- Published on
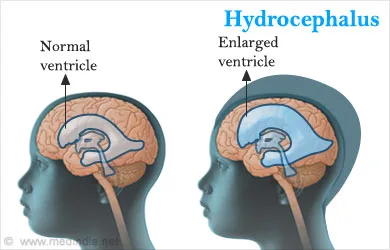
KembaraXtra-Emergency And Acute Medicine: Hydrocephalus
Basics
Description Hydrocephalus is an abnormal increase in cerebrospinal fluid (CSF) volume within the cranial cavity. Cerebral atrophy may also increase CSF volume but without elevated CSF pressure. Obstructive hydrocephalus is the most common form and results from blockage within the ventricular system or subarachnoid space, potentially causing rapid rises in intracranial pressure (ICP) leading to death or permanent brain injury. Nonobstructive hydrocephalus produces subacute symptoms and represents a potentially reversible cause of dementia. Hydrocephalus is also classified as communicating, where CSF flow is blocked after exiting the ventricles, and noncommunicating, where flow is blocked within ventricular pathways.
Etiology Obstructive hydrocephalus results from blockage at specific anatomic sites. Aqueduct of Sylvius obstruction is most common, causing dilation of the lateral and third ventricles with sparing of the fourth ventricle; causes include congenital stenosis, tumor, subarachnoid hemorrhage, postmeningitic scarring, or idiopathic disease. Foramen of Monro obstruction leads to dilation of one or both lateral ventricles. Obstruction at the foramina of Luschka and Magendie causes fourth ventricle blockage with subsequent dilation of the entire ventricular system. Subarachnoid space obstruction around the brainstem may occur after infection or subarachnoid hemorrhage, producing global ventricular dilation. Acute presentations are often due to CSF shunt malfunction, subarachnoid hemorrhage, or severe head trauma. Nonobstructive hydrocephalus, including normal pressure hydrocephalus, involves impaired CSF absorption with ventricular enlargement but no sustained intracranial hypertension and is sometimes termed chronic hydrocephalus. Pediatric hydrocephalus may be congenital or acquired and is commonly related to neonatal hemorrhage, congenital malformations, or postinfectious scarring.
Diagnosis
Signs and symptoms Obstructive hydrocephalus presents with headache, nausea, vomiting, decreased consciousness, urinary incontinence, ocular palsies, papilledema, visual loss, pupillary dilation, and Cushing response with hypertension and bradycardia. Pediatric patients may show a full fontanelle, irritability, lethargy, and elevated blood pressure. Slowly progressive obstruction may resemble nonobstructive hydrocephalus. Nonobstructive hydrocephalus presents with insidious dementia, somnolence, gait disturbance, urinary incontinence, impaired upward gaze, generalized weakness, and lethargy, typically without headache or papilledema.
Pediatric considerations Gradual CSF accumulation may cause craniomegaly, developmental delay, prominent scalp veins, and impaired upward gaze (setting-sun sign).
History Assess symptom onset, presence of a CSF shunt, headache, nausea or vomiting, weakness, confusion, visual changes, and urinary incontinence.
Physical exam Perform a complete neurologic examination including motor, sensory, reflexes, gait, and cranial nerves. Assess mental status and look for papilledema. Palpate any CSF shunt; inability to compress suggests distal malfunction, and failure to refill suggests proximal obstruction. In children, evaluate the anterior fontanelle.
Essential workup Noncontrast CT of the head assesses ventricular size and symmetry and helps identify hemorrhage, mass lesions, or cerebral edema.
Diagnosis tests and interpretation
Laboratory Lumbar puncture is performed only after CT and only for suspected nonobstructive causes; opening pressure may be elevated. Send CSF for routine studies if infection is suspected.
Imaging MRI provides detailed assessment of ventricular anatomy and improved detection of masses compared with CT.
Diagnostic procedures Lumbar puncture may be diagnostic or therapeutic in selected nonobstructive cases.
Differential diagnosis Acute ischemic stroke, intracranial hemorrhage, CNS infection, mass effect from tumor or hematoma, other causes of dementia or delirium, and toxic or metabolic encephalopathies.
Pediatric considerations Consider congenital anomalies such as Dandy–Walker malformation, Arnold–Chiari malformation, meningomyelocele, choroid plexus papilloma, or arachnoid villi dysfunction, as well as infections (rubella, CMV, toxoplasmosis, syphilis, bacterial meningitis), tumors of the posterior fossa, and intraventricular or subarachnoid hemorrhage.
Treatment
Prehospital Hydrocephalus cannot be definitively diagnosed in the field. Provide supplemental oxygen and airway support as needed. Transport with the head elevated to approximately 30° unless hypotension is present, in which case prioritize cerebral perfusion with fluid resuscitation.
Initial stabilization/therapy For signs of impending herniation, perform rapid-sequence intubation using agents such as etomidate or thiopental. Maintain controlled ventilation with PaCO₂ around 35 mm Hg and systolic blood pressure above 100 mm Hg in adults. Administer mannitol as indicated. In patients with CSF shunts and impending herniation, shunt pumping or controlled CSF drainage may be attempted to reduce pressure.
Emergency department management ED intervention is required for acute shunt malfunction or impending herniation. Definitive therapy involves shunt placement or revision or treatment of the underlying cause such as tumor. Symptoms of normal pressure hydrocephalus may transiently improve after removal of 20–30 mL of CSF via lumbar puncture. Acute obstructive hydrocephalus from intraventricular hemorrhage may require ventriculostomy. Provide sedation for agitated or intubated patients, maintain head elevation unless hypotensive, consider mannitol, and use seizure prophylaxis when appropriate.
Medication Atropine 0.02 mg/kg IV (max 0.1 mg), etomidate 0.2–0.3 mg/kg IV, lidocaine 1 mg/kg IV, mannitol 0.5–1.5 g/kg IV, rocuronium 0.6 mg/kg IV, succinylcholine 1–1.5 mg/kg IV, vecuronium 0.1 mg/kg IV, fosphenytoin 15–20 mg/kg loading dose.
Follow-up and disposition
Admission criteria Evidence of increased ICP or suspected shunt malfunction.
Discharge criteria Selected patients with presumed normal pressure hydrocephalus and no acute findings may be discharged with close follow-up.
Issues for referral Early neurosurgical consultation is essential for acute obstructive hydrocephalus or shunt malfunction; transfer should be considered if neurosurgical care is unavailable, with airway secured when indicated.
Follow-up recommendations Stable patients require prompt follow-up with neurology and/or neurosurgery.
Key points Lumbar puncture is contraindicated in obstructive hydrocephalus due to herniation risk. Rapid head growth in children should prompt evaluation for hydrocephalus. Any neurologic complaint in a patient with a CSF shunt should raise concern for shunt malfunction.
Basics
Description Hydrocephalus is an abnormal increase in cerebrospinal fluid (CSF) volume within the cranial cavity. Cerebral atrophy may also increase CSF volume but without elevated CSF pressure. Obstructive hydrocephalus is the most common form and results from blockage within the ventricular system or subarachnoid space, potentially causing rapid rises in intracranial pressure (ICP) leading to death or permanent brain injury. Nonobstructive hydrocephalus produces subacute symptoms and represents a potentially reversible cause of dementia. Hydrocephalus is also classified as communicating, where CSF flow is blocked after exiting the ventricles, and noncommunicating, where flow is blocked within ventricular pathways.
Etiology Obstructive hydrocephalus results from blockage at specific anatomic sites. Aqueduct of Sylvius obstruction is most common, causing dilation of the lateral and third ventricles with sparing of the fourth ventricle; causes include congenital stenosis, tumor, subarachnoid hemorrhage, postmeningitic scarring, or idiopathic disease. Foramen of Monro obstruction leads to dilation of one or both lateral ventricles. Obstruction at the foramina of Luschka and Magendie causes fourth ventricle blockage with subsequent dilation of the entire ventricular system. Subarachnoid space obstruction around the brainstem may occur after infection or subarachnoid hemorrhage, producing global ventricular dilation. Acute presentations are often due to CSF shunt malfunction, subarachnoid hemorrhage, or severe head trauma. Nonobstructive hydrocephalus, including normal pressure hydrocephalus, involves impaired CSF absorption with ventricular enlargement but no sustained intracranial hypertension and is sometimes termed chronic hydrocephalus. Pediatric hydrocephalus may be congenital or acquired and is commonly related to neonatal hemorrhage, congenital malformations, or postinfectious scarring.
Diagnosis
Signs and symptoms Obstructive hydrocephalus presents with headache, nausea, vomiting, decreased consciousness, urinary incontinence, ocular palsies, papilledema, visual loss, pupillary dilation, and Cushing response with hypertension and bradycardia. Pediatric patients may show a full fontanelle, irritability, lethargy, and elevated blood pressure. Slowly progressive obstruction may resemble nonobstructive hydrocephalus. Nonobstructive hydrocephalus presents with insidious dementia, somnolence, gait disturbance, urinary incontinence, impaired upward gaze, generalized weakness, and lethargy, typically without headache or papilledema.
Pediatric considerations Gradual CSF accumulation may cause craniomegaly, developmental delay, prominent scalp veins, and impaired upward gaze (setting-sun sign).
History Assess symptom onset, presence of a CSF shunt, headache, nausea or vomiting, weakness, confusion, visual changes, and urinary incontinence.
Physical exam Perform a complete neurologic examination including motor, sensory, reflexes, gait, and cranial nerves. Assess mental status and look for papilledema. Palpate any CSF shunt; inability to compress suggests distal malfunction, and failure to refill suggests proximal obstruction. In children, evaluate the anterior fontanelle.
Essential workup Noncontrast CT of the head assesses ventricular size and symmetry and helps identify hemorrhage, mass lesions, or cerebral edema.
Diagnosis tests and interpretation
Laboratory Lumbar puncture is performed only after CT and only for suspected nonobstructive causes; opening pressure may be elevated. Send CSF for routine studies if infection is suspected.
Imaging MRI provides detailed assessment of ventricular anatomy and improved detection of masses compared with CT.
Diagnostic procedures Lumbar puncture may be diagnostic or therapeutic in selected nonobstructive cases.
Differential diagnosis Acute ischemic stroke, intracranial hemorrhage, CNS infection, mass effect from tumor or hematoma, other causes of dementia or delirium, and toxic or metabolic encephalopathies.
Pediatric considerations Consider congenital anomalies such as Dandy–Walker malformation, Arnold–Chiari malformation, meningomyelocele, choroid plexus papilloma, or arachnoid villi dysfunction, as well as infections (rubella, CMV, toxoplasmosis, syphilis, bacterial meningitis), tumors of the posterior fossa, and intraventricular or subarachnoid hemorrhage.
Treatment
Prehospital Hydrocephalus cannot be definitively diagnosed in the field. Provide supplemental oxygen and airway support as needed. Transport with the head elevated to approximately 30° unless hypotension is present, in which case prioritize cerebral perfusion with fluid resuscitation.
Initial stabilization/therapy For signs of impending herniation, perform rapid-sequence intubation using agents such as etomidate or thiopental. Maintain controlled ventilation with PaCO₂ around 35 mm Hg and systolic blood pressure above 100 mm Hg in adults. Administer mannitol as indicated. In patients with CSF shunts and impending herniation, shunt pumping or controlled CSF drainage may be attempted to reduce pressure.
Emergency department management ED intervention is required for acute shunt malfunction or impending herniation. Definitive therapy involves shunt placement or revision or treatment of the underlying cause such as tumor. Symptoms of normal pressure hydrocephalus may transiently improve after removal of 20–30 mL of CSF via lumbar puncture. Acute obstructive hydrocephalus from intraventricular hemorrhage may require ventriculostomy. Provide sedation for agitated or intubated patients, maintain head elevation unless hypotensive, consider mannitol, and use seizure prophylaxis when appropriate.
Medication Atropine 0.02 mg/kg IV (max 0.1 mg), etomidate 0.2–0.3 mg/kg IV, lidocaine 1 mg/kg IV, mannitol 0.5–1.5 g/kg IV, rocuronium 0.6 mg/kg IV, succinylcholine 1–1.5 mg/kg IV, vecuronium 0.1 mg/kg IV, fosphenytoin 15–20 mg/kg loading dose.
Follow-up and disposition
Admission criteria Evidence of increased ICP or suspected shunt malfunction.
Discharge criteria Selected patients with presumed normal pressure hydrocephalus and no acute findings may be discharged with close follow-up.
Issues for referral Early neurosurgical consultation is essential for acute obstructive hydrocephalus or shunt malfunction; transfer should be considered if neurosurgical care is unavailable, with airway secured when indicated.
Follow-up recommendations Stable patients require prompt follow-up with neurology and/or neurosurgery.
Key points Lumbar puncture is contraindicated in obstructive hydrocephalus due to herniation risk. Rapid head growth in children should prompt evaluation for hydrocephalus. Any neurologic complaint in a patient with a CSF shunt should raise concern for shunt malfunction.
- Published on
Infectious Diseases and Microbiology: Dysuria and Fever
Basics
Description
Dysuria refers to painful urination. Acute urethral syndrome describes dysuria with urgency and frequency in the absence of significant bacteriuria.
Approach to the Patient
Irritation of urethral and bladder mucosa typically causes frequent, painful voiding of small urine volumes. Dysuria is often assumed to be a urinary tract infection and treated empirically, which can miss important diagnoses in some patients and lead to unnecessary antibiotics in others, so targeted evaluation is preferred. A focused history and examination, including pelvic and rectal examination when indicated, often clarifies the cause and enables directed therapy. Sexually transmitted infections including Chlamydia trachomatis, Neisseria gonorrhoeae, and herpes simplex virus can cause dysuria in any sex. Prostatitis is a key diagnosis in men because it is harder to eradicate and can recur. Fever is uncommon in cystitis but may occur with acute prostatitis; dysuria with fever should also raise concern for upper-tract infection such as pyelonephritis. Primary genital herpes can cause dysuria with fever, while chlamydia, gonorrhea, and nonspecific urethritis rarely cause fever unless complicated by pelvic inflammatory disease or Fitz-Hugh–Curtis syndrome. Dysuria with hematuria suggests infectious or noninfectious cystitis and also warrants consideration of tuberculous cystitis, bladder cancer, trauma, renal stones, and schistosomiasis. Dysuria with urethral or vaginal discharge suggests gonorrhea or chlamydia, nonspecific urethritis (with or without conjunctivitis and arthritis consistent with reactive arthritis), and prostatitis. Urinalysis and urine culture are standard initial tests, though young women with classic uncomplicated symptoms and no risk factors for complicated or recurrent infection may be treated empirically.
Epidemiology
Incidence
UTIs are among the most common infectious syndromes and carry substantial costs, including antibiotic expenditures exceeding one billion dollars annually in the United States. Most patients with primary symptomatic genital herpes experience dysuria, though dysuria is typically absent with recurrences. Sexual intercourse is linked to several dysuria etiologies, with symptom timing differing by syndrome: postcoital cystitis often appears within days, urethritis tends to appear after one to two weeks, and vaginitis may present weeks to months later. Pyelonephritis is a frequent cause of hospitalization, and UTIs account for over 100,000 U.S. admissions annually. Healthcare-associated infections are often UTIs, commonly catheter-related; bacteriuria develops in a substantial proportion of patients with prolonged catheterization with a daily incremental risk of infection, and even single catheterization can cause UTI. Escherichia coli causes most uncomplicated UTIs. In pregnancy, asymptomatic bacteriuria can progress to pyelonephritis and is associated with adverse obstetric outcomes including premature labor
.
Etiology
Beyond bacterial cystitis and pyelonephritis and sexually transmitted causes, dysuria may result from atrophic vaginitis, Candida-associated vaginitis, irritation from a distal urethral stone, chemical exposures, compression from an adnexal mass, radiation injury, and vaginal or urethral trauma including sexual abuse or foreign body insertion. Among women with acute dysuria and frequency, most have significant bacteriuria, and many without significant bacteriuria still have infections of the bladder, kidneys, or urethra. Ureaplasma urealyticum is often detected in symptomatic patients but is also found in asymptomatic individuals, and both U. urealyticum and Mycoplasma hominis have been identified in prostatic and renal tissues in patients with dysuria. Adenovirus can cause acute hemorrhagic cystitis in children and some young adults, sometimes in outbreaks, while other urinary viral isolates are generally not considered causes of infection in immunocompetent hosts.
Diagnosis
History
Dysuria with frequency, urgency, and suprapubic discomfort commonly reflects bladder or urethral inflammation. Prostatitis typically causes dysuria, frequency, and urgency and may be suggested by a boggy, tender prostate on rectal examination. Acute pyelonephritis usually evolves over hours to a day with fever, rigors, nausea, vomiting, and sometimes diarrhea; cystitis symptoms may be absent or present. Examination in pyelonephritis often shows fever, tachycardia, diffuse myalgias, and marked costovertebral angle tenderness. Evaluate predisposing factors for UTI or pyelonephritis, including atrophic vaginitis, which may present with reduced discharge, vaginal tenderness, postcoital spotting, and dyspareunia.
Physical Examination
Check vital signs and hydration, especially when pyelonephritis is possible. Suprapubic tenderness supports lower-tract infection, while flank tenderness suggests upper-tract involvement. Perform a genital examination when sexually transmitted infection is suspected, and perform a prostate examination in all men.
Diagnostic Tests and Interpretation
Laboratory Studies
Pyuria is the most sensitive indicator of UTI, and leukocyte esterase testing is highly sensitive for detecting infection-associated pyuria. Urine colony counts of 10^5 CFU/mL generally indicate infection, while lower thresholds (≥10^2 CFU/mL) can be diagnostic in symptomatic patients and in specimens obtained by suprapubic aspiration or catheterization. Most uropathogens convert nitrate to nitrite; nitrite positivity is highly specific but has low sensitivity. Rapid bacteriuria detection methods using techniques such as photometry or bioluminescence can yield results in one to two hours but may miss infections when lower colony counts are used as the comparison standard. Sterile pyuria suggests atypical infections such as chlamydia, ureaplasma, tuberculosis, or fungal infection and can also occur with prostatitis and noninfectious urologic conditions including stones, structural abnormalities, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis, polycystic kidney disease, and related disorders.
Treatment
Therapy for acute urethritis depends on cause. Uncomplicated lower-tract infection in women is treated with short-course antibiotics (about 3–5 days), while men or those with upper-tract disease generally require longer courses (10–14 days). Suspected or confirmed prostatitis requires prolonged therapy, typically at least four weeks. Patients with acute dysuria and frequency who have negative urine cultures and no pyuria generally do not improve with antibiotics.
Ongoing Care and Follow-Up
Many women experience cystitis during their lifetime, and recurrent episodes are common. Most recurrent UTIs represent reinfections after at least one month without symptoms and are often related to vaginal and rectal colonization with uropathogens; anatomic abnormalities are uncommon in young women with recurrent cystitis.
Complications
Lower-tract infection can ascend and cause upper-tract disease.
Basics
Description
Dysuria refers to painful urination. Acute urethral syndrome describes dysuria with urgency and frequency in the absence of significant bacteriuria.
Approach to the Patient
Irritation of urethral and bladder mucosa typically causes frequent, painful voiding of small urine volumes. Dysuria is often assumed to be a urinary tract infection and treated empirically, which can miss important diagnoses in some patients and lead to unnecessary antibiotics in others, so targeted evaluation is preferred. A focused history and examination, including pelvic and rectal examination when indicated, often clarifies the cause and enables directed therapy. Sexually transmitted infections including Chlamydia trachomatis, Neisseria gonorrhoeae, and herpes simplex virus can cause dysuria in any sex. Prostatitis is a key diagnosis in men because it is harder to eradicate and can recur. Fever is uncommon in cystitis but may occur with acute prostatitis; dysuria with fever should also raise concern for upper-tract infection such as pyelonephritis. Primary genital herpes can cause dysuria with fever, while chlamydia, gonorrhea, and nonspecific urethritis rarely cause fever unless complicated by pelvic inflammatory disease or Fitz-Hugh–Curtis syndrome. Dysuria with hematuria suggests infectious or noninfectious cystitis and also warrants consideration of tuberculous cystitis, bladder cancer, trauma, renal stones, and schistosomiasis. Dysuria with urethral or vaginal discharge suggests gonorrhea or chlamydia, nonspecific urethritis (with or without conjunctivitis and arthritis consistent with reactive arthritis), and prostatitis. Urinalysis and urine culture are standard initial tests, though young women with classic uncomplicated symptoms and no risk factors for complicated or recurrent infection may be treated empirically.
Epidemiology
Incidence
UTIs are among the most common infectious syndromes and carry substantial costs, including antibiotic expenditures exceeding one billion dollars annually in the United States. Most patients with primary symptomatic genital herpes experience dysuria, though dysuria is typically absent with recurrences. Sexual intercourse is linked to several dysuria etiologies, with symptom timing differing by syndrome: postcoital cystitis often appears within days, urethritis tends to appear after one to two weeks, and vaginitis may present weeks to months later. Pyelonephritis is a frequent cause of hospitalization, and UTIs account for over 100,000 U.S. admissions annually. Healthcare-associated infections are often UTIs, commonly catheter-related; bacteriuria develops in a substantial proportion of patients with prolonged catheterization with a daily incremental risk of infection, and even single catheterization can cause UTI. Escherichia coli causes most uncomplicated UTIs. In pregnancy, asymptomatic bacteriuria can progress to pyelonephritis and is associated with adverse obstetric outcomes including premature labor
.
Etiology
Beyond bacterial cystitis and pyelonephritis and sexually transmitted causes, dysuria may result from atrophic vaginitis, Candida-associated vaginitis, irritation from a distal urethral stone, chemical exposures, compression from an adnexal mass, radiation injury, and vaginal or urethral trauma including sexual abuse or foreign body insertion. Among women with acute dysuria and frequency, most have significant bacteriuria, and many without significant bacteriuria still have infections of the bladder, kidneys, or urethra. Ureaplasma urealyticum is often detected in symptomatic patients but is also found in asymptomatic individuals, and both U. urealyticum and Mycoplasma hominis have been identified in prostatic and renal tissues in patients with dysuria. Adenovirus can cause acute hemorrhagic cystitis in children and some young adults, sometimes in outbreaks, while other urinary viral isolates are generally not considered causes of infection in immunocompetent hosts.
Diagnosis
History
Dysuria with frequency, urgency, and suprapubic discomfort commonly reflects bladder or urethral inflammation. Prostatitis typically causes dysuria, frequency, and urgency and may be suggested by a boggy, tender prostate on rectal examination. Acute pyelonephritis usually evolves over hours to a day with fever, rigors, nausea, vomiting, and sometimes diarrhea; cystitis symptoms may be absent or present. Examination in pyelonephritis often shows fever, tachycardia, diffuse myalgias, and marked costovertebral angle tenderness. Evaluate predisposing factors for UTI or pyelonephritis, including atrophic vaginitis, which may present with reduced discharge, vaginal tenderness, postcoital spotting, and dyspareunia.
Physical Examination
Check vital signs and hydration, especially when pyelonephritis is possible. Suprapubic tenderness supports lower-tract infection, while flank tenderness suggests upper-tract involvement. Perform a genital examination when sexually transmitted infection is suspected, and perform a prostate examination in all men.
Diagnostic Tests and Interpretation
Laboratory Studies
Pyuria is the most sensitive indicator of UTI, and leukocyte esterase testing is highly sensitive for detecting infection-associated pyuria. Urine colony counts of 10^5 CFU/mL generally indicate infection, while lower thresholds (≥10^2 CFU/mL) can be diagnostic in symptomatic patients and in specimens obtained by suprapubic aspiration or catheterization. Most uropathogens convert nitrate to nitrite; nitrite positivity is highly specific but has low sensitivity. Rapid bacteriuria detection methods using techniques such as photometry or bioluminescence can yield results in one to two hours but may miss infections when lower colony counts are used as the comparison standard. Sterile pyuria suggests atypical infections such as chlamydia, ureaplasma, tuberculosis, or fungal infection and can also occur with prostatitis and noninfectious urologic conditions including stones, structural abnormalities, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis, polycystic kidney disease, and related disorders.
Treatment
Therapy for acute urethritis depends on cause. Uncomplicated lower-tract infection in women is treated with short-course antibiotics (about 3–5 days), while men or those with upper-tract disease generally require longer courses (10–14 days). Suspected or confirmed prostatitis requires prolonged therapy, typically at least four weeks. Patients with acute dysuria and frequency who have negative urine cultures and no pyuria generally do not improve with antibiotics.
Ongoing Care and Follow-Up
Many women experience cystitis during their lifetime, and recurrent episodes are common. Most recurrent UTIs represent reinfections after at least one month without symptoms and are often related to vaginal and rectal colonization with uropathogens; anatomic abnormalities are uncommon in young women with recurrent cystitis.
Complications
Lower-tract infection can ascend and cause upper-tract disease.

- Published on
Infectious Diseases and Microbiology: Diarrhea and Fever
Basics
Description
Diarrhea is defined as stool output exceeding 200 g/day and, in practice, as three or more loose stools daily. It is acute when <14 days and chronic when>4 weeks. Inflammatory diarrhea presents with frequent, small-volume stools that are mucoid and/or bloody and may include tenesmus, fever, or severe abdominal pain; stool leukocytes are a key feature. Noninflammatory diarrhea is typically watery, may be high volume (>1 L/day), and occurs without blood, pus, severe pain, or fever.
Epidemiology
Incidence
In the United States, acute diarrhea occurs hundreds of millions of times yearly, with tens of millions of episodes linked to identified pathogens, and foodborne spread accounting for a large proportion of known-pathogen disease. Surveillance data have identified non-typhoidal Salmonella, Campylobacter, Shigella, Cryptosporidium, and Shiga toxin–producing E. coli O157 as leading reported causes, with highest bacterial diarrhea rates from Salmonella, Campylobacter, and Yersinia in infants under one year. Post-diarrheal hemolytic uremic syndrome occurs infrequently overall but is most common in children under five. Traveler’s diarrhea affects a substantial fraction of international travelers.
Risk Factors
Risks include consuming undercooked eggs, meat, poultry, seafood, or unpasteurized dairy, and drinking untreated surface water. Greater severity or pathogen-specific risk occurs with HIV, immunosuppressive therapies (including glucocorticoids, TNF inhibitors, and chemotherapy), recent antibiotic exposure, liver disease, neutropenia, malnutrition, zinc deficiency, and IgA deficiency. Oral–anal sexual contact increases risk of enteric infection. Antibiotic exposure is a major risk factor for Clostridioides difficile–associated diarrhea.
General Prevention
Handwashing before eating or food preparation, avoiding undercooked animal products and unpasteurized dairy, and avoiding untreated stream or river water reduce risk. During travel in areas with unsafe water, avoid tap water and ice. Typhoid vaccination is available for travelers, and infant rotavirus vaccination is recommended in the United States; destination-based vaccine guidance is available through travel medicine resources.
Etiology
Bacterial causes include Campylobacter, Salmonella, Shigella, Yersinia enterocolitica, C. difficile, Vibrio cholerae, Vibrio parahaemolyticus, Aeromonas, Plesiomonas shigelloides, and multiple diarrheagenic E. coli pathotypes including ETEC, EPEC, EIEC, STEC (including O157:H7), and EAEC. Viral causes include rotavirus, human caliciviruses such as norovirus, adenovirus, and cytomegalovirus. Parasitic causes include Giardia intestinalis, Cryptosporidium parvum, Entamoeba histolytica, Cyclospora cayetanensis, Isospora belli, and Strongyloides stercoralis. Toxin-mediated syndromes include Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens.
Diagnosis
History
Evaluation should define likely cause, illness severity, and complications. Ask about travel, diet, antibiotic use, sexual practices, day-care exposure, sick contacts, outbreaks, seasonality, and other illnesses, and characterize stool frequency, duration, and appearance. Infectious diarrhea may include fever, chills, vomiting, nausea, abdominal pain, and tenesmus. Dizziness, presyncope, or syncope suggests volume depletion. Dysentery points to invasive pathogens such as Shigella, Salmonella, Campylobacter, STEC (often without fever), or Yersinia. STEC commonly starts watery and becomes bloody and is frequently associated with contaminated beef or produce; fever is often absent. Yersinia and Salmonella may involve the terminal ileum and cecum, producing right lower quadrant pain that mimics appendicitis. Watery diarrhea alone is nonspecific. Enterotoxin-mediated food poisoning from S. aureus, B. cereus, or C. perfringens typically has a short incubation and brief course, with vomiting alone more typical of S. aureus or C. perfringens and watery diarrhea more typical of B. cereus or C. perfringens; fever is usually absent. Extraintestinal features such as arthritis, skin lesions, or eye symptoms suggest inflammatory bowel disease. With recent international travel, likely pathogens depend on location, setting, and season, commonly including ETEC, EAEC, Campylobacter, Salmonella, and norovirus, and travel medicine resources can guide evaluation.
Physical Examination
Assess blood pressure, heart rate, respiratory rate, temperature, and mental status to gauge severity. Look for dehydration signs such as dry mucous membranes, reduced skin turgor, sunken eyes, delayed capillary refill, low jugular venous pressure, and orthostatic hypotension. Examine for abdominal tenderness, peritoneal signs, hepatomegaly, and splenomegaly.
Diagnostic Tests and Interpretation
Laboratory Studies
Testing is indicated with fever, systemic toxicity, bloody stools, dehydration, suspected foodborne outbreak, recent international travel, immunosuppression, or recent antibiotic exposure. Send stool for culture, noting that routine processing commonly targets Shigella, Salmonella, and Campylobacter, so the laboratory should be alerted if suspicion is high for STEC or other E. coli pathotypes, Yersinia, Vibrio, or other organisms. Stool culture yield is generally low. For bloody diarrhea, culture for Salmonella, Shigella, Campylobacter, and STEC and obtain a Shiga toxin immunoassay; if E. coli is isolated, arrange serotyping via a reference laboratory. If there is recent antibiotic exposure, recent hospitalization, day-care exposure, or recent chemotherapy, test stool for C. difficile toxins. If diarrhea persists beyond seven days, submit multiple stools for ova and parasite examination with attention to Giardia, Cryptosporidium, Isospora, and Cyclospora and consider noninfectious causes; in AIDS or immunosuppression, also evaluate for microsporidia, Mycobacterium avium complex, and cytomegalovirus. Fecal polymorphonuclear cells support an inflammatory process. If dehydration or severe illness is present, obtain electrolytes, renal and liver function tests, complete blood count, and blood cultures.
Imaging
If the diagnosis remains unclear in critical illness, with prominent abdominal pain or peritoneal signs, consider CT abdomen with oral and intravenous contrast.
t
Diagnostic Procedures/Other
Further evaluation may require upper endoscopy or colonoscopy with biopsies
.
Differential Diagnosis
Acute inflammatory diarrhea may be noninfectious, including ulcerative colitis, Crohn disease, radiation or ischemic colitis, partial obstruction, diverticulitis, laxative abuse, rectosigmoid abscess, Whipple disease, pernicious anemia, diabetes-related enteropathy, malabsorption disorders, scleroderma, or celiac disease. Fever and diarrhea can also result from infections outside the gut such as malaria or sepsis.
Treatment
Medications
Core management is rehydration with selective antibiotic use. Oral rehydration is effective and cost-efficient across settings, while intravenous fluids are indicated for severe dehydration or major electrolyte disturbances; rice-based oral solutions are superior for cholera in children and adults. Antibiotics are recommended for severe infection and for persistent gastroenteritis and are favored in adults over 65, immunocompromised patients, those with prosthetic material, and invasive infections, except when STEC is suspected or confirmed. Empiric therapy for febrile community-acquired invasive diarrhea or moderate to severe traveler’s diarrhea includes ciprofloxacin 500 mg twice daily or levofloxacin 500 mg daily while awaiting studies unless STEC is suspected; travel to Southeast Asia raises concern for fluoroquinolone-resistant Campylobacter. For suspected antibiotic-associated or nosocomial diarrhea, treat empirically with metronidazole or vancomycin while awaiting C. difficile testing. Pathogen-directed therapy includes treating non-typhoidal Salmonella in high-risk or severe disease with fluoroquinolones, TMP-SMX, or ceftriaxone for typical short courses and longer courses in immunocompromised patients, recognizing antibiotics may prolong shedding; treating Shigella with short-course fluoroquinolones or TMP-SMX when susceptible and longer courses for severe or immunocompromised cases; treating Campylobacter with erythromycin while acknowledging high fluoroquinolone resistance especially in Southeast Asia; avoiding antibiotics in STEC due to increased HUS risk and providing supportive care; treating ETEC/EPEC/EIEC similarly to traveler’s diarrhea regimens; usually avoiding antibiotics in Yersinia unless severe or immunocompromised, in which case doxycycline plus an aminoglycoside, fluoroquinolones, or TMP-SMX may be used; managing C. difficile by stopping unnecessary antibiotics and using metronidazole for milder disease or oral vancomycin for 10–14 days; prioritizing fluids in cholera with antibiotics guided by local resistance; treating amebiasis with metronidazole followed by a luminal agent such as paromomycin or iodoquinol; treating giardiasis with metronidazole or single-dose tinidazole; and treating Cyclospora or Isospora with TMP-SMX with extended therapy and possible suppression in immunocompromised hosts.
Additional Treatment
Most mild cases resolve without specific therapy; supportive care includes hydration and symptom control. Loperamide is preferred for adults with mild to moderate nonbloody diarrhea but is contraindicated in severe inflammatory diarrhea, bloody diarrhea, C. difficile infection, and in children under two. Bismuth subsalicylate can reduce stool volume in adults and children. Severe or persistent unexplained diarrhea warrants gastroenterology and/or infectious diseases consultation, and cases due to major reportable pathogens or suspected outbreaks should be reported to public health authorities.
In-Patient Considerations
Initial Stabilization
Severe acute inflammatory diarrhea with systemic toxicity requires rapid rehydration and empiric antibiotics.
Admission Criteria
Hospitalize patients with severe dehydration or inability to maintain oral intake.
IV Fluids
Use intravenous volume repletion for severe dehydration or altered mental status.
Discharge Criteria
Discharge is appropriate when fever has been absent for more than 24 hours, vital signs are stable, and the patient can maintain adequate oral fluids and nutrition.
Ongoing Care and Follow-Up
Evaluate and treat household members with similar symptoms when appropriate.
Diet
Resume food about four hours after starting rehydration, using small frequent meals of easily digestible foods, and avoid hyperosmolar fruit juices that can worsen diarrhea.
Patient Education
Counsel on food safety and strategies to prevent foodborne illness, especially during travel.
Prognosis
Gastrointestinal illness contributes to a large burden of hospitalization and death annually in the United States.
Complications
Potential complications include dehydration, electrolyte derangements, bacteremia and sepsis, malnutrition and vitamin loss, hemolytic uremic syndrome, and systemic amebiasis.
Basics
Description
Diarrhea is defined as stool output exceeding 200 g/day and, in practice, as three or more loose stools daily. It is acute when <14 days and chronic when>4 weeks. Inflammatory diarrhea presents with frequent, small-volume stools that are mucoid and/or bloody and may include tenesmus, fever, or severe abdominal pain; stool leukocytes are a key feature. Noninflammatory diarrhea is typically watery, may be high volume (>1 L/day), and occurs without blood, pus, severe pain, or fever.
Epidemiology
Incidence
In the United States, acute diarrhea occurs hundreds of millions of times yearly, with tens of millions of episodes linked to identified pathogens, and foodborne spread accounting for a large proportion of known-pathogen disease. Surveillance data have identified non-typhoidal Salmonella, Campylobacter, Shigella, Cryptosporidium, and Shiga toxin–producing E. coli O157 as leading reported causes, with highest bacterial diarrhea rates from Salmonella, Campylobacter, and Yersinia in infants under one year. Post-diarrheal hemolytic uremic syndrome occurs infrequently overall but is most common in children under five. Traveler’s diarrhea affects a substantial fraction of international travelers.
Risk Factors
Risks include consuming undercooked eggs, meat, poultry, seafood, or unpasteurized dairy, and drinking untreated surface water. Greater severity or pathogen-specific risk occurs with HIV, immunosuppressive therapies (including glucocorticoids, TNF inhibitors, and chemotherapy), recent antibiotic exposure, liver disease, neutropenia, malnutrition, zinc deficiency, and IgA deficiency. Oral–anal sexual contact increases risk of enteric infection. Antibiotic exposure is a major risk factor for Clostridioides difficile–associated diarrhea.
General Prevention
Handwashing before eating or food preparation, avoiding undercooked animal products and unpasteurized dairy, and avoiding untreated stream or river water reduce risk. During travel in areas with unsafe water, avoid tap water and ice. Typhoid vaccination is available for travelers, and infant rotavirus vaccination is recommended in the United States; destination-based vaccine guidance is available through travel medicine resources.
Etiology
Bacterial causes include Campylobacter, Salmonella, Shigella, Yersinia enterocolitica, C. difficile, Vibrio cholerae, Vibrio parahaemolyticus, Aeromonas, Plesiomonas shigelloides, and multiple diarrheagenic E. coli pathotypes including ETEC, EPEC, EIEC, STEC (including O157:H7), and EAEC. Viral causes include rotavirus, human caliciviruses such as norovirus, adenovirus, and cytomegalovirus. Parasitic causes include Giardia intestinalis, Cryptosporidium parvum, Entamoeba histolytica, Cyclospora cayetanensis, Isospora belli, and Strongyloides stercoralis. Toxin-mediated syndromes include Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens.
Diagnosis
History
Evaluation should define likely cause, illness severity, and complications. Ask about travel, diet, antibiotic use, sexual practices, day-care exposure, sick contacts, outbreaks, seasonality, and other illnesses, and characterize stool frequency, duration, and appearance. Infectious diarrhea may include fever, chills, vomiting, nausea, abdominal pain, and tenesmus. Dizziness, presyncope, or syncope suggests volume depletion. Dysentery points to invasive pathogens such as Shigella, Salmonella, Campylobacter, STEC (often without fever), or Yersinia. STEC commonly starts watery and becomes bloody and is frequently associated with contaminated beef or produce; fever is often absent. Yersinia and Salmonella may involve the terminal ileum and cecum, producing right lower quadrant pain that mimics appendicitis. Watery diarrhea alone is nonspecific. Enterotoxin-mediated food poisoning from S. aureus, B. cereus, or C. perfringens typically has a short incubation and brief course, with vomiting alone more typical of S. aureus or C. perfringens and watery diarrhea more typical of B. cereus or C. perfringens; fever is usually absent. Extraintestinal features such as arthritis, skin lesions, or eye symptoms suggest inflammatory bowel disease. With recent international travel, likely pathogens depend on location, setting, and season, commonly including ETEC, EAEC, Campylobacter, Salmonella, and norovirus, and travel medicine resources can guide evaluation.
Physical Examination
Assess blood pressure, heart rate, respiratory rate, temperature, and mental status to gauge severity. Look for dehydration signs such as dry mucous membranes, reduced skin turgor, sunken eyes, delayed capillary refill, low jugular venous pressure, and orthostatic hypotension. Examine for abdominal tenderness, peritoneal signs, hepatomegaly, and splenomegaly.
Diagnostic Tests and Interpretation
Laboratory Studies
Testing is indicated with fever, systemic toxicity, bloody stools, dehydration, suspected foodborne outbreak, recent international travel, immunosuppression, or recent antibiotic exposure. Send stool for culture, noting that routine processing commonly targets Shigella, Salmonella, and Campylobacter, so the laboratory should be alerted if suspicion is high for STEC or other E. coli pathotypes, Yersinia, Vibrio, or other organisms. Stool culture yield is generally low. For bloody diarrhea, culture for Salmonella, Shigella, Campylobacter, and STEC and obtain a Shiga toxin immunoassay; if E. coli is isolated, arrange serotyping via a reference laboratory. If there is recent antibiotic exposure, recent hospitalization, day-care exposure, or recent chemotherapy, test stool for C. difficile toxins. If diarrhea persists beyond seven days, submit multiple stools for ova and parasite examination with attention to Giardia, Cryptosporidium, Isospora, and Cyclospora and consider noninfectious causes; in AIDS or immunosuppression, also evaluate for microsporidia, Mycobacterium avium complex, and cytomegalovirus. Fecal polymorphonuclear cells support an inflammatory process. If dehydration or severe illness is present, obtain electrolytes, renal and liver function tests, complete blood count, and blood cultures.
Imaging
If the diagnosis remains unclear in critical illness, with prominent abdominal pain or peritoneal signs, consider CT abdomen with oral and intravenous contrast.
t
Diagnostic Procedures/Other
Further evaluation may require upper endoscopy or colonoscopy with biopsies
.
Differential Diagnosis
Acute inflammatory diarrhea may be noninfectious, including ulcerative colitis, Crohn disease, radiation or ischemic colitis, partial obstruction, diverticulitis, laxative abuse, rectosigmoid abscess, Whipple disease, pernicious anemia, diabetes-related enteropathy, malabsorption disorders, scleroderma, or celiac disease. Fever and diarrhea can also result from infections outside the gut such as malaria or sepsis.
Treatment
Medications
Core management is rehydration with selective antibiotic use. Oral rehydration is effective and cost-efficient across settings, while intravenous fluids are indicated for severe dehydration or major electrolyte disturbances; rice-based oral solutions are superior for cholera in children and adults. Antibiotics are recommended for severe infection and for persistent gastroenteritis and are favored in adults over 65, immunocompromised patients, those with prosthetic material, and invasive infections, except when STEC is suspected or confirmed. Empiric therapy for febrile community-acquired invasive diarrhea or moderate to severe traveler’s diarrhea includes ciprofloxacin 500 mg twice daily or levofloxacin 500 mg daily while awaiting studies unless STEC is suspected; travel to Southeast Asia raises concern for fluoroquinolone-resistant Campylobacter. For suspected antibiotic-associated or nosocomial diarrhea, treat empirically with metronidazole or vancomycin while awaiting C. difficile testing. Pathogen-directed therapy includes treating non-typhoidal Salmonella in high-risk or severe disease with fluoroquinolones, TMP-SMX, or ceftriaxone for typical short courses and longer courses in immunocompromised patients, recognizing antibiotics may prolong shedding; treating Shigella with short-course fluoroquinolones or TMP-SMX when susceptible and longer courses for severe or immunocompromised cases; treating Campylobacter with erythromycin while acknowledging high fluoroquinolone resistance especially in Southeast Asia; avoiding antibiotics in STEC due to increased HUS risk and providing supportive care; treating ETEC/EPEC/EIEC similarly to traveler’s diarrhea regimens; usually avoiding antibiotics in Yersinia unless severe or immunocompromised, in which case doxycycline plus an aminoglycoside, fluoroquinolones, or TMP-SMX may be used; managing C. difficile by stopping unnecessary antibiotics and using metronidazole for milder disease or oral vancomycin for 10–14 days; prioritizing fluids in cholera with antibiotics guided by local resistance; treating amebiasis with metronidazole followed by a luminal agent such as paromomycin or iodoquinol; treating giardiasis with metronidazole or single-dose tinidazole; and treating Cyclospora or Isospora with TMP-SMX with extended therapy and possible suppression in immunocompromised hosts.
Additional Treatment
Most mild cases resolve without specific therapy; supportive care includes hydration and symptom control. Loperamide is preferred for adults with mild to moderate nonbloody diarrhea but is contraindicated in severe inflammatory diarrhea, bloody diarrhea, C. difficile infection, and in children under two. Bismuth subsalicylate can reduce stool volume in adults and children. Severe or persistent unexplained diarrhea warrants gastroenterology and/or infectious diseases consultation, and cases due to major reportable pathogens or suspected outbreaks should be reported to public health authorities.
In-Patient Considerations
Initial Stabilization
Severe acute inflammatory diarrhea with systemic toxicity requires rapid rehydration and empiric antibiotics.
Admission Criteria
Hospitalize patients with severe dehydration or inability to maintain oral intake.
IV Fluids
Use intravenous volume repletion for severe dehydration or altered mental status.
Discharge Criteria
Discharge is appropriate when fever has been absent for more than 24 hours, vital signs are stable, and the patient can maintain adequate oral fluids and nutrition.
Ongoing Care and Follow-Up
Evaluate and treat household members with similar symptoms when appropriate.
Diet
Resume food about four hours after starting rehydration, using small frequent meals of easily digestible foods, and avoid hyperosmolar fruit juices that can worsen diarrhea.
Patient Education
Counsel on food safety and strategies to prevent foodborne illness, especially during travel.
Prognosis
Gastrointestinal illness contributes to a large burden of hospitalization and death annually in the United States.
Complications
Potential complications include dehydration, electrolyte derangements, bacteremia and sepsis, malnutrition and vitamin loss, hemolytic uremic syndrome, and systemic amebiasis.
- Published on
Infectious Diseases and Microbiology: Low Back Pain and Fever
Basics
Description
Back pain refers to acute or chronic pain arising from the spine or paraspinal structures. The combination of back pain and fever requires careful evaluation for nonmechanical causes. History should specifically assess weight loss, pain worse when lying down, morning stiffness, and sudden severe or colicky pain. Serial spinal and neurologic examinations are crucial, and any spinal tenderness or focal pain warrants full diagnostic assessment. Vertebral osteomyelitis is commonly suggested by pain worsened by movement and not relieved by rest, focal vertebral tenderness, and elevated erythrocyte sedimentation rate. Pain from neoplastic nerve infiltration is typically constant, progressively worse, and persists at night without relief, whereas mechanical low back pain usually improves with rest. Work-up often begins with plain radiography followed by bone scintigraphy, MRI, CT, laboratory testing, and biopsy based on abnormal findings.
Epidemiology
A definitive pain source is difficult to establish and is identified in fewer than one-quarter of cases. Mechanical causes account for about 97% of low back pain, with degenerative disk disease and lumbar sprain/strain comprising most cases. The spine is a frequent site of bone metastasis. Vertebral osteomyelitis is uncommon at roughly 1 per 100,000 persons annually, with rising rates attributed to vascular devices and intravenous drug use; it occurs more often in early childhood and in adults over 50. Spinal epidural abscess occurs in about 1 per 10,000 hospital admissions per year, and MRSA-related vertebral osteomyelitis and epidural abscess are increasingly reported. Despite global increases in tuberculosis, the rate of extrapulmonary spinal disease remains relatively stable; Pott disease, typically involving the lower thoracic vertebrae, is the most common musculoskeletal extrapulmonary manifestation. Improved survival in sickle cell disease has been accompanied by more Salmonella vertebral osteomyelitis.
Risk Factors
Infectious complications can follow bites from many animals, often linked to occupational exposure (farmers, laboratory workers, veterinarians) or recreation (hunters, campers, exotic pet owners). Systemic infection after animal or human bites is more likely with extremity edema or impaired lymphatic drainage and in immunocompromised hosts. Fever after a dog bite in an immunosuppressed patient should prompt concern for invasive Capnocytophaga canimorsus infection.
Etiology
Infectious sources of back pain with fever include biliary tract infection, chronic prostatitis, herpes zoster, pyelonephritis, retroperitoneal abscess, spinal epidural abscess, and vertebral osteomyelitis. Noninfectious causes include colonic cancer, pancreatic disease, histiocytosis X, metastatic malignancy (breast, lung, prostate, thyroid, kidney, gastrointestinal tract), multiple myeloma, neoplastic invasion of pelvic nerves, lymphoma, pregnancy, vertebral fracture, renal artery or vein thrombosis, renal stones, retroperitoneal hemorrhage or tumors, and tumors of the posterior stomach or duodenum. Staphylococcus aureus is the leading cause of spinal epidural abscess, accounting for most reported cases, with additional pathogens including Actinomyces israelii, Aspergillus, Blastomyces, Brucella, Cryptococcus, Haemophilus parainfluenzae, Mycobacterium tuberculosis, and Streptococcus milleri. Vertebral osteomyelitis is most often due to staphylococci but may be caused by other bacteria or tuberculosis; one multicenter retrospective study from southern Spain reported a high proportion due to Brucella, with the remainder split between pyogenic and tuberculous disease.
Commonly Associated Conditions
Vertebral osteomyelitis and spinal epidural abscess are frequently associated with diabetes, injection drug use, chronic renal failure, alcohol use disorder, bacteremia or focal infections, and malignancy. Most epidural abscesses arise via hematogenous spread from skin or mucosal sources, though direct extension from adjacent infection is also recognized. Postoperative abscesses account for a substantial minority, and epidural catheter placement is another risk factor. Blunt trauma may precede symptoms and may lead to an epidural hematoma that later becomes infected.
Diagnosis
Spinal epidural abscess classically presents with fever, spinal pain and tenderness, and radicular pain progressing to limb weakness, with pain being the most consistent feature. Early on, spinal pain with or without fever may be the only findings before sudden neurologic decline. When sepsis dominates or when patients are bedbound, neurologic deficits may be missed. Fever is absent in a notable minority of pyogenic vertebral osteomyelitis cases and is even more commonly absent in tuberculous vertebral osteomyelitis.
History
Key elements include age; systemic symptoms such as fever, weakness, weight loss, and night sweats; prior trauma, infection, or cancer; pain characteristics; immune status; glycemic control in diabetes; and injection drug use. Screen for neurologic complaints including weakness, paresthesias, numbness, and bowel, bladder, or sexual dysfunction. Risk is higher in patients over 50, those using steroids, individuals with HIV, those on immunosuppressants, and those with prior surgery.
Physical Examination
Assess general appearance, vital signs, peripheral pulses, and perform a focused cardiopulmonary and abdominal evaluation in unstable patients. Look for referred pain by examining potential primary sources of tenderness. Perform a complete neurologic examination to evaluate for spinal cord compromise and localize deficits; lesions below T12 can produce lower motor neuron findings, and cauda equina syndrome may include bowel or bladder incontinence. In older adults, fever may be low-grade and does not reliably indicate severity. Percussion of spinous processes may reveal focal vertebral tenderness due to trauma, malignancy, or infection. Examine for signs of endocarditis and septic emboli.
Diagnostic Tests and Interpretation
Laboratory Studies
Routine blood tests are often nonspecific for vertebral osteomyelitis, but leukocytosis, neutrophilia, and markedly elevated ESR and C-reactive protein support pyogenic disease. Blood cultures are the most useful routine test and identify the organism in about half of pyogenic and Brucella vertebral osteomyelitis cases. Bone biopsy is often required to confirm the diagnosis, especially in tuberculous disease.
Imaging
Plain spinal radiographs may be normal early in vertebral osteomyelitis. MRI best defines the extent and location of spinal epidural abscess. MRI or CT myelography is preferred when spinal metastasis is suspected.
Diagnostic Procedures/Other
CT-guided needle biopsy reliably diagnoses carcinoma but is less dependable for lymphoma, though performance has improved with CT guidance, immunophenotyping, and larger needles; false-negative rates remain significant. Establishing an etiologic diagnosis of vertebral osteomyelitis often requires percutaneous or surgical vertebral biopsy.
Differential Diagnosis
Tuberculosis may appear early as an opportunistic infection in AIDS and can be AIDS-defining, while Mycobacterium avium complex typically occurs later with very low CD4 counts. Pertussis should be considered when cough is the predominant symptom, particularly with paroxysms, inspiratory whoop, posttussive vomiting, sleep-disrupting cough, or exposure to similar illness.
Treatment
Medications
Suspected vertebral osteomyelitis or epidural abscess warrants empiric vancomycin to cover MRSA, with addition of a third- or fourth-generation cephalosporin when gram-negative bacteremia is suspected, especially with concurrent pyelonephritis. Therapy should be narrowed once the pathogen is identified; for methicillin-sensitive S. aureus, options include nafcillin, oxacillin, or cefazolin. Typical duration is at least six weeks. Management of tuberculous, brucellar, and salmonella bone disease follows their respective regimens. Corticosteroids may help in acute spinal cord compression. NSAIDs provide symptomatic analgesia, and bisphosphonates may be used for fractures related to breast cancer metastases.
Additional Treatment
Prompt diagnosis with targeted therapy is essential. Epidural abscess requires urgent surgical management with early decompression plus antibiotics. Spinal cord compression is a neurosurgical emergency, and decompression via surgery or radiotherapy within 24 hours of symptom onset is needed to reduce permanent neurologic injury. In suspected spinal or paraspinal infection, bactericidal empiric antibiotics should be started immediately.
.
Ongoing Care and Follow-Up
If symptoms persist beyond six weeks, repeat laboratory testing and imaging are recommended. After six weeks of antibiotics for osteomyelitis or epidural abscess, reassessment is needed to determine whether treatment should continue. Ongoing monitoring for medication toxicity is important, particularly in older adults who are more susceptible to adverse drug effects.
Basics
Description
Back pain refers to acute or chronic pain arising from the spine or paraspinal structures. The combination of back pain and fever requires careful evaluation for nonmechanical causes. History should specifically assess weight loss, pain worse when lying down, morning stiffness, and sudden severe or colicky pain. Serial spinal and neurologic examinations are crucial, and any spinal tenderness or focal pain warrants full diagnostic assessment. Vertebral osteomyelitis is commonly suggested by pain worsened by movement and not relieved by rest, focal vertebral tenderness, and elevated erythrocyte sedimentation rate. Pain from neoplastic nerve infiltration is typically constant, progressively worse, and persists at night without relief, whereas mechanical low back pain usually improves with rest. Work-up often begins with plain radiography followed by bone scintigraphy, MRI, CT, laboratory testing, and biopsy based on abnormal findings.
Epidemiology
A definitive pain source is difficult to establish and is identified in fewer than one-quarter of cases. Mechanical causes account for about 97% of low back pain, with degenerative disk disease and lumbar sprain/strain comprising most cases. The spine is a frequent site of bone metastasis. Vertebral osteomyelitis is uncommon at roughly 1 per 100,000 persons annually, with rising rates attributed to vascular devices and intravenous drug use; it occurs more often in early childhood and in adults over 50. Spinal epidural abscess occurs in about 1 per 10,000 hospital admissions per year, and MRSA-related vertebral osteomyelitis and epidural abscess are increasingly reported. Despite global increases in tuberculosis, the rate of extrapulmonary spinal disease remains relatively stable; Pott disease, typically involving the lower thoracic vertebrae, is the most common musculoskeletal extrapulmonary manifestation. Improved survival in sickle cell disease has been accompanied by more Salmonella vertebral osteomyelitis.
Risk Factors
Infectious complications can follow bites from many animals, often linked to occupational exposure (farmers, laboratory workers, veterinarians) or recreation (hunters, campers, exotic pet owners). Systemic infection after animal or human bites is more likely with extremity edema or impaired lymphatic drainage and in immunocompromised hosts. Fever after a dog bite in an immunosuppressed patient should prompt concern for invasive Capnocytophaga canimorsus infection.
Etiology
Infectious sources of back pain with fever include biliary tract infection, chronic prostatitis, herpes zoster, pyelonephritis, retroperitoneal abscess, spinal epidural abscess, and vertebral osteomyelitis. Noninfectious causes include colonic cancer, pancreatic disease, histiocytosis X, metastatic malignancy (breast, lung, prostate, thyroid, kidney, gastrointestinal tract), multiple myeloma, neoplastic invasion of pelvic nerves, lymphoma, pregnancy, vertebral fracture, renal artery or vein thrombosis, renal stones, retroperitoneal hemorrhage or tumors, and tumors of the posterior stomach or duodenum. Staphylococcus aureus is the leading cause of spinal epidural abscess, accounting for most reported cases, with additional pathogens including Actinomyces israelii, Aspergillus, Blastomyces, Brucella, Cryptococcus, Haemophilus parainfluenzae, Mycobacterium tuberculosis, and Streptococcus milleri. Vertebral osteomyelitis is most often due to staphylococci but may be caused by other bacteria or tuberculosis; one multicenter retrospective study from southern Spain reported a high proportion due to Brucella, with the remainder split between pyogenic and tuberculous disease.
Commonly Associated Conditions
Vertebral osteomyelitis and spinal epidural abscess are frequently associated with diabetes, injection drug use, chronic renal failure, alcohol use disorder, bacteremia or focal infections, and malignancy. Most epidural abscesses arise via hematogenous spread from skin or mucosal sources, though direct extension from adjacent infection is also recognized. Postoperative abscesses account for a substantial minority, and epidural catheter placement is another risk factor. Blunt trauma may precede symptoms and may lead to an epidural hematoma that later becomes infected.
Diagnosis
Spinal epidural abscess classically presents with fever, spinal pain and tenderness, and radicular pain progressing to limb weakness, with pain being the most consistent feature. Early on, spinal pain with or without fever may be the only findings before sudden neurologic decline. When sepsis dominates or when patients are bedbound, neurologic deficits may be missed. Fever is absent in a notable minority of pyogenic vertebral osteomyelitis cases and is even more commonly absent in tuberculous vertebral osteomyelitis.
History
Key elements include age; systemic symptoms such as fever, weakness, weight loss, and night sweats; prior trauma, infection, or cancer; pain characteristics; immune status; glycemic control in diabetes; and injection drug use. Screen for neurologic complaints including weakness, paresthesias, numbness, and bowel, bladder, or sexual dysfunction. Risk is higher in patients over 50, those using steroids, individuals with HIV, those on immunosuppressants, and those with prior surgery.
Physical Examination
Assess general appearance, vital signs, peripheral pulses, and perform a focused cardiopulmonary and abdominal evaluation in unstable patients. Look for referred pain by examining potential primary sources of tenderness. Perform a complete neurologic examination to evaluate for spinal cord compromise and localize deficits; lesions below T12 can produce lower motor neuron findings, and cauda equina syndrome may include bowel or bladder incontinence. In older adults, fever may be low-grade and does not reliably indicate severity. Percussion of spinous processes may reveal focal vertebral tenderness due to trauma, malignancy, or infection. Examine for signs of endocarditis and septic emboli.
Diagnostic Tests and Interpretation
Laboratory Studies
Routine blood tests are often nonspecific for vertebral osteomyelitis, but leukocytosis, neutrophilia, and markedly elevated ESR and C-reactive protein support pyogenic disease. Blood cultures are the most useful routine test and identify the organism in about half of pyogenic and Brucella vertebral osteomyelitis cases. Bone biopsy is often required to confirm the diagnosis, especially in tuberculous disease.
Imaging
Plain spinal radiographs may be normal early in vertebral osteomyelitis. MRI best defines the extent and location of spinal epidural abscess. MRI or CT myelography is preferred when spinal metastasis is suspected.
Diagnostic Procedures/Other
CT-guided needle biopsy reliably diagnoses carcinoma but is less dependable for lymphoma, though performance has improved with CT guidance, immunophenotyping, and larger needles; false-negative rates remain significant. Establishing an etiologic diagnosis of vertebral osteomyelitis often requires percutaneous or surgical vertebral biopsy.
Differential Diagnosis
Tuberculosis may appear early as an opportunistic infection in AIDS and can be AIDS-defining, while Mycobacterium avium complex typically occurs later with very low CD4 counts. Pertussis should be considered when cough is the predominant symptom, particularly with paroxysms, inspiratory whoop, posttussive vomiting, sleep-disrupting cough, or exposure to similar illness.
Treatment
Medications
Suspected vertebral osteomyelitis or epidural abscess warrants empiric vancomycin to cover MRSA, with addition of a third- or fourth-generation cephalosporin when gram-negative bacteremia is suspected, especially with concurrent pyelonephritis. Therapy should be narrowed once the pathogen is identified; for methicillin-sensitive S. aureus, options include nafcillin, oxacillin, or cefazolin. Typical duration is at least six weeks. Management of tuberculous, brucellar, and salmonella bone disease follows their respective regimens. Corticosteroids may help in acute spinal cord compression. NSAIDs provide symptomatic analgesia, and bisphosphonates may be used for fractures related to breast cancer metastases.
Additional Treatment
Prompt diagnosis with targeted therapy is essential. Epidural abscess requires urgent surgical management with early decompression plus antibiotics. Spinal cord compression is a neurosurgical emergency, and decompression via surgery or radiotherapy within 24 hours of symptom onset is needed to reduce permanent neurologic injury. In suspected spinal or paraspinal infection, bactericidal empiric antibiotics should be started immediately.
.
Ongoing Care and Follow-Up
If symptoms persist beyond six weeks, repeat laboratory testing and imaging are recommended. After six weeks of antibiotics for osteomyelitis or epidural abscess, reassessment is needed to determine whether treatment should continue. Ongoing monitoring for medication toxicity is important, particularly in older adults who are more susceptible to adverse drug effects.
- Published on
Infectious Diseases and Microbiology: Animal Bite and Clenched-Fist Injury–Related Infections
Basics
Description and Definition
Animal bites produce puncture wounds, scratches, or lacerations with variable tissue injury, while clenched-fist injuries and human bites result from tooth penetration and inoculation of oral flora into the skin.
Approach to the Patient
Immediate assessment focuses on identifying life- or limb-threatening injury, hemorrhage, and neurovascular compromise with a detailed neurologic and vascular examination of the affected area. Patients showing signs of shock require prompt hemodynamic stabilization, empiric antibiotics, and possible surgical consultation. It is critical to determine whether the bite involves a venomous species and to thoroughly explore wounds for deep structural injury involving tendons, vessels, nerves, joints, or organs, as well as retained foreign bodies such as teeth. Copious irrigation with sterile water or saline and meticulous debridement of devitalized tissue and debris are essential and often require local anesthesia. Wounds should be kept moist with topical antibacterial agents and covered to reduce microbial load. After adequate debridement and high-pressure irrigation, select wounds, including some on the hands and feet, may undergo primary closure, but most animal and human bite injuries should heal by secondary intention. Close follow-up is mandatory due to high infection risk. Imaging with radiography, CT, or MRI may be required to detect foreign bodies or deep injury. Bites to the hands and feet frequently warrant surgical evaluation because deep-space and tendon sheath infections can rapidly progress to sepsis and permanent damage. Tetanus and rabies prophylaxis must be addressed, and suspicious human bites should raise concern for child or domestic abuse.
Epidemiology
In the United States, approximately 40% of households own dogs and about one-third own cats. Children are the most common victims of animal bites and frequently sustain injuries to the head and neck. Around 2.5% of dog bites show clinical infection at the time of presentation.
Risk Factors
Severe outcomes are more likely in children due to exposure of the head, neck, and upper torso; in veterinarians and animal handlers; in immunocompromised individuals including those with HIV, malignancy, chemotherapy exposure, steroid use, asplenia, or liver disease; and in patients with diabetes mellitus who have impaired wound healing from vascular disease and neuropathy.
Etiology
Bite-related infections are typically polymicrobial, involving aerobic and anaerobic organisms derived from the biter’s oral flora and the victim’s skin flora, with methicillin-resistant Staphylococcus aureus commonly introduced from human skin. Dog bites are frequently associated with Capnocytophaga species and Pasteurella canis, while cat bites commonly yield Pasteurella multocida. Other zoonotic pathogens include Bartonella henselae, Francisella tularensis, and Leptospira species. Additional aerobic organisms include streptococci, staphylococci, Moraxella, and Neisseria, with anaerobes such as Fusobacterium, Bacteroides, Porphyromonas, and Prevotella contributing to mixed infections. Human bites often involve Streptococcus species, Staphylococcus aureus, Eikenella corrodens, Haemophilus influenzae, and anaerobes including Fusobacterium nucleatum, Prevotella, Porphyromonas, Peptococcus, and Peptostreptococcus. Aquatic animal bites may introduce Aeromonas, Vibrio species, Erysipelothrix, or Mycobacterium marinum. Rodents and rodent predators can transmit Streptobacillus moniliformis or Spirillum species, causing rat-bite fever.
Diagnosis
History
The history should clarify events surrounding the injury, characteristics of the biting animal including species, venom potential, vaccination status, and availability for rabies observation, as well as the patient’s immunization history, antibiotic allergies, liver disease, immunocompromised state, and other factors predisposing to severe infection.
Physical Examination
Assessment includes vital signs, a complete systemic examination, full exposure of the injured area, and secondary skin evaluation for occult trauma. Careful inspection determines wound depth and involvement of bone, joint, or tendon, with attention to tendon sheath pain, spreading erythema, lymphadenopathy, exudate, purulence, or fluctuance. A focused neurologic and vascular exam of the affected region is mandatory. Presentations range from isolated minor wounds to multiple severe injuries. Systemic toxicity, hemorrhage, and septic shock represent emergencies. Delayed complications include osteomyelitis, while meningitis, peritonitis, and endocarditis are rare manifestations of disseminated infection. Isolated ecchymosis or hematoma without skin break may indicate venom-related tissue reaction.
Diagnostic Tests and Interpretation
Laboratory Studies
Evaluation includes complete blood count, electrolytes, renal and liver function tests, and at least two sets of aerobic and anaerobic blood cultures obtained before antibiotics, with prolonged incubation for slow-growing oral flora. Gram stain and wound cultures may assist but are often nonspecific. Pasteurella species appear as gram-negative bacilli growing on blood or chocolate agar, and MRSA is commonly present from host skin contamination
.
Imaging
Plain radiographs assess for retained foreign bodies such as tooth fragments, while CT or MRI better define hemorrhage, abscess formation, tendon sheath involvement, and osteomyelitis.
Treatment
Medications
Tetanus and rabies prophylaxis must always be considered. Prophylactic antibiotics are recommended for most bites except superficial injuries, guided by the expected oral flora of the animal. First-line empiric therapy for human, dog, and cat bites is a beta-lactam/beta-lactamase inhibitor such as amoxicillin-clavulanate. Alternatives include combinations of trimethoprim-sulfamethoxazole, penicillin, fluoroquinolones, or doxycycline with metronidazole or clindamycin, noting that clindamycin and trimethoprim-sulfamethoxazole provide MRSA coverage. Intravenous therapy is required for systemic illness. Venomous snakebites require antivenom and ceftriaxone.
Ongoing Care and Follow-Up
Wounds require daily inspection and dressing changes, with a low threshold for urgent surgical intervention when deep penetration, foreign bodies, or tendon sheath involvement are suspected. Patients must be educated about warning signs of infection prior to discharge, and timely tetanus or rabies immunization may be lifesaving.
Basics
Description and Definition
Animal bites produce puncture wounds, scratches, or lacerations with variable tissue injury, while clenched-fist injuries and human bites result from tooth penetration and inoculation of oral flora into the skin.
Approach to the Patient
Immediate assessment focuses on identifying life- or limb-threatening injury, hemorrhage, and neurovascular compromise with a detailed neurologic and vascular examination of the affected area. Patients showing signs of shock require prompt hemodynamic stabilization, empiric antibiotics, and possible surgical consultation. It is critical to determine whether the bite involves a venomous species and to thoroughly explore wounds for deep structural injury involving tendons, vessels, nerves, joints, or organs, as well as retained foreign bodies such as teeth. Copious irrigation with sterile water or saline and meticulous debridement of devitalized tissue and debris are essential and often require local anesthesia. Wounds should be kept moist with topical antibacterial agents and covered to reduce microbial load. After adequate debridement and high-pressure irrigation, select wounds, including some on the hands and feet, may undergo primary closure, but most animal and human bite injuries should heal by secondary intention. Close follow-up is mandatory due to high infection risk. Imaging with radiography, CT, or MRI may be required to detect foreign bodies or deep injury. Bites to the hands and feet frequently warrant surgical evaluation because deep-space and tendon sheath infections can rapidly progress to sepsis and permanent damage. Tetanus and rabies prophylaxis must be addressed, and suspicious human bites should raise concern for child or domestic abuse.
Epidemiology
In the United States, approximately 40% of households own dogs and about one-third own cats. Children are the most common victims of animal bites and frequently sustain injuries to the head and neck. Around 2.5% of dog bites show clinical infection at the time of presentation.
Risk Factors
Severe outcomes are more likely in children due to exposure of the head, neck, and upper torso; in veterinarians and animal handlers; in immunocompromised individuals including those with HIV, malignancy, chemotherapy exposure, steroid use, asplenia, or liver disease; and in patients with diabetes mellitus who have impaired wound healing from vascular disease and neuropathy.
Etiology
Bite-related infections are typically polymicrobial, involving aerobic and anaerobic organisms derived from the biter’s oral flora and the victim’s skin flora, with methicillin-resistant Staphylococcus aureus commonly introduced from human skin. Dog bites are frequently associated with Capnocytophaga species and Pasteurella canis, while cat bites commonly yield Pasteurella multocida. Other zoonotic pathogens include Bartonella henselae, Francisella tularensis, and Leptospira species. Additional aerobic organisms include streptococci, staphylococci, Moraxella, and Neisseria, with anaerobes such as Fusobacterium, Bacteroides, Porphyromonas, and Prevotella contributing to mixed infections. Human bites often involve Streptococcus species, Staphylococcus aureus, Eikenella corrodens, Haemophilus influenzae, and anaerobes including Fusobacterium nucleatum, Prevotella, Porphyromonas, Peptococcus, and Peptostreptococcus. Aquatic animal bites may introduce Aeromonas, Vibrio species, Erysipelothrix, or Mycobacterium marinum. Rodents and rodent predators can transmit Streptobacillus moniliformis or Spirillum species, causing rat-bite fever.
Diagnosis
History
The history should clarify events surrounding the injury, characteristics of the biting animal including species, venom potential, vaccination status, and availability for rabies observation, as well as the patient’s immunization history, antibiotic allergies, liver disease, immunocompromised state, and other factors predisposing to severe infection.
Physical Examination
Assessment includes vital signs, a complete systemic examination, full exposure of the injured area, and secondary skin evaluation for occult trauma. Careful inspection determines wound depth and involvement of bone, joint, or tendon, with attention to tendon sheath pain, spreading erythema, lymphadenopathy, exudate, purulence, or fluctuance. A focused neurologic and vascular exam of the affected region is mandatory. Presentations range from isolated minor wounds to multiple severe injuries. Systemic toxicity, hemorrhage, and septic shock represent emergencies. Delayed complications include osteomyelitis, while meningitis, peritonitis, and endocarditis are rare manifestations of disseminated infection. Isolated ecchymosis or hematoma without skin break may indicate venom-related tissue reaction.
Diagnostic Tests and Interpretation
Laboratory Studies
Evaluation includes complete blood count, electrolytes, renal and liver function tests, and at least two sets of aerobic and anaerobic blood cultures obtained before antibiotics, with prolonged incubation for slow-growing oral flora. Gram stain and wound cultures may assist but are often nonspecific. Pasteurella species appear as gram-negative bacilli growing on blood or chocolate agar, and MRSA is commonly present from host skin contamination
.
Imaging
Plain radiographs assess for retained foreign bodies such as tooth fragments, while CT or MRI better define hemorrhage, abscess formation, tendon sheath involvement, and osteomyelitis.
Treatment
Medications
Tetanus and rabies prophylaxis must always be considered. Prophylactic antibiotics are recommended for most bites except superficial injuries, guided by the expected oral flora of the animal. First-line empiric therapy for human, dog, and cat bites is a beta-lactam/beta-lactamase inhibitor such as amoxicillin-clavulanate. Alternatives include combinations of trimethoprim-sulfamethoxazole, penicillin, fluoroquinolones, or doxycycline with metronidazole or clindamycin, noting that clindamycin and trimethoprim-sulfamethoxazole provide MRSA coverage. Intravenous therapy is required for systemic illness. Venomous snakebites require antivenom and ceftriaxone.
Ongoing Care and Follow-Up
Wounds require daily inspection and dressing changes, with a low threshold for urgent surgical intervention when deep penetration, foreign bodies, or tendon sheath involvement are suspected. Patients must be educated about warning signs of infection prior to discharge, and timely tetanus or rabies immunization may be lifesaving.
- Published on
Infectious Diseases and Microbiology: Abdominal Pain and Fever
Basics
Description and Definition
This topic reviews conditions in which fever occurs together with abdominal pain.
Approach to the Patient
The initial priority is deciding whether the presentation represents a surgical emergency. Life-threatening diagnoses must be rapidly excluded, and clinicians should remember that pain referred from extra-abdominal sites can mimic primary abdominal disease. Severe intraabdominal infections may present with minimal or atypical findings, particularly in neonates, older adults, and immunocompromised patients. Rapid assessment of symptom onset, severity, and character is essential, along with immediate vital sign evaluation and a comprehensive physical examination. Beyond a careful abdominal exam, full systemic assessment is required, especially of the cardiopulmonary systems. Rectal examination should generally be performed, except in patients with severe neutropenia, in whom careful inspection is preferred.
Epidemiology
Appendicitis commonly presents to emergency departments with fever and abdominal pain. In the United States, most typhoid fever cases are acquired during travel, particularly to Mexico, India, and Pakistan. Travel to tropical regions raises concern for malaria, while travel to areas endemic for louse-borne relapsing fever such as Ethiopia, parts of South America, and East Asia suggests Borrelia recurrentis. HIV infection can produce fever and abdominal pain through multiple mechanisms and should be considered in individuals with risk factors or from high-prevalence regions such as sub-Saharan Africa and Southeast Asia, including those with intravenous drug exposure. Intestinal tuberculosis is associated with ingestion of unpasteurized dairy products, malnutrition, and HIV. Animal exposure may indicate leptospirosis, toxoplasmosis, brucellosis, or Q fever. Other vectors are linked to dengue fever, typhus, and psittacosis. Individuals with sickle cell disease or prior splenectomy are predisposed to salmonellosis. Melena, positive fecal occult blood tests, and weight loss should prompt consideration of solid tumors or lymphoma. Cardiovascular disease, the leading cause of mortality in Western countries, may frequently present with abdominal pain.
Etiology
Diffuse abdominal pain with fever suggests peritonitis, ileus or obstruction, mesenteric ischemia, ruptured aneurysm, or metabolic disorders. Infectious causes vary by location: right upper quadrant pain may result from acute cholecystitis including perforation, hepatitis, Fitz-Hugh–Curtis syndrome, pyelonephritis, pneumonia, or liver abscess; left upper quadrant pain from pyelonephritis, pneumonia, or splenic abscess; epigastric pain from diverticulitis, early appendicitis, primary or secondary peritonitis including tuberculous forms, acute gastroenteritis, pancreatitis, cholangitis, inflammatory bowel disease, Clostridioides difficile colitis, or mediastinitis; right lower quadrant pain from appendicitis, salpingitis, psoas abscess, mesenteric adenitis, pelvic inflammatory disease, or bowel perforation; left lower quadrant pain from diverticulitis, salpingitis, psoas abscess, mesenteric adenitis, pelvic infection, or bowel perforation. Noninfectious causes include acute porphyria, adrenal crisis, systemic inflammatory and granulomatous disorders, diabetic ketoacidosis, esophageal disease, familial Mediterranean fever, lead poisoning, intraabdominal or hematologic malignancy, mediastinal tumors, mesenteric ischemia or thrombosis, myocardial infarction, pancreatitis, pneumothorax complicating pneumonia, pulmonary embolism, ruptured ovarian follicle, and sickle cell crisis. Enteric fever presents with fever and abdominal pain and may include headache, hepatosplenomegaly, and a macular rash known as rose spots. Typhoid fever caused by Salmonella typhi is the classic example, but similar syndromes can result from Salmonella paratyphi and numerous bacterial, rickettsial, viral, fungal, and parasitic pathogens. Mesenteric adenitis often mimics appendicitis and is usually viral or due to Yersinia enterocolitica. Eosinophilia with abdominal cramps or diarrhea and fever suggests helminthic infection or intestinal lymphoma. Enterohemorrhagic Escherichia coli infections typically cause crampy pain before bloody diarrhea and are often afebrile. In patients with HIV, both typical causes seen in immunocompetent hosts and additional conditions such as typhlitis, bowel perforation with abscess, HIV-related cholangiopathy, hepatic abscesses, bacillary angiomatosis, pancreatitis, splenic infarction or abscess, gastrointestinal tuberculosis, cytomegalovirus disease, fungal and mycobacterial infections, parasitic enteritis, Giardia, Strongyloides, Kaposi sarcoma, and lymphoma must be considered.
Diagnosis
History
Assessment should include pain location, intensity, quality, radiation, aggravating and relieving factors, relation to meals, bowel habits, recent travel, dietary and animal exposures, and cardiovascular risk factors.
Physical Examination
Evaluation includes bowel sounds and abdominal bruits, localization and severity of tenderness, and palpation for hepatosplenomegaly. Signs of acute or chronic liver disease such as jaundice, scleral icterus, spider angiomata, clubbing, and ascites should be sought. The oropharynx and anus should be examined for lesions. Relative bradycardia supports enteric fever, which may also present with conjunctivitis, pharyngitis, or pulmonary findings. Acute diarrhea with sterile arthritis suggests Yersinia infection. Right lower quadrant rebound tenderness may reflect mesenteric adenitis, and only about half of appendicitis cases show classic migratory pain.
Diagnostic Tests and Interpretation
Laboratory Studies
Recommended tests include complete blood count with differential, electrolytes, renal function, liver enzymes and function tests, and calcium. Blood cultures should be obtained before empiric antibiotics, along with urine culture and electrocardiography. Blood, stool, and urine cultures are required in suspected enteric fever prior to therapy, with bone marrow cultures considered if blood cultures are negative and typhoid fever is suspected. Widal testing has limited diagnostic value outside Salmonella typhi. Leukopenia is common in typhoid fever. Eosinophilia warrants stool examination for ova and parasites. Fever is uncommon in giardiasis, occurring in a minority of cases, and diagnosis may require stool studies, small-bowel biopsy, or immunoassays. Malaria evaluation requires thick and thin blood smears every 24 hours for three sets, with rapid tests as adjuncts. Stool testing should be guided by context and include evaluation for C. difficile, ova and parasites, and bacterial cultures for major enteric pathogens. Most appendicitis cases demonstrate leukocytosis.
Imaging
Plain abdominal radiographs may reveal free air, loss of psoas shadow, or radiopaque calculi, but ultrasonography or computed tomography is often required. Ultrasound is the preferred initial test for suspected biliary or renal infection but is limited for deep structures and postoperative evaluation. CT imaging offers higher diagnostic accuracy, especially with contrast, though renal toxicity must be considered. Ultrasound is standard for initial assessment of biliary disease, while endoscopic ultrasonography provides very high accuracy for bile duct stones. Magnetic resonance cholangiography offers a noninvasive alternative for biliary imaging. Acute acalculous cholecystitis accounts for a minority of cases, and nuclear scanning is rarely first line but may be useful in selected situations. Endoscopic retrograde, percutaneous transhepatic, and intraoperative cholangiography are highly accurate for common bile duct stones but are invasive and carry complication risks.
Treatment
Medications
Empiric antimicrobial therapy is often required before a definitive diagnosis is established and should be tailored to the suspected infectious syndrome and travel history. Mesenteric adenitis is typically self-limited and may not require antibiotics, though trimethoprim-sulfamethoxazole, third-generation cephalosporins, or fluoroquinolones can be used when indicated. Mild to moderate community-acquired intraabdominal infections such as acute cholecystitis can be treated with a fluoroquinolone plus metronidazole or a beta-lactam/beta-lactamase inhibitor. Vancomycin is added when methicillin-resistant Staphylococcus aureus is suspected, while ampicillin is preferred for susceptible Enterococcus species. Severe community-acquired or health-care–associated intraabdominal infections require early broad-spectrum multidrug regimens targeting nosocomial organisms, often including antipseudomonal cephalosporins or carbapenems.
Ongoing Care and Follow-Up
Clinicians should remain alert for subtle or atypical presentations in neonates, infants, and older adults. Patients require close observation until fever resolves. Persistent unexplained fever and abdominal pain should prompt consideration of abdominal CT imaging when history, examination, and ultrasound are nondiagnostic.
Basics
Description and Definition
This topic reviews conditions in which fever occurs together with abdominal pain.
Approach to the Patient
The initial priority is deciding whether the presentation represents a surgical emergency. Life-threatening diagnoses must be rapidly excluded, and clinicians should remember that pain referred from extra-abdominal sites can mimic primary abdominal disease. Severe intraabdominal infections may present with minimal or atypical findings, particularly in neonates, older adults, and immunocompromised patients. Rapid assessment of symptom onset, severity, and character is essential, along with immediate vital sign evaluation and a comprehensive physical examination. Beyond a careful abdominal exam, full systemic assessment is required, especially of the cardiopulmonary systems. Rectal examination should generally be performed, except in patients with severe neutropenia, in whom careful inspection is preferred.
Epidemiology
Appendicitis commonly presents to emergency departments with fever and abdominal pain. In the United States, most typhoid fever cases are acquired during travel, particularly to Mexico, India, and Pakistan. Travel to tropical regions raises concern for malaria, while travel to areas endemic for louse-borne relapsing fever such as Ethiopia, parts of South America, and East Asia suggests Borrelia recurrentis. HIV infection can produce fever and abdominal pain through multiple mechanisms and should be considered in individuals with risk factors or from high-prevalence regions such as sub-Saharan Africa and Southeast Asia, including those with intravenous drug exposure. Intestinal tuberculosis is associated with ingestion of unpasteurized dairy products, malnutrition, and HIV. Animal exposure may indicate leptospirosis, toxoplasmosis, brucellosis, or Q fever. Other vectors are linked to dengue fever, typhus, and psittacosis. Individuals with sickle cell disease or prior splenectomy are predisposed to salmonellosis. Melena, positive fecal occult blood tests, and weight loss should prompt consideration of solid tumors or lymphoma. Cardiovascular disease, the leading cause of mortality in Western countries, may frequently present with abdominal pain.
Etiology
Diffuse abdominal pain with fever suggests peritonitis, ileus or obstruction, mesenteric ischemia, ruptured aneurysm, or metabolic disorders. Infectious causes vary by location: right upper quadrant pain may result from acute cholecystitis including perforation, hepatitis, Fitz-Hugh–Curtis syndrome, pyelonephritis, pneumonia, or liver abscess; left upper quadrant pain from pyelonephritis, pneumonia, or splenic abscess; epigastric pain from diverticulitis, early appendicitis, primary or secondary peritonitis including tuberculous forms, acute gastroenteritis, pancreatitis, cholangitis, inflammatory bowel disease, Clostridioides difficile colitis, or mediastinitis; right lower quadrant pain from appendicitis, salpingitis, psoas abscess, mesenteric adenitis, pelvic inflammatory disease, or bowel perforation; left lower quadrant pain from diverticulitis, salpingitis, psoas abscess, mesenteric adenitis, pelvic infection, or bowel perforation. Noninfectious causes include acute porphyria, adrenal crisis, systemic inflammatory and granulomatous disorders, diabetic ketoacidosis, esophageal disease, familial Mediterranean fever, lead poisoning, intraabdominal or hematologic malignancy, mediastinal tumors, mesenteric ischemia or thrombosis, myocardial infarction, pancreatitis, pneumothorax complicating pneumonia, pulmonary embolism, ruptured ovarian follicle, and sickle cell crisis. Enteric fever presents with fever and abdominal pain and may include headache, hepatosplenomegaly, and a macular rash known as rose spots. Typhoid fever caused by Salmonella typhi is the classic example, but similar syndromes can result from Salmonella paratyphi and numerous bacterial, rickettsial, viral, fungal, and parasitic pathogens. Mesenteric adenitis often mimics appendicitis and is usually viral or due to Yersinia enterocolitica. Eosinophilia with abdominal cramps or diarrhea and fever suggests helminthic infection or intestinal lymphoma. Enterohemorrhagic Escherichia coli infections typically cause crampy pain before bloody diarrhea and are often afebrile. In patients with HIV, both typical causes seen in immunocompetent hosts and additional conditions such as typhlitis, bowel perforation with abscess, HIV-related cholangiopathy, hepatic abscesses, bacillary angiomatosis, pancreatitis, splenic infarction or abscess, gastrointestinal tuberculosis, cytomegalovirus disease, fungal and mycobacterial infections, parasitic enteritis, Giardia, Strongyloides, Kaposi sarcoma, and lymphoma must be considered.
Diagnosis
History
Assessment should include pain location, intensity, quality, radiation, aggravating and relieving factors, relation to meals, bowel habits, recent travel, dietary and animal exposures, and cardiovascular risk factors.
Physical Examination
Evaluation includes bowel sounds and abdominal bruits, localization and severity of tenderness, and palpation for hepatosplenomegaly. Signs of acute or chronic liver disease such as jaundice, scleral icterus, spider angiomata, clubbing, and ascites should be sought. The oropharynx and anus should be examined for lesions. Relative bradycardia supports enteric fever, which may also present with conjunctivitis, pharyngitis, or pulmonary findings. Acute diarrhea with sterile arthritis suggests Yersinia infection. Right lower quadrant rebound tenderness may reflect mesenteric adenitis, and only about half of appendicitis cases show classic migratory pain.
Diagnostic Tests and Interpretation
Laboratory Studies
Recommended tests include complete blood count with differential, electrolytes, renal function, liver enzymes and function tests, and calcium. Blood cultures should be obtained before empiric antibiotics, along with urine culture and electrocardiography. Blood, stool, and urine cultures are required in suspected enteric fever prior to therapy, with bone marrow cultures considered if blood cultures are negative and typhoid fever is suspected. Widal testing has limited diagnostic value outside Salmonella typhi. Leukopenia is common in typhoid fever. Eosinophilia warrants stool examination for ova and parasites. Fever is uncommon in giardiasis, occurring in a minority of cases, and diagnosis may require stool studies, small-bowel biopsy, or immunoassays. Malaria evaluation requires thick and thin blood smears every 24 hours for three sets, with rapid tests as adjuncts. Stool testing should be guided by context and include evaluation for C. difficile, ova and parasites, and bacterial cultures for major enteric pathogens. Most appendicitis cases demonstrate leukocytosis.
Imaging
Plain abdominal radiographs may reveal free air, loss of psoas shadow, or radiopaque calculi, but ultrasonography or computed tomography is often required. Ultrasound is the preferred initial test for suspected biliary or renal infection but is limited for deep structures and postoperative evaluation. CT imaging offers higher diagnostic accuracy, especially with contrast, though renal toxicity must be considered. Ultrasound is standard for initial assessment of biliary disease, while endoscopic ultrasonography provides very high accuracy for bile duct stones. Magnetic resonance cholangiography offers a noninvasive alternative for biliary imaging. Acute acalculous cholecystitis accounts for a minority of cases, and nuclear scanning is rarely first line but may be useful in selected situations. Endoscopic retrograde, percutaneous transhepatic, and intraoperative cholangiography are highly accurate for common bile duct stones but are invasive and carry complication risks.
Treatment
Medications
Empiric antimicrobial therapy is often required before a definitive diagnosis is established and should be tailored to the suspected infectious syndrome and travel history. Mesenteric adenitis is typically self-limited and may not require antibiotics, though trimethoprim-sulfamethoxazole, third-generation cephalosporins, or fluoroquinolones can be used when indicated. Mild to moderate community-acquired intraabdominal infections such as acute cholecystitis can be treated with a fluoroquinolone plus metronidazole or a beta-lactam/beta-lactamase inhibitor. Vancomycin is added when methicillin-resistant Staphylococcus aureus is suspected, while ampicillin is preferred for susceptible Enterococcus species. Severe community-acquired or health-care–associated intraabdominal infections require early broad-spectrum multidrug regimens targeting nosocomial organisms, often including antipseudomonal cephalosporins or carbapenems.
Ongoing Care and Follow-Up
Clinicians should remain alert for subtle or atypical presentations in neonates, infants, and older adults. Patients require close observation until fever resolves. Persistent unexplained fever and abdominal pain should prompt consideration of abdominal CT imaging when history, examination, and ultrasound are nondiagnostic.
- Published on
Infectious Diseases – Trichomonas Vaginitis
1. What is it?
Trichomonas vaginitis is a sexually transmitted infection caused by Trichomonas vaginalis.
It commonly presents with vaginal discharge, itching, dysuria, and irritation, though some patients may be asymptomatic.
2. How is it treated?
3. What are the characteristic physical exam findings?
4. What is the key diagnostic clue on wet mount?
1. What is it?
Trichomonas vaginitis is a sexually transmitted infection caused by Trichomonas vaginalis.
It commonly presents with vaginal discharge, itching, dysuria, and irritation, though some patients may be asymptomatic.
2. How is it treated?
- Oral metronidazole is the treatment of choice
- Sexual partners must be treated concurrently to prevent reinfection
- Single-dose therapy is preferred due to better patient adherence
3. What are the characteristic physical exam findings?
- Pelvic examination may reveal a “strawberry cervix”
- This appearance is caused by multiple punctate cervical hemorrhages
4. What is the key diagnostic clue on wet mount?
- Trichomonas vaginalis is the only organism that is motile on wet mount
- Its flagella allow it to swim across the slide, making it easily identifiable
- Published on
Symptoms and Signs -Differential Diagnosis of Muscle Flaccidity [Muscle Hypotonicity]
Flaccid muscles exhibit significant weakness and softness, characterized by diminished resistance to movement, enhanced mobility, and an excessive range of motion (ROM). Flaccidity, resulting from disturbed muscular innervation, may be confined to a specific limb or muscle group or may be generalized throughout the whole. The onset may be abrupt, as seen in trauma, or persistent, as observed in neurological disease.
URGENT INTERVENTIONS
Ensure stabilization of the cervical spine if the patient's muscle flaccidity is attributable to trauma. Rapidly assess his breathing condition. If you
Observe signs and symptoms of respiratory insufficiency, including dyspnea, shallow respirations, nasal flaring, cyanosis, and reduced oxygen saturation; give oxygen via nasal cannula or mask. Intubation and mechanical ventilation may be required.
Medical History and Physical Assessment
In the absence of patient discomfort, inquire about the start, duration of muscular flaccidity, and any triggering circumstances. Inquire about concomitant symptoms, including weakness, alterations in muscle function, and sensory deficits or paresthesia.
Assess the impacted muscles for atrophy, signifying a persistent issue. Assess muscle strength and evaluate deep tendon reflexes (DTRs) in all extremities.
Etiological Factors in Medicine
Amyotrophic lateral sclerosis (ALS)
Progressive muscular weakening and paralysis are associated with widespread flaccidity. Generally, these effects initiate in one hand, propagate to the arm, and subsequently manifest in the opposite hand and arm. Ultimately, they disseminate throughout the trunk, neck, tongue, larynx, pharynx, and limbs; advancing respiratory muscle weakness results in respiratory insufficiency. Additional observations encompass muscle cramps, coarse fasciculations, hyperactive deep tendon reflexes, mild leg muscle spasticity, dysphagia, dysarthria, excessive salivation, and sadness.
Cerebral lesions
Lesions in the frontal and parietal lobes can result in contralateral flaccidity, weakness, or paralysis, which may progress to spasticity and potentially lead to contractures. Additional features encompass hyperactive deep tendon reflexes, a positive Babinski sign, loss of proprioception, stereognosis, graphesthesia, anesthesia, and thermoanesthesia.
Guillain-Barré syndrome
Guillain-Barré syndrome induces muscular hypotonia. The progression is generally symmetrical and ascends from the feet to the arms and facial nerves within 24 to 72 hours of commencement. Related findings encompass sensory loss or paresthesia, absent deep tendon reflexes, tachycardia (or, less frequently, bradycardia), variable hypertension and orthostatic hypotension, diaphoresis, incontinence, dysphagia, dysarthria, hypernasality, and facial diplegia. Weakness may advance to complete motor paralysis and respiratory collapse.
Huntington's disease
In addition to flaccidity, significant mental status alterations, culminating in dementia, and choreiform motions are primary concerns.
Indications of a condition
Additional symptoms encompass poor balance, reluctant or explosive speaking, dysphagia, decreased respiration, and incontinence.
Myopathy. Muscle weakness and flaccidity characterize myopathies and muscular dystrophies.
Trauma to peripheral nerves
Flaccidity, paralysis, and the absence of feeling and reflexes in the affected region may manifest.
Peripheral neuropathy
Flaccidity typically manifests in the legs due to prolonged increasing muscular weakening and paralysis. It may also induce mild to intense searing pain, lustrous red skin, anhidrosis, and a diminished sense of vibration. Paresthesia, hyperesthesia, or anesthesia may impact the hands and feet. Deep tendon reflexes may be diminished or missing.
Epileptic condition
Transient episodes of syncope and generalized flaccidity frequently occur subsequent to a generalized tonic-clonic seizure.
Spinal cord damage. Spinal shock may lead to immediate muscular flaccidity or spasticity underneath the lesion site. Signs and symptoms associated with the damage may manifest below the injury site and can include paralysis, absent deep tendon reflexes, analgesia, thermoanesthesia, loss of proprioception, and diminished sensations of vibration, touch, and pressure, as well as unilateral anhidrosis. Hypotension, gastrointestinal and urinary dysfunction, as well as impotence or priapism, may also manifest. Injury in the C1 to C5 area may result in respiratory paralysis and bradycardia.
Particular Considerations
Administer consistent, methodical, passive range of motion exercises to maintain joint mobility and enhance circulation. Reposition a patient exhibiting widespread flaccidity bi-hourly to avert skin breakdown. Cushion bony prominences and other pressure points, and mitigate thermal harm by personally checking the bath water prior to the patient's bathing. Address isolated flaccidity by immobilizing the affected limb using a sling or splint. Enhance patient safety and mitigate fall risk by implementing assistive devices and instructing on their appropriate utilization. Seek the expertise of a physician and an occupational therapist to develop a tailored therapeutic plan that promotes autonomy.
Prepare the patient for diagnostic evaluations, including cranial and spinal X-rays, computed tomography scans, and electromyography.
Patient Consultation
Instruct the patient on the utilization of assistive equipment and examine the planned workout routine with him.
Pediatric Guidelines
Pediatric etiologies of muscle flaccidity encompass myelomeningocele, Lowe syndrome, Werdnig-Hoffmann disease, and muscular dystrophy. A young child exhibiting overall flaccidity may assume a froglike posture, characterized by abducted hips and knees.
Flaccid muscles exhibit significant weakness and softness, characterized by diminished resistance to movement, enhanced mobility, and an excessive range of motion (ROM). Flaccidity, resulting from disturbed muscular innervation, may be confined to a specific limb or muscle group or may be generalized throughout the whole. The onset may be abrupt, as seen in trauma, or persistent, as observed in neurological disease.
URGENT INTERVENTIONS
Ensure stabilization of the cervical spine if the patient's muscle flaccidity is attributable to trauma. Rapidly assess his breathing condition. If you
Observe signs and symptoms of respiratory insufficiency, including dyspnea, shallow respirations, nasal flaring, cyanosis, and reduced oxygen saturation; give oxygen via nasal cannula or mask. Intubation and mechanical ventilation may be required.
Medical History and Physical Assessment
In the absence of patient discomfort, inquire about the start, duration of muscular flaccidity, and any triggering circumstances. Inquire about concomitant symptoms, including weakness, alterations in muscle function, and sensory deficits or paresthesia.
Assess the impacted muscles for atrophy, signifying a persistent issue. Assess muscle strength and evaluate deep tendon reflexes (DTRs) in all extremities.
Etiological Factors in Medicine
Amyotrophic lateral sclerosis (ALS)
Progressive muscular weakening and paralysis are associated with widespread flaccidity. Generally, these effects initiate in one hand, propagate to the arm, and subsequently manifest in the opposite hand and arm. Ultimately, they disseminate throughout the trunk, neck, tongue, larynx, pharynx, and limbs; advancing respiratory muscle weakness results in respiratory insufficiency. Additional observations encompass muscle cramps, coarse fasciculations, hyperactive deep tendon reflexes, mild leg muscle spasticity, dysphagia, dysarthria, excessive salivation, and sadness.
Cerebral lesions
Lesions in the frontal and parietal lobes can result in contralateral flaccidity, weakness, or paralysis, which may progress to spasticity and potentially lead to contractures. Additional features encompass hyperactive deep tendon reflexes, a positive Babinski sign, loss of proprioception, stereognosis, graphesthesia, anesthesia, and thermoanesthesia.
Guillain-Barré syndrome
Guillain-Barré syndrome induces muscular hypotonia. The progression is generally symmetrical and ascends from the feet to the arms and facial nerves within 24 to 72 hours of commencement. Related findings encompass sensory loss or paresthesia, absent deep tendon reflexes, tachycardia (or, less frequently, bradycardia), variable hypertension and orthostatic hypotension, diaphoresis, incontinence, dysphagia, dysarthria, hypernasality, and facial diplegia. Weakness may advance to complete motor paralysis and respiratory collapse.
Huntington's disease
In addition to flaccidity, significant mental status alterations, culminating in dementia, and choreiform motions are primary concerns.
Indications of a condition
Additional symptoms encompass poor balance, reluctant or explosive speaking, dysphagia, decreased respiration, and incontinence.
Myopathy. Muscle weakness and flaccidity characterize myopathies and muscular dystrophies.
Trauma to peripheral nerves
Flaccidity, paralysis, and the absence of feeling and reflexes in the affected region may manifest.
Peripheral neuropathy
Flaccidity typically manifests in the legs due to prolonged increasing muscular weakening and paralysis. It may also induce mild to intense searing pain, lustrous red skin, anhidrosis, and a diminished sense of vibration. Paresthesia, hyperesthesia, or anesthesia may impact the hands and feet. Deep tendon reflexes may be diminished or missing.
Epileptic condition
Transient episodes of syncope and generalized flaccidity frequently occur subsequent to a generalized tonic-clonic seizure.
Spinal cord damage. Spinal shock may lead to immediate muscular flaccidity or spasticity underneath the lesion site. Signs and symptoms associated with the damage may manifest below the injury site and can include paralysis, absent deep tendon reflexes, analgesia, thermoanesthesia, loss of proprioception, and diminished sensations of vibration, touch, and pressure, as well as unilateral anhidrosis. Hypotension, gastrointestinal and urinary dysfunction, as well as impotence or priapism, may also manifest. Injury in the C1 to C5 area may result in respiratory paralysis and bradycardia.
Particular Considerations
Administer consistent, methodical, passive range of motion exercises to maintain joint mobility and enhance circulation. Reposition a patient exhibiting widespread flaccidity bi-hourly to avert skin breakdown. Cushion bony prominences and other pressure points, and mitigate thermal harm by personally checking the bath water prior to the patient's bathing. Address isolated flaccidity by immobilizing the affected limb using a sling or splint. Enhance patient safety and mitigate fall risk by implementing assistive devices and instructing on their appropriate utilization. Seek the expertise of a physician and an occupational therapist to develop a tailored therapeutic plan that promotes autonomy.
Prepare the patient for diagnostic evaluations, including cranial and spinal X-rays, computed tomography scans, and electromyography.
Patient Consultation
Instruct the patient on the utilization of assistive equipment and examine the planned workout routine with him.
Pediatric Guidelines
Pediatric etiologies of muscle flaccidity encompass myelomeningocele, Lowe syndrome, Werdnig-Hoffmann disease, and muscular dystrophy. A young child exhibiting overall flaccidity may assume a froglike posture, characterized by abducted hips and knees.

- Published on
Filariasis
Filariasis is a parasitic tropical disease caused by thread-like nematode worms belonging to the subfamily Filarioidea, spread by vectors.
• Nine species of filarial worms utilize humans as definitive hosts, residing in lymphatics, skin, connective tissue, serous cavities, and blood vessels. • Adult worms can inhabit the host for more than 20 years.
EPIDEMIOLOGY • Bancroftian and Malayan filariasis – Endemic in 83 countries across tropical and subtropical regions of Asia, Africa, Central and South America, and Pacific Island states. Approximately 1.3 billion individuals globally are at risk of illness (1).
- 120 million individuals have already been infected (1).
Approximately 40 million individuals are afflicted with debilitating or disfiguring diseases (1).
• Loiasis
- Restricted to the rainforest region of western and central Africa. Humans constitute the sole identified reservoir. • Onchocerciasis (“river blindness”) - Approximately 18 million individuals are affected (1).
– Approximately 270,000 individuals are blind, and a further 500,000 are visually impaired. Second primary cause of global blindness behind trachoma (1).
- Illness observed in South America and Africa.
Dracunculiasis (Guinea worm) primarily manifests in a limited region encompassing some African nations and Yemen (1). • Dirofilariasis (Canine heartworm) – Symptomatic infection infrequent (1) – Global distribution Mansonelliasis is a disease prevalent in Africa, Central and South America, and the Caribbean.
FACTORS OF RISK
• Residing in or visiting endemic regions • Diminished socio-economic standing
Genetics
No genetic variables are implicated
GENERAL PREVENTION • Health education • Vector control strategies
• Sleep beneath a mosquito net • Apply insect repellent containing a minimum of 30% DEET (N,N-Diethyl-meta-toluamide) on exposed skin and clothing • Wear long-sleeved garments to avert insect bites • Administer diethylcarbamazine 300 mg/week orally as prophylaxis against Loiasis • Dracunculiasis – Consume clean, boiled water – Filter copepods from drinking water – Restrict individuals with Guinea worm ulcers from accessing drinking water sources
- Administer chemical treatments, such as Abate, to eliminate copepods in contaminated water sources. - Introduce fish species that consume copepods into affected water bodies.
PATHOPHYSIOLOGY • Bancroftian and Malayan Filariasis Adult worms induce hypertrophy and dilation of lymphatic channels, resulting in valve dysfunction and subsequent extensive permanent lymphedema.
“Elephantiasis.” • Loiasis – Larvae infiltrate through the bite of a red fly, subsequently molting and migrating beneath the skin, resulting in temporary migratory angioedema (“Calabar” swellings), discomfort, pruritus, and urticaria, which are localized hypersensitivity reactions.
• Onchocerciasis — Larvae are introduced through a blackfly bite, mature, and reproduce, yielding microfilariae around one year post-bite. Adult worms reside in nodules inside the dermis and deep fascia. Microfilariae traverse the dermis and may infiltrate the ocular region, resulting in inflammation that can lead to blindness, known as "river blindness," as well as skin nodules and onchodermatitis.
• Dracunculiasis – Larvae are consumed by contaminated drinking water containing infected copepods. Larvae are discharged. They infiltrate the intestine, develop within the abdominal cavity, and reproduce. Male specimens perish, while gravid females move to the lower extremities, where they generate a papule that ultimately ulcerates. The worm surfaces to discharge larvae upon contact with water. Worms that do not penetrate the skin perish and undergo calcification.
Dirofilariasis involves worms that elicit a mild granulomatous response in subcutaneous tissue or obstruct a pulmonary artery, resulting in a solitary, minor pulmonary infarct.
Mansonelliasis involves the release of antigenic material from dying worms, which triggers an inflammatory response that leads to the formation of localized abscesses and granulomas.
ETIOLOGY
• Lymphatic filariasis – Infection caused by Wuchereria bancrofti, Brugia malayi, and Brugia timori – Transmitted by mosquitoes of the Anopheles, Aedes, Culex, and Mansonia genera
• Loa loa is transmitted by red tabanid flies (Chrysops species). • Onchocerca volvulus is transmitted by blackflies (Simulium species).
Dracunculus medinensis is consumed through drinking water contaminated with infected microcrustaceans (copepods).
Dirofilaria species spread by Culex mosquitoes.
Mansonella streptocerca is transmitted by midges of the Culicoides genus.
Mansonella perstans and Mansonella ozzardi induce serous cavity filariasis.
FREQUENTLY CO-OCCURRING CONDITIONS
No frequently correlated situations
DIAGNOSTIC HISTORY • Bancroftian and Malayan filariasis – Acute manifestations including fever, lymphadenitis, lymphangitis, funiculitis, and epididymitis – Chronic manifestations including abscesses, hyperkeratosis, polyarthritis, hydroceles, lymphoedema, and elephantiasis – Bronchospasm
• Loiasis – Temporary edema, typically of the wrists and ankles, accompanied by pruritus, paresthesia, and urticaria – Worm migration within the ocular region • Onchocerciasis – Subcutaneous nodules, pruritus, rashes, lymphadenopathy, lymphatic obstruction, chronic dermatological conditions, ocular lesions • Dracunculiasis – Painful, inflamed cutaneous lesion harboring a worm and arthritis • Dirofilariasis – Thoracic pain, cough, and hemoptysis • Mansonelliasis
Localized edema, pruritus, pyrexia, cephalalgia, arthralgia, neurological symptoms, and hydroceles
Inquire on travel to endemic regions.
PHYSICAL EXAMINATION
• Bancroftian and Malayan filariasis – Lymphangitis and lymphadenitis – Femoral/inguinal lymphadenopathy – Enlarged epididymis and spermatic cord – Hydrocele, lower extremity lymphoedema – May induce monoarticular arthritis
• Loiasis – Mature worms may migrate beneath the conjunctiva or into the dermis.
Calabar swelling frequently occurs in the wrists and ankles; the edema may persist for only hours but might repeat over several years. • Onchocerciasis – Dermatological alterations range from papular eruptions to regions of hyper- or hypopigmentation.
– Patients may exhibit eczematoid dermatitis and dermal thickening.
– Nontender subcutaneous nodules. – Potential reduction in optical acuity. • Dracunculiasis – A white, filamentous adult worm manifests at the cutaneous surface.
Ulceration in distal extremities. • Dirofilariasis – Typically asymptomatic Mansonelliasis is characterized by angioedema, pruritus, papular rash, alterations in skin pigmentation, fever, headaches, arthralgia, lymphadenopathy, hepatomegaly, and neurological symptoms.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• Bancroftian and Malayan filariasis - Blood smears reveal the presence of filarial worms.
– Serological assays lack specificity in filariasis. – Eosinophilia is frequently absent.
– PCR-based assays for the DNA of W. bancrofti and B. malayi are accessible in research environments.
• Loiasis – Blood smears, skin snips, or skin biopsy
• Onchocerciasis – Microscopic examination of skin biopsies reveals the presence of worms – Dracunculiasis – Diagnosis is clinical.
• Dirofilariasis - Histological Examination
• Mansonelliasis – Blood smears reveal filarial worms.
Microscopic examination of the skin biopsy reveals the presence of worms. Eosinophilia is significant.
Imaging
• Bancroftian and Malayan filariasis — Adult worms may be observed in dilated lymphatics using ultrasound. • Onchocerciasis – Cutaneous and subcutaneous nodules identified with ultrasound and magnetic resonance imaging.
• Dracunculiasis – Standard radiography reveal calcified worms.
• Dirofilariasis – Larvae can become encapsulated within necrotic lung tissue, resulting in distinct pulmonary nodules that may be detectable on computed tomography images.
DIFFERENTIAL DIAGNOSIS
Bancroftian and Malayan filariasis include bacterial lymphangitis, thrombophlebitis, idiopathic hydrocele, congestive heart failure, cirrhosis, and nephrotic syndrome. • Loiasis
– Cutaneous larva migrans, dracunculiasis, gnathostomiasis, myiasis, onchocerciasis • Onchocerciasis – M. streptocerca, scabies, leprosy, eczema, glaucoma, loiasis • Dracunculiasis – Cutaneous larva migrans, loiasis, rat bite infection, gnathostomiasis, myiasis • Dirofilariasis – Asthma, allergies, lung cancer • Mansonelliasis – Loiasis, onchocerciasis
INITIAL THERAPEUTIC AGENT
• Bancroftian and Malayan filariasis — Wolbachia spp., a genus of Rickettsia, are essential for filarial growth. Administer Doxycycline 100 mg orally twice daily for a duration of 4 to 6 weeks to address Wolbachia. Four months subsequent to initiating treatment, a single dosage of albendazole 400 mg orally and ivermectin 150 mg/kg orally was administered.
• Loiasis - Administer a single dosage of diethylcarbamazine citrate (DEC) at 6 mg/kg orally.
• Onchocerciasis - Administer one dosage of ivermectin at 150 mcg/kg orally (ineffective against mature worms). Recur in six months.
– Administer prednisone at a dosage of 1 mg/kg/day orally one week prior to ivermectin if ocular involvement is present.
• Dracunculiasis – Gradual and meticulous removal of the protruding worm.
Metronidazole 250 mg administered orally three times daily may
Mitigate inflammatory response, hence aiding in the expulsion of worms. Mebendazole 400–800 mg each day for 6 days may eradicate the worm.
• M. perstans – Administer albendazole 400 mg orally twice daily for 10 days. • M. streptocerca and M. ozzardi – Administer a single dose of ivermectin at 200 mcg/kg. • Dirofilariasis – No effective pharmacological treatment available. Second Line
• Bancroftian and Malayan filariasis – DEC, as previously mentioned for M. streptocerca. DEC should not be administered in regions with endemic lymphatic filariasis and loiasis/onchocerciasis.
SUPPLEMENTARY THERAPY
Comprehensive Measures
The treatment primarily targets the microfilarial stage of the infection. Adult worms are seldom impacted by a single dose of medicine. Repetitive therapy is frequently required for a cure.
Concerns for Referral
• Specialists in infectious diseases • Ophthalmologist for ocular assessment in onchocerciasis
CHIRURGICAL INTERVENTIONS/ADDITIONAL PROCEDURES
• Nodulectomy of palpable nodules in onchocerciasis • Surgical excision of dirofilariasis from the lung IN-PATIENT CONSIDERATIONS
Preliminary Stabilization
Resuscitation in accordance with advanced life support protocols as necessary
Criteria for Admission
• Patients with septicemia resulting from open wounds • Overnight admission for nocturnal blood sample collection for diagnostic testing
IV Fluids • Administer fluid resuscitation using colloids, such as Gelofusine, in cases of septicemia.
• Maintenance fluids utilizing Ringer's lactate
Nursing
Patients with elephantiasis may require comprehensive nursing care for the affected body portion.
Release Criteria for the resolution of septicemia
CONTINUING CARE POST-TREATMENT RECOMMENDATIONS
Every 4 to 6 weeks for treatment evaluation and symptomatic management
Patient Surveillance
Routine ocular assessments
OUTLOOK
Disability and disfigurement are mitigated by accurate diagnosis and therapy.
COMPLICATIONS
Bancroftian filariasis - Elephantiasis; Septicemia resulting from bacterial infection of exposed sores.
• Onchocerciasis - Visual Impairment
Filariasis is a parasitic tropical disease caused by thread-like nematode worms belonging to the subfamily Filarioidea, spread by vectors.
• Nine species of filarial worms utilize humans as definitive hosts, residing in lymphatics, skin, connective tissue, serous cavities, and blood vessels. • Adult worms can inhabit the host for more than 20 years.
EPIDEMIOLOGY • Bancroftian and Malayan filariasis – Endemic in 83 countries across tropical and subtropical regions of Asia, Africa, Central and South America, and Pacific Island states. Approximately 1.3 billion individuals globally are at risk of illness (1).
- 120 million individuals have already been infected (1).
Approximately 40 million individuals are afflicted with debilitating or disfiguring diseases (1).
• Loiasis
- Restricted to the rainforest region of western and central Africa. Humans constitute the sole identified reservoir. • Onchocerciasis (“river blindness”) - Approximately 18 million individuals are affected (1).
– Approximately 270,000 individuals are blind, and a further 500,000 are visually impaired. Second primary cause of global blindness behind trachoma (1).
- Illness observed in South America and Africa.
Dracunculiasis (Guinea worm) primarily manifests in a limited region encompassing some African nations and Yemen (1). • Dirofilariasis (Canine heartworm) – Symptomatic infection infrequent (1) – Global distribution Mansonelliasis is a disease prevalent in Africa, Central and South America, and the Caribbean.
FACTORS OF RISK
• Residing in or visiting endemic regions • Diminished socio-economic standing
Genetics
No genetic variables are implicated
GENERAL PREVENTION • Health education • Vector control strategies
• Sleep beneath a mosquito net • Apply insect repellent containing a minimum of 30% DEET (N,N-Diethyl-meta-toluamide) on exposed skin and clothing • Wear long-sleeved garments to avert insect bites • Administer diethylcarbamazine 300 mg/week orally as prophylaxis against Loiasis • Dracunculiasis – Consume clean, boiled water – Filter copepods from drinking water – Restrict individuals with Guinea worm ulcers from accessing drinking water sources
- Administer chemical treatments, such as Abate, to eliminate copepods in contaminated water sources. - Introduce fish species that consume copepods into affected water bodies.
PATHOPHYSIOLOGY • Bancroftian and Malayan Filariasis Adult worms induce hypertrophy and dilation of lymphatic channels, resulting in valve dysfunction and subsequent extensive permanent lymphedema.
“Elephantiasis.” • Loiasis – Larvae infiltrate through the bite of a red fly, subsequently molting and migrating beneath the skin, resulting in temporary migratory angioedema (“Calabar” swellings), discomfort, pruritus, and urticaria, which are localized hypersensitivity reactions.
• Onchocerciasis — Larvae are introduced through a blackfly bite, mature, and reproduce, yielding microfilariae around one year post-bite. Adult worms reside in nodules inside the dermis and deep fascia. Microfilariae traverse the dermis and may infiltrate the ocular region, resulting in inflammation that can lead to blindness, known as "river blindness," as well as skin nodules and onchodermatitis.
• Dracunculiasis – Larvae are consumed by contaminated drinking water containing infected copepods. Larvae are discharged. They infiltrate the intestine, develop within the abdominal cavity, and reproduce. Male specimens perish, while gravid females move to the lower extremities, where they generate a papule that ultimately ulcerates. The worm surfaces to discharge larvae upon contact with water. Worms that do not penetrate the skin perish and undergo calcification.
Dirofilariasis involves worms that elicit a mild granulomatous response in subcutaneous tissue or obstruct a pulmonary artery, resulting in a solitary, minor pulmonary infarct.
Mansonelliasis involves the release of antigenic material from dying worms, which triggers an inflammatory response that leads to the formation of localized abscesses and granulomas.
ETIOLOGY
• Lymphatic filariasis – Infection caused by Wuchereria bancrofti, Brugia malayi, and Brugia timori – Transmitted by mosquitoes of the Anopheles, Aedes, Culex, and Mansonia genera
• Loa loa is transmitted by red tabanid flies (Chrysops species). • Onchocerca volvulus is transmitted by blackflies (Simulium species).
Dracunculus medinensis is consumed through drinking water contaminated with infected microcrustaceans (copepods).
Dirofilaria species spread by Culex mosquitoes.
Mansonella streptocerca is transmitted by midges of the Culicoides genus.
Mansonella perstans and Mansonella ozzardi induce serous cavity filariasis.
FREQUENTLY CO-OCCURRING CONDITIONS
No frequently correlated situations
DIAGNOSTIC HISTORY • Bancroftian and Malayan filariasis – Acute manifestations including fever, lymphadenitis, lymphangitis, funiculitis, and epididymitis – Chronic manifestations including abscesses, hyperkeratosis, polyarthritis, hydroceles, lymphoedema, and elephantiasis – Bronchospasm
• Loiasis – Temporary edema, typically of the wrists and ankles, accompanied by pruritus, paresthesia, and urticaria – Worm migration within the ocular region • Onchocerciasis – Subcutaneous nodules, pruritus, rashes, lymphadenopathy, lymphatic obstruction, chronic dermatological conditions, ocular lesions • Dracunculiasis – Painful, inflamed cutaneous lesion harboring a worm and arthritis • Dirofilariasis – Thoracic pain, cough, and hemoptysis • Mansonelliasis
Localized edema, pruritus, pyrexia, cephalalgia, arthralgia, neurological symptoms, and hydroceles
Inquire on travel to endemic regions.
PHYSICAL EXAMINATION
• Bancroftian and Malayan filariasis – Lymphangitis and lymphadenitis – Femoral/inguinal lymphadenopathy – Enlarged epididymis and spermatic cord – Hydrocele, lower extremity lymphoedema – May induce monoarticular arthritis
• Loiasis – Mature worms may migrate beneath the conjunctiva or into the dermis.
Calabar swelling frequently occurs in the wrists and ankles; the edema may persist for only hours but might repeat over several years. • Onchocerciasis – Dermatological alterations range from papular eruptions to regions of hyper- or hypopigmentation.
– Patients may exhibit eczematoid dermatitis and dermal thickening.
– Nontender subcutaneous nodules. – Potential reduction in optical acuity. • Dracunculiasis – A white, filamentous adult worm manifests at the cutaneous surface.
Ulceration in distal extremities. • Dirofilariasis – Typically asymptomatic Mansonelliasis is characterized by angioedema, pruritus, papular rash, alterations in skin pigmentation, fever, headaches, arthralgia, lymphadenopathy, hepatomegaly, and neurological symptoms.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• Bancroftian and Malayan filariasis - Blood smears reveal the presence of filarial worms.
– Serological assays lack specificity in filariasis. – Eosinophilia is frequently absent.
– PCR-based assays for the DNA of W. bancrofti and B. malayi are accessible in research environments.
• Loiasis – Blood smears, skin snips, or skin biopsy
• Onchocerciasis – Microscopic examination of skin biopsies reveals the presence of worms – Dracunculiasis – Diagnosis is clinical.
• Dirofilariasis - Histological Examination
• Mansonelliasis – Blood smears reveal filarial worms.
Microscopic examination of the skin biopsy reveals the presence of worms. Eosinophilia is significant.
Imaging
• Bancroftian and Malayan filariasis — Adult worms may be observed in dilated lymphatics using ultrasound. • Onchocerciasis – Cutaneous and subcutaneous nodules identified with ultrasound and magnetic resonance imaging.
• Dracunculiasis – Standard radiography reveal calcified worms.
• Dirofilariasis – Larvae can become encapsulated within necrotic lung tissue, resulting in distinct pulmonary nodules that may be detectable on computed tomography images.
DIFFERENTIAL DIAGNOSIS
Bancroftian and Malayan filariasis include bacterial lymphangitis, thrombophlebitis, idiopathic hydrocele, congestive heart failure, cirrhosis, and nephrotic syndrome. • Loiasis
– Cutaneous larva migrans, dracunculiasis, gnathostomiasis, myiasis, onchocerciasis • Onchocerciasis – M. streptocerca, scabies, leprosy, eczema, glaucoma, loiasis • Dracunculiasis – Cutaneous larva migrans, loiasis, rat bite infection, gnathostomiasis, myiasis • Dirofilariasis – Asthma, allergies, lung cancer • Mansonelliasis – Loiasis, onchocerciasis
INITIAL THERAPEUTIC AGENT
• Bancroftian and Malayan filariasis — Wolbachia spp., a genus of Rickettsia, are essential for filarial growth. Administer Doxycycline 100 mg orally twice daily for a duration of 4 to 6 weeks to address Wolbachia. Four months subsequent to initiating treatment, a single dosage of albendazole 400 mg orally and ivermectin 150 mg/kg orally was administered.
• Loiasis - Administer a single dosage of diethylcarbamazine citrate (DEC) at 6 mg/kg orally.
• Onchocerciasis - Administer one dosage of ivermectin at 150 mcg/kg orally (ineffective against mature worms). Recur in six months.
– Administer prednisone at a dosage of 1 mg/kg/day orally one week prior to ivermectin if ocular involvement is present.
• Dracunculiasis – Gradual and meticulous removal of the protruding worm.
Metronidazole 250 mg administered orally three times daily may
Mitigate inflammatory response, hence aiding in the expulsion of worms. Mebendazole 400–800 mg each day for 6 days may eradicate the worm.
• M. perstans – Administer albendazole 400 mg orally twice daily for 10 days. • M. streptocerca and M. ozzardi – Administer a single dose of ivermectin at 200 mcg/kg. • Dirofilariasis – No effective pharmacological treatment available. Second Line
• Bancroftian and Malayan filariasis – DEC, as previously mentioned for M. streptocerca. DEC should not be administered in regions with endemic lymphatic filariasis and loiasis/onchocerciasis.
SUPPLEMENTARY THERAPY
Comprehensive Measures
The treatment primarily targets the microfilarial stage of the infection. Adult worms are seldom impacted by a single dose of medicine. Repetitive therapy is frequently required for a cure.
Concerns for Referral
• Specialists in infectious diseases • Ophthalmologist for ocular assessment in onchocerciasis
CHIRURGICAL INTERVENTIONS/ADDITIONAL PROCEDURES
• Nodulectomy of palpable nodules in onchocerciasis • Surgical excision of dirofilariasis from the lung IN-PATIENT CONSIDERATIONS
Preliminary Stabilization
Resuscitation in accordance with advanced life support protocols as necessary
Criteria for Admission
• Patients with septicemia resulting from open wounds • Overnight admission for nocturnal blood sample collection for diagnostic testing
IV Fluids • Administer fluid resuscitation using colloids, such as Gelofusine, in cases of septicemia.
• Maintenance fluids utilizing Ringer's lactate
Nursing
Patients with elephantiasis may require comprehensive nursing care for the affected body portion.
Release Criteria for the resolution of septicemia
CONTINUING CARE POST-TREATMENT RECOMMENDATIONS
Every 4 to 6 weeks for treatment evaluation and symptomatic management
Patient Surveillance
Routine ocular assessments
OUTLOOK
Disability and disfigurement are mitigated by accurate diagnosis and therapy.
COMPLICATIONS
Bancroftian filariasis - Elephantiasis; Septicemia resulting from bacterial infection of exposed sores.
• Onchocerciasis - Visual Impairment

- Published on
Infectious Disease - Exanthem Subitum (Roseola Infantum)
Exanthema subitum is a benign, self-limiting viral infection in children, primarily caused by human herpesvirus 6B (HHV-6B) or, less commonly, by human herpesvirus 7 (HHV-7).
It is sometimes referred to as roseola infantum or sixth sickness.
EPIDEMIOLOGY
Incidence
• It is global.
• Infections predominantly arise between 6 months and 3 years, with 90% occurring prior to the age of 2 years.
Human herpesvirus 7 induces sickness in older children and may correlate with an increased prevalence of febrile seizures.
• Antibody prevalence in the US population over the age of 3 years reaches 100%.
• Antibody titers in the infant, derived from maternal antibodies, are elevated initially, decrease until six months of age, and thereafter increase once more. • Antibody concentrations may remain elevated until the age of 60 years.
Frequency
Human herpesvirus 6B accounts for roughly 10–45% of all febrile illnesses in pediatric patients.
RISK FACTORS
Genetics
In the United States, 1% of individuals are born with hereditary chromosomally integrated HHV-6 infection, originally identified in 1993, with its clinical implications remaining unknown to date.
GENERAL PREVENTION • At present, there is no method to avert initial infection or reactivation of human herpesvirus 6.
Prophylaxis may be required for patients receiving bone marrow transplantation.
PATHOPHYSIOLOGY • The virus remains in a latent condition within secondary lymphoid tissues.
Organs , saliva, and the CNS exhibit a distinct mode of infection following original exposure, unlike other human herpesviruses.
• It can be located in activated CD4+ T-lymphocytes, monocytes, macrophages, endothelial cells, epithelial cells, astrocytes, and B cells, in addition to many organs throughout the body.
Reactivation of the illness predominantly occurs in immunocompromised individuals.
ETIOLOGY • Human herpesvirus 6 exhibits significant genetic similarity to cytomegalovirus (CMV), with a homology of 50%, both belonging to the Beta 2 herpesvirus group.
Human herpesvirus 6A and 6B should be regarded as distinct viruses due to their significant differences.
• The existence of human herpesvirus 7.
FREQUENTLY ASSOCIATED CONDITIONS
This virus may be linked to transplantation.
The association of this virus with several disorders, including AIDS, lymphoma, leukemia, chronic fatigue syndrome, drug-induced hypersensitivity syndrome, and multiple sclerosis in adults, is currently under examination.
HISTORICAL DIAGNOSIS
The incubation phase lasts 10 to 14 days.
Pediatric Patients
• It is a non-threatening condition in children characterized by upper respiratory symptoms, fever, and rash.
• This sickness has been linked to fevers exceeding 41°C.
The child is generally in a mild state of illness, except from the elevated fever.
A maculopapular rash commonly manifests in 10% of cases following the febrile episode, however instances of the disease without a rash are more prevalent. A rash may appear without accompanying fever.
• Upper respiratory symptoms affecting the pharynx, tonsils, and ears, absent conjunctivitis and pharyngeal exudates.
Cervical lymphadenopathy is frequently observed.
• The duration of the illness is 3 to 5 days.
Gastrointestinal symptoms, such as diarrhea and vomiting, may manifest.
• Febrile seizures occur in 10% of cases.
• It is an uncommon etiology of encephalitis in non-transplant patients Grown individuals
• Illness resembling mononucleosis. • This may result in upper respiratory infections or pneumonia accompanied by hepatitis.
Organ Transplant Recipients
Exanthem subitum should be regarded as a potential diagnosis in organ transplant recipients.
Human herpesvirus 6 is a significant contributor to bone marrow suppression and interstitial pneumonitis following bone marrow transplantation.
PHYSICAL EXAMINATION • Fever: Reaching 41°C with sudden onset and rapid resolution.
Rash: Macular or maculopapular, pink, transitory, nonpruritic, devoid of pigmentation and desquamation, emerges when fever abates, initially on the trunk, thereafter disseminating to the face, neck, and limbs, resolving within 1–2 days.
Cervical lymphadenopathy.
• Overall satisfactory condition of the patient.
The anterior fontanelle in neonates may exhibit bulging.
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
• Leukopenia • Mononucleosis • Lymphocytopenia • Atypical lymphocytes • Hepatitis, particularly in adults
• The erythrocyte sedimentation rate is within normal limits. • The cerebrospinal fluid is within normal parameters.
Diagnosis is accomplished using viral isolation, PCR, and serological methods.
• Viral isolation using fast antigen detection from a specimen or tissue culture.
• Serological analysis: IgG and IgM antibodies, antibody avidity, ELISA assay
The existing serological assays are unable to differentiate between HHV-6A and HHV-6B.
• Detection using PCR or real-time PCR in cells or plasma The rapid shell vial assay is employed for transplant recipients.
Magnetic resonance imaging is indicated in cases of suspected central nervous system involvement.
Differential Diagnosis
• Cytomegalovirus (CMV) • Viral upper respiratory infection • Adenovirus • Hepatitis A, B, and C • Measles, rubella
• Significant bacterial infections: The child's health, despite the fever, the rash following the febrile episode, a normal erythrocyte sedimentation rate, and normal CSF fluid support the diagnosis of exanthema subitum. In instances of antibiotic administration, the rash may be regarded as a drug allergy.
THERAPEUTIC MEDICATION • There is no definitive treatment; in the majority of instances, the approach is supportive care.
The condition is responsive to ganciclovir or foscarnet; however, treatment is typically restricted to those who are unwell post-bone marrow transplantation or in severe instances.
SUPPLEMENTARY THERAPY
Comprehensive Strategies
• Medical care is typically provided on an outpatient basis. Instances of febrile seizures or central nervous system involvement necessitate hospitalization.
Utilize acetaminophen/paracetamol and baths to manage fever. • Maintain sufficient hydrated.
ONGOING CARE PROGNOSIS
It is non-threatening and self-resolving, typically associated with a favorable prognosis.
COMPLICATIONS
• Primarily manifest in immunocompromised individuals: Pneumonia
• Hepatitis • Bone marrow suppression
• Encephalitis, meningoencephalitis, and aseptic meningitis
Exanthema subitum is a benign, self-limiting viral infection in children, primarily caused by human herpesvirus 6B (HHV-6B) or, less commonly, by human herpesvirus 7 (HHV-7).
It is sometimes referred to as roseola infantum or sixth sickness.
EPIDEMIOLOGY
Incidence
• It is global.
• Infections predominantly arise between 6 months and 3 years, with 90% occurring prior to the age of 2 years.
Human herpesvirus 7 induces sickness in older children and may correlate with an increased prevalence of febrile seizures.
• Antibody prevalence in the US population over the age of 3 years reaches 100%.
• Antibody titers in the infant, derived from maternal antibodies, are elevated initially, decrease until six months of age, and thereafter increase once more. • Antibody concentrations may remain elevated until the age of 60 years.
Frequency
Human herpesvirus 6B accounts for roughly 10–45% of all febrile illnesses in pediatric patients.
RISK FACTORS
Genetics
In the United States, 1% of individuals are born with hereditary chromosomally integrated HHV-6 infection, originally identified in 1993, with its clinical implications remaining unknown to date.
GENERAL PREVENTION • At present, there is no method to avert initial infection or reactivation of human herpesvirus 6.
Prophylaxis may be required for patients receiving bone marrow transplantation.
PATHOPHYSIOLOGY • The virus remains in a latent condition within secondary lymphoid tissues.
Organs , saliva, and the CNS exhibit a distinct mode of infection following original exposure, unlike other human herpesviruses.
• It can be located in activated CD4+ T-lymphocytes, monocytes, macrophages, endothelial cells, epithelial cells, astrocytes, and B cells, in addition to many organs throughout the body.
Reactivation of the illness predominantly occurs in immunocompromised individuals.
ETIOLOGY • Human herpesvirus 6 exhibits significant genetic similarity to cytomegalovirus (CMV), with a homology of 50%, both belonging to the Beta 2 herpesvirus group.
Human herpesvirus 6A and 6B should be regarded as distinct viruses due to their significant differences.
• The existence of human herpesvirus 7.
FREQUENTLY ASSOCIATED CONDITIONS
This virus may be linked to transplantation.
The association of this virus with several disorders, including AIDS, lymphoma, leukemia, chronic fatigue syndrome, drug-induced hypersensitivity syndrome, and multiple sclerosis in adults, is currently under examination.
HISTORICAL DIAGNOSIS
The incubation phase lasts 10 to 14 days.
Pediatric Patients
• It is a non-threatening condition in children characterized by upper respiratory symptoms, fever, and rash.
• This sickness has been linked to fevers exceeding 41°C.
The child is generally in a mild state of illness, except from the elevated fever.
A maculopapular rash commonly manifests in 10% of cases following the febrile episode, however instances of the disease without a rash are more prevalent. A rash may appear without accompanying fever.
• Upper respiratory symptoms affecting the pharynx, tonsils, and ears, absent conjunctivitis and pharyngeal exudates.
Cervical lymphadenopathy is frequently observed.
• The duration of the illness is 3 to 5 days.
Gastrointestinal symptoms, such as diarrhea and vomiting, may manifest.
• Febrile seizures occur in 10% of cases.
• It is an uncommon etiology of encephalitis in non-transplant patients Grown individuals
• Illness resembling mononucleosis. • This may result in upper respiratory infections or pneumonia accompanied by hepatitis.
Organ Transplant Recipients
Exanthem subitum should be regarded as a potential diagnosis in organ transplant recipients.
Human herpesvirus 6 is a significant contributor to bone marrow suppression and interstitial pneumonitis following bone marrow transplantation.
PHYSICAL EXAMINATION • Fever: Reaching 41°C with sudden onset and rapid resolution.
Rash: Macular or maculopapular, pink, transitory, nonpruritic, devoid of pigmentation and desquamation, emerges when fever abates, initially on the trunk, thereafter disseminating to the face, neck, and limbs, resolving within 1–2 days.
Cervical lymphadenopathy.
• Overall satisfactory condition of the patient.
The anterior fontanelle in neonates may exhibit bulging.
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
• Leukopenia • Mononucleosis • Lymphocytopenia • Atypical lymphocytes • Hepatitis, particularly in adults
• The erythrocyte sedimentation rate is within normal limits. • The cerebrospinal fluid is within normal parameters.
Diagnosis is accomplished using viral isolation, PCR, and serological methods.
• Viral isolation using fast antigen detection from a specimen or tissue culture.
• Serological analysis: IgG and IgM antibodies, antibody avidity, ELISA assay
The existing serological assays are unable to differentiate between HHV-6A and HHV-6B.
• Detection using PCR or real-time PCR in cells or plasma The rapid shell vial assay is employed for transplant recipients.
Magnetic resonance imaging is indicated in cases of suspected central nervous system involvement.
Differential Diagnosis
• Cytomegalovirus (CMV) • Viral upper respiratory infection • Adenovirus • Hepatitis A, B, and C • Measles, rubella
• Significant bacterial infections: The child's health, despite the fever, the rash following the febrile episode, a normal erythrocyte sedimentation rate, and normal CSF fluid support the diagnosis of exanthema subitum. In instances of antibiotic administration, the rash may be regarded as a drug allergy.
THERAPEUTIC MEDICATION • There is no definitive treatment; in the majority of instances, the approach is supportive care.
The condition is responsive to ganciclovir or foscarnet; however, treatment is typically restricted to those who are unwell post-bone marrow transplantation or in severe instances.
SUPPLEMENTARY THERAPY
Comprehensive Strategies
• Medical care is typically provided on an outpatient basis. Instances of febrile seizures or central nervous system involvement necessitate hospitalization.
Utilize acetaminophen/paracetamol and baths to manage fever. • Maintain sufficient hydrated.
ONGOING CARE PROGNOSIS
It is non-threatening and self-resolving, typically associated with a favorable prognosis.
COMPLICATIONS
• Primarily manifest in immunocompromised individuals: Pneumonia
• Hepatitis • Bone marrow suppression
• Encephalitis, meningoencephalitis, and aseptic meningitis

