- Published on
Symptoms and Signs – Differential Diagnosis of Murmurs
Auscultatory murmurs are noises detected within the heart chambers or main arteries. They are categorized according on their timing and length within the cardiac cycle, auscultatory site, intensity, configuration, pitch, and quality.
Timing may be classified as systolic (between S1 and S2), holosystolic (persistent throughout systole), diastolic (between S2 and S1), or continuous across both systole and diastole; systolic and diastolic murmurs can additionally be categorized as early, mid, or late.
Location denotes the region of peak audibility, including the apex, the lower left sternal boundary, or an intercostal space. Loudness is assessed on a scale from 1 to 6. A grade 1 murmur is exceedingly subtle, discernible just by meticulous auscultation. A grade 2 murmur is a faint yet discernible murmur. Murmurs classified as grade 3 are of moderate loudness. A grade 4 murmur is a pronounced murmur accompanied with a potential intermittent thrill. Grade 5 murmurs are pronounced and accompanied by a detectable precordial thrill. Grade 6 murmurs are pronounced and, similar to grade 5 murmurs, are accompanied by a palpable excitement. A grade 6 murmur is discernible even after the stethoscope is removed from the thoracic wall.
Configuration, or shape, pertains to the characteristics of loudness — crescendo (increases in volume), decrescendo (decreases in volume), crescendo-decrescendo (first rises, then falls), decrescendo-crescendo (initially falls, then rises), plateau (constant intensity), or varied (inconsistent intensity). The pitch of the murmur may be elevated or diminished. The quality might be characterized as harsh, rumbling, blowing, scratching, buzzing, melodic, or squeaking.
Murmurs may indicate increased blood flow through either normal or pathological conditions. Valves facilitate forward blood flow through a constricted or irregular valve or into a dilated channel; let blood backflow through an incompetent valve, septal defect, or patent ductus arteriosus; or result in decreased blood viscosity. Murmurs, typically indicative of organic heart illness, may occasionally denote an emergency; for instance, a pronounced holosystolic murmur following an acute myocardial infarction (MI) may indicate papillary muscle rupture or a ventricular septal defect. Murmurs may also arise with the surgical implantation of a replacement valve.
Certain murmurs are benign or functioning. An innocent systolic murmur is often quiet, medium-pitched, and most pronounced along the left sternal border at the second or third intercostal space. It is intensified by physical exertion, agitation, fever, pregnancy, anemia, or thyrotoxicosis. Examples include Still's murmur in children and mammary souffle, typically auscultated across either breast during late pregnancy and early postpartum periods.
Medical History and Physical Assessment
Upon detecting a murmur, endeavor to ascertain its classification by meticulous auscultation.. Utilize the bell of your stethoscope for low-frequency murmurs and the diaphragm for high-frequency murmurs.
URGENT INTERVENTIONS
When Murmurs Indicate an Emergency Murmurs, particularly newly acquired ones, may indicate a significant complication in individuals with bacterial endocarditis or a recent acute myocardial infarction (MI), while not typically being an emergency sign.
When managing a patient with confirmed or suspected bacterial endocarditis, meticulously auscultate for the presence of new murmurs. Their advancement, accompanied by crackles, jugular vein distention, orthopnea, and dyspnea, these symptoms may indicate heart failure.
Consistent auscultation is crucial for a patient who has suffered an acute myocardial infarction. A pronounced decrescendo holosystolic murmur at the apex, radiating to the axilla and left sternal border or throughout the chest, is noteworthy, especially when accompanied by a widely divided S2 and an atrial gallop (S4). The presence of this murmur, alongside indications of severe pulmonary edema, typically signifies the onset of acute mitral regurgitation resulting from the rupture of the chordae tendineae – a medical emergency.
Subsequently, acquire the patient's medical history. Inquire whether the murmur is a recent finding or if it has been recognized since birth or infancy. Determine whether the patient has encountered concomitant symptoms, specifically palpitations, dizziness, syncope, chest discomfort, dyspnea, and weariness. Examine the patient's medical history, with specific attention to any occurrences of rheumatic fever, heart disease, or heart surgery, especially prosthetic valve replacement.
Conduct a methodical physical assessment. Particularly observe the occurrence of cardiac arrhythmias, jugular vein distention, and pulmonary manifestations like dyspnea, orthopnea, and crackles. Is the patient's liver painful or palpable? Does he exhibit peripheral edema?
Etiological Factors
Aortic regurgitation.
Acute aortic insufficiency generally generates a quiet, brief diastolic murmur along the left sternal boundary, most audible when the patient is seated and leans forward, as well as at the conclusion of a forced expiration. S2 may be diminished or missing. A quiet, brief midsystolic murmur may occasionally be auscultated above the second right intercostal region. Accompanying findings consist of tachycardia, dyspnea, jugular vein distention, crackles, heightened tiredness, and pale, chilly extremities.
Chronic aortic insufficiency produces a high-pitched, blown, decrescendo diastolic murmur, optimally auscultated over the second or third right intercostal space or the left sternal border, with the patient in a seated position, leaning forward, and holding their breath following deep expiration. An Austin Flint murmur — a low-frequency, mid-to-late diastolic murmur most prominently detected near the apex — may also manifest. Complications may not manifest until the patient reaches ages 40 to 50; subsequent observations typically include palpitations, tachycardia, angina, heightened tiredness, dyspnea, orthopnea, and crackles.
Aortic stenosis
The murmur associated with aortic stenosis is systolic, commencing after S1 and concluding at or prior to the closing of the aortic valve. It is abrasive and jarring, of medium pitch, exhibiting a crescendo and decrescendo. The murmur is most pronounced over the second right intercostal space when the patient is seated and leaning forward; it may also be audible at the apex, the suprasternal notch (Erb’s point), and the carotid arteries.
In cases of advanced disease, S2 may be perceived as a singular sound, with aortic closure being inaudible. An early systolic ejection click at the apex is characteristic but is missing in cases of extensive valve calcification. Associated signs and symptoms often manifest by age 30 in congenital aortic stenosis, between ages 30 and 65 in rheumatic disease-related stenosis, and post age 65 in calcific aortic stenosis. Symptoms may encompass dizziness, syncope, exertional dyspnea, paroxysmal nocturnal dyspnea, weariness, and angina.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy produces a pronounced late systolic murmur that concludes at S2. The murmur is best detected around the left sternal border and at the apex, often accompanied by an audible S3 or S4. The murmur diminishes with squatting and intensifies with sitting. Primary related symptoms include dyspnea and chest discomfort; palpitations, disorientation, and syncope may additionally manifest.
Mitral regurgitation
Acute mitral insufficiency is marked by a medium-pitched, blown, early systolic or holosystolic decrescendo murmur near the apex, accompanied by a widely split S2 and frequently an S4. This murmur does not intensify during inspiration, unlike tricuspid insufficiency. Commonly observed findings often encompass tachycardia and indications of acute pulmonary edema.
Chronic mitral insufficiency results in a high-pitched, blowing, holosystolic plateau murmur that is most pronounced at the apex and typically radiates to the axilla or back. Fatigue, dyspnea, and palpitations may additionally manifest.
Mitral valve prolapse
Mitral prolapse produces a midsystolic to late-systolic click accompanied by a high-pitched late-systolic crescendo murmur, most prominently audible at the apex. Intermittently, many clicks may be audible, with or without a systolic murmur. Related symptoms encompass cardiac awareness, migraine headaches, dizziness, weakness, syncope, palpitations, chest discomfort, dyspnea, significant episodic fatigue, mood fluctuations, and anxiety.
Mitral stenosis
In mitral stenosis, the murmur is characterized as mild, low-pitched, rumbling, crescendo-decrescendo, and diastolic, often accompanied by a pronounced S1 or an opening snap, which is a key indicator. The optimal auscultation occurs at the apex with the patient positioned laterally to the left. Moderate exertion facilitates the audibility of this murmur.
In cases of severe stenosis, a murmur indicative of mitral regurgitation may be audible. Additional observations encompass hemoptysis, exertional dyspnea, tiredness, and indications of acute pulmonary edema.
Myxomas
A left atrial myxoma, the most prevalent type, typically generates a middiastolic murmur and a holosystolic murmur that is most pronounced at the apex, accompanied by an S4, an early diastolic thudding sound (tumor plop), and a loud, widely divided S1. Associated symptoms including dyspnea, orthopnea, thoracic discomfort, exhaustion, weight reduction, and syncope.
A right atrial myxoma produces a late diastolic rumbling murmur, a holosystolic crescendo murmur, and a tumor plop, most prominently audible near the lower left sternal boundary. Additional findings including tiredness, peripheral edema, ascites, and hepatomegaly.
A left ventricular myxoma, which is rare, generates a systolic murmur most prominently detected at the lower left sternal border, along with arrhythmias, dyspnea, and syncope.
A right ventricular myxoma typically produces a systolic ejection murmur accompanied by a delayed S2 and a tumor plop, most prominently audible near the left sternal boundary. It is associated with peripheral edema, hepatomegaly, ascites, dyspnea, and syncope.
Rupture of the papillary muscle
A loud holosystolic murmur can be auscultated near the apex in cases of papillary muscle rupture, a life-threatening consequence of acute myocardial infarction. Associated findings encompass significant dyspnea, thoracic discomfort, syncope, hemoptysis, tachycardia, and hypotension.
Rheumatic fever accompanied by pericarditis
A pericardial friction rub, accompanied by murmurs and gallops, is optimally auscultated when the patient is positioned on hands and knees during forced expiration. The predominant murmurs detected include the systolic murmur of mitral regurgitation, a midsystolic murmur resulting from mitral valve leaflet edema, and the diastolic murmur of aortic regurgitation. Additional signs and symptoms encompass fever, joint and sternal discomfort, edema, and tachypnea.
Tricuspid regurgitation
Tricuspid insufficiency is a valve disorder characterized by a mild, high-pitched, holosystolic blowing murmur that intensifies with inspiration (Carvallo’s sign), diminishes with exhale and Valsalva maneuver, and is optimally auscultated over the lower left sternal border and the xiphoid region. After an extended asymptomatic phase, symptoms such as exertional dyspnea and orthopnea may manifest, accompanied by jugular vein distention, ascites, peripheral cyanosis and edema, muscle wasting, lethargy, weakness, and syncope.
Tricuspid stenosis
Tricuspid stenosis is a valve condition that generates a diastolic murmur like to that of mitral stenosis, although more pronounced during inspiration and diminished during exhale and the Valsalva maneuver. S1 may also exhibit increased loudness. Accompanying signs and symptoms encompass fatigue, syncope, peripheral edema, jugular vein distention, ascites, hepatomegaly, and dyspnea.
Alternative Causes
Therapies. Prosthetic valve replacement can produce diverse murmurs, influenced by the location, valve material, and operational technique.
Particular Considerations
Prepare the patient for diagnostic procedures, including electrocardiography, echocardiography, and angiography. Administer an antibiotic and an anticoagulant as indicated. Due to the distressing nature of a heart problem, offer emotional support.
Patient Consultation
Detail the indications and symptoms the patient must communicate and the applicability of prophylactic antibiotics, if relevant.
Pediatric Guidelines
Innocuous murmurs, such as Still's murmur, are frequently seen in young children and generally resolve after puberty. Pathognomonic heart murmurs in newborns and young children typically arise from congenital heart disease, including atrial and ventricular septal abnormalities. Additional murmurs may be acquired, as seen in rheumatic heart disease.
Auscultatory murmurs are noises detected within the heart chambers or main arteries. They are categorized according on their timing and length within the cardiac cycle, auscultatory site, intensity, configuration, pitch, and quality.
Timing may be classified as systolic (between S1 and S2), holosystolic (persistent throughout systole), diastolic (between S2 and S1), or continuous across both systole and diastole; systolic and diastolic murmurs can additionally be categorized as early, mid, or late.
Location denotes the region of peak audibility, including the apex, the lower left sternal boundary, or an intercostal space. Loudness is assessed on a scale from 1 to 6. A grade 1 murmur is exceedingly subtle, discernible just by meticulous auscultation. A grade 2 murmur is a faint yet discernible murmur. Murmurs classified as grade 3 are of moderate loudness. A grade 4 murmur is a pronounced murmur accompanied with a potential intermittent thrill. Grade 5 murmurs are pronounced and accompanied by a detectable precordial thrill. Grade 6 murmurs are pronounced and, similar to grade 5 murmurs, are accompanied by a palpable excitement. A grade 6 murmur is discernible even after the stethoscope is removed from the thoracic wall.
Configuration, or shape, pertains to the characteristics of loudness — crescendo (increases in volume), decrescendo (decreases in volume), crescendo-decrescendo (first rises, then falls), decrescendo-crescendo (initially falls, then rises), plateau (constant intensity), or varied (inconsistent intensity). The pitch of the murmur may be elevated or diminished. The quality might be characterized as harsh, rumbling, blowing, scratching, buzzing, melodic, or squeaking.
Murmurs may indicate increased blood flow through either normal or pathological conditions. Valves facilitate forward blood flow through a constricted or irregular valve or into a dilated channel; let blood backflow through an incompetent valve, septal defect, or patent ductus arteriosus; or result in decreased blood viscosity. Murmurs, typically indicative of organic heart illness, may occasionally denote an emergency; for instance, a pronounced holosystolic murmur following an acute myocardial infarction (MI) may indicate papillary muscle rupture or a ventricular septal defect. Murmurs may also arise with the surgical implantation of a replacement valve.
Certain murmurs are benign or functioning. An innocent systolic murmur is often quiet, medium-pitched, and most pronounced along the left sternal border at the second or third intercostal space. It is intensified by physical exertion, agitation, fever, pregnancy, anemia, or thyrotoxicosis. Examples include Still's murmur in children and mammary souffle, typically auscultated across either breast during late pregnancy and early postpartum periods.
Medical History and Physical Assessment
Upon detecting a murmur, endeavor to ascertain its classification by meticulous auscultation.. Utilize the bell of your stethoscope for low-frequency murmurs and the diaphragm for high-frequency murmurs.
URGENT INTERVENTIONS
When Murmurs Indicate an Emergency Murmurs, particularly newly acquired ones, may indicate a significant complication in individuals with bacterial endocarditis or a recent acute myocardial infarction (MI), while not typically being an emergency sign.
When managing a patient with confirmed or suspected bacterial endocarditis, meticulously auscultate for the presence of new murmurs. Their advancement, accompanied by crackles, jugular vein distention, orthopnea, and dyspnea, these symptoms may indicate heart failure.
Consistent auscultation is crucial for a patient who has suffered an acute myocardial infarction. A pronounced decrescendo holosystolic murmur at the apex, radiating to the axilla and left sternal border or throughout the chest, is noteworthy, especially when accompanied by a widely divided S2 and an atrial gallop (S4). The presence of this murmur, alongside indications of severe pulmonary edema, typically signifies the onset of acute mitral regurgitation resulting from the rupture of the chordae tendineae – a medical emergency.
Subsequently, acquire the patient's medical history. Inquire whether the murmur is a recent finding or if it has been recognized since birth or infancy. Determine whether the patient has encountered concomitant symptoms, specifically palpitations, dizziness, syncope, chest discomfort, dyspnea, and weariness. Examine the patient's medical history, with specific attention to any occurrences of rheumatic fever, heart disease, or heart surgery, especially prosthetic valve replacement.
Conduct a methodical physical assessment. Particularly observe the occurrence of cardiac arrhythmias, jugular vein distention, and pulmonary manifestations like dyspnea, orthopnea, and crackles. Is the patient's liver painful or palpable? Does he exhibit peripheral edema?
Etiological Factors
Aortic regurgitation.
Acute aortic insufficiency generally generates a quiet, brief diastolic murmur along the left sternal boundary, most audible when the patient is seated and leans forward, as well as at the conclusion of a forced expiration. S2 may be diminished or missing. A quiet, brief midsystolic murmur may occasionally be auscultated above the second right intercostal region. Accompanying findings consist of tachycardia, dyspnea, jugular vein distention, crackles, heightened tiredness, and pale, chilly extremities.
Chronic aortic insufficiency produces a high-pitched, blown, decrescendo diastolic murmur, optimally auscultated over the second or third right intercostal space or the left sternal border, with the patient in a seated position, leaning forward, and holding their breath following deep expiration. An Austin Flint murmur — a low-frequency, mid-to-late diastolic murmur most prominently detected near the apex — may also manifest. Complications may not manifest until the patient reaches ages 40 to 50; subsequent observations typically include palpitations, tachycardia, angina, heightened tiredness, dyspnea, orthopnea, and crackles.
Aortic stenosis
The murmur associated with aortic stenosis is systolic, commencing after S1 and concluding at or prior to the closing of the aortic valve. It is abrasive and jarring, of medium pitch, exhibiting a crescendo and decrescendo. The murmur is most pronounced over the second right intercostal space when the patient is seated and leaning forward; it may also be audible at the apex, the suprasternal notch (Erb’s point), and the carotid arteries.
In cases of advanced disease, S2 may be perceived as a singular sound, with aortic closure being inaudible. An early systolic ejection click at the apex is characteristic but is missing in cases of extensive valve calcification. Associated signs and symptoms often manifest by age 30 in congenital aortic stenosis, between ages 30 and 65 in rheumatic disease-related stenosis, and post age 65 in calcific aortic stenosis. Symptoms may encompass dizziness, syncope, exertional dyspnea, paroxysmal nocturnal dyspnea, weariness, and angina.
Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy produces a pronounced late systolic murmur that concludes at S2. The murmur is best detected around the left sternal border and at the apex, often accompanied by an audible S3 or S4. The murmur diminishes with squatting and intensifies with sitting. Primary related symptoms include dyspnea and chest discomfort; palpitations, disorientation, and syncope may additionally manifest.
Mitral regurgitation
Acute mitral insufficiency is marked by a medium-pitched, blown, early systolic or holosystolic decrescendo murmur near the apex, accompanied by a widely split S2 and frequently an S4. This murmur does not intensify during inspiration, unlike tricuspid insufficiency. Commonly observed findings often encompass tachycardia and indications of acute pulmonary edema.
Chronic mitral insufficiency results in a high-pitched, blowing, holosystolic plateau murmur that is most pronounced at the apex and typically radiates to the axilla or back. Fatigue, dyspnea, and palpitations may additionally manifest.
Mitral valve prolapse
Mitral prolapse produces a midsystolic to late-systolic click accompanied by a high-pitched late-systolic crescendo murmur, most prominently audible at the apex. Intermittently, many clicks may be audible, with or without a systolic murmur. Related symptoms encompass cardiac awareness, migraine headaches, dizziness, weakness, syncope, palpitations, chest discomfort, dyspnea, significant episodic fatigue, mood fluctuations, and anxiety.
Mitral stenosis
In mitral stenosis, the murmur is characterized as mild, low-pitched, rumbling, crescendo-decrescendo, and diastolic, often accompanied by a pronounced S1 or an opening snap, which is a key indicator. The optimal auscultation occurs at the apex with the patient positioned laterally to the left. Moderate exertion facilitates the audibility of this murmur.
In cases of severe stenosis, a murmur indicative of mitral regurgitation may be audible. Additional observations encompass hemoptysis, exertional dyspnea, tiredness, and indications of acute pulmonary edema.
Myxomas
A left atrial myxoma, the most prevalent type, typically generates a middiastolic murmur and a holosystolic murmur that is most pronounced at the apex, accompanied by an S4, an early diastolic thudding sound (tumor plop), and a loud, widely divided S1. Associated symptoms including dyspnea, orthopnea, thoracic discomfort, exhaustion, weight reduction, and syncope.
A right atrial myxoma produces a late diastolic rumbling murmur, a holosystolic crescendo murmur, and a tumor plop, most prominently audible near the lower left sternal boundary. Additional findings including tiredness, peripheral edema, ascites, and hepatomegaly.
A left ventricular myxoma, which is rare, generates a systolic murmur most prominently detected at the lower left sternal border, along with arrhythmias, dyspnea, and syncope.
A right ventricular myxoma typically produces a systolic ejection murmur accompanied by a delayed S2 and a tumor plop, most prominently audible near the left sternal boundary. It is associated with peripheral edema, hepatomegaly, ascites, dyspnea, and syncope.
Rupture of the papillary muscle
A loud holosystolic murmur can be auscultated near the apex in cases of papillary muscle rupture, a life-threatening consequence of acute myocardial infarction. Associated findings encompass significant dyspnea, thoracic discomfort, syncope, hemoptysis, tachycardia, and hypotension.
Rheumatic fever accompanied by pericarditis
A pericardial friction rub, accompanied by murmurs and gallops, is optimally auscultated when the patient is positioned on hands and knees during forced expiration. The predominant murmurs detected include the systolic murmur of mitral regurgitation, a midsystolic murmur resulting from mitral valve leaflet edema, and the diastolic murmur of aortic regurgitation. Additional signs and symptoms encompass fever, joint and sternal discomfort, edema, and tachypnea.
Tricuspid regurgitation
Tricuspid insufficiency is a valve disorder characterized by a mild, high-pitched, holosystolic blowing murmur that intensifies with inspiration (Carvallo’s sign), diminishes with exhale and Valsalva maneuver, and is optimally auscultated over the lower left sternal border and the xiphoid region. After an extended asymptomatic phase, symptoms such as exertional dyspnea and orthopnea may manifest, accompanied by jugular vein distention, ascites, peripheral cyanosis and edema, muscle wasting, lethargy, weakness, and syncope.
Tricuspid stenosis
Tricuspid stenosis is a valve condition that generates a diastolic murmur like to that of mitral stenosis, although more pronounced during inspiration and diminished during exhale and the Valsalva maneuver. S1 may also exhibit increased loudness. Accompanying signs and symptoms encompass fatigue, syncope, peripheral edema, jugular vein distention, ascites, hepatomegaly, and dyspnea.
Alternative Causes
Therapies. Prosthetic valve replacement can produce diverse murmurs, influenced by the location, valve material, and operational technique.
Particular Considerations
Prepare the patient for diagnostic procedures, including electrocardiography, echocardiography, and angiography. Administer an antibiotic and an anticoagulant as indicated. Due to the distressing nature of a heart problem, offer emotional support.
Patient Consultation
Detail the indications and symptoms the patient must communicate and the applicability of prophylactic antibiotics, if relevant.
Pediatric Guidelines
Innocuous murmurs, such as Still's murmur, are frequently seen in young children and generally resolve after puberty. Pathognomonic heart murmurs in newborns and young children typically arise from congenital heart disease, including atrial and ventricular septal abnormalities. Additional murmurs may be acquired, as seen in rheumatic heart disease.

- Published on
Infectious Disease - Infective Esophagitis
FUNDAMENTAL DESCRIPTION
Esophageal infection caused by various fungus, viruses, and bacteria
EPIDEMIOLOGY Incidence
• Infectious esophagitis is uncommon in individuals with a normal immune system but prevalent among immunocompromised patients, those on medications that alter the normal esophageal microflora or immune function, and in cases where abnormalities impede the clearance of the esophageal lumen. • Primary cytomegalovirus (CMV) infections are prevalent in preschool children and young adults. Nonetheless, they infrequently induce esophagitis in immunocompetent individuals.
RISK FACTORS
• Immune deficiencies • Pharmacological agents that may modify immune function or esophageal microbiota • Anatomical anomalies or motility issues of the esophagus
GENERAL PREVENTION • Mitigation of risk factors, when feasible
• Suitable antiretroviral therapy to reduce immunosuppression in HIV-positive individuals
ETIOLOGY • The predominant etiological agents of infectious esophagitis in both immunocompromised and immunocompetent patients are one or a combination of the following three organisms: Candida spp., herpes simplex virus (HSV), and cytomegalovirus (CMV).
• The majority of Candida esophagitis cases are attributed to C. albicans. Diseases symptomatic of C. glabrata and C. krusei have also been documented.
• Other pathogens that may seldom induce infectious esophagitis include the following:
– Aspergillus species – Histoplasma species – Blastomyces dermatitidis – Varicella zoster virus
– Epstein–Barr virus – Human papillomavirus – Mycobacterium TB and Mycobacterium avium – Normal oropharyngeal flora (rarely) including Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus viridans, and Bacillus species – Acute HIV infection
HISTORY OF DIAGNOSIS
Dysphagia, odynophagia, or both are the most prevalent symptoms.
• Chronic chest pain is also prevalent.
• Additional nonspecific clinical signs, such as weight loss, may arise from these symptoms or indicate an underlying illness responsible for the esophagitis.
Local problems, such as hemorrhage, esophageal perforation, or fistula formation, may arise in the presence of deep esophageal ulcerations caused by infected esophagitis.
Infectious esophagitis might be asymptomatic. The prevalence of asymptomatic esophageal infections is indeterminate.
PHYSICAL EXAMINATION
CMV esophagitis may manifest with systemic symptoms (e.g., fever, nausea, vomiting, or abdominal pain), while Candida and HSV esophagitis typically arise.
Oral lesions. Nonetheless, these sporadic discrepancies are not distinctive. The lack of thrush does not exclude the possibility of Candida esophagitis.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• Hematologic profile • Serological testing for HSV, CMV, and HIV • CMV antigenemia assays or CMV molecular amplification methods
• Brush cytology specimens acquired via endoscopy for the diagnosis of Candida and HSV esophagitis. • Tissue culture for the diagnosis of HSV and CMV esophagitis. Culture is not typically advised for diagnosing Candida esophagitis. This is designated for instances exhibiting clinical characteristics indicative of a pathogen resistant to conventional antifungal treatment.
Imaging
Radiographic assessment following a barium swallow reveals an uneven, frayed look of the esophagus mucosa in instances of Candida esophagitis. At times, the image is indistinguishable from that observed in instances of HSV and CMV esophagitis.
Diagnostic Procedures/Other • Endoscopy and tissue sampling for histological evaluation or brush cytology.
The standard endoscopic presentation of Candida esophagitis features white plaques on the mucosa that frequently hemorrhage upon removal by the endoscope.
Endoscopy in HSV esophagitis demonstrates tiny, well-defined ulcers with a yellowish base. The esophageal mucosa between lesions may frequently appear normal. Shallow, elongated ulcerations, encircled by seemingly normal mucosa, may characterize the endoscopic presentation of CMV esophagitis. Nevertheless, the endoscopic characteristics of Candida, HSV, or CMV esophagitis may be indistinguishable.
Pathological Observations
• Endoscopic tissue specimens may reveal: – Budding yeast cells, hyphae, or pseudohyphae in Candida esophagitis – Multinucleated giant cells and intranuclear inclusion bodies in HSV esophagitis – Cytomegaly of fibroblasts and endothelial cells with intranuclear and cytoplasmic inclusion bodies in
CMV esophagitis.
DIFFERENTIAL DIAGNOSIS
• Esophageal carcinoma (primary or metastatic). • Systemic conditions including: – Crohn's disease
Sarcoidosis
Collagen vascular disorders
Pill esophagitis may occur following the administration of specific antibiotics (such as tetracycline, doxycycline, clindamycin, ciprofloxacin, among others), potassium chloride, nonsteroidal anti-inflammatory medications, and quinidine.
Chemotherapy-induced esophagitis (dactinomycin, bleomycin, cytarabine, methotrexate, and other agents).
• Esophagitis resulting from radiation or the simultaneous application of radiation and chemotherapy.
• Inflammation resulting from sclerotherapy of esophageal varices.
• Idiopathic (aphthous) esophageal ulcers associated with HIV infection.
Oral lesions are frequently observed in patients with Candida and HSV esophagitis, although CMV esophagitis is infrequently linked to stomatitis.
INITIAL THERAPY MEDICATION
Systemic antifungal therapy is invariably necessary for Candida esophagitis (A-II).
A diagnostic trial of antifungal medication is warranted prior to doing an endoscopic examination (B-II).
Oral fluconazole at a dosage of 200–400 mg (3–6 mg/kg) daily for a duration of 14–21 days is advised (A-I). For individuals unable to endure oral therapy: Administer intravenous fluconazole 400 mg (6 mg/kg) daily, deoxycholate amphotericin B 0.3–0.7 mg/kg daily, or an echinocandin (B-II).
For fluconazole-refractory disease: Itraconazole solution 200 mg daily, posaconazole suspension 400 mg twice daily, or voriconazole 200 mg twice daily, taken intravenously or orally for 14–21 days.
• For recurring infections: Administer suppressive therapy with fluconazole at a dosage of 100–200 mg three times weekly (3) (A-I).
• In individuals with AIDS, the use of HAART is advised to mitigate recurring infections (A-I).
HSV esophagitis typically resolves spontaneously in immunocompetent individuals.
Immunocompromised people ought to receive antiviral medications for a duration of 14 to 21 days. Acyclovir 400 mg orally five times daily, valacyclovir 1 g orally three times daily, famciclovir 500 mg orally three times daily. For individuals unable to endure oral therapy: Acyclovir 5 mg/kg intravenously every 8 hours for 7 to 14 days, succeeded by an oral antiviral for a minimum of 1 further week.
Prophylactic therapy with acyclovir at a dosage of 200–400 mg orally per day or 5 mg/kg intravenously twice day may be warranted in cases with elevated risk for HSV reactivation.
CMV esophagitis is managed with ganciclovir at a dosage of 5 mg/kg intravenously twice day for a minimum duration of 2 weeks.
Maintenance therapy with valganciclovir 900 mg orally daily may be required to prevent recurrence of CMV esophagitis in individuals with significant immunocompromise.
To avert CMV infection, CMV seronegative transplant recipients from seropositive donors should undergo antiviral prophylaxis.
Idiopathic (aphthous) esophageal ulcers in HIV infection are managed with prednisone or thalidomide.
Second Line
• For fluconazole-refractory Candida esophagitis: Micafungin 150 mg daily, caspofungin 50 mg daily, anidulafungin 200 mg daily, or deoxycholate
Amphotericin B 0.3–0.7 mg/kg per day (B-II).
• Echinocandins correlate with elevated relapse rates in comparison to fluconazole. • For ganciclovir-resistant HSV or CMV esophagitis: Foscarnet.
INPATIENT CONSIDERATIONS
Criteria for Admission
Outpatient care is suitable unless the patient's immune state is significantly weakened or the infection is exceedingly severe. In such instances, hospitalization may be required.
Intravenous Fluids
Should the patient endure significant odynophagia or if esophagitis is coupled with oral lesions that hinder chewing or swallowing, the provision of intravenous fluids may be requisite.
CONTINUING MANAGEMENT POST-TREATMENT SUGGESTIONS
The anticipated course and prognosis are contingent upon the underlying disease and pathogen; in cases of severe immunosuppression, extended therapy with efficacious drugs is required.
• Patients diagnosed with infectious esophagitis should schedule a follow-up appointment two weeks post-symptom resolution. • The majority of patients with Candida esophagitis typically experience symptom clearance within seven days of initiating treatment.
Myelosuppression is the primary adverse effect of ganciclovir therapy. The simultaneous use of zidovudine may exacerbate myelosuppression.
COMPLICATIONS
• Complications are rare. Severe local consequences may arise from deep esophageal ulcers, including massive hemorrhage.
– Esophageal perforation – Esophagobronchial or esophagomediastinal fistulas
FUNDAMENTAL DESCRIPTION
Esophageal infection caused by various fungus, viruses, and bacteria
EPIDEMIOLOGY Incidence
• Infectious esophagitis is uncommon in individuals with a normal immune system but prevalent among immunocompromised patients, those on medications that alter the normal esophageal microflora or immune function, and in cases where abnormalities impede the clearance of the esophageal lumen. • Primary cytomegalovirus (CMV) infections are prevalent in preschool children and young adults. Nonetheless, they infrequently induce esophagitis in immunocompetent individuals.
RISK FACTORS
• Immune deficiencies • Pharmacological agents that may modify immune function or esophageal microbiota • Anatomical anomalies or motility issues of the esophagus
GENERAL PREVENTION • Mitigation of risk factors, when feasible
• Suitable antiretroviral therapy to reduce immunosuppression in HIV-positive individuals
ETIOLOGY • The predominant etiological agents of infectious esophagitis in both immunocompromised and immunocompetent patients are one or a combination of the following three organisms: Candida spp., herpes simplex virus (HSV), and cytomegalovirus (CMV).
• The majority of Candida esophagitis cases are attributed to C. albicans. Diseases symptomatic of C. glabrata and C. krusei have also been documented.
• Other pathogens that may seldom induce infectious esophagitis include the following:
– Aspergillus species – Histoplasma species – Blastomyces dermatitidis – Varicella zoster virus
– Epstein–Barr virus – Human papillomavirus – Mycobacterium TB and Mycobacterium avium – Normal oropharyngeal flora (rarely) including Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus viridans, and Bacillus species – Acute HIV infection
HISTORY OF DIAGNOSIS
Dysphagia, odynophagia, or both are the most prevalent symptoms.
• Chronic chest pain is also prevalent.
• Additional nonspecific clinical signs, such as weight loss, may arise from these symptoms or indicate an underlying illness responsible for the esophagitis.
Local problems, such as hemorrhage, esophageal perforation, or fistula formation, may arise in the presence of deep esophageal ulcerations caused by infected esophagitis.
Infectious esophagitis might be asymptomatic. The prevalence of asymptomatic esophageal infections is indeterminate.
PHYSICAL EXAMINATION
CMV esophagitis may manifest with systemic symptoms (e.g., fever, nausea, vomiting, or abdominal pain), while Candida and HSV esophagitis typically arise.
Oral lesions. Nonetheless, these sporadic discrepancies are not distinctive. The lack of thrush does not exclude the possibility of Candida esophagitis.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• Hematologic profile • Serological testing for HSV, CMV, and HIV • CMV antigenemia assays or CMV molecular amplification methods
• Brush cytology specimens acquired via endoscopy for the diagnosis of Candida and HSV esophagitis. • Tissue culture for the diagnosis of HSV and CMV esophagitis. Culture is not typically advised for diagnosing Candida esophagitis. This is designated for instances exhibiting clinical characteristics indicative of a pathogen resistant to conventional antifungal treatment.
Imaging
Radiographic assessment following a barium swallow reveals an uneven, frayed look of the esophagus mucosa in instances of Candida esophagitis. At times, the image is indistinguishable from that observed in instances of HSV and CMV esophagitis.
Diagnostic Procedures/Other • Endoscopy and tissue sampling for histological evaluation or brush cytology.
The standard endoscopic presentation of Candida esophagitis features white plaques on the mucosa that frequently hemorrhage upon removal by the endoscope.
Endoscopy in HSV esophagitis demonstrates tiny, well-defined ulcers with a yellowish base. The esophageal mucosa between lesions may frequently appear normal. Shallow, elongated ulcerations, encircled by seemingly normal mucosa, may characterize the endoscopic presentation of CMV esophagitis. Nevertheless, the endoscopic characteristics of Candida, HSV, or CMV esophagitis may be indistinguishable.
Pathological Observations
• Endoscopic tissue specimens may reveal: – Budding yeast cells, hyphae, or pseudohyphae in Candida esophagitis – Multinucleated giant cells and intranuclear inclusion bodies in HSV esophagitis – Cytomegaly of fibroblasts and endothelial cells with intranuclear and cytoplasmic inclusion bodies in
CMV esophagitis.
DIFFERENTIAL DIAGNOSIS
• Esophageal carcinoma (primary or metastatic). • Systemic conditions including: – Crohn's disease
Sarcoidosis
Collagen vascular disorders
Pill esophagitis may occur following the administration of specific antibiotics (such as tetracycline, doxycycline, clindamycin, ciprofloxacin, among others), potassium chloride, nonsteroidal anti-inflammatory medications, and quinidine.
Chemotherapy-induced esophagitis (dactinomycin, bleomycin, cytarabine, methotrexate, and other agents).
• Esophagitis resulting from radiation or the simultaneous application of radiation and chemotherapy.
• Inflammation resulting from sclerotherapy of esophageal varices.
• Idiopathic (aphthous) esophageal ulcers associated with HIV infection.
Oral lesions are frequently observed in patients with Candida and HSV esophagitis, although CMV esophagitis is infrequently linked to stomatitis.
INITIAL THERAPY MEDICATION
Systemic antifungal therapy is invariably necessary for Candida esophagitis (A-II).
A diagnostic trial of antifungal medication is warranted prior to doing an endoscopic examination (B-II).
Oral fluconazole at a dosage of 200–400 mg (3–6 mg/kg) daily for a duration of 14–21 days is advised (A-I). For individuals unable to endure oral therapy: Administer intravenous fluconazole 400 mg (6 mg/kg) daily, deoxycholate amphotericin B 0.3–0.7 mg/kg daily, or an echinocandin (B-II).
For fluconazole-refractory disease: Itraconazole solution 200 mg daily, posaconazole suspension 400 mg twice daily, or voriconazole 200 mg twice daily, taken intravenously or orally for 14–21 days.
• For recurring infections: Administer suppressive therapy with fluconazole at a dosage of 100–200 mg three times weekly (3) (A-I).
• In individuals with AIDS, the use of HAART is advised to mitigate recurring infections (A-I).
HSV esophagitis typically resolves spontaneously in immunocompetent individuals.
Immunocompromised people ought to receive antiviral medications for a duration of 14 to 21 days. Acyclovir 400 mg orally five times daily, valacyclovir 1 g orally three times daily, famciclovir 500 mg orally three times daily. For individuals unable to endure oral therapy: Acyclovir 5 mg/kg intravenously every 8 hours for 7 to 14 days, succeeded by an oral antiviral for a minimum of 1 further week.
Prophylactic therapy with acyclovir at a dosage of 200–400 mg orally per day or 5 mg/kg intravenously twice day may be warranted in cases with elevated risk for HSV reactivation.
CMV esophagitis is managed with ganciclovir at a dosage of 5 mg/kg intravenously twice day for a minimum duration of 2 weeks.
Maintenance therapy with valganciclovir 900 mg orally daily may be required to prevent recurrence of CMV esophagitis in individuals with significant immunocompromise.
To avert CMV infection, CMV seronegative transplant recipients from seropositive donors should undergo antiviral prophylaxis.
Idiopathic (aphthous) esophageal ulcers in HIV infection are managed with prednisone or thalidomide.
Second Line
• For fluconazole-refractory Candida esophagitis: Micafungin 150 mg daily, caspofungin 50 mg daily, anidulafungin 200 mg daily, or deoxycholate
Amphotericin B 0.3–0.7 mg/kg per day (B-II).
• Echinocandins correlate with elevated relapse rates in comparison to fluconazole. • For ganciclovir-resistant HSV or CMV esophagitis: Foscarnet.
INPATIENT CONSIDERATIONS
Criteria for Admission
Outpatient care is suitable unless the patient's immune state is significantly weakened or the infection is exceedingly severe. In such instances, hospitalization may be required.
Intravenous Fluids
Should the patient endure significant odynophagia or if esophagitis is coupled with oral lesions that hinder chewing or swallowing, the provision of intravenous fluids may be requisite.
CONTINUING MANAGEMENT POST-TREATMENT SUGGESTIONS
The anticipated course and prognosis are contingent upon the underlying disease and pathogen; in cases of severe immunosuppression, extended therapy with efficacious drugs is required.
• Patients diagnosed with infectious esophagitis should schedule a follow-up appointment two weeks post-symptom resolution. • The majority of patients with Candida esophagitis typically experience symptom clearance within seven days of initiating treatment.
Myelosuppression is the primary adverse effect of ganciclovir therapy. The simultaneous use of zidovudine may exacerbate myelosuppression.
COMPLICATIONS
• Complications are rare. Severe local consequences may arise from deep esophageal ulcers, including massive hemorrhage.
– Esophageal perforation – Esophagobronchial or esophagomediastinal fistulas

- Published on
Infectious Disease - Erythema Nodosum
ERYTHEMA NODOSUM
FUNDAMENTALS OVERVIEW
Erythema nodosum is the most prevalent form of panniculitis. The clinical presentation includes inflammatory, painful, nodular lesions. The lesions are predominantly situated on the lower limbs.
EPIDEMIOLOGY
Incidence • The highest incidence is observed between the ages of 18 and 34 years. The annual incidence rate of biopsy-confirmed erythema nodosum in hospitalized patients aged 14 years and older was estimated at 52 occurrences per million individuals. • Predominantly observed in females.
Prevalence • 2.4 cases per 1,000 individuals annually. • Seasonal aggregation of sarcoidosis presenting with erythema nodosum has also been documented. Clustering peaked in August, September, and October.
RISK FACTORS: Genetics Particular human leukocyte antigens, HLA-B8 and HLA-DR3, were identified as correlated with the occurrence of erythema nodosum in sarcoidosis.
PATHOPHYSIOLOGY
Erythema nodosum can be classified as a type IV delayed hypersensitivity reaction to many antigens.
CAUSES
Multiple etiological variables have been linked to erythema nodosum: Bacterial infections: Streptococcal infections (Group A beta-hemolytic Streptococcus) are the most prevalent infectious etiologies of erythema nodosum, along with mycobacterial infections (Hansen's bacillus, tuberculosis), brucellosis, cat-scratch disease, and Yersinia enterocolitica. Syphilis, along with infections caused by Salmonella spp. (S. enteritidis and S. typhi), Mycoplasma spp., Chlamydia spp. (including C. psittaci, C. pneumoniae, and C. trachomatis), Neisseria meningitidis, N. gonorrhoeae, Francisella tularensis, and Rickettsiae spp., may also induce erythema nodosum. • Viral infections: Cytomegalovirus (CMV), Epstein-Barr virus (EBV), Human Immunodeficiency Virus (HIV), Hepatitis B virus (HBV), Herpes Simplex Virus (HSV) • Fungal infections: Coccidioidomycosis, aspergillosis, histoplasmosis • Protozoal infections: Amebiasis, toxoplasmosis, giardiasis • Pharmacological agents: Sulphonamides, sulfones, bromides, oral contraceptives • Malignancies: Hodgkin’s disease, non-Hodgkin’s lymphoma, leukemia, pancreatic carcinoma, colon adenocarcinoma • Other pathological conditions: Sarcoidosis, Adamantiades–Behcet’s disease, Crohn’s disease, ulcerative colitis, Sweet’s syndrome, lupus erythematosus, Sjögren’s syndrome • Gestation • Idiopathic (likely the predominant etiology)
DIAGNOSIS HISTORY
• Diligent medical history acquisition is critically significant. • Abrupt emergence of painful, erythematous nodules and elevated plaques typically found on the shins, ankles, and knees. • Erythema nodosum frequently presents with fever ranging from approximately 38–39°C, along with exhaustion and joint pain. • Generally self-resolving within several weeks.
PHYSICAL EXAM • Erythematous, sensitive red nodules and elevated plaques situated on the shins, ankles, knees, and infrequently on the extensor surfaces of the arms, neck, or face. Initially, the nodules exhibit a vivid red hue and are elevated; however, within a few days, they flatten and assume a livid red or purplish tint. Ultimately, they transition to a yellow or greenish hue and frequently resemble a pronounced bruise (“erythema contusiformis”). The nodules resolve without atrophy or scarring. Ulceration is never noticed.
DIAGNOSTIC TESTS AND INTERPRETATION LAB • Complete blood count • Erythrocyte sedimentation rate • Antistreptolysin O titer • Rapid antigen test for streptococcus • Polymerase chain reaction for streptococcal DNA detection • Throat culture • Urinalysis • Intradermal tuberculin test Chest radiograph (tuberculosis, bilateral hilar lymphadenopathy [Lofgren’s syndrome])
Diagnostic Procedures and Additional Methods
• Evaluate stool culture and parasite examination if abdominal pain, bloating, or diarrhea is present. • Conduct a punch biopsy of the skin. • Perform a transbronchial lung biopsy for histological confirmation of sarcoidosis. • Execute a biopsy of the gastrocnemius muscle, as myopathy is frequently observed in Lofgren’s syndrome. • Administer an interferon-γ release assay. • Consider colonoscopy to exclude inflammatory bowel disease. Pathological Observations The histopathologic hallmark is the presence of "Miescher's radial granulomas." It comprises discrete, distinct nodular clusters of histiocytes surrounding a central cleft. Additionally, infiltration of polymorphonuclear leukocytes is another histopathological observation.
DIFFERENTIAL DIAGNOSIS • Erythema induratum of Bazin: – Histopathological distinctions: Erythema induratum of Bazin mostly presents as lobular panniculitis, in contrast to erythema nodosum, which predominantly exhibits septal panniculitis. The nodules of erythema induratum of Bazin are primarily situated on the posterior aspect of the legs, exhibit greater persistence, and may also present with ulceration. • Dermatological manifestations of superficial thrombophlebitis: The lesions are predominantly situated on the lateral aspects of the legs and present as firm, irregular, fibrotic cords or plaques. The biopsy indicates minimal to no signs of inflammatory infiltration, suggesting a vasculitic rather than a panniculitic disease. • Lyme disease • Etiologies of panniculitis (e.g., systemic lupus erythematosus [SLE], acute pancreatitis)
TREATMENT MEDICATION
Initial Line Erythema nodosum is predominantly self-limiting, resolving in most individuals within several weeks. Treatment must be tailored to the underlying condition. • Symptomatic management may involve nonsteroidal anti-inflammatory medications (NSAIDs): Indomethacin 100–150 mg daily, naproxen 500 mg daily. Avoid NSAIDs if the etiology is inflammatory bowel illness. • Steroids may be administered in severe situations when infectious etiologies or malignancies have been excluded. • Prednisone administered at a dosage of 1 mg/kg, gradually reduced over many days. • Potassium iodide: The maximum dosage for adults is 300 mg administered three times daily. Nonetheless, significant secondary hyperthyroidism may arise. • Hydroxychloroquine (specifically for persistent erythema nodosum; 200 mg bi-daily). Colchicine (effective for erythema nodosum linked to Adamantiades–Behcet’s illness; 1–2 mg daily, administered in two doses). Erythema nodosum leprosum: Evidence exists supporting the efficacy of thalidomide and clofazimine. Furthermore, a markedly reduced incidence of mild side events was observed with a low-dose thalidomide regimen in comparison to a high-dose regimen . Second Line: Infliximab is indicated for erythema nodosum linked to inflammatory bowel illness.
SUPPLEMENTARY THERAPY
General Measures: • Bed rest • Consistent elevation • Compression
CONTINUING TREATMENT OUTLOOK • Most cases cure within 3 to 4 weeks. • Recurrence is infrequent, however more prevalent in idiopathic cases of erythema nodosum and in those associated with upper respiratory tract infections (either streptococcal or non-streptococcal).
COMPLICATIONS • Optic nerve neuritis has been documented in a patient during an acute episode of erythema nodosum.
ERYTHEMA NODOSUM
FUNDAMENTALS OVERVIEW
Erythema nodosum is the most prevalent form of panniculitis. The clinical presentation includes inflammatory, painful, nodular lesions. The lesions are predominantly situated on the lower limbs.
EPIDEMIOLOGY
Incidence • The highest incidence is observed between the ages of 18 and 34 years. The annual incidence rate of biopsy-confirmed erythema nodosum in hospitalized patients aged 14 years and older was estimated at 52 occurrences per million individuals. • Predominantly observed in females.
Prevalence • 2.4 cases per 1,000 individuals annually. • Seasonal aggregation of sarcoidosis presenting with erythema nodosum has also been documented. Clustering peaked in August, September, and October.
RISK FACTORS: Genetics Particular human leukocyte antigens, HLA-B8 and HLA-DR3, were identified as correlated with the occurrence of erythema nodosum in sarcoidosis.
PATHOPHYSIOLOGY
Erythema nodosum can be classified as a type IV delayed hypersensitivity reaction to many antigens.
CAUSES
Multiple etiological variables have been linked to erythema nodosum: Bacterial infections: Streptococcal infections (Group A beta-hemolytic Streptococcus) are the most prevalent infectious etiologies of erythema nodosum, along with mycobacterial infections (Hansen's bacillus, tuberculosis), brucellosis, cat-scratch disease, and Yersinia enterocolitica. Syphilis, along with infections caused by Salmonella spp. (S. enteritidis and S. typhi), Mycoplasma spp., Chlamydia spp. (including C. psittaci, C. pneumoniae, and C. trachomatis), Neisseria meningitidis, N. gonorrhoeae, Francisella tularensis, and Rickettsiae spp., may also induce erythema nodosum. • Viral infections: Cytomegalovirus (CMV), Epstein-Barr virus (EBV), Human Immunodeficiency Virus (HIV), Hepatitis B virus (HBV), Herpes Simplex Virus (HSV) • Fungal infections: Coccidioidomycosis, aspergillosis, histoplasmosis • Protozoal infections: Amebiasis, toxoplasmosis, giardiasis • Pharmacological agents: Sulphonamides, sulfones, bromides, oral contraceptives • Malignancies: Hodgkin’s disease, non-Hodgkin’s lymphoma, leukemia, pancreatic carcinoma, colon adenocarcinoma • Other pathological conditions: Sarcoidosis, Adamantiades–Behcet’s disease, Crohn’s disease, ulcerative colitis, Sweet’s syndrome, lupus erythematosus, Sjögren’s syndrome • Gestation • Idiopathic (likely the predominant etiology)
DIAGNOSIS HISTORY
• Diligent medical history acquisition is critically significant. • Abrupt emergence of painful, erythematous nodules and elevated plaques typically found on the shins, ankles, and knees. • Erythema nodosum frequently presents with fever ranging from approximately 38–39°C, along with exhaustion and joint pain. • Generally self-resolving within several weeks.
PHYSICAL EXAM • Erythematous, sensitive red nodules and elevated plaques situated on the shins, ankles, knees, and infrequently on the extensor surfaces of the arms, neck, or face. Initially, the nodules exhibit a vivid red hue and are elevated; however, within a few days, they flatten and assume a livid red or purplish tint. Ultimately, they transition to a yellow or greenish hue and frequently resemble a pronounced bruise (“erythema contusiformis”). The nodules resolve without atrophy or scarring. Ulceration is never noticed.
DIAGNOSTIC TESTS AND INTERPRETATION LAB • Complete blood count • Erythrocyte sedimentation rate • Antistreptolysin O titer • Rapid antigen test for streptococcus • Polymerase chain reaction for streptococcal DNA detection • Throat culture • Urinalysis • Intradermal tuberculin test Chest radiograph (tuberculosis, bilateral hilar lymphadenopathy [Lofgren’s syndrome])
Diagnostic Procedures and Additional Methods
• Evaluate stool culture and parasite examination if abdominal pain, bloating, or diarrhea is present. • Conduct a punch biopsy of the skin. • Perform a transbronchial lung biopsy for histological confirmation of sarcoidosis. • Execute a biopsy of the gastrocnemius muscle, as myopathy is frequently observed in Lofgren’s syndrome. • Administer an interferon-γ release assay. • Consider colonoscopy to exclude inflammatory bowel disease. Pathological Observations The histopathologic hallmark is the presence of "Miescher's radial granulomas." It comprises discrete, distinct nodular clusters of histiocytes surrounding a central cleft. Additionally, infiltration of polymorphonuclear leukocytes is another histopathological observation.
DIFFERENTIAL DIAGNOSIS • Erythema induratum of Bazin: – Histopathological distinctions: Erythema induratum of Bazin mostly presents as lobular panniculitis, in contrast to erythema nodosum, which predominantly exhibits septal panniculitis. The nodules of erythema induratum of Bazin are primarily situated on the posterior aspect of the legs, exhibit greater persistence, and may also present with ulceration. • Dermatological manifestations of superficial thrombophlebitis: The lesions are predominantly situated on the lateral aspects of the legs and present as firm, irregular, fibrotic cords or plaques. The biopsy indicates minimal to no signs of inflammatory infiltration, suggesting a vasculitic rather than a panniculitic disease. • Lyme disease • Etiologies of panniculitis (e.g., systemic lupus erythematosus [SLE], acute pancreatitis)
TREATMENT MEDICATION
Initial Line Erythema nodosum is predominantly self-limiting, resolving in most individuals within several weeks. Treatment must be tailored to the underlying condition. • Symptomatic management may involve nonsteroidal anti-inflammatory medications (NSAIDs): Indomethacin 100–150 mg daily, naproxen 500 mg daily. Avoid NSAIDs if the etiology is inflammatory bowel illness. • Steroids may be administered in severe situations when infectious etiologies or malignancies have been excluded. • Prednisone administered at a dosage of 1 mg/kg, gradually reduced over many days. • Potassium iodide: The maximum dosage for adults is 300 mg administered three times daily. Nonetheless, significant secondary hyperthyroidism may arise. • Hydroxychloroquine (specifically for persistent erythema nodosum; 200 mg bi-daily). Colchicine (effective for erythema nodosum linked to Adamantiades–Behcet’s illness; 1–2 mg daily, administered in two doses). Erythema nodosum leprosum: Evidence exists supporting the efficacy of thalidomide and clofazimine. Furthermore, a markedly reduced incidence of mild side events was observed with a low-dose thalidomide regimen in comparison to a high-dose regimen . Second Line: Infliximab is indicated for erythema nodosum linked to inflammatory bowel illness.
SUPPLEMENTARY THERAPY
General Measures: • Bed rest • Consistent elevation • Compression
CONTINUING TREATMENT OUTLOOK • Most cases cure within 3 to 4 weeks. • Recurrence is infrequent, however more prevalent in idiopathic cases of erythema nodosum and in those associated with upper respiratory tract infections (either streptococcal or non-streptococcal).
COMPLICATIONS • Optic nerve neuritis has been documented in a patient during an acute episode of erythema nodosum.


- Published on
Infectious Disease - Epiglottitis
DESCRIPTION
Accelerated infection of the epiglottis and surrounding supraglottic tissues.
Epidemiology
Occurrence
The incidence has significantly declined in nations with extensive vaccination against Haemophilus influenzae type b (1)[A].
• Incidence ranges from 0.9 to 3.1 per 100,000 individuals in the general population. • The average age of a patient with epiglottitis is 44.9 years.
FACTORS OF RISK
• Age below 4 years
The mean age of pediatric patients in the immunization era has roughly doubled to 11.6 years. • Children who are unvaccinated
• Immunodeficiency • Post-splenectomy • Non-immune adults!
GENERAL PREVENTION • Vaccination for H. influenzae type b (1)[A].
In cases of H. influenzae epiglottitis, if the patient has household contacts that include an unvaccinated child under the age of 4, it is advisable to administer rifampin prophylaxis at a dosage of 20 mg/kg/d (maximum 600 mg/d) orally once daily for 4 days to all household members and the patient to eliminate H. influenzae carriage. ETIOLOGY • Haemophilus influenzae type b accounts for the predominant majority of pediatric cases (exceeding 90%) and is commonly isolated from the bloodstream. In adult patients, blood cultures yield positive results in around 25% of instances.
• Additional pathogens identified in the pharynx of adults with epiglottitis comprise the following:
– Haemophilus parainfluenzae – Streptococcus pneumoniae – Group A Streptococcus – Staphylococcus aureus
In immunosuppressed patients, additional infections, including Candida spp. and Aspergillus spp., may be responsible.
Viral infections, including varicella zoster, infectious mononucleosis, HIV, and herpes simplex, may lead to complications such as epiglottitis.
DIAGNOSTIC HISTORY
• The onset of symptoms is typically acute.
• Young children typically exhibit symptoms such as fever, dysphonia, dysphagia, and irritability within 24 hours after beginning.
• Fever may be absent in adults.
PHYSICAL EXAMINATION
• Respiratory distress, inspiratory stridor, and a muffled voice resembling that of having hot food in the mouth may manifest.
• As many as one-third of pediatric patients present in shock, exhibiting cyanosis and loss of consciousness upon admission.
The patient prefers to sit in a forward-leaning position with the upper limbs extended.
• Oral secretions often result in drooling.
The direct inspection of a child's pharynx with a tongue blade should be avoided due to the risk of laryngospasm and total airway obstruction.
• Adolescents and adults may exhibit a less severe manifestation.
The most notable symptom is a sore throat, absent any indications of pharyngitis.
Neck discomfort and sensitivity over the hyoid bone in adult patients may indicate the diagnosis. DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• It is imperative that upon suspicion of epiglottitis in a juvenile child, diagnostic testing is conducted only after ensuring airway security.
• Moderate leukocytosis accompanied by a left shift. • Positive cultures of blood and epiglottis.
Imaging
A lateral neck radiograph may reveal an inflated epiglottis (the thumb sign), hypopharyngeal ballooning, and intact subglottic structures.
Radiography should only be conducted in the presence of physicians capable of managing acute airway blockage.
Ultrasound has been infrequently employed in emergency departments to visualize the enlarged epiglottis in adult patients.
A chest X-ray may reveal pneumonia or atelectasis in as many as 50% of instances.
Diagnostic Procedures and Additional Methods
• The patient must be sent to an operating room for epiglottic visualization with a fiberoptic laryngoscope following all preparations for prompt airway management. • The diagnosis is confirmed by observing an edematous, "cherry-red" epiglottis.
Histopathological Observations
Epiglottic edema and leukocytic infiltration. An abscess may be present.
DIFFERENTIAL DIAGNOSIS
• Croup syndrome – Typically has a more gradual onset.
– Is often preceded by an upper respiratory tract infection. – Primarily affects younger children (ages 3 months to 3 years). - Exhibits a viral etiology.
– Children with croup do not exhibit significant drooling or dysphagia and are more inclined to assume a supine position.
• Diphtheria – A pseudomembrane is observable in the pharynx. The smear and culture of the membrane reveal characteristic gram-positive bacilli.
• Allergic laryngeal edema – Patients typically present with minimal toxicity and absence of fever.
• Aspiration of foreign bodies • Lingual tonsillitis • Peritonsillar abscess, retropharyngeal abscess
INITIAL THERAPY MEDICATION
Acute epiglottitis is a medical emergency due to the potential for rapid airway blockage.
• It is inadvisable to observe children with epiglottitis without intubation, as mortality rates may surpass 25% with a careful waiting strategy.
An uncuffed endotracheal or nasotracheal tube should be implanted, and the kid must be monitored in an intensive care unit.
Tracheostomy, or needle cricothyrotomy as a temporary solution, should be executed if an unobstructed airway cannot be preserved by other means. In adult patients, a less aggressive treatment strategy is occasionally used, involving intubation in select cases only. Adhering to this strategy necessitates acknowledging that respiratory distress, stridor, a muffled voice, or laryngoscopic findings indicating less than 50% visibility of the vocal cords are factors linked to the requirement for airway management.
• Intravenous antibiotic treatment targeting H. influenzae should be administered.
Cefotaxime 100–200 mg/kg/day in four split doses (maximum adult daily dosage: 12 g)
Ceftriaxone 50–100 mg/kg/day administered in one or two split doses (maximum adult daily dosage: 2 g)
Ampicillin/sulbactam 200–300 mg/kg/day (of ampicillin) in 4 split doses (maximum adult daily dose: 12 g)
The therapeutic duration is 10 days.
Second Line
The usage of chloramphenicol (50–100 mg/kg/d in 4 split doses) alongside ampicillin has significantly declined due to the risk of toxicity.
SUPPLEMENTARY THERAPY
Supplementary Treatments
No controlled data exist to substantiate the use of corticosteroids or epinephrine in the management of acute epiglottitis.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Tracheostomy, when intubation is unfeasible.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
Maintaining airway patency is the foremost objective.
Criteria for Admission
All individuals diagnosed with epiglottitis should be hospitalized.
Intravenous Fluids
Often required. Do not attempt to establish intravenous access in a child prior to securing the airway.
Nursing
Avoid inducing anxiety in the child.
CONTINUOUS CARE POST-TREATMENT RECOMMENDATIONS
• Patients with epiglottitis typically exhibit quick improvement, specifically within 12–48 hours following the initiation of suitable antibiotic therapy. • Patients may be extubated once they are afebrile, alert, clinically improved, and demonstrate laryngoscopic evidence of edema reduction.
Patient Surveillance
In the adult patient who opts against intubation, ICU surveillance is essential.
PROGNOSIS • Relies on the timely securing of the airway. Hypoxia caused by airway obstruction is the primary factor influencing prognosis.
• The mortality rate in the US is recorded at 0.89%. • Recurrence is exceedingly rare but may occur.
COMPLICATIONS
• Total airway blockage leading to hypoxia/anoxia in multiple organs (anoxemic encephalopathy is the most serious consequence).
H. influenzae bacteremia is infrequently linked to metastatic illnesses, including meningitis and arthritis.
Iatrogenic consequences, primarily linked to intubation.
– Aspiration – Dislodgment of endotracheal tube – Tracheal erosion –
Pneumomediastinum – Pneumothorax – Pulmonary edema
DESCRIPTION
Accelerated infection of the epiglottis and surrounding supraglottic tissues.
Epidemiology
Occurrence
The incidence has significantly declined in nations with extensive vaccination against Haemophilus influenzae type b (1)[A].
• Incidence ranges from 0.9 to 3.1 per 100,000 individuals in the general population. • The average age of a patient with epiglottitis is 44.9 years.
FACTORS OF RISK
• Age below 4 years
The mean age of pediatric patients in the immunization era has roughly doubled to 11.6 years. • Children who are unvaccinated
• Immunodeficiency • Post-splenectomy • Non-immune adults!
GENERAL PREVENTION • Vaccination for H. influenzae type b (1)[A].
In cases of H. influenzae epiglottitis, if the patient has household contacts that include an unvaccinated child under the age of 4, it is advisable to administer rifampin prophylaxis at a dosage of 20 mg/kg/d (maximum 600 mg/d) orally once daily for 4 days to all household members and the patient to eliminate H. influenzae carriage. ETIOLOGY • Haemophilus influenzae type b accounts for the predominant majority of pediatric cases (exceeding 90%) and is commonly isolated from the bloodstream. In adult patients, blood cultures yield positive results in around 25% of instances.
• Additional pathogens identified in the pharynx of adults with epiglottitis comprise the following:
– Haemophilus parainfluenzae – Streptococcus pneumoniae – Group A Streptococcus – Staphylococcus aureus
In immunosuppressed patients, additional infections, including Candida spp. and Aspergillus spp., may be responsible.
Viral infections, including varicella zoster, infectious mononucleosis, HIV, and herpes simplex, may lead to complications such as epiglottitis.
DIAGNOSTIC HISTORY
• The onset of symptoms is typically acute.
• Young children typically exhibit symptoms such as fever, dysphonia, dysphagia, and irritability within 24 hours after beginning.
• Fever may be absent in adults.
PHYSICAL EXAMINATION
• Respiratory distress, inspiratory stridor, and a muffled voice resembling that of having hot food in the mouth may manifest.
• As many as one-third of pediatric patients present in shock, exhibiting cyanosis and loss of consciousness upon admission.
The patient prefers to sit in a forward-leaning position with the upper limbs extended.
• Oral secretions often result in drooling.
The direct inspection of a child's pharynx with a tongue blade should be avoided due to the risk of laryngospasm and total airway obstruction.
• Adolescents and adults may exhibit a less severe manifestation.
The most notable symptom is a sore throat, absent any indications of pharyngitis.
Neck discomfort and sensitivity over the hyoid bone in adult patients may indicate the diagnosis. DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• It is imperative that upon suspicion of epiglottitis in a juvenile child, diagnostic testing is conducted only after ensuring airway security.
• Moderate leukocytosis accompanied by a left shift. • Positive cultures of blood and epiglottis.
Imaging
A lateral neck radiograph may reveal an inflated epiglottis (the thumb sign), hypopharyngeal ballooning, and intact subglottic structures.
Radiography should only be conducted in the presence of physicians capable of managing acute airway blockage.
Ultrasound has been infrequently employed in emergency departments to visualize the enlarged epiglottis in adult patients.
A chest X-ray may reveal pneumonia or atelectasis in as many as 50% of instances.
Diagnostic Procedures and Additional Methods
• The patient must be sent to an operating room for epiglottic visualization with a fiberoptic laryngoscope following all preparations for prompt airway management. • The diagnosis is confirmed by observing an edematous, "cherry-red" epiglottis.
Histopathological Observations
Epiglottic edema and leukocytic infiltration. An abscess may be present.
DIFFERENTIAL DIAGNOSIS
• Croup syndrome – Typically has a more gradual onset.
– Is often preceded by an upper respiratory tract infection. – Primarily affects younger children (ages 3 months to 3 years). - Exhibits a viral etiology.
– Children with croup do not exhibit significant drooling or dysphagia and are more inclined to assume a supine position.
• Diphtheria – A pseudomembrane is observable in the pharynx. The smear and culture of the membrane reveal characteristic gram-positive bacilli.
• Allergic laryngeal edema – Patients typically present with minimal toxicity and absence of fever.
• Aspiration of foreign bodies • Lingual tonsillitis • Peritonsillar abscess, retropharyngeal abscess
INITIAL THERAPY MEDICATION
Acute epiglottitis is a medical emergency due to the potential for rapid airway blockage.
• It is inadvisable to observe children with epiglottitis without intubation, as mortality rates may surpass 25% with a careful waiting strategy.
An uncuffed endotracheal or nasotracheal tube should be implanted, and the kid must be monitored in an intensive care unit.
Tracheostomy, or needle cricothyrotomy as a temporary solution, should be executed if an unobstructed airway cannot be preserved by other means. In adult patients, a less aggressive treatment strategy is occasionally used, involving intubation in select cases only. Adhering to this strategy necessitates acknowledging that respiratory distress, stridor, a muffled voice, or laryngoscopic findings indicating less than 50% visibility of the vocal cords are factors linked to the requirement for airway management.
• Intravenous antibiotic treatment targeting H. influenzae should be administered.
Cefotaxime 100–200 mg/kg/day in four split doses (maximum adult daily dosage: 12 g)
Ceftriaxone 50–100 mg/kg/day administered in one or two split doses (maximum adult daily dosage: 2 g)
Ampicillin/sulbactam 200–300 mg/kg/day (of ampicillin) in 4 split doses (maximum adult daily dose: 12 g)
The therapeutic duration is 10 days.
Second Line
The usage of chloramphenicol (50–100 mg/kg/d in 4 split doses) alongside ampicillin has significantly declined due to the risk of toxicity.
SUPPLEMENTARY THERAPY
Supplementary Treatments
No controlled data exist to substantiate the use of corticosteroids or epinephrine in the management of acute epiglottitis.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Tracheostomy, when intubation is unfeasible.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
Maintaining airway patency is the foremost objective.
Criteria for Admission
All individuals diagnosed with epiglottitis should be hospitalized.
Intravenous Fluids
Often required. Do not attempt to establish intravenous access in a child prior to securing the airway.
Nursing
Avoid inducing anxiety in the child.
CONTINUOUS CARE POST-TREATMENT RECOMMENDATIONS
• Patients with epiglottitis typically exhibit quick improvement, specifically within 12–48 hours following the initiation of suitable antibiotic therapy. • Patients may be extubated once they are afebrile, alert, clinically improved, and demonstrate laryngoscopic evidence of edema reduction.
Patient Surveillance
In the adult patient who opts against intubation, ICU surveillance is essential.
PROGNOSIS • Relies on the timely securing of the airway. Hypoxia caused by airway obstruction is the primary factor influencing prognosis.
• The mortality rate in the US is recorded at 0.89%. • Recurrence is exceedingly rare but may occur.
COMPLICATIONS
• Total airway blockage leading to hypoxia/anoxia in multiple organs (anoxemic encephalopathy is the most serious consequence).
H. influenzae bacteremia is infrequently linked to metastatic illnesses, including meningitis and arthritis.
Iatrogenic consequences, primarily linked to intubation.
– Aspiration – Dislodgment of endotracheal tube – Tracheal erosion –
Pneumomediastinum – Pneumothorax – Pulmonary edema

- Published on
Infectious Disease - Epididymitis
BASICS DESCRIPTION: Epididymitis is an inflammatory response of the epididymis caused by a variety of infectious agents, as well as rare noninfectious disorders or local trauma. It can be either acute or chronic, with the latter being defined by symptoms that have persisted for three months or more.
The fifth most frequent urologic diagnosis in men between the ages of 18 and 50 is epididymitis )Patients between the ages of 20 and 39 make up the largest group (43%), followed by those between the ages of 40 and 59 (29%), (2).
• More man-hours are lost due to epididymitis than any other urologic condition in the US military
• A bimodal distribution was seen in an examination of 121 ambulatory patients with epididymitis, with men aged 16 to 30 having the highest prevalence.
between the ages of 51 and 70 l
• A rise in the number of homosexual males having unprotected anal sex.
Risk factors include: bacteriuria; sexual activity; strenuous physical activity; riding a bicycle or motorcycle; prolonged sitting (for example, while traveling or working at a sedentary job); patients older than 35 and those in prepuberty; recent urinary tract surgery or instrumentation; posterior urethral valves or meatal stenosis (prepuberty); and prostate obstruction (elderly).
OVERALL PREVENTION
Avoiding sexual activity or maintaining a long-term, mutually monogamous relationship with a partner who has been tested and is known to be uninfected are two ways to prevent sexually transmitted diseases (STDs). When used properly and consistently, latex condoms can lower the risk of sexually transmitted diseases.
Pathophysiology
Pathogens may ascend retrogradely, and high voiding pressures may increase the risk of epididymitis by encouraging urethrovasal reflux. Proximal urethral strictures, anomalies of the bladder neck, and dyssynergia of the detrusor external sphincter induce voiding dysfunction in approximately half of the patients
Ethiology
• Infectious: Frequently occurring specific medical conditions
STDs: The leading cause of death for young men. Chlamydia trachomatis or Neisseria gonorrhoeae are common; their frequency peaks between the ages of 14 and 35 (6). Less frequent: Urealyticum (Ureaplasma)
Common bacteria linked to urinary tract infections include Pseudomonas aeruginosa, Proteus species, Klebsiella pneumoniae, and Escherichia coli. Uncommon: Streptococci, Staphylococci, and Salmonella spp. are nonspecific and rare clinical diseases. Bacterial: Brucella species, Nocardia species, and Mycobacterium tuberculosis. There have been numerous documented iatrogenic cases of epididymitis following Calmette-Guérin bacillus therapy for bladder transitional cell cancer.
Candida species, Histoplasma capsule, and Blastomyces dermatitidis are examples of fungi.
Schistosoma haematobium and Wuchereria are parasites.
Bancrofti
• Noninfectious Vasculitides: Henoch-Schönlein purpura, Polyarteritis nodosa, and Behcet's disease Substances: Trauma from Amiodarone
• COMMONLY ASSOCIATED Idiopathic Conditions
Orchitis
History of Diagnosis
• Scrotal pain and swelling that develops gradually over a few days, rather than hours as with testicular torsion.
Typically, it is unilateral.
• The lower abdomen is occasionally affected by pain that originates posterior to the testis.
• Although pain is usually unilateral, it may radiate to the nearby testis.
• There may be signs of a lower urinary tract infection, including fever, urgency, frequency, hematuria, and dysuria.
• Fever and chills: up to 71% of children but 25% of adults experience these symptoms.
• One crucial indicator that epididymitis is brought on by sexually transmitted diseases is preceding urethral discharge.
• Patients with chronic epididymitis have experienced continuous or sporadic pain for more than six weeks.
MEDICAL EXAMINATION
• When the urethra is examined or stripped, urethral discharge may be visible.
• Localized discomfort in the epididyma that develops into swelling and tenderness in the testicles.
• Normal cremasteric reflex (unilateral testis elevation caused by ipsilateral cremasteric muscle contraction).
• Testicular elevation (Prehn's sign) relieves pain.
• Reactive hydrocele and scrotal wall erythema may develop; the scrotum is typically not enlarged.
Tests for Diagnosis and Interpretation
Lab
First laboratory testing
• Urethritis can be identified by Gram stain and swabbed urethral discharge culture. Don't empty your bladder for less than two hours after urethral testing.
• Patients should also be checked for other sexually transmitted diseases if urethritis is discovered.
• Urinalysis and urine culture, ideally on urine samples taken at the initial void.
• Leukocyte esterase and white blood cells are helpful in distinguishing testicular torsion from C-reactive protein levels and erythrocyte sedimentation rate.
suggests that you have urethritis.
• urethral swabs or urine samples should be used for polymerase chain reaction (PCR) tests for C. trachomatis and N. gonorrhoeae.
• When urosepsis and epididymitis are linked, blood culture may be used as a diagnostic tool.
Follow-up and Particular Points to Remember
• For all surgically removed tissue specimens, cultures, histopathologic analysis, and PCR assays (if available) should be carried out.
Blood cultures and serologic testing are used to diagnose brucellar epididymitis.
Imaging First Step
Specifically, to rule out testicular torsion, use color Doppler ultrasonography. Epididymitis is suggested by an elevated Doppler wave pulsation, which indicates higher blood flow.
Follow-up and Particular Points to Remember
Chest X-rays and suitable urine cultures should be carried out if tuberculosis is suspected. If there are any scrotal draining sinuses, they should also be cultured.
DIFFERENTIAL DIAGNOSIS • Torsion of the testicles • Neoplasms (infrequently)
FIRST LINE TREATMENT MEDICATION
• The majority of people with bacterial epididymitis can be treated medically.
• Before laboratory testing is finished, empirical treatment for epididymitis should be started based on probable pathogens.
• Nonsteroidal anti-inflammatory medicines (NSAIDs) may be beneficial, and bed rest, scrotal elevation and support, and analgesics are advised (7).
• Age, sexual history, recent instrumentation or catheterization, and local knowledge of antibiotic sensitivities of the main sexual and urinary infections should all be taken into consideration when choosing empirical antibiotics.
• The empirical treatment for sexually transmitted epididymitis involves treating N. gonorrhoeae and C. trachomatis infections with a 250 mg intramuscular dose of ceftriaxone and 100 mg twice day for 10 days of oral doxycycline. Doxycycline can be substituted by a single 1 g dose of azithromycin, which
might increase adherence. Ofloxacin 300 mg taken twice daily for 10 days or levofloxacin 500 mg taken once daily for 10 days may also be administered to patients with acute epididymitis most likely brought on by enteric organisms or to those who are hypersensitive to cephalosporins and/or tetracyclines (6).
• Fluoroquinolones (ofloxacin 300 mg orally twice a day for 10 days, levofloxacin 500 mg orally once daily for 10 days, or ciprofloxacin 500 mg twice daily for 10 days) were found to be efficacious in treating acute epididymitis that was most likely caused by urinary pathogens (6).
ALERT HIV Infection: Follow the same guidelines as people without HIV. However, these people are more likely to have mycobacteria and fungi.
OTHER PROCEDURES AND SURGERY
In order to treat acute epididymal infection consequences including testicular infarction, abscess, or scrotal pyocele, surgery may be required.
Considering the patient
Requirements for Admission
Initial intravenous therapy is recommended for severe infections with systemic disruption or characteristics that suggest bacteremia.
Ongoing Care Patient Education: Patients with N. gonorrhoeae or C. trachomatis-induced acute epididymitis should be advised to refer sex partners for assessment and treatment if they had contact with the index patient within 60 days of the patient's symptoms starting.
• Patients should be told not to have sex until they and their partners are healed, meaning that they are both symptom-free once therapy is finished.
Bacteremia, testicular infarction, scrotal abscess, pyocele, chronic draining scrotal sinus, chronic epididymitis, infertility, and pediatric considerations are among the complications.
When it comes to testicular torsion, differential diagnosis is especially crucial.
• In a Canadian children's hospital, epididymitis was identified in only 15% of 113 consecutive occurrences of scrotal discomfort (8).
• Most of the time, no specific etiology is identified.
BASICS DESCRIPTION: Epididymitis is an inflammatory response of the epididymis caused by a variety of infectious agents, as well as rare noninfectious disorders or local trauma. It can be either acute or chronic, with the latter being defined by symptoms that have persisted for three months or more.
The fifth most frequent urologic diagnosis in men between the ages of 18 and 50 is epididymitis )Patients between the ages of 20 and 39 make up the largest group (43%), followed by those between the ages of 40 and 59 (29%), (2).
• More man-hours are lost due to epididymitis than any other urologic condition in the US military
• A bimodal distribution was seen in an examination of 121 ambulatory patients with epididymitis, with men aged 16 to 30 having the highest prevalence.
between the ages of 51 and 70 l
• A rise in the number of homosexual males having unprotected anal sex.
Risk factors include: bacteriuria; sexual activity; strenuous physical activity; riding a bicycle or motorcycle; prolonged sitting (for example, while traveling or working at a sedentary job); patients older than 35 and those in prepuberty; recent urinary tract surgery or instrumentation; posterior urethral valves or meatal stenosis (prepuberty); and prostate obstruction (elderly).
OVERALL PREVENTION
Avoiding sexual activity or maintaining a long-term, mutually monogamous relationship with a partner who has been tested and is known to be uninfected are two ways to prevent sexually transmitted diseases (STDs). When used properly and consistently, latex condoms can lower the risk of sexually transmitted diseases.
Pathophysiology
Pathogens may ascend retrogradely, and high voiding pressures may increase the risk of epididymitis by encouraging urethrovasal reflux. Proximal urethral strictures, anomalies of the bladder neck, and dyssynergia of the detrusor external sphincter induce voiding dysfunction in approximately half of the patients
Ethiology
• Infectious: Frequently occurring specific medical conditions
STDs: The leading cause of death for young men. Chlamydia trachomatis or Neisseria gonorrhoeae are common; their frequency peaks between the ages of 14 and 35 (6). Less frequent: Urealyticum (Ureaplasma)
Common bacteria linked to urinary tract infections include Pseudomonas aeruginosa, Proteus species, Klebsiella pneumoniae, and Escherichia coli. Uncommon: Streptococci, Staphylococci, and Salmonella spp. are nonspecific and rare clinical diseases. Bacterial: Brucella species, Nocardia species, and Mycobacterium tuberculosis. There have been numerous documented iatrogenic cases of epididymitis following Calmette-Guérin bacillus therapy for bladder transitional cell cancer.
Candida species, Histoplasma capsule, and Blastomyces dermatitidis are examples of fungi.
Schistosoma haematobium and Wuchereria are parasites.
Bancrofti
• Noninfectious Vasculitides: Henoch-Schönlein purpura, Polyarteritis nodosa, and Behcet's disease Substances: Trauma from Amiodarone
• COMMONLY ASSOCIATED Idiopathic Conditions
Orchitis
History of Diagnosis
• Scrotal pain and swelling that develops gradually over a few days, rather than hours as with testicular torsion.
Typically, it is unilateral.
• The lower abdomen is occasionally affected by pain that originates posterior to the testis.
• Although pain is usually unilateral, it may radiate to the nearby testis.
• There may be signs of a lower urinary tract infection, including fever, urgency, frequency, hematuria, and dysuria.
• Fever and chills: up to 71% of children but 25% of adults experience these symptoms.
• One crucial indicator that epididymitis is brought on by sexually transmitted diseases is preceding urethral discharge.
• Patients with chronic epididymitis have experienced continuous or sporadic pain for more than six weeks.
MEDICAL EXAMINATION
• When the urethra is examined or stripped, urethral discharge may be visible.
• Localized discomfort in the epididyma that develops into swelling and tenderness in the testicles.
• Normal cremasteric reflex (unilateral testis elevation caused by ipsilateral cremasteric muscle contraction).
• Testicular elevation (Prehn's sign) relieves pain.
• Reactive hydrocele and scrotal wall erythema may develop; the scrotum is typically not enlarged.
Tests for Diagnosis and Interpretation
Lab
First laboratory testing
• Urethritis can be identified by Gram stain and swabbed urethral discharge culture. Don't empty your bladder for less than two hours after urethral testing.
• Patients should also be checked for other sexually transmitted diseases if urethritis is discovered.
• Urinalysis and urine culture, ideally on urine samples taken at the initial void.
• Leukocyte esterase and white blood cells are helpful in distinguishing testicular torsion from C-reactive protein levels and erythrocyte sedimentation rate.
suggests that you have urethritis.
• urethral swabs or urine samples should be used for polymerase chain reaction (PCR) tests for C. trachomatis and N. gonorrhoeae.
• When urosepsis and epididymitis are linked, blood culture may be used as a diagnostic tool.
Follow-up and Particular Points to Remember
• For all surgically removed tissue specimens, cultures, histopathologic analysis, and PCR assays (if available) should be carried out.
Blood cultures and serologic testing are used to diagnose brucellar epididymitis.
Imaging First Step
Specifically, to rule out testicular torsion, use color Doppler ultrasonography. Epididymitis is suggested by an elevated Doppler wave pulsation, which indicates higher blood flow.
Follow-up and Particular Points to Remember
Chest X-rays and suitable urine cultures should be carried out if tuberculosis is suspected. If there are any scrotal draining sinuses, they should also be cultured.
DIFFERENTIAL DIAGNOSIS • Torsion of the testicles • Neoplasms (infrequently)
FIRST LINE TREATMENT MEDICATION
• The majority of people with bacterial epididymitis can be treated medically.
• Before laboratory testing is finished, empirical treatment for epididymitis should be started based on probable pathogens.
• Nonsteroidal anti-inflammatory medicines (NSAIDs) may be beneficial, and bed rest, scrotal elevation and support, and analgesics are advised (7).
• Age, sexual history, recent instrumentation or catheterization, and local knowledge of antibiotic sensitivities of the main sexual and urinary infections should all be taken into consideration when choosing empirical antibiotics.
• The empirical treatment for sexually transmitted epididymitis involves treating N. gonorrhoeae and C. trachomatis infections with a 250 mg intramuscular dose of ceftriaxone and 100 mg twice day for 10 days of oral doxycycline. Doxycycline can be substituted by a single 1 g dose of azithromycin, which
might increase adherence. Ofloxacin 300 mg taken twice daily for 10 days or levofloxacin 500 mg taken once daily for 10 days may also be administered to patients with acute epididymitis most likely brought on by enteric organisms or to those who are hypersensitive to cephalosporins and/or tetracyclines (6).
• Fluoroquinolones (ofloxacin 300 mg orally twice a day for 10 days, levofloxacin 500 mg orally once daily for 10 days, or ciprofloxacin 500 mg twice daily for 10 days) were found to be efficacious in treating acute epididymitis that was most likely caused by urinary pathogens (6).
ALERT HIV Infection: Follow the same guidelines as people without HIV. However, these people are more likely to have mycobacteria and fungi.
OTHER PROCEDURES AND SURGERY
In order to treat acute epididymal infection consequences including testicular infarction, abscess, or scrotal pyocele, surgery may be required.
Considering the patient
Requirements for Admission
Initial intravenous therapy is recommended for severe infections with systemic disruption or characteristics that suggest bacteremia.
Ongoing Care Patient Education: Patients with N. gonorrhoeae or C. trachomatis-induced acute epididymitis should be advised to refer sex partners for assessment and treatment if they had contact with the index patient within 60 days of the patient's symptoms starting.
• Patients should be told not to have sex until they and their partners are healed, meaning that they are both symptom-free once therapy is finished.
Bacteremia, testicular infarction, scrotal abscess, pyocele, chronic draining scrotal sinus, chronic epididymitis, infertility, and pediatric considerations are among the complications.
When it comes to testicular torsion, differential diagnosis is especially crucial.
• In a Canadian children's hospital, epididymitis was identified in only 15% of 113 consecutive occurrences of scrotal discomfort (8).
• Most of the time, no specific etiology is identified.

- Published on
Infectious Disease – Bornholm Disease
Epidemic pleurodynia (Bornholm disease)
FUNDAMENTAL DESCRIPTION Epidemic pleurodynia is an acute, febrile illness marked by the sudden onset of thoracic or abdominal pain and spasms. It is sometimes referred to as epidemic myalgia, Bornholm illness (called after the Danish island of Bornholm), or devil's grasp. Epidemiology (3) Occurrence • Typically manifests in little or major epidemics, with several family members exhibiting symptoms. • Symptoms in other family members may commence simultaneously or sequentially, with intervals of several days between occurrences. Enteroviral infections, including coxsackievirus families A and B, echoviruses, and the recently identified numbered enteroviruses, are prevalent, particularly during late summer and early autumn. • The peak prevalence of enteroviral infection correlates with the football and soccer seasons, resulting in It has been posited that intimate proximity, whether on the playing field or in the locker room, promotes person-to-person transmission. Another argument is that water and ubiquitous vessels become contaminated via direct oral contact with infected individuals, thereby acting as a source of the infection. • Vigorous physical activity during the incubation phase may lead to exacerbated clinical infection, rendering illness in athletes more conspicuous. • Pediatric cases have less severe disease compared to adults. • Infections can manifest in neonates (1).
COMPREHENSIVE PREVENTION
• Recommended specific control methods to prevent outbreaks include the following: Avoid oral contact. – Utilization of disposable cups or personal drinking vessels – Employment of ice packs instead of ice cubes from a communal ice chest for injuries - Delivery of education and information for kids, school nurses, and coaching personnel
PATHOPHYSIOLOGY
Likely arises from direct viral infiltration of the thoracic and abdominal musculature.
ETIOLOGY
• As indicated by its nomenclature, the disease frequently manifests in localized epidemics, predominantly attributed to coxsackievirus B. • Additional viruses, including echoviruses 1, 6, 9, 16, and 19, as well as group A coxsackieviruses 4, 6, 9, and 10, have been correlated with the condition.DIAGNOSTIC HISTORY • Typically presents without a prodrome, commencing with the sudden onset of fever and spasms of pleuritic chest or upper abdomen discomfort. Fever typically ranges from 38.0 to 39.5°C, peaks within one hour following the commencement of paroxysms, and diminishes with the resolution of discomfort, often accompanied by headaches. Chest pain occurs more frequently in adults, although stomach discomfort is more prevalent in youngsters. Paroxysms of intense, acute, stabbing rib pain typically endure for 15–30 minutes and are accompanied by diaphoresis and tachypnea. The affected muscles exhibit tenderness upon examination, and a pleural rub may be audible. Periumbilical pain and discomfort in the lower abdomen quadrants may manifest, particularly in pediatric populations. • Instances of pain confined to the cervical region and extremities have been documented. • The illness often endures for 4 to 6 days in the majority of instances
PHYSICAL EXAMINATION
• Pain is often provoked by pressure on the affected muscles. • Muscle swelling may be observed or palpated in certain instances.
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
The leukocyte count is often within the normal range
Virologic diagnosis can be established by isolating group B coxsackievirus from throat washings or feces, or by demonstrating an elevation in antibody titers. Chest radiographs appear normal; nevertheless, minor pleural effusions may occasionally be present.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis encompasses pneumonia, pulmonary infarction, myocardial ischemia, pulmonary embolism, herpes zoster, and any etiology of acute abdominal pain, especially acute appendicitis or renal colic
THERAPEUTIC PHARMACEUTICAL
Initial Line The administration of nonsteroidal anti-inflammatory drugs and the application of heat to the afflicted muscles have proven effective. • Opiate analgesics are prescribed for severe situations. SUPPLEMENTARY THERAPY Comprehensive Strategies Application of thermal energy to the impacted musculature
CONTINUING TREATMENT POST-CARE SUGGESTIONS
According to clinical findings and symptom recurrence PROGNOSIS The illness typically endures for 4 to 7 days and is seldom lethal. • Relapses may transpire.
COMPLICATIONS
Symptoms often resolve after a few days (mostly 4–6 days; range, 12 hours to 3 weeks), and recurrences are infrequent. Aseptic meningitis and orchitis may manifest in fewer than 10% of cases, whereas pericarditis and pneumonia are extremely rarer.
Epidemic pleurodynia (Bornholm disease)
FUNDAMENTAL DESCRIPTION Epidemic pleurodynia is an acute, febrile illness marked by the sudden onset of thoracic or abdominal pain and spasms. It is sometimes referred to as epidemic myalgia, Bornholm illness (called after the Danish island of Bornholm), or devil's grasp. Epidemiology (3) Occurrence • Typically manifests in little or major epidemics, with several family members exhibiting symptoms. • Symptoms in other family members may commence simultaneously or sequentially, with intervals of several days between occurrences. Enteroviral infections, including coxsackievirus families A and B, echoviruses, and the recently identified numbered enteroviruses, are prevalent, particularly during late summer and early autumn. • The peak prevalence of enteroviral infection correlates with the football and soccer seasons, resulting in It has been posited that intimate proximity, whether on the playing field or in the locker room, promotes person-to-person transmission. Another argument is that water and ubiquitous vessels become contaminated via direct oral contact with infected individuals, thereby acting as a source of the infection. • Vigorous physical activity during the incubation phase may lead to exacerbated clinical infection, rendering illness in athletes more conspicuous. • Pediatric cases have less severe disease compared to adults. • Infections can manifest in neonates (1).
COMPREHENSIVE PREVENTION
• Recommended specific control methods to prevent outbreaks include the following: Avoid oral contact. – Utilization of disposable cups or personal drinking vessels – Employment of ice packs instead of ice cubes from a communal ice chest for injuries - Delivery of education and information for kids, school nurses, and coaching personnel
PATHOPHYSIOLOGY
Likely arises from direct viral infiltration of the thoracic and abdominal musculature.
ETIOLOGY
• As indicated by its nomenclature, the disease frequently manifests in localized epidemics, predominantly attributed to coxsackievirus B. • Additional viruses, including echoviruses 1, 6, 9, 16, and 19, as well as group A coxsackieviruses 4, 6, 9, and 10, have been correlated with the condition.DIAGNOSTIC HISTORY • Typically presents without a prodrome, commencing with the sudden onset of fever and spasms of pleuritic chest or upper abdomen discomfort. Fever typically ranges from 38.0 to 39.5°C, peaks within one hour following the commencement of paroxysms, and diminishes with the resolution of discomfort, often accompanied by headaches. Chest pain occurs more frequently in adults, although stomach discomfort is more prevalent in youngsters. Paroxysms of intense, acute, stabbing rib pain typically endure for 15–30 minutes and are accompanied by diaphoresis and tachypnea. The affected muscles exhibit tenderness upon examination, and a pleural rub may be audible. Periumbilical pain and discomfort in the lower abdomen quadrants may manifest, particularly in pediatric populations. • Instances of pain confined to the cervical region and extremities have been documented. • The illness often endures for 4 to 6 days in the majority of instances
PHYSICAL EXAMINATION
• Pain is often provoked by pressure on the affected muscles. • Muscle swelling may be observed or palpated in certain instances.
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
The leukocyte count is often within the normal range
Virologic diagnosis can be established by isolating group B coxsackievirus from throat washings or feces, or by demonstrating an elevation in antibody titers. Chest radiographs appear normal; nevertheless, minor pleural effusions may occasionally be present.
DIFFERENTIAL DIAGNOSIS
The differential diagnosis encompasses pneumonia, pulmonary infarction, myocardial ischemia, pulmonary embolism, herpes zoster, and any etiology of acute abdominal pain, especially acute appendicitis or renal colic
THERAPEUTIC PHARMACEUTICAL
Initial Line The administration of nonsteroidal anti-inflammatory drugs and the application of heat to the afflicted muscles have proven effective. • Opiate analgesics are prescribed for severe situations. SUPPLEMENTARY THERAPY Comprehensive Strategies Application of thermal energy to the impacted musculature
CONTINUING TREATMENT POST-CARE SUGGESTIONS
According to clinical findings and symptom recurrence PROGNOSIS The illness typically endures for 4 to 7 days and is seldom lethal. • Relapses may transpire.
COMPLICATIONS
Symptoms often resolve after a few days (mostly 4–6 days; range, 12 hours to 3 weeks), and recurrences are infrequent. Aseptic meningitis and orchitis may manifest in fewer than 10% of cases, whereas pericarditis and pneumonia are extremely rarer.

- Published on
Infectious Disease : Endophthalmitis
ENDOPHTHALMITIS
BASIC DESCRIPTION: Endophthalmitis is an infectious condition that affects the ocular (vitreous) cavity, while panophthalmitis is an inflammation that affects every eye structure.
The incidence of epidemiology
While the incidence of endophthalmitis following penetrating ocular trauma is reported to be between 3 and 30% and is typically higher in situations with retained intraocular foreign bodies, the rate following cataract surgery is between 0.1% and 0.3%.
RISK FACTORS • The most common risk factors include untreated blepharitis, poor surgical technique, and intraoperative complications/extended operating time.
• significant risk factors for acute endophthalmitis following surgery.
Patients who are immunocompromised, diabetic, or chronically unwell are most at risk for endogenous endophthalmitis, which has been reported to occur in 1 in 5,000 to 10,000 hospitalizations, particularly those who have indwelling intravenous catheters and/or positive blood cultures.
OVERALL PREVENTION
• Despite the absence of data showing a decrease in the incidence of post-operative endophthalmitis, routine post-operative administration of topical fluoroquinolones is thought to be the standard of care following cataract surgery.
• It has recently been demonstrated that intracameral administration of cefuroxime reduces the incidence of post-operative endophthalmitis following cataract surgery (1).
• For penetrating ocular injuries with a high risk of infection, such as intraocular foreign bodies, several authorities advise systemic intravenous prophylaxis with vancomycin (1 g i.v. b.i.d.) or moxifloxacin (400 mg p.o. each day).
• For anterior segment trauma, such as corneal laceration, topical antibiotics that are fortified (vancomycin 25–50 mg/mL, cefazolin 50 mg/mL, and/or tobramycin 15 mg/mL) or topical fluoroquinolones, as well as subconjunctival injections at the conclusion of the surgical procedure, can generate therapeutic levels of
antibiotics in the anterior chamber. Patients with infection foci, particularly those suffering from Candida spp.-caused fungemia, should be closely watched for the onset of endogenous endophthalmitis.
Pathophysiology
• Post-operative endophthalmitis can result from improper wound creation following cataract surgery, which permits conjunctival and eyelid flora to enter the anterior chamber.
• In individuals with infectious processes elsewhere, bacteria can spread through the bloodstream and initially impact the choroid, resulting in endogenous endophthalmitis.
ETIOLOGY • The causes of infectious endophthalmitis might be parasitic, bacterial, or fungal. Acinetobacter species, Actinomyces israelii, Bacillus species, Clostridium species, Corynebacterium species, Escherichia coli, Haemophilus influenzae, Klebsiella species, Listeria monocytogenes, Neisseria meningitides, Proteus species, and Propionibacterium are among the most frequent causes, listed alphabetically.
Salmonella typhimurium, Pseudomonas aeruginosa, Serratia marcescens, Streptococcus species, Staphylococcus species, acnes
- Parasites (Taenia solium, Toxocara canis, Toxoplasma gondii) - Fungi (Aspergillus species, Blastomyces dermatitidis, Candida species, Coccidioides immitis, Fusarium species, Penicillium species, Rhizopus species, and Sporothrix schenckii)
• Endophthalmitis can develop six weeks following eye surgery or an intravitreal injection (acute post-operative endophthalmitis) or months or even years following the procedure as a result of less virulent organisms (such as Propionibacterium acnes); in the latter case, it is referred to as chronic endophthalmitis. – Following penetrating ocular trauma to the globe
The thinned and stretched conjunctiva's incapacity to operate as a barrier against bacterial invasion late after a glaucoma filtering operation
Gram-positive organisms make up the majority of identified isolates in cases of acute post-operative endophthalmitis following cataract surgery. Rarely, hematogenous seeding from a distant site can cause endogenous endophthalmitis, which is caused by septic emboli from a diseased heart valve that lodge into the choroidal circulation.
• Gram-negative and streptococcal bacteria
Infections caused by organisms have a worse prognosis.
• Infections caused by mixed flora are more common following trauma; in open globe injuries from rural locations where organic materials is causing the damage, the prevalence can reach 42%.
• As seen in Uveitis-Chorioretinitis, parasites frequently result in chorioretinal lesions and a slower inflammatory response that may be more harmful than the infection itself.
COMMON CONNECTED CIRCUMSTANCES
The most frequent related condition is a history of penetrating trauma or recent eye surgery.
History of Diagnosis
• The majority of endophthalmitis patients arrive with conjunctival injection (redness) and eye pain. Light sensitivity, or photophobia, is a symptom of this condition. There may also be eyelid edema and conjunctival chemosis. Sometimes, though, the only sign is sight loss.
• In certain cases, a seemingly minor injury could not prompt the patient to seek medical attention until days or weeks later, when the signs and symptoms of an infection have emerged, exposing an occult penetrating injury, especially if the infecting organism is a fungus.
• The beginning of pain and severe sight loss are indicators of an aggressive course in some cases, particularly Bacillus cereus infections.
• One of the symptoms of panophthalmitis is pain when moving the eye.
MEDICAL EXAMINATION
• The formation of vitreous opacities is crucial for
diagnosis.
• White blood cell (WBC) layering in the anterior chamber, or hypopyon, is a typical occurrence.
• Hematogenous dissemination of infections is commonly characterized by chorioretinal infiltrates with secondary vitreous involvement.
Tests for Diagnosis and Interpretation Lab
First laboratory testing
• Although aqueous and vitreous aspiration for microbial cultures and smear should be carried out in cases of suspected endophthalmitis, this procedure can occasionally be inconclusive (cultures are positive in around 70% of suspected cases of post-operative infectious endophthalmitis).
• Smears should be cultured for aerobic and anaerobic bacteria, mycobacteria, and fungi (blood, chocolate, thioglycolate, Sabouraud, etc.) after being stained with Gram, Giemsa, and methenamine-silver.
Follow-up and Particular Points to Remember
• Although culture findings are usually positive in 48 hours, treatment shouldn't be postponed.
• Inadequate sampling may be the cause of negative outcomes.
fastidious organisms or due to sterile post-operative inflammation. • During vitrectomy, which is done for therapeutic or diagnostic purposes, vitreous aspiration material is regularly collected and can be either passed through a filter that can be stained and cultured or centrifuged and smeared.
Imagining
In cases of suspected retained intraocular foreign bodies, imaging using computer tomography or ultrasonography might be helpful, particularly when cloudy media make vision less than ideal.
Diagnostic Techniques and Other
Using a 25–30 G needle, aqueous humor should be extracted and sent for culture during a local anesthetic office procedure. A 23 G needle can be used to acquire vitreous samples through the pars plana.
Pathological Results
The presence of neutrophils is a characteristic of acute endophthalmitis.
DIFFERENTIAL DIAGNOSIS: Idiopathic or non-idiopathic uveitis, postoperative sterile inflammation brought on by intraocular pharmacologic agents (such as toxic anterior segment syndrome, or TASS), and postoperative sterile inflammation brought on by retained lens fragments in cases of complex cataract surgery are additional intraocular inflammatory syndromes that can resemble infectious endophthalmitis.
FIRST LINE TREATMENT MEDICATION
• Since acute post-operative bacterial endophthalmitis is a real ophthalmologic emergency, treatment needs to start right away.
• The current suggested treatment strategy is to provide 0.1 mL of each drug intravitreally: 1.0 mg/0.1 mL of vancomycin for Gram-positive coverage and 2.25 mg/0.1 mL of ceftazidime or 0.4 mg/0.1 mL of amikacin for Gram-negative coverage in cases of β-lactam hypersensitivity. The possible harmful effect of some drugs on the retina limits the selection of antibiotics.
In cases of exposed sutures or wound leaks, topical fluoroquinolone or fortified topical antibiotic preparations (e.g., cefazolin 50 mg/mL, vancomycin 25–50 mg/mL, and/or tobramycin 15 mg/mL) should be administered hourly to achieve adequate concentrations in the anterior chamber.
• After cataract surgery, systemic antibiotic administration
• The endophthalmitis vitrectomy study does not support infections related to surgery. The choice of aminoglycosides for the treatment of an illness primarily caused by Gram-positive isolates in this particular investigation limits the methodology of this conclusion.
Despite the lack of prospective evidence, systemic 4th-generation fluoroquinolones, such as moxifloxacin 400 mg p.o. daily, should be taken into consideration because of the high intraocular concentration that these antibiotics achieve.
• In addition to the aforesaid intravitreal vancomycin and ceftazidime, empirical systemic treatment of the presumed cause is advised in cases of bacterial endogenous endophthalmitis. The results of the culture should be used to customize the antibiotic treatment.
• The majority of treatment protocols advise intravitreal infusion of 0.1 mL of amphotericin B (5–10 μg/0.1 mL) for traumatic fungal endophthalmitis or post-operative fungal endophthalmitis. However, it is important to consider the possibility of retinal toxicity. Amphotericin B does not seem to reach adequate intraocular concentrations when administered systemically. For endogenous cases, however, systemic treatment is required.
• When intravenous drug abusers develop traumatic endophthalmitis or endogenous endophthalmitis, systemic clindamycin therapy (150–300 mg i.v. t.i.d.) or intravitreal clindamycin (0.1 mL of a 1 mg/0.1 mL) may be necessary.
Some experts advise using preparation) rather than vancomycin to provide protection against B. cereus, which is linked to a very aggressive course.
Although no comparable data are available, systemic fluconazole (400–600 mg i.v. or p.o. loading dosage per day followed by 200–400 mg p.o. or i.v. per day) may be less harmful than systemic amphotericin B for endogenous endophthalmitis caused by Candida albicans. Other alternatives include caspofungin and voriconazole.
ADDITIONAL MEDICATION
Overall Actions
Topical cycloplegic eye drops (atropine 1% daily or b.i.d.) and appropriate oral drugs are required to manage the associated pain.
Referral Issues
The patient should be sent to ophthalmology as soon as the diagnosis is suspected or confirmed.
COMPlementary and substitute Methods
It is generally acknowledged that topical (prednisolone acetate 1% eye drops) or periocular corticosteroids can alter the host immune response. It is debatable whether steroids (triamcinolone acetate 4 mg/0.1 mL [1 mL] or prednisone 60 mg p.o.) should be administered intravitreally or systemically.
OTHER PROCEDURES AND SURGERY
Pars Per the endophthalmitis vitrectomy trial, in instances related to cataract surgery, plana vitrectomy is helpful if visual acuity at presentation is light perception or worse. Early vitrectomy can clear the eye of toxins and necrotic tissue while also reducing the bacterial burden.
Considering the patient
First Stabilization
It is possible to treat post-operative endophthalmitis as an outpatient.
Getting in Criteria Hospitalization may be required because to social
factors or in patients who are monocular.
Continuing Care Follow-Up Suggestions
If the patient's health deteriorates 48 hours after starting intravitreal antibiotics, re-administration of the medication—with or without vitrectomy—should be taken into consideration.
Monitoring of Patients
The treating ophthalmologist should monitor the patient every day.
PROGNOSIS • The range of microorganisms involved and the resulting direct tissue damage contribute to the visual prognosis of traumatic endophthalmitis being poorer than postoperative endophthalmitis.
• In a recent combined series of post-traumatic endophthalmitis, only 30% of eyes were 20/400 or better after elective cataract surgery, whereas culture-proven infected eyes achieved visual acuity of 20/40 or better 50% of the time and 20/400 or better 85% of the time.
better. Seventy-four percent of participants in the endophthalmitis vitrectomy study experienced visual recovery of 20/100 or higher.
• The prognosis for endophthalmitis caused by B. cereus is nearly always poor.
COMPLICATIONS
The most frequent causes of vision loss are tissue necrosis and the inflammatory reaction to the retina. Phthisis, secondary glaucoma, and retinal detachment may ensue.
ENDOPHTHALMITIS
BASIC DESCRIPTION: Endophthalmitis is an infectious condition that affects the ocular (vitreous) cavity, while panophthalmitis is an inflammation that affects every eye structure.
The incidence of epidemiology
While the incidence of endophthalmitis following penetrating ocular trauma is reported to be between 3 and 30% and is typically higher in situations with retained intraocular foreign bodies, the rate following cataract surgery is between 0.1% and 0.3%.
RISK FACTORS • The most common risk factors include untreated blepharitis, poor surgical technique, and intraoperative complications/extended operating time.
• significant risk factors for acute endophthalmitis following surgery.
Patients who are immunocompromised, diabetic, or chronically unwell are most at risk for endogenous endophthalmitis, which has been reported to occur in 1 in 5,000 to 10,000 hospitalizations, particularly those who have indwelling intravenous catheters and/or positive blood cultures.
OVERALL PREVENTION
• Despite the absence of data showing a decrease in the incidence of post-operative endophthalmitis, routine post-operative administration of topical fluoroquinolones is thought to be the standard of care following cataract surgery.
• It has recently been demonstrated that intracameral administration of cefuroxime reduces the incidence of post-operative endophthalmitis following cataract surgery (1).
• For penetrating ocular injuries with a high risk of infection, such as intraocular foreign bodies, several authorities advise systemic intravenous prophylaxis with vancomycin (1 g i.v. b.i.d.) or moxifloxacin (400 mg p.o. each day).
• For anterior segment trauma, such as corneal laceration, topical antibiotics that are fortified (vancomycin 25–50 mg/mL, cefazolin 50 mg/mL, and/or tobramycin 15 mg/mL) or topical fluoroquinolones, as well as subconjunctival injections at the conclusion of the surgical procedure, can generate therapeutic levels of
antibiotics in the anterior chamber. Patients with infection foci, particularly those suffering from Candida spp.-caused fungemia, should be closely watched for the onset of endogenous endophthalmitis.
Pathophysiology
• Post-operative endophthalmitis can result from improper wound creation following cataract surgery, which permits conjunctival and eyelid flora to enter the anterior chamber.
• In individuals with infectious processes elsewhere, bacteria can spread through the bloodstream and initially impact the choroid, resulting in endogenous endophthalmitis.
ETIOLOGY • The causes of infectious endophthalmitis might be parasitic, bacterial, or fungal. Acinetobacter species, Actinomyces israelii, Bacillus species, Clostridium species, Corynebacterium species, Escherichia coli, Haemophilus influenzae, Klebsiella species, Listeria monocytogenes, Neisseria meningitides, Proteus species, and Propionibacterium are among the most frequent causes, listed alphabetically.
Salmonella typhimurium, Pseudomonas aeruginosa, Serratia marcescens, Streptococcus species, Staphylococcus species, acnes
- Parasites (Taenia solium, Toxocara canis, Toxoplasma gondii) - Fungi (Aspergillus species, Blastomyces dermatitidis, Candida species, Coccidioides immitis, Fusarium species, Penicillium species, Rhizopus species, and Sporothrix schenckii)
• Endophthalmitis can develop six weeks following eye surgery or an intravitreal injection (acute post-operative endophthalmitis) or months or even years following the procedure as a result of less virulent organisms (such as Propionibacterium acnes); in the latter case, it is referred to as chronic endophthalmitis. – Following penetrating ocular trauma to the globe
The thinned and stretched conjunctiva's incapacity to operate as a barrier against bacterial invasion late after a glaucoma filtering operation
Gram-positive organisms make up the majority of identified isolates in cases of acute post-operative endophthalmitis following cataract surgery. Rarely, hematogenous seeding from a distant site can cause endogenous endophthalmitis, which is caused by septic emboli from a diseased heart valve that lodge into the choroidal circulation.
• Gram-negative and streptococcal bacteria
Infections caused by organisms have a worse prognosis.
• Infections caused by mixed flora are more common following trauma; in open globe injuries from rural locations where organic materials is causing the damage, the prevalence can reach 42%.
• As seen in Uveitis-Chorioretinitis, parasites frequently result in chorioretinal lesions and a slower inflammatory response that may be more harmful than the infection itself.
COMMON CONNECTED CIRCUMSTANCES
The most frequent related condition is a history of penetrating trauma or recent eye surgery.
History of Diagnosis
• The majority of endophthalmitis patients arrive with conjunctival injection (redness) and eye pain. Light sensitivity, or photophobia, is a symptom of this condition. There may also be eyelid edema and conjunctival chemosis. Sometimes, though, the only sign is sight loss.
• In certain cases, a seemingly minor injury could not prompt the patient to seek medical attention until days or weeks later, when the signs and symptoms of an infection have emerged, exposing an occult penetrating injury, especially if the infecting organism is a fungus.
• The beginning of pain and severe sight loss are indicators of an aggressive course in some cases, particularly Bacillus cereus infections.
• One of the symptoms of panophthalmitis is pain when moving the eye.
MEDICAL EXAMINATION
• The formation of vitreous opacities is crucial for
diagnosis.
• White blood cell (WBC) layering in the anterior chamber, or hypopyon, is a typical occurrence.
• Hematogenous dissemination of infections is commonly characterized by chorioretinal infiltrates with secondary vitreous involvement.
Tests for Diagnosis and Interpretation Lab
First laboratory testing
• Although aqueous and vitreous aspiration for microbial cultures and smear should be carried out in cases of suspected endophthalmitis, this procedure can occasionally be inconclusive (cultures are positive in around 70% of suspected cases of post-operative infectious endophthalmitis).
• Smears should be cultured for aerobic and anaerobic bacteria, mycobacteria, and fungi (blood, chocolate, thioglycolate, Sabouraud, etc.) after being stained with Gram, Giemsa, and methenamine-silver.
Follow-up and Particular Points to Remember
• Although culture findings are usually positive in 48 hours, treatment shouldn't be postponed.
• Inadequate sampling may be the cause of negative outcomes.
fastidious organisms or due to sterile post-operative inflammation. • During vitrectomy, which is done for therapeutic or diagnostic purposes, vitreous aspiration material is regularly collected and can be either passed through a filter that can be stained and cultured or centrifuged and smeared.
Imagining
In cases of suspected retained intraocular foreign bodies, imaging using computer tomography or ultrasonography might be helpful, particularly when cloudy media make vision less than ideal.
Diagnostic Techniques and Other
Using a 25–30 G needle, aqueous humor should be extracted and sent for culture during a local anesthetic office procedure. A 23 G needle can be used to acquire vitreous samples through the pars plana.
Pathological Results
The presence of neutrophils is a characteristic of acute endophthalmitis.
DIFFERENTIAL DIAGNOSIS: Idiopathic or non-idiopathic uveitis, postoperative sterile inflammation brought on by intraocular pharmacologic agents (such as toxic anterior segment syndrome, or TASS), and postoperative sterile inflammation brought on by retained lens fragments in cases of complex cataract surgery are additional intraocular inflammatory syndromes that can resemble infectious endophthalmitis.
FIRST LINE TREATMENT MEDICATION
• Since acute post-operative bacterial endophthalmitis is a real ophthalmologic emergency, treatment needs to start right away.
• The current suggested treatment strategy is to provide 0.1 mL of each drug intravitreally: 1.0 mg/0.1 mL of vancomycin for Gram-positive coverage and 2.25 mg/0.1 mL of ceftazidime or 0.4 mg/0.1 mL of amikacin for Gram-negative coverage in cases of β-lactam hypersensitivity. The possible harmful effect of some drugs on the retina limits the selection of antibiotics.
In cases of exposed sutures or wound leaks, topical fluoroquinolone or fortified topical antibiotic preparations (e.g., cefazolin 50 mg/mL, vancomycin 25–50 mg/mL, and/or tobramycin 15 mg/mL) should be administered hourly to achieve adequate concentrations in the anterior chamber.
• After cataract surgery, systemic antibiotic administration
• The endophthalmitis vitrectomy study does not support infections related to surgery. The choice of aminoglycosides for the treatment of an illness primarily caused by Gram-positive isolates in this particular investigation limits the methodology of this conclusion.
Despite the lack of prospective evidence, systemic 4th-generation fluoroquinolones, such as moxifloxacin 400 mg p.o. daily, should be taken into consideration because of the high intraocular concentration that these antibiotics achieve.
• In addition to the aforesaid intravitreal vancomycin and ceftazidime, empirical systemic treatment of the presumed cause is advised in cases of bacterial endogenous endophthalmitis. The results of the culture should be used to customize the antibiotic treatment.
• The majority of treatment protocols advise intravitreal infusion of 0.1 mL of amphotericin B (5–10 μg/0.1 mL) for traumatic fungal endophthalmitis or post-operative fungal endophthalmitis. However, it is important to consider the possibility of retinal toxicity. Amphotericin B does not seem to reach adequate intraocular concentrations when administered systemically. For endogenous cases, however, systemic treatment is required.
• When intravenous drug abusers develop traumatic endophthalmitis or endogenous endophthalmitis, systemic clindamycin therapy (150–300 mg i.v. t.i.d.) or intravitreal clindamycin (0.1 mL of a 1 mg/0.1 mL) may be necessary.
Some experts advise using preparation) rather than vancomycin to provide protection against B. cereus, which is linked to a very aggressive course.
Although no comparable data are available, systemic fluconazole (400–600 mg i.v. or p.o. loading dosage per day followed by 200–400 mg p.o. or i.v. per day) may be less harmful than systemic amphotericin B for endogenous endophthalmitis caused by Candida albicans. Other alternatives include caspofungin and voriconazole.
ADDITIONAL MEDICATION
Overall Actions
Topical cycloplegic eye drops (atropine 1% daily or b.i.d.) and appropriate oral drugs are required to manage the associated pain.
Referral Issues
The patient should be sent to ophthalmology as soon as the diagnosis is suspected or confirmed.
COMPlementary and substitute Methods
It is generally acknowledged that topical (prednisolone acetate 1% eye drops) or periocular corticosteroids can alter the host immune response. It is debatable whether steroids (triamcinolone acetate 4 mg/0.1 mL [1 mL] or prednisone 60 mg p.o.) should be administered intravitreally or systemically.
OTHER PROCEDURES AND SURGERY
Pars Per the endophthalmitis vitrectomy trial, in instances related to cataract surgery, plana vitrectomy is helpful if visual acuity at presentation is light perception or worse. Early vitrectomy can clear the eye of toxins and necrotic tissue while also reducing the bacterial burden.
Considering the patient
First Stabilization
It is possible to treat post-operative endophthalmitis as an outpatient.
Getting in Criteria Hospitalization may be required because to social
factors or in patients who are monocular.
Continuing Care Follow-Up Suggestions
If the patient's health deteriorates 48 hours after starting intravitreal antibiotics, re-administration of the medication—with or without vitrectomy—should be taken into consideration.
Monitoring of Patients
The treating ophthalmologist should monitor the patient every day.
PROGNOSIS • The range of microorganisms involved and the resulting direct tissue damage contribute to the visual prognosis of traumatic endophthalmitis being poorer than postoperative endophthalmitis.
• In a recent combined series of post-traumatic endophthalmitis, only 30% of eyes were 20/400 or better after elective cataract surgery, whereas culture-proven infected eyes achieved visual acuity of 20/40 or better 50% of the time and 20/400 or better 85% of the time.
better. Seventy-four percent of participants in the endophthalmitis vitrectomy study experienced visual recovery of 20/100 or higher.
• The prognosis for endophthalmitis caused by B. cereus is nearly always poor.
COMPLICATIONS
The most frequent causes of vision loss are tissue necrosis and the inflammatory reaction to the retina. Phthisis, secondary glaucoma, and retinal detachment may ensue.

- Published on
Infectious Disease – Infective Endocarditis
ENDOCARDITIS (VALVE PROSTHETIC)
ESSENTIALS DESCRIPTION
An infection of prosthetic heart valves or prosthetic material by bacteria, fungus, or infrequently chlamydiae or rickettsiae is known as prosthetic valve endocarditis.
The incidence of epidemiology
Prosthetic valve infective endocarditis (PVIE) affects between 0.3 and 1% of patients annually.
RISK ELEMENTS
• Healthcare-associated infections are the most significant risk factors for the development of prosthetic valve infection.
• Hemodialysis and long-term intravascular access are additional risk factors.
OVERALL PREVENTION
• Patients with the following conditions are advised to avoid endocarditis by taking antibiotics (2):
A prosthetic heart valve or material for valve repair; prior endocarditis
Congenital heart disease (repaired CHD with a persisting defect, unrepaired cyanotic CHD)
Cardiac valvulopathy in recipients of heart transplants
• Prophylaxis is advised for dental operations that include gingival manipulation and disruption of the oral mucosa.
• Patients with the high-risk disorders mentioned above who have procedures involving the respiratory system, soft tissues of the skin, or muscles should also consider prophylaxis. It is not advised to use antibiotics during GI or GU procedures in order to prevent IE.
• Among the antibiotic regimens are a single dosage of either 600 mg of clindamycin or 2 g of amoxicillin 30 to 60 minutes before the surgery.
Pathophysiology
Prosthetic valve endocarditis may arise as a result of contiguous infection spread, secondary infection by hematogenous dissemination, or contamination of the device during implantation.
ETIOLOGY • The most frequent cause of prosthetic valve infection is Staphylococci.
• There are two types of prosthetic valve IE: early-onset, which happens within 60 days of surgery, and late-onset, which happens later.
• While late-onset PVIE is brought on by pathogens that are similar to native valve IE, early-onset PVIE is frequently caused by hospital-acquired pathogens.
• Staphylococcus aureus (20–35%), including MRSA, coagulase negative staphylococcus (17–30%), Streptococcus spp. (1–4%), Enterococcus spp. (5–10%), fungal (5–10%), gram-negative bacilli (6–15%), or culture-negative IE (3–17%) are the most common microbiologic etiologies for early onset IE.
S. aureus (15–20%), coagulase negative staphylococcus (10–20%), Streptococcus spp. (20–30%), Enterococcus spp. (8–13%), fungal (1–3%), gram-negative bacilli (4–7%), or culture-negative (3–12%) IE are the most prevalent microbiologic causes of late onset IE.
• Antibiotics taken within the previous seven days, slow-growing, picky anaerobes, fungi (non-Candida species), Bartonella spp., Coxiella burnetii (Q fever), Legionella spp., Tropheryma whippelii, Chlamydia spp., or Brucella spp. are some of the potential causes of culture-negative endocarditis.
History of Diagnosis
• PVIE's clinical characteristics vary greatly. It might manifest as an acute, toxic illness with high fevers or as a chronic, indolent illness.
• A comprehensive workup for endocarditis is necessary in individuals with prosthetic valves and an inexplicable fever.
• More than 70% of people with PVIE have a fever. Weakness, chills, sweats, anorexia, weight loss, nausea, and malaise are examples of nonspecific symptoms.
• Get a thorough medical history that includes recent travel, exposure to animals, and dietary practices such eating unpasteurized dairy products.
• One popular set of diagnostic criteria for Internet Explorer is the modified Duke criteria. To determine if endocarditis is definite or conceivable, or to rule out the diagnosis completely, they integrate clinical characteristics, microbiologic data, echocardiography, and pathologic data. (Taken from Li and others).
• The primary criterion is microbiological (1) Two sets of blood cultures tested positive for common pathogens, such as Streptococcus bovis, Viridans streptococci, HACEK group, and S.
aureus; or enterococci from the population that don't have a primary focus; or (2) IE-consistent microorganisms from blood cultures that consistently test positive; or (3) a single positive blood culture for Coxiella burnetii or anti-phase 1 IgG antibody titer more than 1:800
Evidence of involvement of the endocardium (1) Positive echocardiography (new partial dehiscence of prosthetic valve, abscess, or oscillating intracardiac mass on valve) (2) New valvular regurgitation (inadequate preexisting murmur or worsening or altering)
• Minor criteria: IDU, predisposing cardiac disease, or predisposition A fever
Vascular manifestations include Janeway's lesions, mycotic aneurysms, septic pulmonary infarcts, cerebral hemorrhages, conjunctival hemorrhages, and major arterial emboli.
Immunologic phenomena include rheumatoid factor, Osler's nodes, Roth's spots, and glomerulonephritis.
Microbiological evidence: Serological evidence of a current infection with an organism consistent with IE or a positive blood culture that does not satisfy one of the key criteria mentioned above
• Two main criteria, one major criterion plus three minor criteria, or five minor criteria are the clinical criteria for definitive endocarditis.
• The pathologic criteria for definitive endocarditis:
microorganisms detected by pathologic or cultural analysis of vegetation, embolized vegetation, or intracardiac abscess; or histological analysis of vegetation or intracardiac abscess exhibiting active endocarditis.
• One main criterion plus one minor criterion, or three minor criteria, may indicate endocarditis.
• Rejected: Does not fulfill clinical criteria for probable IE; has no pathologic evidence of IE at surgery with less than 4 days of antibiotics; has a firm alternative diagnosis; and resolves symptoms in less than 4 days.
MEDICAL EXAMINATION
• A new or altered murmur or signs of congestive heart failure may be found during the cardiac examination.
• A comprehensive examination should be performed to detect embolic events (stroke) or other infection sites (epidural abscess, psoas abscess, septic arthritis).
Tests for Diagnosis and Interpretation Lab
First laboratory testing
• Complete blood count with differential, electrolytes, blood urea nitrogen, creatinine, liver function tests, several sets of blood cultures, urinalysis, and ESR are all part of the initial laboratory examination for suspected IE.
• Get at least three sets of blood cultures within the first twenty-four hours. To increase the likelihood of detecting the causing bacterium, draw multiple sets of blood cultures prior to giving antibiotics. Up to 90% of patients had positive results from the first two sets.
• Elevations of serum inflammatory markers (CRP, ESR) and leukocytosis are frequent.
Follow-up and Particular Points to Remember
• Serologic testing for uncommon pathogens including Q fever and Bartonella spp. may be necessary in cases of culture-negative endocarditis.
• Until the endovascular infection has resolved, obtain two sets of blood cultures every 24 to 48 hours.
Imaging First Step
• The preferred imaging procedure is transesophageal echocardiography (TEE). Because of the high incidence of paravalvular problems and artifact from mechanical prosthesis, TEE is recommended over transthoracic echocardiography.
and a tiny amount of greenery. TEE can identify vegetation with a sensitivity of 86–94% and a specificity of 91–100%.
• When prosthetic valve IE is suspected, a TEE should be conducted as soon as feasible.
Follow-up and Particular Points to Remember
If there is a suspicion of emboli, abscesses, or mycotic aneurysm, further imaging of the brain, spine, abdomen, or lungs is necessary.
Diagnostic Techniques and Other
To determine a baseline heart rhythm and detect any conduction diseases, have an EKG. Bradycardia, syncope, presyncope, or a change in clinical state all call for a repeat EKG.
Pathological Results
• According to histopathologic analysis, vegetations are made up of bacterial or fungal masses, fibrin, and platelet aggregates.
• Some laboratories offer PCR-based assays on blood or valvular tissue for hard-to-culture organisms including T. whippleii and Bartonella spp., which may be indicated in certain cases of culture negative results.
endocarditis.
DISTINCTIVE DIAGNOSIS
Other systemic illnesses including malaria, bacteriemia, or fungemia without IE, as well as noninfectious endocarditis.
MEDICATION FOR TREATMENT
• To break through the vegetation and stop recurrence, prolonged antibacterial treatment is necessary. It is critical to identify the causal organism and medication susceptibilities.
• The severity of the illness, local resistance patterns, and patient risk factors for different pathogens are the foundations of empirical therapy.
• The following is a list of suggested treatment plans for specific pathogens (1).
• Penicillin G 24 million U/24 h (given continuously or in 4–6 doses) • Penicillin susceptible Viridans streptococci, S. bovis, or other streptococci (minimum inhibitory concentration ≤0.12 μg/mL) or, if PCN and ceftriaxone are intolerant or allergic, ceftriaxone 2g IV daily for 6 weeks + gentamicin 3 mg/kg/d in a single dosage for 2 weeks – Vancomycin 30 mg/kg/d in 2 divided doses for 6 weeks
MIC >0.12 μg/mL or ≤0.5 μg/mL for streptococci that are highly resistant to penicillin; Penicillin G 24 million U/24 h (dosed continuously or
Vancomycin 30 mg/kg/d in 2 divided doses plus gentamicin 3 mg/kg/d in 3 divided doses for 6 weeks if ampicillin allergy; or ceftriaxone 2g IV daily plus gentamicin 3 mg/kg/d in 1 dose for 6 weeks; Streptococci resistant to penicillin (MIC >0.5 μg/mL) and enterococci – Ampicillin 12 g/d in 6 divided doses plus gentamicin 3 mg/kg/d in 3 divided doses for 6 weeks
Methicillin-resistant staphylococci: Vancomycin 30 mg/kg/d in 2 divided doses plus rifampin 900 mg/d in 3 divided doses for ≥6 weeks plus gentamicin 3 mg/kg/d in 2 or 3 divided doses for 2 weeks; Methicillin-susceptible staphylococci: Nafcillin 12 g/d IV in 6 divided doses plus rifampin 900 mg/d in 3 divided doses for ≥6 weeks plus gentamicin 3 mg/kg/d in 2 or 3 divided doses for 2 weeks; The doses above are based on normal renal function.
ADDITIONAL MEDICATION
Overall Actions
When clinically stable, refer IDU patients to drug treatment programs.
Referral Issues
Infectious endocarditis of the prosthetic valve and its aftereffects can be fatal, and complicated management problems are frequent. It is crucial to have a multidisciplinary strategy that incorporates input from infectious diseases, cardiology, and cardiovascular surgery.
OTHER PROCEDURES AND SURGERY
• Patients with endocarditis from prosthetic valves should be assessed for possible surgery as soon as possible. Each patient has a different need and time for valve replacement.
• Dehiscence of the valve, perforation, fistula, rupture, big abscess, or insufficient antimicrobial therapy (very resistant infections) are indications for considering valve replacement.
Considering the patient
First Stabilization
Evaluate and maintain the heart and respiratory systems in
Acute endocarditis is suspected. It is necessary to promptly assess cardiac conduction and volume status.
Admission Requirements Hospitalization is necessary for monitoring, the start of intravenous antibiotics, and a speedy workup for patients with endocarditis.
Criteria for Discharge
When fevers have subsided for longer than twenty-four hours, vital signs are normal, an antibiotic is prescribed, and follow-up arrangements are established, patients may be released.
Continuing Care Follow-Up Suggestions
• In the short term, keep a watchful eye on patients for endocarditis problems or recurrence, as well as side effects associated with antibiotic medication.
• To record new baseline valve and heart function, a TTE is advised at the end of IE therapy.
Weekly monitoring labs should be sent to patients receiving intravenous antibiotics in accordance with the package insert or guidelines (http://www.idsociety.org/content.aspx?id = 4428#opat).
PATIENT EDUCATION Patients with IE need to know about the symptoms and indicators of valve dysfunction, the significance of maintaining proper oral hygiene, and how to avoid IE related to dental operations.
PROGNOSIS • Higher mortality rates have been linked to infections related to health care, congestive heart failure, aging, S. aureus infections, chronic bacteremia, stroke, and intracardiac abscesses.
• A recent study found that the in-hospital mortality rate linked to PVIE was 22.8%.
COMPLICATIONS
Mycotic aneurysm, meningitis, cerebritis, splenic infarctions, ring abscess, congestive heart failure, cerebral emboli, stroke, kidney infarctions, immune complex glomerulonephritis, periprosthetic leak, heart block, pulmonary embolism with or without infarction in right-sided endocarditis, and splenic abscess.
ENDOCARDITIS (VALVE PROSTHETIC)
ESSENTIALS DESCRIPTION
An infection of prosthetic heart valves or prosthetic material by bacteria, fungus, or infrequently chlamydiae or rickettsiae is known as prosthetic valve endocarditis.
The incidence of epidemiology
Prosthetic valve infective endocarditis (PVIE) affects between 0.3 and 1% of patients annually.
RISK ELEMENTS
• Healthcare-associated infections are the most significant risk factors for the development of prosthetic valve infection.
• Hemodialysis and long-term intravascular access are additional risk factors.
OVERALL PREVENTION
• Patients with the following conditions are advised to avoid endocarditis by taking antibiotics (2):
A prosthetic heart valve or material for valve repair; prior endocarditis
Congenital heart disease (repaired CHD with a persisting defect, unrepaired cyanotic CHD)
Cardiac valvulopathy in recipients of heart transplants
• Prophylaxis is advised for dental operations that include gingival manipulation and disruption of the oral mucosa.
• Patients with the high-risk disorders mentioned above who have procedures involving the respiratory system, soft tissues of the skin, or muscles should also consider prophylaxis. It is not advised to use antibiotics during GI or GU procedures in order to prevent IE.
• Among the antibiotic regimens are a single dosage of either 600 mg of clindamycin or 2 g of amoxicillin 30 to 60 minutes before the surgery.
Pathophysiology
Prosthetic valve endocarditis may arise as a result of contiguous infection spread, secondary infection by hematogenous dissemination, or contamination of the device during implantation.
ETIOLOGY • The most frequent cause of prosthetic valve infection is Staphylococci.
• There are two types of prosthetic valve IE: early-onset, which happens within 60 days of surgery, and late-onset, which happens later.
• While late-onset PVIE is brought on by pathogens that are similar to native valve IE, early-onset PVIE is frequently caused by hospital-acquired pathogens.
• Staphylococcus aureus (20–35%), including MRSA, coagulase negative staphylococcus (17–30%), Streptococcus spp. (1–4%), Enterococcus spp. (5–10%), fungal (5–10%), gram-negative bacilli (6–15%), or culture-negative IE (3–17%) are the most common microbiologic etiologies for early onset IE.
S. aureus (15–20%), coagulase negative staphylococcus (10–20%), Streptococcus spp. (20–30%), Enterococcus spp. (8–13%), fungal (1–3%), gram-negative bacilli (4–7%), or culture-negative (3–12%) IE are the most prevalent microbiologic causes of late onset IE.
• Antibiotics taken within the previous seven days, slow-growing, picky anaerobes, fungi (non-Candida species), Bartonella spp., Coxiella burnetii (Q fever), Legionella spp., Tropheryma whippelii, Chlamydia spp., or Brucella spp. are some of the potential causes of culture-negative endocarditis.
History of Diagnosis
• PVIE's clinical characteristics vary greatly. It might manifest as an acute, toxic illness with high fevers or as a chronic, indolent illness.
• A comprehensive workup for endocarditis is necessary in individuals with prosthetic valves and an inexplicable fever.
• More than 70% of people with PVIE have a fever. Weakness, chills, sweats, anorexia, weight loss, nausea, and malaise are examples of nonspecific symptoms.
• Get a thorough medical history that includes recent travel, exposure to animals, and dietary practices such eating unpasteurized dairy products.
• One popular set of diagnostic criteria for Internet Explorer is the modified Duke criteria. To determine if endocarditis is definite or conceivable, or to rule out the diagnosis completely, they integrate clinical characteristics, microbiologic data, echocardiography, and pathologic data. (Taken from Li and others).
• The primary criterion is microbiological (1) Two sets of blood cultures tested positive for common pathogens, such as Streptococcus bovis, Viridans streptococci, HACEK group, and S.
aureus; or enterococci from the population that don't have a primary focus; or (2) IE-consistent microorganisms from blood cultures that consistently test positive; or (3) a single positive blood culture for Coxiella burnetii or anti-phase 1 IgG antibody titer more than 1:800
Evidence of involvement of the endocardium (1) Positive echocardiography (new partial dehiscence of prosthetic valve, abscess, or oscillating intracardiac mass on valve) (2) New valvular regurgitation (inadequate preexisting murmur or worsening or altering)
• Minor criteria: IDU, predisposing cardiac disease, or predisposition A fever
Vascular manifestations include Janeway's lesions, mycotic aneurysms, septic pulmonary infarcts, cerebral hemorrhages, conjunctival hemorrhages, and major arterial emboli.
Immunologic phenomena include rheumatoid factor, Osler's nodes, Roth's spots, and glomerulonephritis.
Microbiological evidence: Serological evidence of a current infection with an organism consistent with IE or a positive blood culture that does not satisfy one of the key criteria mentioned above
• Two main criteria, one major criterion plus three minor criteria, or five minor criteria are the clinical criteria for definitive endocarditis.
• The pathologic criteria for definitive endocarditis:
microorganisms detected by pathologic or cultural analysis of vegetation, embolized vegetation, or intracardiac abscess; or histological analysis of vegetation or intracardiac abscess exhibiting active endocarditis.
• One main criterion plus one minor criterion, or three minor criteria, may indicate endocarditis.
• Rejected: Does not fulfill clinical criteria for probable IE; has no pathologic evidence of IE at surgery with less than 4 days of antibiotics; has a firm alternative diagnosis; and resolves symptoms in less than 4 days.
MEDICAL EXAMINATION
• A new or altered murmur or signs of congestive heart failure may be found during the cardiac examination.
• A comprehensive examination should be performed to detect embolic events (stroke) or other infection sites (epidural abscess, psoas abscess, septic arthritis).
Tests for Diagnosis and Interpretation Lab
First laboratory testing
• Complete blood count with differential, electrolytes, blood urea nitrogen, creatinine, liver function tests, several sets of blood cultures, urinalysis, and ESR are all part of the initial laboratory examination for suspected IE.
• Get at least three sets of blood cultures within the first twenty-four hours. To increase the likelihood of detecting the causing bacterium, draw multiple sets of blood cultures prior to giving antibiotics. Up to 90% of patients had positive results from the first two sets.
• Elevations of serum inflammatory markers (CRP, ESR) and leukocytosis are frequent.
Follow-up and Particular Points to Remember
• Serologic testing for uncommon pathogens including Q fever and Bartonella spp. may be necessary in cases of culture-negative endocarditis.
• Until the endovascular infection has resolved, obtain two sets of blood cultures every 24 to 48 hours.
Imaging First Step
• The preferred imaging procedure is transesophageal echocardiography (TEE). Because of the high incidence of paravalvular problems and artifact from mechanical prosthesis, TEE is recommended over transthoracic echocardiography.
and a tiny amount of greenery. TEE can identify vegetation with a sensitivity of 86–94% and a specificity of 91–100%.
• When prosthetic valve IE is suspected, a TEE should be conducted as soon as feasible.
Follow-up and Particular Points to Remember
If there is a suspicion of emboli, abscesses, or mycotic aneurysm, further imaging of the brain, spine, abdomen, or lungs is necessary.
Diagnostic Techniques and Other
To determine a baseline heart rhythm and detect any conduction diseases, have an EKG. Bradycardia, syncope, presyncope, or a change in clinical state all call for a repeat EKG.
Pathological Results
• According to histopathologic analysis, vegetations are made up of bacterial or fungal masses, fibrin, and platelet aggregates.
• Some laboratories offer PCR-based assays on blood or valvular tissue for hard-to-culture organisms including T. whippleii and Bartonella spp., which may be indicated in certain cases of culture negative results.
endocarditis.
DISTINCTIVE DIAGNOSIS
Other systemic illnesses including malaria, bacteriemia, or fungemia without IE, as well as noninfectious endocarditis.
MEDICATION FOR TREATMENT
• To break through the vegetation and stop recurrence, prolonged antibacterial treatment is necessary. It is critical to identify the causal organism and medication susceptibilities.
• The severity of the illness, local resistance patterns, and patient risk factors for different pathogens are the foundations of empirical therapy.
• The following is a list of suggested treatment plans for specific pathogens (1).
• Penicillin G 24 million U/24 h (given continuously or in 4–6 doses) • Penicillin susceptible Viridans streptococci, S. bovis, or other streptococci (minimum inhibitory concentration ≤0.12 μg/mL) or, if PCN and ceftriaxone are intolerant or allergic, ceftriaxone 2g IV daily for 6 weeks + gentamicin 3 mg/kg/d in a single dosage for 2 weeks – Vancomycin 30 mg/kg/d in 2 divided doses for 6 weeks
MIC >0.12 μg/mL or ≤0.5 μg/mL for streptococci that are highly resistant to penicillin; Penicillin G 24 million U/24 h (dosed continuously or
Vancomycin 30 mg/kg/d in 2 divided doses plus gentamicin 3 mg/kg/d in 3 divided doses for 6 weeks if ampicillin allergy; or ceftriaxone 2g IV daily plus gentamicin 3 mg/kg/d in 1 dose for 6 weeks; Streptococci resistant to penicillin (MIC >0.5 μg/mL) and enterococci – Ampicillin 12 g/d in 6 divided doses plus gentamicin 3 mg/kg/d in 3 divided doses for 6 weeks
Methicillin-resistant staphylococci: Vancomycin 30 mg/kg/d in 2 divided doses plus rifampin 900 mg/d in 3 divided doses for ≥6 weeks plus gentamicin 3 mg/kg/d in 2 or 3 divided doses for 2 weeks; Methicillin-susceptible staphylococci: Nafcillin 12 g/d IV in 6 divided doses plus rifampin 900 mg/d in 3 divided doses for ≥6 weeks plus gentamicin 3 mg/kg/d in 2 or 3 divided doses for 2 weeks; The doses above are based on normal renal function.
ADDITIONAL MEDICATION
Overall Actions
When clinically stable, refer IDU patients to drug treatment programs.
Referral Issues
Infectious endocarditis of the prosthetic valve and its aftereffects can be fatal, and complicated management problems are frequent. It is crucial to have a multidisciplinary strategy that incorporates input from infectious diseases, cardiology, and cardiovascular surgery.
OTHER PROCEDURES AND SURGERY
• Patients with endocarditis from prosthetic valves should be assessed for possible surgery as soon as possible. Each patient has a different need and time for valve replacement.
• Dehiscence of the valve, perforation, fistula, rupture, big abscess, or insufficient antimicrobial therapy (very resistant infections) are indications for considering valve replacement.
Considering the patient
First Stabilization
Evaluate and maintain the heart and respiratory systems in
Acute endocarditis is suspected. It is necessary to promptly assess cardiac conduction and volume status.
Admission Requirements Hospitalization is necessary for monitoring, the start of intravenous antibiotics, and a speedy workup for patients with endocarditis.
Criteria for Discharge
When fevers have subsided for longer than twenty-four hours, vital signs are normal, an antibiotic is prescribed, and follow-up arrangements are established, patients may be released.
Continuing Care Follow-Up Suggestions
• In the short term, keep a watchful eye on patients for endocarditis problems or recurrence, as well as side effects associated with antibiotic medication.
• To record new baseline valve and heart function, a TTE is advised at the end of IE therapy.
Weekly monitoring labs should be sent to patients receiving intravenous antibiotics in accordance with the package insert or guidelines (http://www.idsociety.org/content.aspx?id = 4428#opat).
PATIENT EDUCATION Patients with IE need to know about the symptoms and indicators of valve dysfunction, the significance of maintaining proper oral hygiene, and how to avoid IE related to dental operations.
PROGNOSIS • Higher mortality rates have been linked to infections related to health care, congestive heart failure, aging, S. aureus infections, chronic bacteremia, stroke, and intracardiac abscesses.
• A recent study found that the in-hospital mortality rate linked to PVIE was 22.8%.
COMPLICATIONS
Mycotic aneurysm, meningitis, cerebritis, splenic infarctions, ring abscess, congestive heart failure, cerebral emboli, stroke, kidney infarctions, immune complex glomerulonephritis, periprosthetic leak, heart block, pulmonary embolism with or without infarction in right-sided endocarditis, and splenic abscess.

- Published on
Infectious Disease - Endocarditis (Native Valves)
Endocarditis is an infection of the heart valves or endocardium caused by bacteria, fungus, or, less commonly, chlamydiae or rickettsiae. The mitral valve (41%) and aortic valve (38%) are the most frequently implicated in native valve infective endocarditis (NVIE). Tricuspid valve endocarditis is more prevalent among intravenous drug users. Pulmonic valve endocarditis is exceedingly uncommon. Several valves may be affected.
EPIDEMIOLOGY Incidence The prevalence of NVIE is between 1.7–6.2 cases per 100,000 patient-years. The incidence among intravenous drug users is estimated to be 1500–3300 cases per 100,000 patient-years.
Risk Factors
Predisposing factors encompass active intravenous drug use, a history of endocarditis, chronic intravascular access, the presence of an implantable cardiac device, congenital heart anomalies, a bicuspid aortic valve, rheumatic heart disease, and degenerative valvular disease.
GENERAL PREVENTION • Antibiotic prophylaxis for endocarditis is advised for people with the following conditions: – Prosthetic heart valve or valve repair utilizing prosthetic material – History of endocarditis - Congenital heart disease (unrepaired cyanotic CHD, treated CHD with residual abnormality) - Recipients of cardiac transplants with valvular heart disease
Prophylaxis is advised for dental procedures that include disruption of the oral mucosa and manipulation of the gingiva.
Prophylaxis is advisable for individuals with high-risk disorders, as previously mentioned, who are undergoing procedures involving the respiratory tract, skin, soft tissue, or muscle. Antibiotics for the prophylaxis of infective endocarditis are not advised for gastrointestinal or genitourinary surgeries.
Antibiotic protocols consist of a single dosage of amoxicillin 2 g or clindamycin 600 mg administered 30–60 minutes before the surgery.
ETIOLOGY • The predominant causal pathogens are gram-positive bacteria. Staphylococcus aureus has recently emerged as the predominant cause of NVIE. • The prevalent microbiological etiologies for NVIE are enumerated below: S. aureus (25–35%) — Coagulase-negative Staphylococcus (3–11%) - Viridans group streptococci (17–40 percent) - Streptococcus bovis (6 percent) - Additional streptococcus (6–19%) - Enterococcus species (10–18%) - HACEK (2–5 percent) Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella species. - Fungi/yeast (2–4 percent) • Culture-negative endocarditis (10%) The predominant cause is the administration of antibiotics within the preceding 7 days. – Alternative potential etiologies encompass slow-growing fastidious anaerobes, non-Candida fungal species, Bartonella spp., Coxiella burnetii (Q fever), Legionella spp., Tropheryma whippelii, Chlamydia spp., and Brucella spp. In intravenous drug users, polymicrobial non-valvular infective endocarditis (NVIE) is more prevalent.
DIAGNOSIS HISTORY
The clinical manifestations of NVIE exhibit significant variability, encompassing symptoms and indications attributable to the infected valve, embolic events, metastatic infection locations, and circulating immune complexes. Fever occurs in more than 90% of people with NVIE. General symptoms including weakness, chills, diaphoresis, anorexia, weight loss, nausea, and malaise may occur (3). • The revised Duke criteria are extensively utilized diagnostic standards for NVIE. • Principal criteria: – Microbiological evidence includes two sets of blood cultures positive for typical microorganisms such as Viridans streptococci, S. bovis, HACEK group, S. aureus; or community-acquired enterococci without a primary focus; or microorganisms consistent with infective endocarditis from persistently positive blood cultures; or a single positive blood culture for Coxiella burnetii or an anti-phase 1 IgG antibody titer exceeding 1:800. - Indications of endocardial involvement Favorable echocardiography (oscillating intracardiac mass on valve, abscess, or fresh partial dehiscence of prosthetic valve) New valvular regurgitation (deterioration or alteration of a preexisting murmur is inadequate)
• Minor criterion – Predisposition, preexisting cardiac disease, or intravenous drug use (IDU) – Pyrexia – Vascular manifestations: Significant artery emboli, septic pulmonary infarcts, mycotic aneurysms, cerebral hemorrhage, conjunctival hemorrhages, and Janeway lesions - Immunological manifestations: Glomerulonephritis, Osler's nodes, Roth's spots, and rheumatoid factor - Microbiological evidence: Positive blood culture; however, it does not fulfill a significant requirement as previously indicated, nor is there serological evidence of current infection with an organism consistent with infective endocarditis. • Definitive endocarditis (clinical criteria): 2 main criteria; or 1 major criterion in conjunction with 3 minor criteria; or 5 minor criteria • Conclusive endocarditis (pathological criteria): Microorganisms discovered through culture or pathological study of vegetation, embolized vegetation, or intracardiac abscess; or vegetation or intracardiac abscess exhibiting active endocarditis via histological evaluation. • Potential endocarditis: 1 major criterion + 1 minor criterion; or 3 minor criteria • Rejected: Definitive alternative diagnosis; symptom remission within 4 days of antibiotic treatment; absence of pathological evidence of infective endocarditis during surgery after fewer than 4 days of antibiotics; does not fulfill clinical criteria for probable infective endocarditis.
PHYSICAL EXAM • Clinical manifestations of infective endocarditis (IE) may present as a new or altered murmur in up to 85% of cases. • Petechiae occur in 20–40% of patients. Other cutaneous manifestations (Osler nodes, Janeway lesions, splinter hemorrhages) or Roth spots are observed in a minority of patients. A comprehensive examination is necessary to detect further infection sites (epidural abscess, psoas abscess, septic arthritis) or to discover embolic occurrences (stroke).
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Preliminary laboratory assessments In cases of suspected NVIE, the initial laboratory assessment include a full blood count with differential, electrolytes, blood urea nitrogen, creatinine, liver function tests, several sets of blood cultures, urinalysis, and erythrocyte sedimentation rate (ESR). • Within the initial 24 hours, get a minimum of 3 sets of blood cultures. Obtain multiple sets of blood cultures prior to administering antibiotics to enhance the likelihood of identifying the causal bacteria. The initial two sets yield positive results in up to 90% of patients. Leukocytosis is prevalent. Over fifty percent of patients exhibit elevated serum inflammatory markers (ESR, C-reactive protein). The urinalysis often indicates the presence of proteinuria or microscopic hematuria.
Subsequent Actions & Unique Considerations
• In instances of culture-negative endocarditis, serological assessment for uncommon pathogens such as Q fever and Bartonella spp. may be warranted. • Acquire two sets of blood cultures every 24 to 48 hours until the endovascular infection has resolved. Imaging: Preliminary Approach Echocardiography is the preferred imaging modality and should be conducted promptly in all instances of suspected NVIE.
• The sensitivity of transthoracic echocardiography (TTE) for identifying left-sided vegetations varies between 40% and 63%, with a specificity of 91% to 98%. The sensitivity for right-sided lesions is elevated due to the proximity of the tricuspid and pulmonic valves to the chest wall. Transesophageal echocardiography may be constrained by obesity, chronic pulmonary illness, or thoracic wall deformities.
Transesophageal echocardiography (TEE) exhibits a sensitivity of 90–100% and a specificity of 91–98% in the identification of vegetations. TEE exhibits greater sensitivity than TTE in detecting valve perforation, pacemaker-associated infective endocarditis, and cardiac abscess.
Transesophageal echocardiography (TEE) is advised as the primary diagnostic test when transthoracic echocardiography (TTE) is anticipated to yield suboptimal results, there is a strong clinical suspicion of infective endocarditis (IE), or perivalvular extension is predicted. If the initial TTE is negative and there is a moderate to high clinical suspicion for IE, proceed with a TEE.
Subsequent Actions & Unique Considerations
Further imaging of the chest, abdomen, spine, or brain is necessary if emboli, abscesses, or mycotic aneurysms are suspected. Diagnostic Procedures and Additional Methods Acquire an EKG to determine a baseline heart rhythm and detect any conduction abnormalities. A repeat EKG is indicated for alterations in clinical status, bradycardia, syncope, or presyncope. Pathological Observations Histopathologic investigation reveals that vegetations comprise fibrin, platelet aggregates, and bacterial or fungal masses. PCR-based assays for detecting organisms such as Bartonella spp. and T. whippleii in blood or valvular tissue are accessible at some laboratories.
DIFFERENTIAL DIAGNOSIS
Noninfective endocarditis, alternative systemic infection, bacteremia, or fungemia absent of infective endocarditis.
Treatment Medication
Extended antibacterial treatment is necessary to infiltrate the vegetation and avert recurrence. Identifying the causative organism and its therapeutic susceptibilities is essential. Empiric therapy is predicated on patient risk factors for diverse infections, the severity of sickness, and local resistance patterns. • Below are the recommended treatment regimens for specific pathogens (1). • Penicillin-susceptible Viridans streptococci, S. bovis, or other streptococci (minimum inhibitory concentration ≤0.12 μg/mL) – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks. – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily, in addition to gentamicin 3 mg/kg/day in a single dose for 2 weeks. – Vancomycin 30 mg/kg/day in 2 divided doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Streptococci exhibit relative resistance to penicillin (MIC >0.12 μg/mL or ≤0.5 μg/mL) – Penicillin G 24 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks, in conjunction with gentamicin 3 mg/kg daily in a single dosage for 2 weeks. – Vancomycin 30 mg/kg daily in 2 split doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Penicillin-resistant streptococci (MIC >0.5 μg/mL) and enterococci: - Administer ampicillin 12 g/day in 6 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 4–6 weeks. - If allergic to ampicillin, use vancomycin 30 mg/kg/day in 2 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 6 weeks. • Methicillin-susceptible S. aureus: - Administer nafcillin 12 g/day IV in 4–6 divided doses for 6 weeks, optionally with gentamicin 3 mg/kg/day in 2 or 3 divided doses for 3–5 days. - If allergic to penicillin (without anaphylactoid reactions) but tolerant of cephalosporins, use cefazolin 6 g/day in 3 divided doses for 6 weeks. • Methicillin-resistant S. aureus: - Administer vancomycin 30 mg/kg/day in 2 divided doses for 6 weeks. • Target vancomycin trough level is 15–20 μg/mL. The aforementioned doses are predicated on standard renal function.
SUPPLEMENTARY THERAPY
Concerns for Referral Infective endocarditis of native valves and its complications can be fatal, and intricate management challenges frequently arise. A multidisciplinary approach involving cardiology, cardiovascular surgery, and infectious diseases is advised.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Approximately 30–50% of individuals with NVIE receive a combination of antibacterial and surgical interventions for IE. Patients with decompensated heart failure must be promptly assessed for the possibility of early surgical intervention. The timing and urgency of valve replacement are tailored to each patient with NVIE. Other potential criteria for valve replacement encompass substantial valvular dysfunction, uncontrolled infection, multiple severe systemic emboli, insufficient antibiotic therapy (very resistant bacteria), and cardiac consequences such as perivalvular or myocardial abscesses.
INPATIENT CONSIDERATIONS
Preliminary Stabilization Evaluate and stabilize the respiratory and cardiovascular systems in cases of suspected acute endocarditis. A prompt assessment of volume status and heart rhythm is necessary. Criteria for Admission Patients diagnosed with endocarditis require hospitalization for observation, commencement of intravenous antibiotics, and prompt evaluation. Criteria for Discharge Patients may be discharged when fevers have subsided for over 24 hours, vital signs are stable, and antibiotic and follow-up protocols are established.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
• In the immediate term, monitor patients diligently for complications or recurrence of endocarditis and adverse reactions associated with antimicrobial treatment. • Upon conclusion of therapy for infective endocarditis, a transthoracic echocardiogram is advised to establish a new baseline of valve and heart function. Patient Monitoring For patients undergoing intravenous antibiotic treatment, do weekly laboratory monitoring in accordance with established guidelines (http://www.idsociety.org/content.aspx?id=4428#opat) or the package insert.
INFORMATION FOR PATIENTS
Patients with infective endocarditis require knowledge regarding the significance of proper oral hygiene, methods to prevent infective endocarditis related to dental treatments, and the symptoms and signs of valve dysfunction.
PROGNOSIS • Congestive heart failure, infection extension beyond the valve annulus, concomitant diseases, advanced age, immunosuppression, and S. aureus infection are correlated with elevated mortality rates. Infection with Viridians group streptococci is linked to reduced mortality. • In-hospital mortality linked to infective endocarditis is reduced in drug abusers (10% vs to 17% in a recent research). The one-year mortality rate for all individuals with infective endocarditis is approximately 40%.
COMPLICATIONS
Congestive heart failure, cerebral emboli, stroke, renal infarctions, immune complex glomerulonephritis, mycotic aneurysm, meningitis, cerebritis, splenic infarctions, splenic abscess, and pulmonary embolism with or without infarction in right-sided endocarditis.
Endocarditis is an infection of the heart valves or endocardium caused by bacteria, fungus, or, less commonly, chlamydiae or rickettsiae. The mitral valve (41%) and aortic valve (38%) are the most frequently implicated in native valve infective endocarditis (NVIE). Tricuspid valve endocarditis is more prevalent among intravenous drug users. Pulmonic valve endocarditis is exceedingly uncommon. Several valves may be affected.
EPIDEMIOLOGY Incidence The prevalence of NVIE is between 1.7–6.2 cases per 100,000 patient-years. The incidence among intravenous drug users is estimated to be 1500–3300 cases per 100,000 patient-years.
Risk Factors
Predisposing factors encompass active intravenous drug use, a history of endocarditis, chronic intravascular access, the presence of an implantable cardiac device, congenital heart anomalies, a bicuspid aortic valve, rheumatic heart disease, and degenerative valvular disease.
GENERAL PREVENTION • Antibiotic prophylaxis for endocarditis is advised for people with the following conditions: – Prosthetic heart valve or valve repair utilizing prosthetic material – History of endocarditis - Congenital heart disease (unrepaired cyanotic CHD, treated CHD with residual abnormality) - Recipients of cardiac transplants with valvular heart disease
Prophylaxis is advised for dental procedures that include disruption of the oral mucosa and manipulation of the gingiva.
Prophylaxis is advisable for individuals with high-risk disorders, as previously mentioned, who are undergoing procedures involving the respiratory tract, skin, soft tissue, or muscle. Antibiotics for the prophylaxis of infective endocarditis are not advised for gastrointestinal or genitourinary surgeries.
Antibiotic protocols consist of a single dosage of amoxicillin 2 g or clindamycin 600 mg administered 30–60 minutes before the surgery.
ETIOLOGY • The predominant causal pathogens are gram-positive bacteria. Staphylococcus aureus has recently emerged as the predominant cause of NVIE. • The prevalent microbiological etiologies for NVIE are enumerated below: S. aureus (25–35%) — Coagulase-negative Staphylococcus (3–11%) - Viridans group streptococci (17–40 percent) - Streptococcus bovis (6 percent) - Additional streptococcus (6–19%) - Enterococcus species (10–18%) - HACEK (2–5 percent) Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella species. - Fungi/yeast (2–4 percent) • Culture-negative endocarditis (10%) The predominant cause is the administration of antibiotics within the preceding 7 days. – Alternative potential etiologies encompass slow-growing fastidious anaerobes, non-Candida fungal species, Bartonella spp., Coxiella burnetii (Q fever), Legionella spp., Tropheryma whippelii, Chlamydia spp., and Brucella spp. In intravenous drug users, polymicrobial non-valvular infective endocarditis (NVIE) is more prevalent.
DIAGNOSIS HISTORY
The clinical manifestations of NVIE exhibit significant variability, encompassing symptoms and indications attributable to the infected valve, embolic events, metastatic infection locations, and circulating immune complexes. Fever occurs in more than 90% of people with NVIE. General symptoms including weakness, chills, diaphoresis, anorexia, weight loss, nausea, and malaise may occur (3). • The revised Duke criteria are extensively utilized diagnostic standards for NVIE. • Principal criteria: – Microbiological evidence includes two sets of blood cultures positive for typical microorganisms such as Viridans streptococci, S. bovis, HACEK group, S. aureus; or community-acquired enterococci without a primary focus; or microorganisms consistent with infective endocarditis from persistently positive blood cultures; or a single positive blood culture for Coxiella burnetii or an anti-phase 1 IgG antibody titer exceeding 1:800. - Indications of endocardial involvement Favorable echocardiography (oscillating intracardiac mass on valve, abscess, or fresh partial dehiscence of prosthetic valve) New valvular regurgitation (deterioration or alteration of a preexisting murmur is inadequate)
• Minor criterion – Predisposition, preexisting cardiac disease, or intravenous drug use (IDU) – Pyrexia – Vascular manifestations: Significant artery emboli, septic pulmonary infarcts, mycotic aneurysms, cerebral hemorrhage, conjunctival hemorrhages, and Janeway lesions - Immunological manifestations: Glomerulonephritis, Osler's nodes, Roth's spots, and rheumatoid factor - Microbiological evidence: Positive blood culture; however, it does not fulfill a significant requirement as previously indicated, nor is there serological evidence of current infection with an organism consistent with infective endocarditis. • Definitive endocarditis (clinical criteria): 2 main criteria; or 1 major criterion in conjunction with 3 minor criteria; or 5 minor criteria • Conclusive endocarditis (pathological criteria): Microorganisms discovered through culture or pathological study of vegetation, embolized vegetation, or intracardiac abscess; or vegetation or intracardiac abscess exhibiting active endocarditis via histological evaluation. • Potential endocarditis: 1 major criterion + 1 minor criterion; or 3 minor criteria • Rejected: Definitive alternative diagnosis; symptom remission within 4 days of antibiotic treatment; absence of pathological evidence of infective endocarditis during surgery after fewer than 4 days of antibiotics; does not fulfill clinical criteria for probable infective endocarditis.
PHYSICAL EXAM • Clinical manifestations of infective endocarditis (IE) may present as a new or altered murmur in up to 85% of cases. • Petechiae occur in 20–40% of patients. Other cutaneous manifestations (Osler nodes, Janeway lesions, splinter hemorrhages) or Roth spots are observed in a minority of patients. A comprehensive examination is necessary to detect further infection sites (epidural abscess, psoas abscess, septic arthritis) or to discover embolic occurrences (stroke).
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Preliminary laboratory assessments In cases of suspected NVIE, the initial laboratory assessment include a full blood count with differential, electrolytes, blood urea nitrogen, creatinine, liver function tests, several sets of blood cultures, urinalysis, and erythrocyte sedimentation rate (ESR). • Within the initial 24 hours, get a minimum of 3 sets of blood cultures. Obtain multiple sets of blood cultures prior to administering antibiotics to enhance the likelihood of identifying the causal bacteria. The initial two sets yield positive results in up to 90% of patients. Leukocytosis is prevalent. Over fifty percent of patients exhibit elevated serum inflammatory markers (ESR, C-reactive protein). The urinalysis often indicates the presence of proteinuria or microscopic hematuria.
Subsequent Actions & Unique Considerations
• In instances of culture-negative endocarditis, serological assessment for uncommon pathogens such as Q fever and Bartonella spp. may be warranted. • Acquire two sets of blood cultures every 24 to 48 hours until the endovascular infection has resolved. Imaging: Preliminary Approach Echocardiography is the preferred imaging modality and should be conducted promptly in all instances of suspected NVIE.
• The sensitivity of transthoracic echocardiography (TTE) for identifying left-sided vegetations varies between 40% and 63%, with a specificity of 91% to 98%. The sensitivity for right-sided lesions is elevated due to the proximity of the tricuspid and pulmonic valves to the chest wall. Transesophageal echocardiography may be constrained by obesity, chronic pulmonary illness, or thoracic wall deformities.
Transesophageal echocardiography (TEE) exhibits a sensitivity of 90–100% and a specificity of 91–98% in the identification of vegetations. TEE exhibits greater sensitivity than TTE in detecting valve perforation, pacemaker-associated infective endocarditis, and cardiac abscess.
Transesophageal echocardiography (TEE) is advised as the primary diagnostic test when transthoracic echocardiography (TTE) is anticipated to yield suboptimal results, there is a strong clinical suspicion of infective endocarditis (IE), or perivalvular extension is predicted. If the initial TTE is negative and there is a moderate to high clinical suspicion for IE, proceed with a TEE.
Subsequent Actions & Unique Considerations
Further imaging of the chest, abdomen, spine, or brain is necessary if emboli, abscesses, or mycotic aneurysms are suspected. Diagnostic Procedures and Additional Methods Acquire an EKG to determine a baseline heart rhythm and detect any conduction abnormalities. A repeat EKG is indicated for alterations in clinical status, bradycardia, syncope, or presyncope. Pathological Observations Histopathologic investigation reveals that vegetations comprise fibrin, platelet aggregates, and bacterial or fungal masses. PCR-based assays for detecting organisms such as Bartonella spp. and T. whippleii in blood or valvular tissue are accessible at some laboratories.
DIFFERENTIAL DIAGNOSIS
Noninfective endocarditis, alternative systemic infection, bacteremia, or fungemia absent of infective endocarditis.
Treatment Medication
Extended antibacterial treatment is necessary to infiltrate the vegetation and avert recurrence. Identifying the causative organism and its therapeutic susceptibilities is essential. Empiric therapy is predicated on patient risk factors for diverse infections, the severity of sickness, and local resistance patterns. • Below are the recommended treatment regimens for specific pathogens (1). • Penicillin-susceptible Viridans streptococci, S. bovis, or other streptococci (minimum inhibitory concentration ≤0.12 μg/mL) – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks. – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily, in addition to gentamicin 3 mg/kg/day in a single dose for 2 weeks. – Vancomycin 30 mg/kg/day in 2 divided doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Streptococci exhibit relative resistance to penicillin (MIC >0.12 μg/mL or ≤0.5 μg/mL) – Penicillin G 24 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks, in conjunction with gentamicin 3 mg/kg daily in a single dosage for 2 weeks. – Vancomycin 30 mg/kg daily in 2 split doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Penicillin-resistant streptococci (MIC >0.5 μg/mL) and enterococci: - Administer ampicillin 12 g/day in 6 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 4–6 weeks. - If allergic to ampicillin, use vancomycin 30 mg/kg/day in 2 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 6 weeks. • Methicillin-susceptible S. aureus: - Administer nafcillin 12 g/day IV in 4–6 divided doses for 6 weeks, optionally with gentamicin 3 mg/kg/day in 2 or 3 divided doses for 3–5 days. - If allergic to penicillin (without anaphylactoid reactions) but tolerant of cephalosporins, use cefazolin 6 g/day in 3 divided doses for 6 weeks. • Methicillin-resistant S. aureus: - Administer vancomycin 30 mg/kg/day in 2 divided doses for 6 weeks. • Target vancomycin trough level is 15–20 μg/mL. The aforementioned doses are predicated on standard renal function.
SUPPLEMENTARY THERAPY
Concerns for Referral Infective endocarditis of native valves and its complications can be fatal, and intricate management challenges frequently arise. A multidisciplinary approach involving cardiology, cardiovascular surgery, and infectious diseases is advised.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Approximately 30–50% of individuals with NVIE receive a combination of antibacterial and surgical interventions for IE. Patients with decompensated heart failure must be promptly assessed for the possibility of early surgical intervention. The timing and urgency of valve replacement are tailored to each patient with NVIE. Other potential criteria for valve replacement encompass substantial valvular dysfunction, uncontrolled infection, multiple severe systemic emboli, insufficient antibiotic therapy (very resistant bacteria), and cardiac consequences such as perivalvular or myocardial abscesses.
INPATIENT CONSIDERATIONS
Preliminary Stabilization Evaluate and stabilize the respiratory and cardiovascular systems in cases of suspected acute endocarditis. A prompt assessment of volume status and heart rhythm is necessary. Criteria for Admission Patients diagnosed with endocarditis require hospitalization for observation, commencement of intravenous antibiotics, and prompt evaluation. Criteria for Discharge Patients may be discharged when fevers have subsided for over 24 hours, vital signs are stable, and antibiotic and follow-up protocols are established.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
• In the immediate term, monitor patients diligently for complications or recurrence of endocarditis and adverse reactions associated with antimicrobial treatment. • Upon conclusion of therapy for infective endocarditis, a transthoracic echocardiogram is advised to establish a new baseline of valve and heart function. Patient Monitoring For patients undergoing intravenous antibiotic treatment, do weekly laboratory monitoring in accordance with established guidelines (http://www.idsociety.org/content.aspx?id=4428#opat) or the package insert.
INFORMATION FOR PATIENTS
Patients with infective endocarditis require knowledge regarding the significance of proper oral hygiene, methods to prevent infective endocarditis related to dental treatments, and the symptoms and signs of valve dysfunction.
PROGNOSIS • Congestive heart failure, infection extension beyond the valve annulus, concomitant diseases, advanced age, immunosuppression, and S. aureus infection are correlated with elevated mortality rates. Infection with Viridians group streptococci is linked to reduced mortality. • In-hospital mortality linked to infective endocarditis is reduced in drug abusers (10% vs to 17% in a recent research). The one-year mortality rate for all individuals with infective endocarditis is approximately 40%.
COMPLICATIONS
Congestive heart failure, cerebral emboli, stroke, renal infarctions, immune complex glomerulonephritis, mycotic aneurysm, meningitis, cerebritis, splenic infarctions, splenic abscess, and pulmonary embolism with or without infarction in right-sided endocarditis.
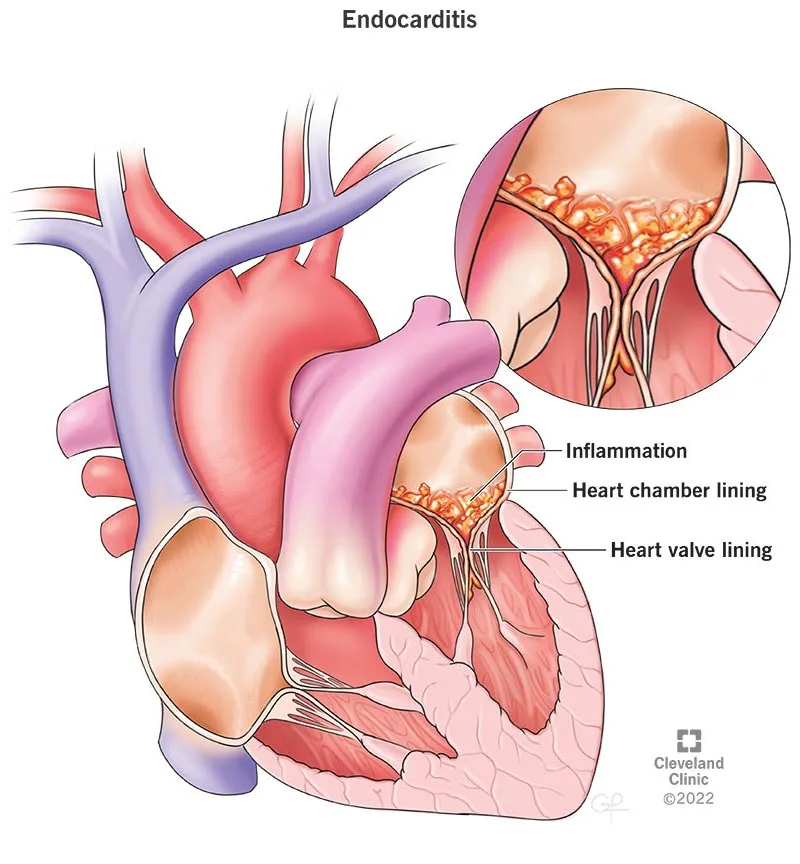
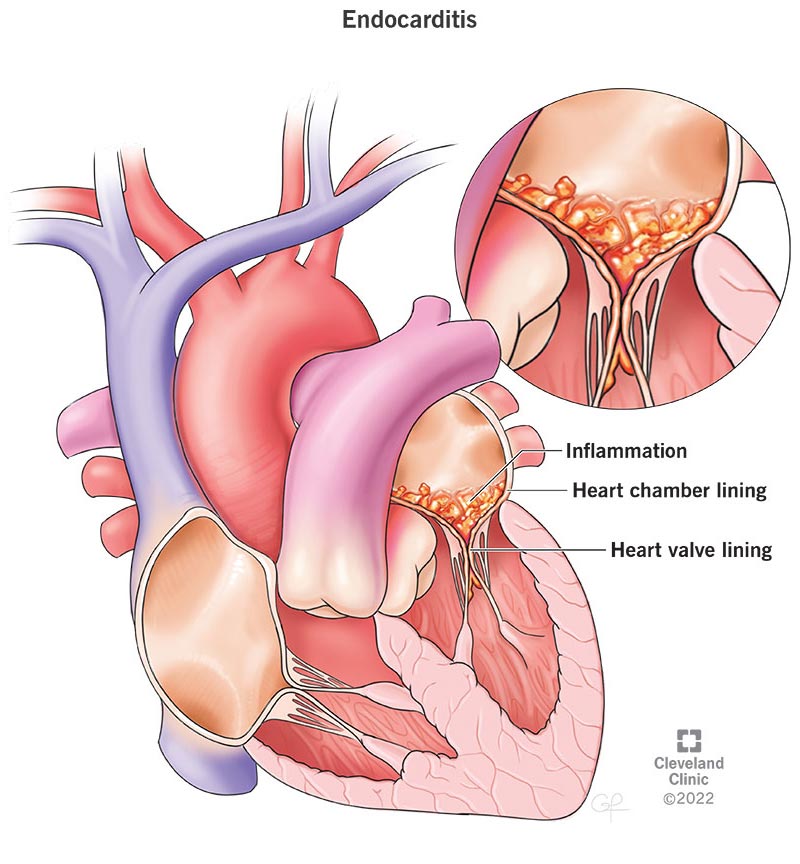
- Published on
Infectious Disease - Encephalitis
ENCEPHALITIS
BASICS DESCRIPTION
Viruses, bacteria, fungi, and protozoa are among the infectious organisms that can cause encephalitis, which is an inflammation of the brain parenchyma that results in neurological symptoms. Any of these organisms can infect the central nervous system and cause encephalitis, mainly through hematogenous dissemination. Fever, disorientation, and headache are common initial symptoms, while seizures are also possible.
The incidence of epidemiology
• The elderly and the young are more likely to be affected by encephalitis.
• Herpes simplex virus (HSV) is the most frequent cause of viral encephalitis in the United States, accounting for 10% of all encephalitis cases. The most frequent cause in newborns is HSV-2, which is contracted during birth.
• Viral encephalitis's yearly incidence (the most
3.5–7.4/100,000 person-years (common etiology), with about 20,000 new cases annually.
RISK ELEMENTS
Age, season (i.e., HSV occurs irregularly throughout the year, while arboviruses are more prevalent in the summer and fall), immunological state, and potential exposures through travel, activities, and contact with animals and insects are risk factors.
OVERALL PREVENTION
• Transmission may be reduced by avoiding tick and mosquito bites.
• Vector control should be taken into consideration in regions where disease is on the rise.
• The risk of enteroviral infections may be reduced by avoiding swimming in ponds in the latter part of the summer.
• Those who live in or want to move to endemic areas should receive the Japanese encephalitis vaccine, which is already available.
• Disease can probably be avoided by avoiding mosquito bites.
• Measles, mumps, rubella, polio, and varicella vaccinations prevent these encephalitis-causing diseases.
Pathophysiology
The particular organism has a significant role in the pathophysiology of infection. Through hematogenous spread, viremia causes the reticuloendothelial system to be seeded, followed by distant locations like the central nervous system. Retrograde peripheral nerve transmission is the cause of infection in rabies encephalitis.
Ethiology
The most prevalent infectious etiology is viral. It is possible to identify no etiologic agent in as many as 75% of cases.
• Viral-Flaviviridae: Powassan virus, Russian spring-summer encephalitis, Central European encephalitis, West Nile virus, Japanese encephalitis virus, and St. Louis encephalitis virus
Togaviridae: Rubella virus, Venezuelan equine encephalitis, Western equine encephalitis, and Eastern equine encephalitis (EEE)
Bunyaviridae: Rift Valley fever, California, and La Crosse - Herpesviridae: HHV6, herpes B virus, varicella zoster virus (VZV), cytomegalovirus (CMV), and HSV The Paramyxoviridae family includes the Hendra, measles, mumps, and Nipah viruses. Other viruses that are frequently thought of include HIV and JC.
• • • •
influenza, mumps, rabies, adenovirus, enteroviridae (coxsackievirus, echovirus, and poliovirus), and Bacteria include Tropheryma whippelii (Whipple's illness), Mycobacterium tuberculosis, Mycoplasma, Listeria monocytogenes, Nocardia, Bartonella bacilliformis (Oroya fever), and Bartonella henselae (cat scratch disease). Ehrlichia chaffeensis (human monocytotropic ehrlichiosis), Coxiella burnetii (Q fever), Anaplasma phagocytophilum (human granulocytotropic ehrlichiosis), and Rickettsia rickettsii (Rocky Mountain spotted fever) are examples of ehrlichiosis and rickettsiosis. Spirochetes: Treponema pallidum (syphilis) and Borrelia burgdorferi (Lyme disease)
Fungal: Candida, Coccidioidomycosis, Cryptococcus neoformans, Aspergillus
Protozoa include Plasmodium falciparum (malaria), Acanthamoeba, Balamuthia mandrillaris, Toxoplasma gondii, and Naegleria fowleri. The trypanosomiasis caused by Trypanosoma brucei gambiense (West Africa) and Trypanosoma brucei rhodesiense (East Africa)
Helminths: Taenia solium (cysticercosis), Gnathostoma species, and Baylisascaris procyonis
History of Diagnosis
The history can be highly instructive, depending on the organism. For instance, the patient's immunological status, recreational activities, insect and animal exposures, travel history, and the incidence of specific diseases in the area can all assist to narrow the differential.
MEDICAL EXAMINATION
• Although a thorough skin examination should be performed to check for rashes, the neurological examination takes up the majority of the physical examination. It might be challenging to differentiate between meningitis and encephalitis due to the possibility of meningeal inflammation causing meningitis symptoms.
• Increased intracranial pressure may result in cranial nerve anomalies and early focal symptoms.
• When they appear, rashes are most useful for diagnosis. There might not be enough proof of tick or mosquito bites.
• Certain etiologies are linked to distinctive
physical manifestations: Lyme disease is linked to anomalies of the cranial nerves; Japanese encephalitis is linked to a movement problem resembling Parkinson's disease:
The temporal lobes are where HSV tends to localize, and patients can exhibit strange behavior as a prodrome.
Initial diagnostic and interpretation lab tests
• Although the white blood cell count (WBC) may be low in viral infections and elevated in bacterial infections, initial laboratory tests, such as the complete blood count (CBC) with differential, are not very useful.
• As soon as a non-contrast head CT scan or clinical examination rules out a space-occupying lesion, a lumbar puncture should be carried out.
• Cell counts, total protein, glucose, bacterial and viral cultures, fungal stain and culture, India ink stain, and HSV 1 and 2 as well as CMV and VZV should all be assessed using polymerase chain reaction (PCR) in cerebrospinal fluid (CSF).
• The usual CSF profile in viral encephalitis will show lymphocytic pleocytosis.
glucose, as well as increased protein. Malaria smears and WBC analysis for morulae in
• If there is a clinical suspicion that a patient may have ehrlichiosis or malaria, ehrlichia should be taken into consideration.
Cultures of non-CNS locations, such as blood, sputum, the nasopharynx, and stool, should be carried out as directed by clinical and epidemiologic guidelines. Serology is frequently used to make the diagnosis. It is important to get both acute and convalescent serologies. A range of PCR-based diagnostics are also available, and serologic testing can be performed in cases of Japanese encephalitis, dengue, and West Nile virus. • More CSF ought to be kept on hand.
Follow-up and Particular Points to Remember
It is recommended to closely monitor patients with specialists, such as those in infectious diseases and neurology.
Imaging To rule out imminent herniation, bleeding, and other problems, brain imaging should be done before lumbar puncture.
• The gold standard is a brain MRI, which every patient should get. For instance, in the instance of HSV
• Temporal lobe lesions, which can be unilateral or bilateral and hemorrhagic, are a characteristic finding in encephalitis. Gray matter involvement may be seen on MRI in cases with Japanese B encephalitis.
Hyperintense lesions in the brainstem are revealed by enterovirus-induced rhombencephalitis.
• When MRI is not accessible, brain CT should be performed. As a non-specific test, it is unable to distinguish between different etiological agents.
Diagnostic Techniques and Other
• The above-described lumbar puncture.
• In certain situations, EEG can be useful. For instance, EEG may show widespread slowing, focal temporal alterations, and PLEDS (periodic complexes and periodic lateralizing epileptiform discharges) in cases of HSV encephalitis. Alpha coma pattern, delta activity with spikes, and diffuse continuous delta activity are all linked to Japanese B encephalitis. Diffuse delta activity is linked to St. Louis encephalitis.
Pathological Results
• Inflammation of cortical arteries in the gray matter or at the gray–white matter junction is observed in viral encephalitis. Necrosis, demyelination, perivascular cuffing, and round cell infiltration are typical.
• There are several distinct histopathologic features for various etiologies, such as Japanese B encephalitis, necrosis in EEE, Negri bodies in rabies, and Cowdry type A inclusion bodies in HSV.
• Certain viruses may exhibit distinct patterns of dispersion. For example, HSV may typically be detected in the pons and temporal lobes, but it can also cause extensive lesions. The temporal lobes are also favored by rabies. The brainstem seems to be preferred by the West Nile virus.
DISTINCTIVE DIAGNOSIS
Acute disseminated encephalomyelitis (ADEM), encephalopathy, brain abscess, bacterial or viral meningitis, and Reye's syndrome
• Toxic metabolic abnormalities • Aseptic meningitis brought on by drugs including metronidazole, ibuprofen, and trimethrim–sulfamethoxazole
Vasculitis, vascular disorders caused by collagen, and paraneoplastic syndromes
MEDICAL CARE
Treatment for both HSV and bacterial meningitis should be part of empirical therapy until bacterial meningitis is ruled out. The empirical regimen should include doxycycline if rickettsial or Ehrlichia infection is suspected.
MEDICATION
• For 14–21 days, acyclovir 10 mg/kg is administered intravenously every 8 hours to treat HSV encephalitis. For neonates, higher doses—20 mg/kg intravenously every 8 hours—are advised.
• Ganciclovir is used to treat CMV encephalitis either by alone or in conjunction with foscarnet.
• HHV6 in immunocompromised hosts is treated with ganciclovir or foscarnet.
In the context of HIV, highly aggressive antiviral therapy (HAART) is recommended as an adjuvant treatment. Other targeted medicines are contingent upon the etiologic agent.
Considering the patient
Requirements for Admission
Hospitalization and specialized care, maybe including intensive care unit (ICU) level care, are necessary for patients suffering from encephalitis.
Intravenous Fluids
Because acyclovir is linked to kidney damage, patients should drink plenty of water while receiving treatment.
Continuing Care Follow-Up Suggestions
Patients' reactions to treatment should be regularly observed. Notably, recovery could be delayed or not happen at all, much like in the case of HSV encephalitis.
Monitoring of Patients
Clinical conditions determine the type and scope of patient monitoring. Long-term effects of the initial illness may be revealed by neuropsychological testing.
Depending on the etiological agent, the prognosis varies. For instance, early diagnosis and treatment commencement can significantly improve outcome in cases with HSV encephalitis. Poorer results are linked to delays in proper therapy.
• Untreated HSV encephalitis has a 70% fatality rate; with treatment, that number drops to 6–19%, with roughly half of survivors experiencing moderate to severe
impairment of the nervous system. Better results are linked to younger ages (less than 30).
COMPLICATIONS
Incorporate death, irreversible neurological impairments, and seizures. Although there is considerable disagreement about whether relapse is a result of a recurring viral infection or the host immune system's reaction to infection, it has been demonstrated that relapse occurs in 5–26% of patients with HSV encephalitis, with some cases perhaps being caused by insufficient therapy.
ENCEPHALITIS
BASICS DESCRIPTION
Viruses, bacteria, fungi, and protozoa are among the infectious organisms that can cause encephalitis, which is an inflammation of the brain parenchyma that results in neurological symptoms. Any of these organisms can infect the central nervous system and cause encephalitis, mainly through hematogenous dissemination. Fever, disorientation, and headache are common initial symptoms, while seizures are also possible.
The incidence of epidemiology
• The elderly and the young are more likely to be affected by encephalitis.
• Herpes simplex virus (HSV) is the most frequent cause of viral encephalitis in the United States, accounting for 10% of all encephalitis cases. The most frequent cause in newborns is HSV-2, which is contracted during birth.
• Viral encephalitis's yearly incidence (the most
3.5–7.4/100,000 person-years (common etiology), with about 20,000 new cases annually.
RISK ELEMENTS
Age, season (i.e., HSV occurs irregularly throughout the year, while arboviruses are more prevalent in the summer and fall), immunological state, and potential exposures through travel, activities, and contact with animals and insects are risk factors.
OVERALL PREVENTION
• Transmission may be reduced by avoiding tick and mosquito bites.
• Vector control should be taken into consideration in regions where disease is on the rise.
• The risk of enteroviral infections may be reduced by avoiding swimming in ponds in the latter part of the summer.
• Those who live in or want to move to endemic areas should receive the Japanese encephalitis vaccine, which is already available.
• Disease can probably be avoided by avoiding mosquito bites.
• Measles, mumps, rubella, polio, and varicella vaccinations prevent these encephalitis-causing diseases.
Pathophysiology
The particular organism has a significant role in the pathophysiology of infection. Through hematogenous spread, viremia causes the reticuloendothelial system to be seeded, followed by distant locations like the central nervous system. Retrograde peripheral nerve transmission is the cause of infection in rabies encephalitis.
Ethiology
The most prevalent infectious etiology is viral. It is possible to identify no etiologic agent in as many as 75% of cases.
• Viral-Flaviviridae: Powassan virus, Russian spring-summer encephalitis, Central European encephalitis, West Nile virus, Japanese encephalitis virus, and St. Louis encephalitis virus
Togaviridae: Rubella virus, Venezuelan equine encephalitis, Western equine encephalitis, and Eastern equine encephalitis (EEE)
Bunyaviridae: Rift Valley fever, California, and La Crosse - Herpesviridae: HHV6, herpes B virus, varicella zoster virus (VZV), cytomegalovirus (CMV), and HSV The Paramyxoviridae family includes the Hendra, measles, mumps, and Nipah viruses. Other viruses that are frequently thought of include HIV and JC.
• • • •
influenza, mumps, rabies, adenovirus, enteroviridae (coxsackievirus, echovirus, and poliovirus), and Bacteria include Tropheryma whippelii (Whipple's illness), Mycobacterium tuberculosis, Mycoplasma, Listeria monocytogenes, Nocardia, Bartonella bacilliformis (Oroya fever), and Bartonella henselae (cat scratch disease). Ehrlichia chaffeensis (human monocytotropic ehrlichiosis), Coxiella burnetii (Q fever), Anaplasma phagocytophilum (human granulocytotropic ehrlichiosis), and Rickettsia rickettsii (Rocky Mountain spotted fever) are examples of ehrlichiosis and rickettsiosis. Spirochetes: Treponema pallidum (syphilis) and Borrelia burgdorferi (Lyme disease)
Fungal: Candida, Coccidioidomycosis, Cryptococcus neoformans, Aspergillus
Protozoa include Plasmodium falciparum (malaria), Acanthamoeba, Balamuthia mandrillaris, Toxoplasma gondii, and Naegleria fowleri. The trypanosomiasis caused by Trypanosoma brucei gambiense (West Africa) and Trypanosoma brucei rhodesiense (East Africa)
Helminths: Taenia solium (cysticercosis), Gnathostoma species, and Baylisascaris procyonis
History of Diagnosis
The history can be highly instructive, depending on the organism. For instance, the patient's immunological status, recreational activities, insect and animal exposures, travel history, and the incidence of specific diseases in the area can all assist to narrow the differential.
MEDICAL EXAMINATION
• Although a thorough skin examination should be performed to check for rashes, the neurological examination takes up the majority of the physical examination. It might be challenging to differentiate between meningitis and encephalitis due to the possibility of meningeal inflammation causing meningitis symptoms.
• Increased intracranial pressure may result in cranial nerve anomalies and early focal symptoms.
• When they appear, rashes are most useful for diagnosis. There might not be enough proof of tick or mosquito bites.
• Certain etiologies are linked to distinctive
physical manifestations: Lyme disease is linked to anomalies of the cranial nerves; Japanese encephalitis is linked to a movement problem resembling Parkinson's disease:
The temporal lobes are where HSV tends to localize, and patients can exhibit strange behavior as a prodrome.
Initial diagnostic and interpretation lab tests
• Although the white blood cell count (WBC) may be low in viral infections and elevated in bacterial infections, initial laboratory tests, such as the complete blood count (CBC) with differential, are not very useful.
• As soon as a non-contrast head CT scan or clinical examination rules out a space-occupying lesion, a lumbar puncture should be carried out.
• Cell counts, total protein, glucose, bacterial and viral cultures, fungal stain and culture, India ink stain, and HSV 1 and 2 as well as CMV and VZV should all be assessed using polymerase chain reaction (PCR) in cerebrospinal fluid (CSF).
• The usual CSF profile in viral encephalitis will show lymphocytic pleocytosis.
glucose, as well as increased protein. Malaria smears and WBC analysis for morulae in
• If there is a clinical suspicion that a patient may have ehrlichiosis or malaria, ehrlichia should be taken into consideration.
Cultures of non-CNS locations, such as blood, sputum, the nasopharynx, and stool, should be carried out as directed by clinical and epidemiologic guidelines. Serology is frequently used to make the diagnosis. It is important to get both acute and convalescent serologies. A range of PCR-based diagnostics are also available, and serologic testing can be performed in cases of Japanese encephalitis, dengue, and West Nile virus. • More CSF ought to be kept on hand.
Follow-up and Particular Points to Remember
It is recommended to closely monitor patients with specialists, such as those in infectious diseases and neurology.
Imaging To rule out imminent herniation, bleeding, and other problems, brain imaging should be done before lumbar puncture.
• The gold standard is a brain MRI, which every patient should get. For instance, in the instance of HSV
• Temporal lobe lesions, which can be unilateral or bilateral and hemorrhagic, are a characteristic finding in encephalitis. Gray matter involvement may be seen on MRI in cases with Japanese B encephalitis.
Hyperintense lesions in the brainstem are revealed by enterovirus-induced rhombencephalitis.
• When MRI is not accessible, brain CT should be performed. As a non-specific test, it is unable to distinguish between different etiological agents.
Diagnostic Techniques and Other
• The above-described lumbar puncture.
• In certain situations, EEG can be useful. For instance, EEG may show widespread slowing, focal temporal alterations, and PLEDS (periodic complexes and periodic lateralizing epileptiform discharges) in cases of HSV encephalitis. Alpha coma pattern, delta activity with spikes, and diffuse continuous delta activity are all linked to Japanese B encephalitis. Diffuse delta activity is linked to St. Louis encephalitis.
Pathological Results
• Inflammation of cortical arteries in the gray matter or at the gray–white matter junction is observed in viral encephalitis. Necrosis, demyelination, perivascular cuffing, and round cell infiltration are typical.
• There are several distinct histopathologic features for various etiologies, such as Japanese B encephalitis, necrosis in EEE, Negri bodies in rabies, and Cowdry type A inclusion bodies in HSV.
• Certain viruses may exhibit distinct patterns of dispersion. For example, HSV may typically be detected in the pons and temporal lobes, but it can also cause extensive lesions. The temporal lobes are also favored by rabies. The brainstem seems to be preferred by the West Nile virus.
DISTINCTIVE DIAGNOSIS
Acute disseminated encephalomyelitis (ADEM), encephalopathy, brain abscess, bacterial or viral meningitis, and Reye's syndrome
• Toxic metabolic abnormalities • Aseptic meningitis brought on by drugs including metronidazole, ibuprofen, and trimethrim–sulfamethoxazole
Vasculitis, vascular disorders caused by collagen, and paraneoplastic syndromes
MEDICAL CARE
Treatment for both HSV and bacterial meningitis should be part of empirical therapy until bacterial meningitis is ruled out. The empirical regimen should include doxycycline if rickettsial or Ehrlichia infection is suspected.
MEDICATION
• For 14–21 days, acyclovir 10 mg/kg is administered intravenously every 8 hours to treat HSV encephalitis. For neonates, higher doses—20 mg/kg intravenously every 8 hours—are advised.
• Ganciclovir is used to treat CMV encephalitis either by alone or in conjunction with foscarnet.
• HHV6 in immunocompromised hosts is treated with ganciclovir or foscarnet.
In the context of HIV, highly aggressive antiviral therapy (HAART) is recommended as an adjuvant treatment. Other targeted medicines are contingent upon the etiologic agent.
Considering the patient
Requirements for Admission
Hospitalization and specialized care, maybe including intensive care unit (ICU) level care, are necessary for patients suffering from encephalitis.
Intravenous Fluids
Because acyclovir is linked to kidney damage, patients should drink plenty of water while receiving treatment.
Continuing Care Follow-Up Suggestions
Patients' reactions to treatment should be regularly observed. Notably, recovery could be delayed or not happen at all, much like in the case of HSV encephalitis.
Monitoring of Patients
Clinical conditions determine the type and scope of patient monitoring. Long-term effects of the initial illness may be revealed by neuropsychological testing.
Depending on the etiological agent, the prognosis varies. For instance, early diagnosis and treatment commencement can significantly improve outcome in cases with HSV encephalitis. Poorer results are linked to delays in proper therapy.
• Untreated HSV encephalitis has a 70% fatality rate; with treatment, that number drops to 6–19%, with roughly half of survivors experiencing moderate to severe
impairment of the nervous system. Better results are linked to younger ages (less than 30).
COMPLICATIONS
Incorporate death, irreversible neurological impairments, and seizures. Although there is considerable disagreement about whether relapse is a result of a recurring viral infection or the host immune system's reaction to infection, it has been demonstrated that relapse occurs in 5–26% of patients with HSV encephalitis, with some cases perhaps being caused by insufficient therapy.

