruction of bile flow. The condition is usually precipitated by prolonged blockage of the gallbladder neck or cystic duct, leading to bile stasis, rising intraluminal pressure, mucosal injury, and subsequent inflammatory changes such as edema and increased vascularity.
Underlying causes
The most common form is acute calculous cholecystitis, caused by gallstone obstruction in the gallbladder neck, cystic duct, or occasionally the common bile duct. Secondary bacterial infection with coliforms and anaerobes may occur, although their primary role remains debated. Acalculous cholecystitis accounts for roughly 10% of cases and typically develops in critically ill patients due to biliary stasis and gallbladder ischemia, followed by inflammation and infection. In children, calculous cholecystitis is rare, whereas the acalculous form is more common and often associated with systemic infections such as sepsis, scarlet fever, Kawasaki disease, or parasitic illness.
Clinical features
Patients with calculous cholecystitis usually present with dull, aching epigastric or right upper quadrant pain that may radiate to the right scapula, shoulder, or thoracic spine. Pain persisting longer than six hours favors cholecystitis over uncomplicated biliary colic. As inflammation progresses, pain becomes sharper and more localized due to parietal peritoneal irritation. Nausea, vomiting, fever, and chills are common but not universal, and jaundice occurs in a minority of patients. A history of prior biliary colic or known gallstones supports the diagnosis. In contrast, acalculous cholecystitis often presents atypically in critically ill patients, with minimal localized abdominal pain and features of sepsis without an obvious source.
Physical examination findings
Localized right upper quadrant tenderness with percussion sensitivity or rebound may develop as inflammation advances. A positive Murphy sign—sudden inspiratory arrest during gentle palpation of the right upper quadrant—is present in most cases. In severe disease, signs of peritonitis or systemic toxicity may be evident.
Initial evaluation
Essential investigations include a complete blood count, liver function tests, amylase and lipase, urinalysis, and pregnancy testing when appropriate. Electrocardiography is recommended in patients at risk for coronary artery disease to exclude cardiac causes of pain. Imaging with right upper quadrant ultrasound is the preferred initial diagnostic test, with hepatobiliary scintigraphy reserved for equivocal cases or suspected acalculous cholecystitis.
Laboratory and imaging characteristics
Leukocytosis supports the diagnosis but may be absent in many patients. Liver enzymes and pancreatic markers are usually normal or only mildly elevated; disproportionate elevations in bilirubin or alkaline phosphatase raise concern for common bile duct obstruction or cholangitis. Ultrasound typically demonstrates gallbladder wall thickening, pericholecystic fluid, or gallstones and has high sensitivity and specificity. Hepatobiliary scintigraphy is highly sensitive and specific when ultrasound findings are inconclusive. CT imaging is useful to exclude complications such as perforation, emphysematous cholecystitis, or alternative intra-abdominal pathology.
Diagnostic considerations
Conditions that may mimic acute cholecystitis include biliary colic, cholangitis, hepatitis, hepatic abscess, pancreatitis, peptic ulcer disease, intestinal perforation, right lower lobe pneumonia, myocardial infarction, abdominal aortic aneurysm, appendicitis, and pyelonephritis.
Early management
Initial treatment focuses on supportive care, including intravenous access, fluid resuscitation for dehydration or sepsis, supplemental oxygen, and cardiac monitoring until myocardial ischemia is excluded. Patients should be kept nil per os, with nasogastric decompression if vomiting or ileus is present.
Emergency department therapy
Broad-spectrum intravenous antibiotics covering gram-negative coliforms, anaerobes, and Enterococcus species should be started promptly. Suitable regimens include beta-lactam/beta-lactamase inhibitor combinations, with aminoglycosides added if sepsis or cholangitis is suspected. Alternative regimens are required for patients with penicillin allergy. Antiemetics and opioid analgesics may be administered once the diagnosis is reasonably secure, with caution regarding sphincter of Oddi spasm. Early surgical consultation is mandatory.
Disposition and follow-up
All patients with acute cholecystitis require hospital admission for intravenous antibiotics, analgesia, fluid management, and definitive surgical treatment, typically cholecystectomy within 24–72 hours. Unstable patients or those with complications such as perforation or sepsis require urgent operative intervention. Discharge from the emergency department is not appropriate.
Clinical pearls
Ultrasound is the first-line imaging modality in suspected cholecystitis. Hepatobiliary scintigraphy should be obtained when ultrasound is inconclusive or acalculous cholecystitis is suspected. Early recognition, prompt antibiotics, and timely surgical involvement are essential to prevent complications.
Definition and pathogenesis
Acute cholecystitis refers to inflammation of the gallbladder, most often resulting from obstruction of bile flow. The condition is usually precipitated by prolonged blockage of the gallbladder neck or cystic duct, leading to bile stasis, rising intraluminal pressure, mucosal injury, and subsequent inflammatory changes such as edema and increased vascularity.
Underlying causes
The most common form is acute calculous cholecystitis, caused by gallstone obstruction in the gallbladder neck, cystic duct, or occasionally the common bile duct. Secondary bacterial infection with coliforms and anaerobes may occur, although their primary role remains debated. Acalculous cholecystitis accounts for roughly 10% of cases and typically develops in critically ill patients due to biliary stasis and gallbladder ischemia, followed by inflammation and infection. In children, calculous cholecystitis is rare, whereas the acalculous form is more common and often associated with systemic infections such as sepsis, scarlet fever, Kawasaki disease, or parasitic illness.
Clinical features
Patients with calculous cholecystitis usually present with dull, aching epigastric or right upper quadrant pain that may radiate to the right scapula, shoulder, or thoracic spine. Pain persisting longer than six hours favors cholecystitis over uncomplicated biliary colic. As inflammation progresses, pain becomes sharper and more localized due to parietal peritoneal irritation. Nausea, vomiting, fever, and chills are common but not universal, and jaundice occurs in a minority of patients. A history of prior biliary colic or known gallstones supports the diagnosis. In contrast, acalculous cholecystitis often presents atypically in critically ill patients, with minimal localized abdominal pain and features of sepsis without an obvious source.
Physical examination findings
Localized right upper quadrant tenderness with percussion sensitivity or rebound may develop as inflammation advances. A positive Murphy sign—sudden inspiratory arrest during gentle palpation of the right upper quadrant—is present in most cases. In severe disease, signs of peritonitis or systemic toxicity may be evident.
Initial evaluation
Essential investigations include a complete blood count, liver function tests, amylase and lipase, urinalysis, and pregnancy testing when appropriate. Electrocardiography is recommended in patients at risk for coronary artery disease to exclude cardiac causes of pain. Imaging with right upper quadrant ultrasound is the preferred initial diagnostic test, with hepatobiliary scintigraphy reserved for equivocal cases or suspected acalculous cholecystitis.
Laboratory and imaging characteristics
Leukocytosis supports the diagnosis but may be absent in many patients. Liver enzymes and pancreatic markers are usually normal or only mildly elevated; disproportionate elevations in bilirubin or alkaline phosphatase raise concern for common bile duct obstruction or cholangitis. Ultrasound typically demonstrates gallbladder wall thickening, pericholecystic fluid, or gallstones and has high sensitivity and specificity. Hepatobiliary scintigraphy is highly sensitive and specific when ultrasound findings are inconclusive. CT imaging is useful to exclude complications such as perforation, emphysematous cholecystitis, or alternative intra-abdominal pathology.
Diagnostic considerations
Conditions that may mimic acute cholecystitis include biliary colic, cholangitis, hepatitis, hepatic abscess, pancreatitis, peptic ulcer disease, intestinal perforation, right lower lobe pneumonia, myocardial infarction, abdominal aortic aneurysm, appendicitis, and pyelonephritis.
Early management
Initial treatment focuses on supportive care, including intravenous access, fluid resuscitation for dehydration or sepsis, supplemental oxygen, and cardiac monitoring until myocardial ischemia is excluded. Patients should be kept nil per os, with nasogastric decompression if vomiting or ileus is present.
Emergency department therapy
Broad-spectrum intravenous antibiotics covering gram-negative coliforms, anaerobes, and Enterococcus species should be started promptly. Suitable regimens include beta-lactam/beta-lactamase inhibitor combinations, with aminoglycosides added if sepsis or cholangitis is suspected. Alternative regimens are required for patients with penicillin allergy. Antiemetics and opioid analgesics may be administered once the diagnosis is reasonably secure, with caution regarding sphincter of Oddi spasm. Early surgical consultation is mandatory.
Disposition and follow-up
All patients with acute cholecystitis require hospital admission for intravenous antibiotics, analgesia, fluid management, and definitive surgical treatment, typically cholecystectomy within 24–72 hours. Unstable patients or those with complications such as perforation or sepsis require urgent operative intervention. Discharge from the emergency department is not appropriate.
Clinical pearls
Ultrasound is the first-line imaging modality in suspected cholecystitis. Hepatobiliary scintigraphy should be obtained when ultrasound is inconclusive or acalculous cholecystitis is suspected. Early recognition, prompt antibiotics, and timely surgical involvement are essential to prevent complications.

- Published on
Emergency and acute medicine – acute cholangitis
Overview and pathophysiology
Acute cholangitis is a purulent infection of the biliary tree that develops when there is partial or complete obstruction of the common bile duct. Obstruction may be caused by gallstones, tumors, cysts, or strictures, leading to increased intraluminal pressure and bacterial overgrowth. This process commonly results in bacteremia and sepsis and may extend to involve the liver and gallbladder. Mirizzi syndrome refers to bile duct obstruction caused by extrinsic compression from gallbladder or cystic duct stones or edema.
Causative factors
Infection typically arises from ascending bacteria originating in the duodenum, gallbladder infection, portal venous seeding, hematogenous spread with hepatic secretion, or lymphatic spread. Common organisms include intestinal coliforms such as Escherichia coli, Enterococcus species, and anaerobes including Bacteroides and Clostridium. In patients with AIDS, sclerosing cholangitis may occur, characterized by papillary stenosis, sclerosing cholangitis, and extrahepatic biliary obstruction; organisms such as cytomegalovirus, Cryptosporidium, and microsporidia are frequently isolated, although their exact causal role remains uncertain.
Clinical presentation
The classic presentation is Charcot triad, consisting of fever with chills, right upper quadrant abdominal pain, and jaundice, although all three features are present in only about half of patients. Progression to hypotension and altered mental status indicates severe biliary sepsis, known as Reynolds pentad. Abdominal pain is present in most patients and usually localizes to the right upper quadrant. Fever is common, while clinically apparent jaundice may be absent in a significant proportion of cases. In AIDS-related cholangitis, symptoms tend to be more indolent, with relatively normal bilirubin levels.
Initial evaluation
Early evaluation should include assessment for sepsis and organ dysfunction. Recommended studies include complete blood count, liver function tests, amylase and lipase, urinalysis, blood cultures, and electrocardiography in patients at risk for cardiac disease. Right upper quadrant ultrasound is the initial imaging study of choice to assess for biliary dilation and gallstones, with hepatobiliary scintigraphy considered when ultrasound findings are inconclusive.
Laboratory and imaging findings
Laboratory testing typically demonstrates leukocytosis with a left shift, unless the patient is immunocompromised or in advanced sepsis. Liver function tests show a cholestatic pattern with elevated direct bilirubin and alkaline phosphatase, while transaminase elevations are usually mild. Amylase and lipase are normal or only slightly elevated. Ultrasound helps identify the level of obstruction and gallstone etiology. Hepatobiliary scintigraphy is sensitive early in the disease before ductal dilation develops. CT imaging may assist in excluding alternative diagnoses. MR cholangiopancreatography is highly accurate but generally unnecessary if therapeutic ERCP is planned.
Differential considerations
Conditions that may mimic cholangitis include acute cholecystitis, hepatitis, hepatic abscess, acute pancreatitis, right-sided pyelonephritis, right lower lobe pneumonia or pulmonary embolism, perforated peptic ulcer, appendicitis, and sepsis with nonspecific liver enzyme elevation.
Early management
Initial management focuses on aggressive treatment of sepsis. Prompt intravenous fluid resuscitation is essential to correct dehydration and hemodynamic compromise. Most patients show clinical improvement within the first 24 hours of appropriate antibiotic therapy. Vasopressors may be required for hypotension refractory to fluids.
Emergency department treatment
Broad-spectrum intravenous antibiotics should be initiated early to cover gram-negative coliforms, anaerobes, and Enterococcus. Acceptable regimens include beta-lactam/beta-lactamase inhibitor combinations, carbapenems, or combination therapy with an aminoglycoside. Alternative regimens should be used in patients with penicillin allergy or renal insufficiency. Patients should be kept nil per os, with nasogastric decompression if vomiting or ileus is present. Analgesia and antiemetics may be provided once hemodynamic stability is ensured. Early gastroenterology and surgical consultation is mandatory. If there is no clinical response within 12–24 hours, urgent biliary decompression via ERCP, percutaneous drainage, or surgery is required.
Disposition and follow-up
All patients with acute cholangitis require hospital admission, with intensive care unit placement for those with septic shock or organ failure. There are no criteria for emergency department discharge. Definitive management involves continued intravenous antibiotics and timely biliary drainage when indicated.
Key clinical points
Acute cholangitis is a medical emergency with high risk of sepsis. Early recognition, aggressive fluid resuscitation, prompt administration of broad-spectrum antibiotics, and rapid consultation for biliary drainage are critical to improving outcomes.
Overview and pathophysiology
Acute cholangitis is a purulent infection of the biliary tree that develops when there is partial or complete obstruction of the common bile duct. Obstruction may be caused by gallstones, tumors, cysts, or strictures, leading to increased intraluminal pressure and bacterial overgrowth. This process commonly results in bacteremia and sepsis and may extend to involve the liver and gallbladder. Mirizzi syndrome refers to bile duct obstruction caused by extrinsic compression from gallbladder or cystic duct stones or edema.
Causative factors
Infection typically arises from ascending bacteria originating in the duodenum, gallbladder infection, portal venous seeding, hematogenous spread with hepatic secretion, or lymphatic spread. Common organisms include intestinal coliforms such as Escherichia coli, Enterococcus species, and anaerobes including Bacteroides and Clostridium. In patients with AIDS, sclerosing cholangitis may occur, characterized by papillary stenosis, sclerosing cholangitis, and extrahepatic biliary obstruction; organisms such as cytomegalovirus, Cryptosporidium, and microsporidia are frequently isolated, although their exact causal role remains uncertain.
Clinical presentation
The classic presentation is Charcot triad, consisting of fever with chills, right upper quadrant abdominal pain, and jaundice, although all three features are present in only about half of patients. Progression to hypotension and altered mental status indicates severe biliary sepsis, known as Reynolds pentad. Abdominal pain is present in most patients and usually localizes to the right upper quadrant. Fever is common, while clinically apparent jaundice may be absent in a significant proportion of cases. In AIDS-related cholangitis, symptoms tend to be more indolent, with relatively normal bilirubin levels.
Initial evaluation
Early evaluation should include assessment for sepsis and organ dysfunction. Recommended studies include complete blood count, liver function tests, amylase and lipase, urinalysis, blood cultures, and electrocardiography in patients at risk for cardiac disease. Right upper quadrant ultrasound is the initial imaging study of choice to assess for biliary dilation and gallstones, with hepatobiliary scintigraphy considered when ultrasound findings are inconclusive.
Laboratory and imaging findings
Laboratory testing typically demonstrates leukocytosis with a left shift, unless the patient is immunocompromised or in advanced sepsis. Liver function tests show a cholestatic pattern with elevated direct bilirubin and alkaline phosphatase, while transaminase elevations are usually mild. Amylase and lipase are normal or only slightly elevated. Ultrasound helps identify the level of obstruction and gallstone etiology. Hepatobiliary scintigraphy is sensitive early in the disease before ductal dilation develops. CT imaging may assist in excluding alternative diagnoses. MR cholangiopancreatography is highly accurate but generally unnecessary if therapeutic ERCP is planned.
Differential considerations
Conditions that may mimic cholangitis include acute cholecystitis, hepatitis, hepatic abscess, acute pancreatitis, right-sided pyelonephritis, right lower lobe pneumonia or pulmonary embolism, perforated peptic ulcer, appendicitis, and sepsis with nonspecific liver enzyme elevation.
Early management
Initial management focuses on aggressive treatment of sepsis. Prompt intravenous fluid resuscitation is essential to correct dehydration and hemodynamic compromise. Most patients show clinical improvement within the first 24 hours of appropriate antibiotic therapy. Vasopressors may be required for hypotension refractory to fluids.
Emergency department treatment
Broad-spectrum intravenous antibiotics should be initiated early to cover gram-negative coliforms, anaerobes, and Enterococcus. Acceptable regimens include beta-lactam/beta-lactamase inhibitor combinations, carbapenems, or combination therapy with an aminoglycoside. Alternative regimens should be used in patients with penicillin allergy or renal insufficiency. Patients should be kept nil per os, with nasogastric decompression if vomiting or ileus is present. Analgesia and antiemetics may be provided once hemodynamic stability is ensured. Early gastroenterology and surgical consultation is mandatory. If there is no clinical response within 12–24 hours, urgent biliary decompression via ERCP, percutaneous drainage, or surgery is required.
Disposition and follow-up
All patients with acute cholangitis require hospital admission, with intensive care unit placement for those with septic shock or organ failure. There are no criteria for emergency department discharge. Definitive management involves continued intravenous antibiotics and timely biliary drainage when indicated.
Key clinical points
Acute cholangitis is a medical emergency with high risk of sepsis. Early recognition, aggressive fluid resuscitation, prompt administration of broad-spectrum antibiotics, and rapid consultation for biliary drainage are critical to improving outcomes.
- Published on
Emergency and acute medicine – penetrating chest trauma
Cause and mechanism
Penetrating chest trauma most commonly results from gunshot wounds or stab wounds. Less frequently, injury occurs from impalement on a sharp object following a fall or high-energy impact. These mechanisms place intrathoracic organs and major vessels at high risk for rapid deterioration.
Clinical features
Patients may present with an object impaled in the chest wall or an obvious penetrating wound with variable external bleeding. Common symptoms include chest pain, dyspnea, and respiratory distress. Altered mental status may occur secondary to hypoxemia or shock. Physical findings can include absent or asymmetric breath sounds, hypotension, and jugular venous distention, suggesting pneumothorax, hemothorax, or cardiac tamponade.
Initial evaluation
A rapid assessment of airway, breathing, and circulation is mandatory. The focused exam should evaluate respiratory effort, chest wall excursion, crepitus, subcutaneous emphysema, breath sounds, and heart sounds. An upright chest radiograph is preferred to identify pneumothorax, although a supine film should be obtained first if spinal precautions are required. Baseline hemoglobin, pulse oximetry, arterial blood gas, serum lactate, and type and screen should be obtained early.
Diagnostic studies
Echocardiography is indicated when tamponade is suspected or when a wound is near the heart. In penetrating precordial injuries, hemopericardium may decompress into the pleural space, so repeat pericardial ultrasound after chest tube placement is recommended. Electrocardiography assists in identifying myocardial injury. With gunshot wounds, imaging must account for all entry and exit sites, and additional studies of the abdomen or pelvis may be required. Arteriography is indicated if great vessel injury is suspected. Esophageal evaluation with contrast swallow or endoscopy and bronchoscopy should be considered when aerodigestive injury is possible.
Differential considerations
Life-threatening diagnoses include pneumothorax, tension or open pneumothorax, hemothorax, pulmonary contusion, myocardial contusion or rupture, pericardial tamponade, traumatic aortic injury, tracheobronchial or esophageal injury, diaphragmatic rupture, intra-abdominal injury, and spinal cord injury.
Prehospital priorities
All patients with signs of life should be transported rapidly to a trauma center. Full spinal immobilization is indicated when spinal injury is suspected. Impaled objects must never be removed in the field because they may be tamponading major bleeding. Suspected tension pneumothorax requires immediate needle decompression. Large open pneumothoraces should be covered with a three-sided occlusive dressing to prevent tension physiology. Transport should not be delayed for intravenous access.
Early resuscitation
Airway, breathing, and circulation management is the priority. Endotracheal intubation is indicated for respiratory distress, hypoxia, or hypotension. Supplemental oxygen should be provided to stable patients. Two large-bore peripheral IV lines should be established, with cautious fluid resuscitation. In penetrating aortic injury, permissive hypotension with a systolic pressure around 90 mm Hg is recommended until surgical control is achieved. Suspected tension pneumothorax requires immediate needle thoracostomy followed by chest tube placement without waiting for imaging. Pericardial tamponade with instability warrants emergency pericardiocentesis followed by rapid operative intervention.
Emergency department management
The trauma surgeon should be notified immediately. Tube thoracostomy is required for pneumothorax or hemothorax, using appropriately sized tubes. Aggressive crystalloid resuscitation should be avoided when pulmonary contusion is present. Wounds below the nipple line or posterior scapular tip raise concern for intra-abdominal injury and require further evaluation with ultrasound, CT, diagnostic peritoneal lavage, or operative exploration. Chest wounds should not be probed, and impaled objects should only be removed in the operating room. All foreign material should be preserved as forensic evidence. Tetanus prophylaxis should be updated as indicated.
Medications and supportive care
Analgesia and sedation should be provided using small, titrated doses of short-acting agents to avoid respiratory compromise. High-dose steroids for spinal cord injury remain controversial and should follow institutional protocols. Broad-spectrum intravenous antibiotics are indicated if wounds are grossly contaminated.
Disposition and outcomes
All patients with penetrating chest trauma require hospital admission. Hemodynamically unstable patients should proceed directly to the operating room. Emergency department thoracotomy may be lifesaving in selected patients with penetrating torso trauma who had signs of life in the field and short prehospital CPR duration. Large initial chest tube output or persistent bleeding mandates surgical intervention. Patients with isolated minor chest wall wounds and normal imaging may be observed briefly and discharged if repeat evaluation excludes intrathoracic injury and the patient remains stable.
Cause and mechanism
Penetrating chest trauma most commonly results from gunshot wounds or stab wounds. Less frequently, injury occurs from impalement on a sharp object following a fall or high-energy impact. These mechanisms place intrathoracic organs and major vessels at high risk for rapid deterioration.
Clinical features
Patients may present with an object impaled in the chest wall or an obvious penetrating wound with variable external bleeding. Common symptoms include chest pain, dyspnea, and respiratory distress. Altered mental status may occur secondary to hypoxemia or shock. Physical findings can include absent or asymmetric breath sounds, hypotension, and jugular venous distention, suggesting pneumothorax, hemothorax, or cardiac tamponade.
Initial evaluation
A rapid assessment of airway, breathing, and circulation is mandatory. The focused exam should evaluate respiratory effort, chest wall excursion, crepitus, subcutaneous emphysema, breath sounds, and heart sounds. An upright chest radiograph is preferred to identify pneumothorax, although a supine film should be obtained first if spinal precautions are required. Baseline hemoglobin, pulse oximetry, arterial blood gas, serum lactate, and type and screen should be obtained early.
Diagnostic studies
Echocardiography is indicated when tamponade is suspected or when a wound is near the heart. In penetrating precordial injuries, hemopericardium may decompress into the pleural space, so repeat pericardial ultrasound after chest tube placement is recommended. Electrocardiography assists in identifying myocardial injury. With gunshot wounds, imaging must account for all entry and exit sites, and additional studies of the abdomen or pelvis may be required. Arteriography is indicated if great vessel injury is suspected. Esophageal evaluation with contrast swallow or endoscopy and bronchoscopy should be considered when aerodigestive injury is possible.
Differential considerations
Life-threatening diagnoses include pneumothorax, tension or open pneumothorax, hemothorax, pulmonary contusion, myocardial contusion or rupture, pericardial tamponade, traumatic aortic injury, tracheobronchial or esophageal injury, diaphragmatic rupture, intra-abdominal injury, and spinal cord injury.
Prehospital priorities
All patients with signs of life should be transported rapidly to a trauma center. Full spinal immobilization is indicated when spinal injury is suspected. Impaled objects must never be removed in the field because they may be tamponading major bleeding. Suspected tension pneumothorax requires immediate needle decompression. Large open pneumothoraces should be covered with a three-sided occlusive dressing to prevent tension physiology. Transport should not be delayed for intravenous access.
Early resuscitation
Airway, breathing, and circulation management is the priority. Endotracheal intubation is indicated for respiratory distress, hypoxia, or hypotension. Supplemental oxygen should be provided to stable patients. Two large-bore peripheral IV lines should be established, with cautious fluid resuscitation. In penetrating aortic injury, permissive hypotension with a systolic pressure around 90 mm Hg is recommended until surgical control is achieved. Suspected tension pneumothorax requires immediate needle thoracostomy followed by chest tube placement without waiting for imaging. Pericardial tamponade with instability warrants emergency pericardiocentesis followed by rapid operative intervention.
Emergency department management
The trauma surgeon should be notified immediately. Tube thoracostomy is required for pneumothorax or hemothorax, using appropriately sized tubes. Aggressive crystalloid resuscitation should be avoided when pulmonary contusion is present. Wounds below the nipple line or posterior scapular tip raise concern for intra-abdominal injury and require further evaluation with ultrasound, CT, diagnostic peritoneal lavage, or operative exploration. Chest wounds should not be probed, and impaled objects should only be removed in the operating room. All foreign material should be preserved as forensic evidence. Tetanus prophylaxis should be updated as indicated.
Medications and supportive care
Analgesia and sedation should be provided using small, titrated doses of short-acting agents to avoid respiratory compromise. High-dose steroids for spinal cord injury remain controversial and should follow institutional protocols. Broad-spectrum intravenous antibiotics are indicated if wounds are grossly contaminated.
Disposition and outcomes
All patients with penetrating chest trauma require hospital admission. Hemodynamically unstable patients should proceed directly to the operating room. Emergency department thoracotomy may be lifesaving in selected patients with penetrating torso trauma who had signs of life in the field and short prehospital CPR duration. Large initial chest tube output or persistent bleeding mandates surgical intervention. Patients with isolated minor chest wall wounds and normal imaging may be observed briefly and discharged if repeat evaluation excludes intrathoracic injury and the patient remains stable.
- Published on
Emergency and acute medicine – Chest Pain
Overview
Chest pain is one of the most common presenting complaints in the emergency department and frequently represents a potentially life-threatening condition such as acute coronary syndrome, pulmonary embolism, or aortic dissection. Until proven otherwise, chest pain should always be considered dangerous. Although categorization can suggest etiology, presentations are often variable, vague, and misleading.
Anatomic patterns of pain
Thoracic pain arises from structures such as the myocardium, pericardium, ascending aorta, pulmonary artery, mediastinum, or esophagus. It is typically deep, visceral, and poorly localized, ranging from crushing pressure to burning or indigestion-like discomfort.
Epigastric pain may originate from the descending aorta, diaphragm, gallbladder, pancreas, duodenum, or stomach and is often referred to the xiphoid area or back.
Pleuritic pain results from inflammation or trauma of ribs, muscles, pleura, or pericardium and worsens with breathing, coughing, laughing, or sneezing; tenderness to palpation may be present.
Diaphragmatic pleurisy causes sharp epigastric, lower retrosternal, or shoulder pain that intensifies with thoracic movement.
Chest wall pain involves skin and subcutaneous structures and is reproducible with palpation, arm movement, neck extension, or vertical pressure on the head.
Causes
Thoracic causes include acute coronary syndrome, myocarditis, pericarditis, stress-induced cardiomyopathy, stimulant use, thoracic aortic dissection, and esophageal disorders such as reflux, spasm, rupture, or mediastinitis.
Epigastric causes include descending aortic dissection, peptic ulcer disease, pancreatitis, cholecystitis, splenic or hepatic injury, and subdiaphragmatic abscess.
Pleuritic pain may result from pulmonary embolism, pneumothorax, pneumonia, costochondritis, or sickle cell acute chest syndrome.
Chest wall causes include musculoskeletal strain, rib fractures, herpes zoster, thrombophlebitis, xiphisternal arthritis, and breast pathology.
Clinical features
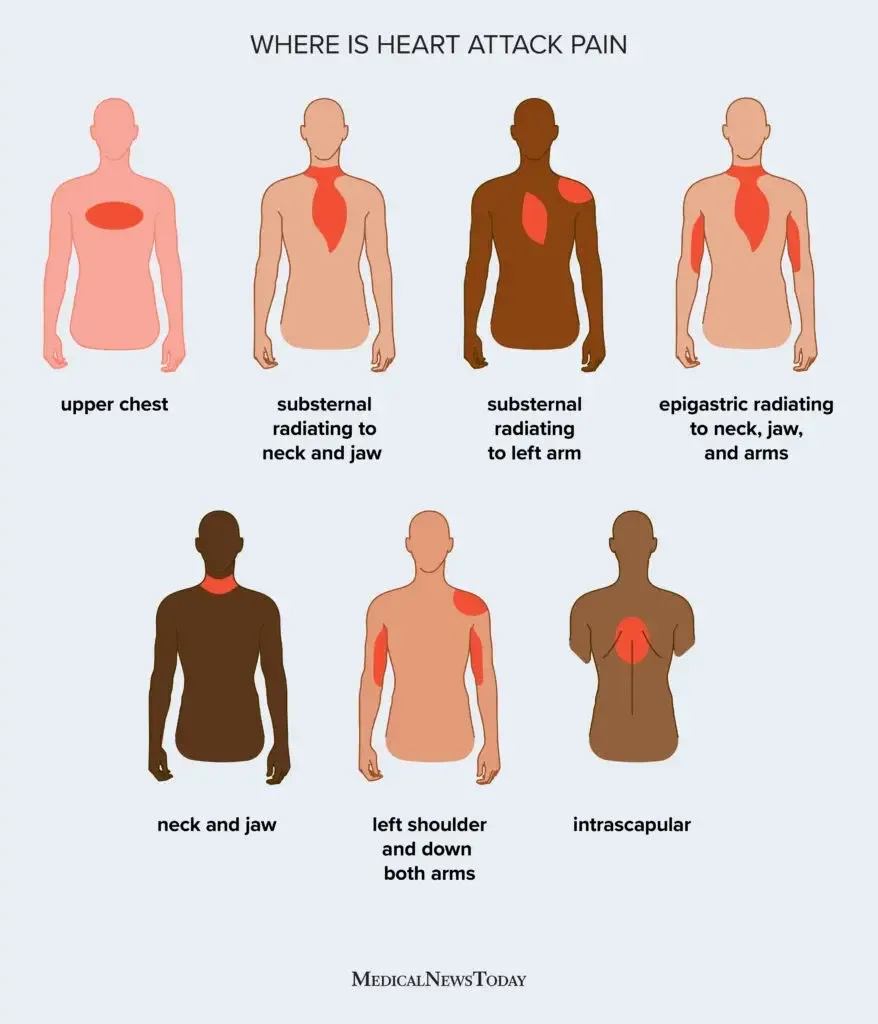
Coronary ischemia commonly presents with pressure-like or squeezing pain radiating to the arm or jaw, associated with dyspnea, diaphoresis, nausea, vomiting, weakness, or fatigue, especially in women and older adults.
Aortic dissection typically causes sudden, severe pain with maximal intensity at onset, often tearing and radiating to the back or flank, accompanied by hypertension, pulse deficits, murmurs, syncope, or neurologic symptoms.
Pulmonary embolism presents with pleuritic pain, dyspnea, anxiety, tachycardia, tachypnea, syncope, or low-grade fever.
Acute pericarditis causes substernal pain worsened by lying flat and relieved by leaning forward, often with fever and a friction rub.
Pneumothorax produces sudden pleuritic pain with dyspnea and unilateral decreased breath sounds.
History and examination
History is the most critical diagnostic tool and should focus on onset, duration, location, quality, radiation, provoking and relieving factors, associated symptoms, and prior cardiac risk factors. Physical examination should include careful cardiac, pulmonary, vascular, abdominal, and skin assessments, looking for murmurs, rubs, breath sound asymmetry, pulse deficits, abdominal tenderness, or zoster lesions.
Investigations
An electrocardiogram should be obtained and interpreted within 10 minutes of arrival, with serial tracings when suspicion for acute coronary syndrome persists. Laboratory testing is individualized based on risk and presentation and may include cardiac biomarkers and D-dimer in selected low-risk patients.
Chest radiography evaluates for pneumothorax, pneumonia, heart failure, mediastinal widening, or esophageal rupture. Computed tomography is useful for pulmonary embolism and aortic dissection. Ultrasound and echocardiography rapidly assess pericardial effusion, valvular disease, right ventricular strain, pneumothorax, and pleural effusion.
Management principles
Prehospital and early emergency care should be guided by risk assessment and may include intravenous access, cardiac monitoring, oxygen, aspirin, nitrates, and analgesia when a cardiac cause is suspected.
Initial stabilization focuses on airway, breathing, circulation, oxygenation, intravenous access, and continuous monitoring. Definitive treatment depends on the suspected underlying cause and should not be delayed in high-risk presentations.
Disposition and follow-up
Admission decisions depend on the likelihood of life-threatening cardiopulmonary disease. Patients deemed low risk after thorough evaluation may be discharged with close outpatient follow-up. Patients should receive clear return precautions for persistent, worsening, or recurrent chest pain, associated dyspnea, diaphoresis, syncope, or radiation of pain.
Clinical cautions
Avoid reliance on a single cardiac biomarker, response to medications, or a single electrocardiogram. Serial ECGs and reassessment are essential in patients with suspected acute coronary syndrome or recurrent symptoms.
Overview
Chest pain is one of the most common presenting complaints in the emergency department and frequently represents a potentially life-threatening condition such as acute coronary syndrome, pulmonary embolism, or aortic dissection. Until proven otherwise, chest pain should always be considered dangerous. Although categorization can suggest etiology, presentations are often variable, vague, and misleading.
Anatomic patterns of pain
Thoracic pain arises from structures such as the myocardium, pericardium, ascending aorta, pulmonary artery, mediastinum, or esophagus. It is typically deep, visceral, and poorly localized, ranging from crushing pressure to burning or indigestion-like discomfort.
Epigastric pain may originate from the descending aorta, diaphragm, gallbladder, pancreas, duodenum, or stomach and is often referred to the xiphoid area or back.
Pleuritic pain results from inflammation or trauma of ribs, muscles, pleura, or pericardium and worsens with breathing, coughing, laughing, or sneezing; tenderness to palpation may be present.
Diaphragmatic pleurisy causes sharp epigastric, lower retrosternal, or shoulder pain that intensifies with thoracic movement.
Chest wall pain involves skin and subcutaneous structures and is reproducible with palpation, arm movement, neck extension, or vertical pressure on the head.
Causes
Thoracic causes include acute coronary syndrome, myocarditis, pericarditis, stress-induced cardiomyopathy, stimulant use, thoracic aortic dissection, and esophageal disorders such as reflux, spasm, rupture, or mediastinitis.
Epigastric causes include descending aortic dissection, peptic ulcer disease, pancreatitis, cholecystitis, splenic or hepatic injury, and subdiaphragmatic abscess.
Pleuritic pain may result from pulmonary embolism, pneumothorax, pneumonia, costochondritis, or sickle cell acute chest syndrome.
Chest wall causes include musculoskeletal strain, rib fractures, herpes zoster, thrombophlebitis, xiphisternal arthritis, and breast pathology.
Clinical features
Coronary ischemia commonly presents with pressure-like or squeezing pain radiating to the arm or jaw, associated with dyspnea, diaphoresis, nausea, vomiting, weakness, or fatigue, especially in women and older adults.
Aortic dissection typically causes sudden, severe pain with maximal intensity at onset, often tearing and radiating to the back or flank, accompanied by hypertension, pulse deficits, murmurs, syncope, or neurologic symptoms.
Pulmonary embolism presents with pleuritic pain, dyspnea, anxiety, tachycardia, tachypnea, syncope, or low-grade fever.
Acute pericarditis causes substernal pain worsened by lying flat and relieved by leaning forward, often with fever and a friction rub.
Pneumothorax produces sudden pleuritic pain with dyspnea and unilateral decreased breath sounds.
History and examination
History is the most critical diagnostic tool and should focus on onset, duration, location, quality, radiation, provoking and relieving factors, associated symptoms, and prior cardiac risk factors. Physical examination should include careful cardiac, pulmonary, vascular, abdominal, and skin assessments, looking for murmurs, rubs, breath sound asymmetry, pulse deficits, abdominal tenderness, or zoster lesions.
Investigations
An electrocardiogram should be obtained and interpreted within 10 minutes of arrival, with serial tracings when suspicion for acute coronary syndrome persists. Laboratory testing is individualized based on risk and presentation and may include cardiac biomarkers and D-dimer in selected low-risk patients.
Chest radiography evaluates for pneumothorax, pneumonia, heart failure, mediastinal widening, or esophageal rupture. Computed tomography is useful for pulmonary embolism and aortic dissection. Ultrasound and echocardiography rapidly assess pericardial effusion, valvular disease, right ventricular strain, pneumothorax, and pleural effusion.
Management principles
Prehospital and early emergency care should be guided by risk assessment and may include intravenous access, cardiac monitoring, oxygen, aspirin, nitrates, and analgesia when a cardiac cause is suspected.
Initial stabilization focuses on airway, breathing, circulation, oxygenation, intravenous access, and continuous monitoring. Definitive treatment depends on the suspected underlying cause and should not be delayed in high-risk presentations.
Disposition and follow-up
Admission decisions depend on the likelihood of life-threatening cardiopulmonary disease. Patients deemed low risk after thorough evaluation may be discharged with close outpatient follow-up. Patients should receive clear return precautions for persistent, worsening, or recurrent chest pain, associated dyspnea, diaphoresis, syncope, or radiation of pain.
Clinical cautions
Avoid reliance on a single cardiac biomarker, response to medications, or a single electrocardiogram. Serial ECGs and reassessment are essential in patients with suspected acute coronary syndrome or recurrent symptoms.
- Published on
Emergency and acute medicine – Chemical Weapons Poisoning
General overview
Chemical weapons poisoning refers to exposure to toxic agents designed to cause injury or death by affecting the central nervous system, lungs, cardiovascular system, skin, eyes, or gastrointestinal tract. These agents may be encountered in warfare, terrorism, industrial accidents, or mass casualty incidents and often involve multiple victims presenting simultaneously.
Types of agents and mechanisms
Blood agents such as cyanide disrupt cellular respiration by binding to cytochrome oxidase and uncoupling oxidative phosphorylation, leading to rapid tissue hypoxia.
Blister agents, including sulfur mustard, nitrogen mustard, lewisite, and phosgene oxime, cause alkylation and cross-linking of DNA and proteins, resulting in cellular membrane damage and delayed tissue necrosis.
Lacrimators and riot control agents, such as CN (Mace), CS, oleoresin capsaicin, chloropicrin, and adamsite, primarily irritate mucous membranes.
Pulmonary irritants, also known as choking agents, vary by water solubility. Highly soluble agents like ammonia mainly affect the upper airway, intermediate agents such as chlorine damage both upper and lower airways through free radical formation, and low-solubility agents like phosgene cause delayed pulmonary edema after hydrolysis in the lungs.
Nerve agents, including sarin, tabun, soman, and VX, inhibit acetylcholinesterase, resulting in widespread cholinergic overstimulation at muscarinic, nicotinic, and central nervous system receptors.
Incapacitating agents such as 3-quinuclidinyl benzilate (BZ) produce an anticholinergic toxidrome through antimuscarinic effects.
Clinical features
History often suggests exposure through reports of multiple affected individuals, fires, industrial incidents, or known chemical release.
Blood agents cause early tachypnea, hypertension, and tachycardia followed by respiratory depression, hypotension, bradycardia, seizures, coma, and rapid death. Cyanosis is uncommon, and metabolic acidosis is prominent.
Blister agents lead to delayed skin erythema, edema, pruritus, vesiculation, and necrosis, along with severe ocular injury, airway sloughing, bronchospasm, and bone marrow suppression.
Lacrimators cause intense eye pain, lacrimation, blepharospasm, temporary blindness, skin irritation, cough, and chest tightness.
Pulmonary irritants produce dyspnea, cough, bronchospasm, chest pain, and delayed pulmonary edema that may appear up to 24 hours after exposure.
Nerve agents produce the classic SLUDGEBAM syndrome with salivation, lacrimation, urination, defecation, gastrointestinal cramps, emesis, bronchorrhea, bronchoconstriction, bradycardia, miosis, seizures, muscle fasciculations, weakness, and paralysis.
Incapacitating agents result in anticholinergic findings including hyperthermia, dry skin, flushed appearance, delirium, tachycardia, urinary retention, and decreased bowel sounds.
Evaluation and recognition
Diagnosis is primarily clinical and based on exposure history and toxidrome recognition. Physical examination may reveal clues such as bitter almond odor and severe acidosis in cyanide poisoning, blistering and skin sloughing with mustard agents, or marked secretions and miosis with nerve agents.
Laboratory and imaging findings
Arterial blood gases may show severe metabolic acidosis and elevated lactate in cyanide exposure. Complete blood counts can reveal leukopenia, thrombocytopenia, or anemia after mustard exposure. Electrolytes, renal function, creatine phosphokinase, and urinalysis assist in monitoring systemic injury. Erythrocyte cholinesterase activity supports nerve agent exposure. Chest radiography is useful to assess pulmonary edema.
Differential considerations
Conditions that may mimic chemical weapons exposure include asthma or COPD exacerbations, Stevens–Johnson syndrome, toxic epidermal necrolysis, organophosphate pesticide poisoning, botulism, radiation injury, congestive heart failure, and anaphylactoid reactions.
Prehospital priorities
Prevent secondary contamination by using appropriate personal protective equipment. Immediate decontamination is critical, with removal of clothing and either dry or wet decontamination depending on the agent. Atropine should be administered early in suspected nerve agent exposure even if tachycardia is present.
Initial stabilization
Airway, breathing, and circulation take priority. Patients require rapid decontamination, copious irrigation of skin and eyes, supplemental oxygen, cardiac monitoring, pulse oximetry, and intravenous access with isotonic fluids. Health care workers must remain protected throughout care.
Emergency department management
Treatment focuses on decontamination, supportive care, and agent-specific antidotes. Cyanide exposure requires high-flow oxygen, seizure control, and hydroxocobalamin as first-line therapy, with traditional cyanide antidote kits as alternatives.
Blister agents are managed with supportive and burn care, fluid and electrolyte monitoring, and management of hematologic complications.
Pulmonary irritants and lacrimators are treated with supportive respiratory care, bronchodilators, eye irrigation, and observation for delayed pulmonary edema.
Nerve agent poisoning requires aggressive airway management, repeated high-dose atropine titrated to respiratory improvement, pralidoxime to reverse neuromuscular effects, and benzodiazepines for seizures.
Incapacitating agents are managed with supportive care, hydration, benzodiazepines for agitation, and consideration of physostigmine in consultation with a poison center.
Pharmacologic therapy
Key medications include atropine, pralidoxime, hydroxocobalamin, benzodiazepines, bronchodilators, and components of the cyanide antidote kit, dosed according to severity and patient age.
Disposition and monitoring
Patients with significant exposure or symptoms require hospital or intensive care admission for monitoring and supportive care. Those exposed to riot control agents alone may be observed in the emergency department and discharged if symptoms resolve.
Clinical pearls
Effective decontamination is essential to protect both patients and clinicians. Recognition of toxidromes allows early, life-saving antidote administration. Delayed complications, particularly pulmonary edema after choking agents, require vigilant observation even when initial symptoms are mild.
General overview
Chemical weapons poisoning refers to exposure to toxic agents designed to cause injury or death by affecting the central nervous system, lungs, cardiovascular system, skin, eyes, or gastrointestinal tract. These agents may be encountered in warfare, terrorism, industrial accidents, or mass casualty incidents and often involve multiple victims presenting simultaneously.
Types of agents and mechanisms
Blood agents such as cyanide disrupt cellular respiration by binding to cytochrome oxidase and uncoupling oxidative phosphorylation, leading to rapid tissue hypoxia.
Blister agents, including sulfur mustard, nitrogen mustard, lewisite, and phosgene oxime, cause alkylation and cross-linking of DNA and proteins, resulting in cellular membrane damage and delayed tissue necrosis.
Lacrimators and riot control agents, such as CN (Mace), CS, oleoresin capsaicin, chloropicrin, and adamsite, primarily irritate mucous membranes.
Pulmonary irritants, also known as choking agents, vary by water solubility. Highly soluble agents like ammonia mainly affect the upper airway, intermediate agents such as chlorine damage both upper and lower airways through free radical formation, and low-solubility agents like phosgene cause delayed pulmonary edema after hydrolysis in the lungs.
Nerve agents, including sarin, tabun, soman, and VX, inhibit acetylcholinesterase, resulting in widespread cholinergic overstimulation at muscarinic, nicotinic, and central nervous system receptors.
Incapacitating agents such as 3-quinuclidinyl benzilate (BZ) produce an anticholinergic toxidrome through antimuscarinic effects.
Clinical features
History often suggests exposure through reports of multiple affected individuals, fires, industrial incidents, or known chemical release.
Blood agents cause early tachypnea, hypertension, and tachycardia followed by respiratory depression, hypotension, bradycardia, seizures, coma, and rapid death. Cyanosis is uncommon, and metabolic acidosis is prominent.
Blister agents lead to delayed skin erythema, edema, pruritus, vesiculation, and necrosis, along with severe ocular injury, airway sloughing, bronchospasm, and bone marrow suppression.
Lacrimators cause intense eye pain, lacrimation, blepharospasm, temporary blindness, skin irritation, cough, and chest tightness.
Pulmonary irritants produce dyspnea, cough, bronchospasm, chest pain, and delayed pulmonary edema that may appear up to 24 hours after exposure.
Nerve agents produce the classic SLUDGEBAM syndrome with salivation, lacrimation, urination, defecation, gastrointestinal cramps, emesis, bronchorrhea, bronchoconstriction, bradycardia, miosis, seizures, muscle fasciculations, weakness, and paralysis.
Incapacitating agents result in anticholinergic findings including hyperthermia, dry skin, flushed appearance, delirium, tachycardia, urinary retention, and decreased bowel sounds.
Evaluation and recognition
Diagnosis is primarily clinical and based on exposure history and toxidrome recognition. Physical examination may reveal clues such as bitter almond odor and severe acidosis in cyanide poisoning, blistering and skin sloughing with mustard agents, or marked secretions and miosis with nerve agents.
Laboratory and imaging findings
Arterial blood gases may show severe metabolic acidosis and elevated lactate in cyanide exposure. Complete blood counts can reveal leukopenia, thrombocytopenia, or anemia after mustard exposure. Electrolytes, renal function, creatine phosphokinase, and urinalysis assist in monitoring systemic injury. Erythrocyte cholinesterase activity supports nerve agent exposure. Chest radiography is useful to assess pulmonary edema.
Differential considerations
Conditions that may mimic chemical weapons exposure include asthma or COPD exacerbations, Stevens–Johnson syndrome, toxic epidermal necrolysis, organophosphate pesticide poisoning, botulism, radiation injury, congestive heart failure, and anaphylactoid reactions.
Prehospital priorities
Prevent secondary contamination by using appropriate personal protective equipment. Immediate decontamination is critical, with removal of clothing and either dry or wet decontamination depending on the agent. Atropine should be administered early in suspected nerve agent exposure even if tachycardia is present.
Initial stabilization
Airway, breathing, and circulation take priority. Patients require rapid decontamination, copious irrigation of skin and eyes, supplemental oxygen, cardiac monitoring, pulse oximetry, and intravenous access with isotonic fluids. Health care workers must remain protected throughout care.
Emergency department management
Treatment focuses on decontamination, supportive care, and agent-specific antidotes. Cyanide exposure requires high-flow oxygen, seizure control, and hydroxocobalamin as first-line therapy, with traditional cyanide antidote kits as alternatives.
Blister agents are managed with supportive and burn care, fluid and electrolyte monitoring, and management of hematologic complications.
Pulmonary irritants and lacrimators are treated with supportive respiratory care, bronchodilators, eye irrigation, and observation for delayed pulmonary edema.
Nerve agent poisoning requires aggressive airway management, repeated high-dose atropine titrated to respiratory improvement, pralidoxime to reverse neuromuscular effects, and benzodiazepines for seizures.
Incapacitating agents are managed with supportive care, hydration, benzodiazepines for agitation, and consideration of physostigmine in consultation with a poison center.
Pharmacologic therapy
Key medications include atropine, pralidoxime, hydroxocobalamin, benzodiazepines, bronchodilators, and components of the cyanide antidote kit, dosed according to severity and patient age.
Disposition and monitoring
Patients with significant exposure or symptoms require hospital or intensive care admission for monitoring and supportive care. Those exposed to riot control agents alone may be observed in the emergency department and discharged if symptoms resolve.
Clinical pearls
Effective decontamination is essential to protect both patients and clinicians. Recognition of toxidromes allows early, life-saving antidote administration. Delayed complications, particularly pulmonary edema after choking agents, require vigilant observation even when initial symptoms are mild.

- Published on
Emergency and acute medicine – chancroid
Basic description
Chancroid is a sexually transmitted genital ulcer disease associated with an increased risk of HIV acquisition. It is common in parts of Africa, Southeast Asia, and Latin America but uncommon in the United States, where herpes simplex virus and syphilis are far more frequent causes of genital ulcers. Despite this, chancroid is likely underreported due to diagnostic challenges.
Cause and microbiology
The disease is caused by Haemophilus ducreyi, a highly infectious gram-negative bacterium transmitted through sexual contact.
Clinical presentation
Chancroid typically begins as a small erythematous papule or pustule that rapidly ulcerates into a painful lesion measuring 1–20 mm. The ulcers are soft, friable, and have ragged, irregular borders with an excavated appearance. The base contains moist granulation tissue and may produce purulent or hemorrhagic exudate.
In men, lesions most often involve the penile shaft, glans, foreskin, or anus, whereas in women they may occur on the cervix, vagina, vulva, perineum, or anus. Symptoms usually appear 4–7 days after exposure, with an incubation period ranging from 1–35 days.
Painful inguinal lymphadenopathy develops in approximately half of affected men and less frequently in women. These nodes are typically unilateral, may become suppurative, and can rupture to form chronic draining sinuses. Dysuria and dyspareunia may occur due to lesion contact. Several variants exist, including phagedenic chancroid with rapid tissue destruction, giant chancroid with a single large ulcer, serpiginous ulcers that spread superficially, and follicular chancroid with multiple small perifollicular lesions.
Diagnostic approach
Diagnosis is primarily clinical but often inaccurate because laboratory confirmation is difficult. The Centers for Disease Control and Prevention defines a probable diagnosis as the presence of typical painful genital ulcers with negative testing for syphilis and herpes simplex virus. A definite diagnosis requires isolation of H. ducreyi on culture, which is rarely feasible in routine practice.
Laboratory evaluation
Gram stain is unreliable and shows characteristic gram-negative coccobacilli in a linear “school-of-fish” pattern in only 50–80% of cases. Culture requires specialized media and has variable sensitivity. Polymerase chain reaction testing is sensitive and specific but not widely available. Serologic testing for syphilis, herpes simplex virus, and HIV is recommended because coinfection is common.
Differential diagnosis
Infectious considerations include syphilis, genital herpes, granuloma inguinale, and lymphogranuloma venereum. Noninfectious causes such as drug reactions, pyoderma gangrenosum, and Behçet disease should also be considered when presentation is atypical.
Management principles
Standard infection control precautions should be used during evaluation. Treatment should not be delayed when clinical criteria for probable chancroid are met.
Emergency department treatment
First-line therapy includes single-dose azithromycin or intramuscular ceftriaxone, with ceftriaxone preferred during pregnancy. Alternative regimens include ciprofloxacin for three days (avoided in pregnancy and lactation) or erythromycin for seven days. Suppurative lymph nodes larger than 5 cm should be aspirated with a large-bore needle through intact skin to prevent chronic sinus formation. Patients should undergo concurrent testing for HIV, syphilis, and herpes simplex virus, with repeat testing at three months if initially negative.
Medications
Recommended regimens include azithromycin 1 g orally once or ceftriaxone 250 mg intramuscularly once. Alternatives are ciprofloxacin 500 mg orally twice daily for three days or erythromycin base 500 mg orally four times daily for seven days.
Disposition and follow-up
Patients should abstain from sexual activity or use condoms until complete lesion healing. Clinical improvement is usually seen within two days, with ulcer resolution in 3–7 days, though healing may be delayed in HIV-positive or uncircumcised patients.
Ongoing care recommendations
All sexual partners with exposure within 10 days of symptom onset should be examined and treated regardless of symptoms. HIV-positive patients require close follow-up, particularly when treated with single-dose regimens due to higher failure rates.
Key clinical pearls
Treatment should be initiated based on clinical probability rather than awaiting culture confirmation. Treatment failure should prompt evaluation for nonadherence, antimicrobial resistance, or coinfection, particularly syphilis.
Basic description
Chancroid is a sexually transmitted genital ulcer disease associated with an increased risk of HIV acquisition. It is common in parts of Africa, Southeast Asia, and Latin America but uncommon in the United States, where herpes simplex virus and syphilis are far more frequent causes of genital ulcers. Despite this, chancroid is likely underreported due to diagnostic challenges.
Cause and microbiology
The disease is caused by Haemophilus ducreyi, a highly infectious gram-negative bacterium transmitted through sexual contact.
Clinical presentation
Chancroid typically begins as a small erythematous papule or pustule that rapidly ulcerates into a painful lesion measuring 1–20 mm. The ulcers are soft, friable, and have ragged, irregular borders with an excavated appearance. The base contains moist granulation tissue and may produce purulent or hemorrhagic exudate.
In men, lesions most often involve the penile shaft, glans, foreskin, or anus, whereas in women they may occur on the cervix, vagina, vulva, perineum, or anus. Symptoms usually appear 4–7 days after exposure, with an incubation period ranging from 1–35 days.
Painful inguinal lymphadenopathy develops in approximately half of affected men and less frequently in women. These nodes are typically unilateral, may become suppurative, and can rupture to form chronic draining sinuses. Dysuria and dyspareunia may occur due to lesion contact. Several variants exist, including phagedenic chancroid with rapid tissue destruction, giant chancroid with a single large ulcer, serpiginous ulcers that spread superficially, and follicular chancroid with multiple small perifollicular lesions.
Diagnostic approach
Diagnosis is primarily clinical but often inaccurate because laboratory confirmation is difficult. The Centers for Disease Control and Prevention defines a probable diagnosis as the presence of typical painful genital ulcers with negative testing for syphilis and herpes simplex virus. A definite diagnosis requires isolation of H. ducreyi on culture, which is rarely feasible in routine practice.
Laboratory evaluation
Gram stain is unreliable and shows characteristic gram-negative coccobacilli in a linear “school-of-fish” pattern in only 50–80% of cases. Culture requires specialized media and has variable sensitivity. Polymerase chain reaction testing is sensitive and specific but not widely available. Serologic testing for syphilis, herpes simplex virus, and HIV is recommended because coinfection is common.
Differential diagnosis
Infectious considerations include syphilis, genital herpes, granuloma inguinale, and lymphogranuloma venereum. Noninfectious causes such as drug reactions, pyoderma gangrenosum, and Behçet disease should also be considered when presentation is atypical.
Management principles
Standard infection control precautions should be used during evaluation. Treatment should not be delayed when clinical criteria for probable chancroid are met.
Emergency department treatment
First-line therapy includes single-dose azithromycin or intramuscular ceftriaxone, with ceftriaxone preferred during pregnancy. Alternative regimens include ciprofloxacin for three days (avoided in pregnancy and lactation) or erythromycin for seven days. Suppurative lymph nodes larger than 5 cm should be aspirated with a large-bore needle through intact skin to prevent chronic sinus formation. Patients should undergo concurrent testing for HIV, syphilis, and herpes simplex virus, with repeat testing at three months if initially negative.
Medications
Recommended regimens include azithromycin 1 g orally once or ceftriaxone 250 mg intramuscularly once. Alternatives are ciprofloxacin 500 mg orally twice daily for three days or erythromycin base 500 mg orally four times daily for seven days.
Disposition and follow-up
Patients should abstain from sexual activity or use condoms until complete lesion healing. Clinical improvement is usually seen within two days, with ulcer resolution in 3–7 days, though healing may be delayed in HIV-positive or uncircumcised patients.
Ongoing care recommendations
All sexual partners with exposure within 10 days of symptom onset should be examined and treated regardless of symptoms. HIV-positive patients require close follow-up, particularly when treated with single-dose regimens due to higher failure rates.
Key clinical pearls
Treatment should be initiated based on clinical probability rather than awaiting culture confirmation. Treatment failure should prompt evaluation for nonadherence, antimicrobial resistance, or coinfection, particularly syphilis.
- Published on
Emergency and Acute Medicine – Emergency Cesarean Section
Alert
The sole indication for an emergency department physician to perform an emergency perimortem cesarean section is a gravid female (>24 weeks gestation) in cardiopulmonary arrest who has not responded to initial resuscitative measures, regardless of cause. The most important predictor of fetal survival is the time interval between maternal cardiac arrest and cesarean delivery. The procedure should begin within 4 minutes of maternal arrest with a goal of fetal delivery within 1 minute. Immediate consultation with obstetrics, pediatrics, and surgery (if trauma related) should be obtained, but the procedure must not be delayed while awaiting consultant arrival. Emergent cesarean section should not be performed if gestational age is <24 weeks.< />pan>
Overview and Definition
Emergency (perimortem) cesarean section is a resuscitative intervention performed during maternal cardiopulmonary arrest to improve maternal hemodynamics by relieving aortocaval compression and to allow potential fetal survival. Uterine decompression improves venous return, cardiac output, and the effectiveness of cardiopulmonary resuscitation.
Etiology
Trauma, both penetrating and blunt, is the most common cause of maternal mortality. Nontraumatic causes include pulmonary embolism, cerebral vascular accident, amniotic fluid embolism, disseminated intravascular coagulation, placenta previa, eclampsia, and medical conditions such as asthma, congestive heart failure, myocardial infarction, and drug overdose.
Diagnosis
Diagnosis is clinical and based on the presence of cardiopulmonary arrest in a gravid female estimated to be beyond 24 weeks gestation.
Signs and Symptoms
The patient is unresponsive, apneic, and pulseless. Gestational age is estimated clinically.
Physical Examination
A uterus palpated at least four fingerbreadths above the umbilicus corresponds to an estimated gestational age of ≥24 weeks.
Essential Assessment
Rapid confirmation of apnea and pulselessness should occur simultaneously with evaluation for reversible causes of arrest including hypoxia, hypovolemia, acidosis, electrolyte abnormalities, hypoglycemia, hypothermia, trauma, thromboembolism, toxins, tension pneumothorax, cardiac tamponade, and supine hypotension syndrome. Fundal height in centimeters approximates gestational age in weeks. Ultrasound may be used only if immediately available and without delay.
Diagnostic Tests and Interpretation
No imaging or laboratory studies are required to establish the diagnosis. Fetal heart tones should not be assessed if this delays intervention.
Prehospital Care
Scene time should be minimized. The patient should be positioned in the left lateral decubitus position to relieve inferior vena cava compression. In trauma patients requiring spinal immobilization, manual uterine displacement or elevation of the right hip should be performed.
Initial Stabilization
Standard ACLS measures should be initiated, including airway management with a smaller endotracheal tube, high-flow oxygen, cardiac monitoring, and large-bore IV access with aggressive fluid resuscitation. If gestational age is ≥24 weeks and no return of spontaneous circulation occurs after 4 minutes of resuscitation, immediate cesarean section is indicated.
Emergency Department Procedure
Do not delay for consultants. Perform a vertical midline abdominal incision from the pubic hairline to approximately 5 cm above the umbilicus. Incise through fascia and peritoneum, retract the bladder inferiorly, make a vertical uterine incision, deliver the fetus, clamp and cut the umbilical cord, deliver the placenta, reassess maternal circulation, and continue resuscitative efforts.
Disposition
The neonate requires admission to the neonatal intensive care unit. If maternal circulation returns, the mother requires intensive care unit admission. Neither patient should be discharged from the emergency department.
Pearls and Pitfalls
Only gravid patients ≥24 weeks gestation qualify for perimortem cesarean section. The decision must be made within 4 minutes of maternal arrest, and delivery should be completed within 1 minute. Speed and decisiveness are critical.

- Published on
Emergency and Acute Medicine – Bladder Injury
Overview and Definitions
Bladder injury most commonly results from blunt trauma. Approximately 10% of patients with pelvic fractures sustain significant bladder injury, and 80–90% of bladder ruptures are associated with pelvic fractures. Overall mortality ranges from 17–22%, increasing to nearly 60% in combined intraperitoneal and extraperitoneal ruptures.
Etiology and Classification
Trauma accounts for about 82% of bladder injuries. Blunt mechanisms include motor vehicle accidents (87%), falls (7%), and assault (6%). Penetrating injuries are most often due to gunshot wounds (85%) and stabbings (15%). Iatrogenic causes account for 14% and include TURP, urologic, gynecologic, obstetric, abdominal, and orthopedic hip procedures, biopsies, indwelling Foley catheters, and IUD placement. Intoxication accounts for 2.9%, and spontaneous rupture occurs in less than 1%.
Extraperitoneal rupture (62%) is usually associated with pelvic fractures and results from blunt force or bone fragments. Intraperitoneal rupture (25%) occurs from direct compression of a distended bladder, typically involving the bladder dome. Combined intraperitoneal and extraperitoneal rupture (12%) carries the highest mortality due to associated injuries. Bladder contusion involves injury to the endothelial lining or muscularis with an intact bladder wall and may cause gross hematuria with normal imaging; it usually resolves without intervention.
In children, the bladder is intra-abdominal until late adolescence, making intraperitoneal rupture more common and overall bladder injury more frequent due to a less rigid pelvis.
Clinical Presentation
The classic triad includes gross hematuria, suprapubic pain, and difficulty voiding. History should focus on traumatic mechanism or recent procedures. On examination, the urethral meatus must be inspected; if blood is present, Foley catheter placement should be deferred until a retrograde urethrogram is performed, as concomitant urethral injury occurs in 10–29% of cases.
Evaluation and Diagnostic Testing
Initial evaluation includes urinalysis, which shows gross hematuria in 95–100% of significant injuries and microscopic hematuria in about 5%. BUN may be elevated due to intraperitoneal urine resorption, and electrolyte abnormalities such as hyperkalemia or hypernatremia may be present.
Retrograde cystography or CT cystography is the diagnostic modality of choice, with sensitivity around 95% and specificity near 100%. If urethral injury is suspected, a retrograde urethrogram is performed first. Proper cystography requires adequate bladder distension with diluted contrast and postdrainage imaging, as up to 10% of ruptures are detected only after bladder emptying. Extraperitoneal ruptures show teardrop- or star-shaped extravasation, whereas intraperitoneal ruptures demonstrate contrast outlining bowel loops or filling paracolic gutters. FAST examination showing free pelvic fluid should heighten suspicion for bladder injury.
Differential Diagnosis
Consider peritoneal trauma, urethral injury, and renal or ureteral trauma.
Management
Prehospital bladder catheterization should be avoided. Initial management follows standard ABCs with early urologic consultation. Extraperitoneal nonpenetrating ruptures may be managed with Foley catheter drainage (20F or larger) for approximately 14 days, with most lacerations sealing within 3 weeks; surgical repair is recommended if the patient is undergoing pelvic or abdominal surgery for other injuries. Intraperitoneal ruptures require surgical exploration and repair. Bladder contusions require no specific intervention. Broad-spectrum antibiotics are indicated for intraperitoneal rupture.
Disposition and Follow-Up
Admission is required for patients with associated major trauma or those needing surgical intervention. Bladder contusions without rupture and without other injuries may be discharged. Most bladder ruptures require admission, and discharge should occur only after urologic clearance. Urology follow-up is required for all outpatient-managed injuries, with Foley catheter removal typically at 14 days for conservatively managed extraperitoneal ruptures.
Clinical Insights and Common Errors
Free pelvic fluid on CT or ultrasound should prompt concern for bladder injury. Unresponsive, intoxicated, or altered patients require careful evaluation. Any penetrating injury to the lower abdomen with hematuria warrants cystography.
Overview and Definitions
Bladder injury most commonly results from blunt trauma. Approximately 10% of patients with pelvic fractures sustain significant bladder injury, and 80–90% of bladder ruptures are associated with pelvic fractures. Overall mortality ranges from 17–22%, increasing to nearly 60% in combined intraperitoneal and extraperitoneal ruptures.
Etiology and Classification
Trauma accounts for about 82% of bladder injuries. Blunt mechanisms include motor vehicle accidents (87%), falls (7%), and assault (6%). Penetrating injuries are most often due to gunshot wounds (85%) and stabbings (15%). Iatrogenic causes account for 14% and include TURP, urologic, gynecologic, obstetric, abdominal, and orthopedic hip procedures, biopsies, indwelling Foley catheters, and IUD placement. Intoxication accounts for 2.9%, and spontaneous rupture occurs in less than 1%.
Extraperitoneal rupture (62%) is usually associated with pelvic fractures and results from blunt force or bone fragments. Intraperitoneal rupture (25%) occurs from direct compression of a distended bladder, typically involving the bladder dome. Combined intraperitoneal and extraperitoneal rupture (12%) carries the highest mortality due to associated injuries. Bladder contusion involves injury to the endothelial lining or muscularis with an intact bladder wall and may cause gross hematuria with normal imaging; it usually resolves without intervention.
In children, the bladder is intra-abdominal until late adolescence, making intraperitoneal rupture more common and overall bladder injury more frequent due to a less rigid pelvis.
Clinical Presentation
The classic triad includes gross hematuria, suprapubic pain, and difficulty voiding. History should focus on traumatic mechanism or recent procedures. On examination, the urethral meatus must be inspected; if blood is present, Foley catheter placement should be deferred until a retrograde urethrogram is performed, as concomitant urethral injury occurs in 10–29% of cases.
Evaluation and Diagnostic Testing
Initial evaluation includes urinalysis, which shows gross hematuria in 95–100% of significant injuries and microscopic hematuria in about 5%. BUN may be elevated due to intraperitoneal urine resorption, and electrolyte abnormalities such as hyperkalemia or hypernatremia may be present.
Retrograde cystography or CT cystography is the diagnostic modality of choice, with sensitivity around 95% and specificity near 100%. If urethral injury is suspected, a retrograde urethrogram is performed first. Proper cystography requires adequate bladder distension with diluted contrast and postdrainage imaging, as up to 10% of ruptures are detected only after bladder emptying. Extraperitoneal ruptures show teardrop- or star-shaped extravasation, whereas intraperitoneal ruptures demonstrate contrast outlining bowel loops or filling paracolic gutters. FAST examination showing free pelvic fluid should heighten suspicion for bladder injury.
Differential Diagnosis
Consider peritoneal trauma, urethral injury, and renal or ureteral trauma.
Management
Prehospital bladder catheterization should be avoided. Initial management follows standard ABCs with early urologic consultation. Extraperitoneal nonpenetrating ruptures may be managed with Foley catheter drainage (20F or larger) for approximately 14 days, with most lacerations sealing within 3 weeks; surgical repair is recommended if the patient is undergoing pelvic or abdominal surgery for other injuries. Intraperitoneal ruptures require surgical exploration and repair. Bladder contusions require no specific intervention. Broad-spectrum antibiotics are indicated for intraperitoneal rupture.
Disposition and Follow-Up
Admission is required for patients with associated major trauma or those needing surgical intervention. Bladder contusions without rupture and without other injuries may be discharged. Most bladder ruptures require admission, and discharge should occur only after urologic clearance. Urology follow-up is required for all outpatient-managed injuries, with Foley catheter removal typically at 14 days for conservatively managed extraperitoneal ruptures.
Clinical Insights and Common Errors
Free pelvic fluid on CT or ultrasound should prompt concern for bladder injury. Unresponsive, intoxicated, or altered patients require careful evaluation. Any penetrating injury to the lower abdomen with hematuria warrants cystography.

