- Published on
Diagnostic Tests: IGF-1 (Insulin-Like Growth Factor-1)
Diseases for Which IGF-1 Is the Best Initial Test
Serum IGF-1 measurement is the single best initial screening test for acromegaly. Because growth hormone (GH) secretion is pulsatile and varies throughout the day, a random GH level is unreliable. IGF-1 levels, however, are stable and reflect average GH secretion over time, making them ideal for diagnosing GH excess.
What IGF-1 Is
IGF-1 is a somatomedin produced primarily by the liver in response to growth hormone stimulation. In children, IGF-1 mediates linear skeletal growth when GH acts in conjunction with thyroid hormone. In both children and adults, IGF-1 promotes protein synthesis in muscle (anabolic effects) and lipolysis in adipose tissue (catabolic effects). Because IGF-1 has a longer half-life and minimal diurnal variation, it provides a reliable measure of GH activity.
Best Test to Confirm the Diagnosis
The best confirmatory test for acromegaly is the oral glucose tolerance test (OGTT). Under normal conditions, glucose ingestion suppresses GH secretion. In acromegaly, GH levels fail to suppress after glucose administration, confirming autonomous GH production.
Most Common Wrong Answer
The most common incorrect answer for confirming acromegaly is measuring random growth hormone (GH) levels. Because GH is secreted in pulses, a single measurement may be normal despite active disease and should not be used as a confirmatory test.
Diseases for Which IGF-1 Is the Best Initial Test
Serum IGF-1 measurement is the single best initial screening test for acromegaly. Because growth hormone (GH) secretion is pulsatile and varies throughout the day, a random GH level is unreliable. IGF-1 levels, however, are stable and reflect average GH secretion over time, making them ideal for diagnosing GH excess.
What IGF-1 Is
IGF-1 is a somatomedin produced primarily by the liver in response to growth hormone stimulation. In children, IGF-1 mediates linear skeletal growth when GH acts in conjunction with thyroid hormone. In both children and adults, IGF-1 promotes protein synthesis in muscle (anabolic effects) and lipolysis in adipose tissue (catabolic effects). Because IGF-1 has a longer half-life and minimal diurnal variation, it provides a reliable measure of GH activity.
Best Test to Confirm the Diagnosis
The best confirmatory test for acromegaly is the oral glucose tolerance test (OGTT). Under normal conditions, glucose ingestion suppresses GH secretion. In acromegaly, GH levels fail to suppress after glucose administration, confirming autonomous GH production.
Most Common Wrong Answer
The most common incorrect answer for confirming acromegaly is measuring random growth hormone (GH) levels. Because GH is secreted in pulses, a single measurement may be normal despite active disease and should not be used as a confirmatory test.

- Published on
Diagnostic Tests: Beta–Human Chorionic Gonadotropin (β-hCG)
Overview — What This Test Is
Beta–human chorionic gonadotropin (β-hCG) is a hormone produced by the placenta shortly after implantation. Measurement of β-hCG in urine or serum is used to detect pregnancy. Serum testing is more sensitive than urine testing and allows for quantitative measurement, which is useful for monitoring early pregnancy progression and identifying abnormal pregnancies.
When β-hCG Is the Correct Answer
β-hCG is the best initial diagnostic test for any woman of reproductive age who presents with symptoms that could indicate pregnancy or pregnancy-related complications. You should answer β-hCG when the clinical scenario includes:
- Amenorrhea or a missed/delayed period
- Vaginal bleeding
- Lower abdominal or pelvic pain
- Unexplained abdominal pain in a woman of childbearing age
A key exam principle is that any unexplained abdominal pain in a woman of reproductive age should be considered an ectopic pregnancy until proven otherwise, and β-hCG must be obtained first before further imaging or intervention.

- Published on
Diagnostic Tests: C-Peptide
Overview — What This Test Is
The C-peptide test measures the serum level of C-peptide, a byproduct released when proinsulin is cleaved into insulin within pancreatic β-cells. Because C-peptide is secreted only with endogenous insulin and is absent in injected (exogenous) insulin, it is the best test for distinguishing endogenous from exogenous hyperinsulinemia in patients presenting with hypoglycemia.
Interpretation of Low C-Peptide Levels
Low C-peptide levels in the setting of hypoglycemia indicate exogenous insulin administration. In this situation, insulin levels are elevated, but C-peptide is suppressed because the insulin is being injected rather than produced by the pancreas. This finding is classic for factitious hypoglycemia, often due to insulin abuse, and may be seen in patients with psychiatric disease or repeated unexplained hospital visits.
Interpretation of High C-Peptide Levels
High C-peptide levels reflect endogenous insulin production. This occurs when the pancreas is actively secreting insulin, such as in:
In these cases, both insulin and C-peptide levels are elevated during episodes of hypoglycemia.
When to Choose a C-Peptide Level
You should answer C-peptide level when a patient presents with:
In exam questions, C-peptide is the next best diagnostic step to determine the cause of hyperinsulinemic hypoglycemia and to differentiate insulin abuse from endogenous insulin excess.
Overview — What This Test Is
The C-peptide test measures the serum level of C-peptide, a byproduct released when proinsulin is cleaved into insulin within pancreatic β-cells. Because C-peptide is secreted only with endogenous insulin and is absent in injected (exogenous) insulin, it is the best test for distinguishing endogenous from exogenous hyperinsulinemia in patients presenting with hypoglycemia.
Interpretation of Low C-Peptide Levels
Low C-peptide levels in the setting of hypoglycemia indicate exogenous insulin administration. In this situation, insulin levels are elevated, but C-peptide is suppressed because the insulin is being injected rather than produced by the pancreas. This finding is classic for factitious hypoglycemia, often due to insulin abuse, and may be seen in patients with psychiatric disease or repeated unexplained hospital visits.
Interpretation of High C-Peptide Levels
High C-peptide levels reflect endogenous insulin production. This occurs when the pancreas is actively secreting insulin, such as in:
- Insulinoma
- Sulfonylurea use, which stimulates pancreatic insulin release
In these cases, both insulin and C-peptide levels are elevated during episodes of hypoglycemia.
When to Choose a C-Peptide Level
You should answer C-peptide level when a patient presents with:
- Unexplained hypoglycemia
- Elevated insulin levels
- Recurrent or unexplained hospital admissions
- Suspicion of factitious disorder or insulin-secreting tumor
In exam questions, C-peptide is the next best diagnostic step to determine the cause of hyperinsulinemic hypoglycemia and to differentiate insulin abuse from endogenous insulin excess.
- Published on
Diagnostic Tests: Prenatal Screening
Routine Prenatal Screening Tests
Basic prenatal screening is recommended for all pregnancies to assess maternal health, identify infectious risks, and evaluate fetal development. These tests are part of standard obstetric care and are not dependent on maternal age or risk status. Routine prenatal screening includes cervical cytology, a complete blood count (CBC), and urinalysis to detect anemia, infection, or renal abnormalities. Maternal blood testing also includes blood group, Rh factor, and antibody screening to prevent hemolytic disease of the newborn, along with serologic testing for syphilis and assessment of rubella immunity.
Additional routine evaluations include glucose screening for gestational diabetes and fetal ultrasound for pregnancy dating, growth monitoring, and anatomic assessment. Cervical cultures are obtained to screen for Neisseria gonorrhoeae, Chlamydia trachomatis, and Group B Streptococcus, which are important causes of maternal and neonatal infection.
High-Risk Pregnancies and Mothers Over Age 35
In high-risk pregnancies, particularly in women 35 years of age or older, additional testing is required because of the increased risk of chromosomal abnormalities. In these cases, the appropriate diagnostic approach is chromosomal screening for fetal abnormalities.
On exams, when the clinical stem emphasizes advanced maternal age or otherwise labels the pregnancy as high risk, the correct answer is chromosomal screening, rather than repeating routine prenatal laboratory tests.
.
Routine Prenatal Screening Tests
Basic prenatal screening is recommended for all pregnancies to assess maternal health, identify infectious risks, and evaluate fetal development. These tests are part of standard obstetric care and are not dependent on maternal age or risk status. Routine prenatal screening includes cervical cytology, a complete blood count (CBC), and urinalysis to detect anemia, infection, or renal abnormalities. Maternal blood testing also includes blood group, Rh factor, and antibody screening to prevent hemolytic disease of the newborn, along with serologic testing for syphilis and assessment of rubella immunity.
Additional routine evaluations include glucose screening for gestational diabetes and fetal ultrasound for pregnancy dating, growth monitoring, and anatomic assessment. Cervical cultures are obtained to screen for Neisseria gonorrhoeae, Chlamydia trachomatis, and Group B Streptococcus, which are important causes of maternal and neonatal infection.
High-Risk Pregnancies and Mothers Over Age 35
In high-risk pregnancies, particularly in women 35 years of age or older, additional testing is required because of the increased risk of chromosomal abnormalities. In these cases, the appropriate diagnostic approach is chromosomal screening for fetal abnormalities.
On exams, when the clinical stem emphasizes advanced maternal age or otherwise labels the pregnancy as high risk, the correct answer is chromosomal screening, rather than repeating routine prenatal laboratory tests.
.

- Published on
Diagnostic Tests: Diagnostic Abdominal Laparoscopy (DAL)
Overview — What This Test Is
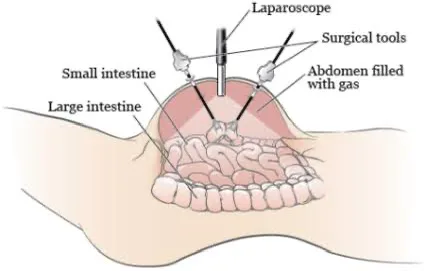
Diagnostic abdominal laparoscopy (DAL) is a minimally invasive surgical procedure that allows direct visualization of intra-abdominal structures using a laparoscope inserted through small abdominal incisions. Because it permits real-time inspection of organs, DAL is highly accurate when noninvasive tests fail to provide a clear diagnosis. It can also guide immediate management decisions and, in some cases, allow therapeutic intervention.
DAL is particularly useful in evaluating conditions where imaging or biopsy results are inconclusive and where a full exploratory laparotomy may be unnecessarily invasive.
Non-Trauma Indications for DAL
Diagnostic abdominal laparoscopy is used for direct evaluation in several non-trauma scenarios, including:
In these cases, DAL provides superior anatomic detail compared with imaging alone.
When to Answer DAL in Trauma Patients
In trauma settings, DAL is indicated in hemodynamically stable patients as a less invasive alternative to exploratory laparotomy. It is especially valuable when:
DAL is particularly useful for detecting diaphragmatic injuries, which are often difficult to identify on CT imaging alone.
A classic scenario is a motor vehicle accident victim with persistent concern for abdominal injury despite inconclusive imaging studies.
Overview — What This Test Is
Diagnostic abdominal laparoscopy (DAL) is a minimally invasive surgical procedure that allows direct visualization of intra-abdominal structures using a laparoscope inserted through small abdominal incisions. Because it permits real-time inspection of organs, DAL is highly accurate when noninvasive tests fail to provide a clear diagnosis. It can also guide immediate management decisions and, in some cases, allow therapeutic intervention.
DAL is particularly useful in evaluating conditions where imaging or biopsy results are inconclusive and where a full exploratory laparotomy may be unnecessarily invasive.
Non-Trauma Indications for DAL
Diagnostic abdominal laparoscopy is used for direct evaluation in several non-trauma scenarios, including:
- Ascites of unclear etiology, when fluid analysis and imaging are nondiagnostic
- Liver disease with an inconclusive biopsy, allowing direct inspection and targeted sampling
- Staging of abdominal malignancies, to assess tumor spread and operability
In these cases, DAL provides superior anatomic detail compared with imaging alone.
When to Answer DAL in Trauma Patients
In trauma settings, DAL is indicated in hemodynamically stable patients as a less invasive alternative to exploratory laparotomy. It is especially valuable when:
- The patient has suffered blunt or penetrating trauma
- Abdominal CT scan is nondiagnostic or equivocal
- There is ongoing suspicion of intra-abdominal organ injury
DAL is particularly useful for detecting diaphragmatic injuries, which are often difficult to identify on CT imaging alone.
A classic scenario is a motor vehicle accident victim with persistent concern for abdominal injury despite inconclusive imaging studies.
- Published on
Diagnostic Tests: Diagnostic Peritoneal Lavage (DPL)
When to Answer DPL
Diagnostic peritoneal lavage is indicated in the setting of blunt abdominal trauma when the patient is hemodynamically unstable or unconscious and the abdomen cannot be reliably examined. The classic scenario is a comatose or intoxicated trauma patient with multiple injuries and unexplained shock, where rapid determination of intra-abdominal bleeding is required. In this procedure, a catheter is placed into the peritoneal cavity, saline is infused, then aspirated and analyzed for evidence of injury.
Patients in Whom DPL Should NOT Be Used
DPL is not appropriate in several important clinical situations:
Findings That Make DPL Positive
A DPL is considered positive when any of the following are found in the aspirated fluid:
Any of these findings indicates significant intra-abdominal injury requiring surgical intervention.
What DPL Misses
A major limitation of DPL is that it is inadequate for detecting retroperitoneal injuries. Injuries to retroperitoneal structures such as the pancreas, kidneys, duodenum, or great vessels may be missed, making CT imaging superior in stable patients.
When to Answer DPL
Diagnostic peritoneal lavage is indicated in the setting of blunt abdominal trauma when the patient is hemodynamically unstable or unconscious and the abdomen cannot be reliably examined. The classic scenario is a comatose or intoxicated trauma patient with multiple injuries and unexplained shock, where rapid determination of intra-abdominal bleeding is required. In this procedure, a catheter is placed into the peritoneal cavity, saline is infused, then aspirated and analyzed for evidence of injury.
Patients in Whom DPL Should NOT Be Used
DPL is not appropriate in several important clinical situations:
- Patients with signs of an acute abdomen
Any evidence of a perforated viscus or clear intra-abdominal bleeding mandates immediate surgical exploration, not DPL. - Patients with gunshot wounds to the abdomen
Penetrating abdominal trauma from firearms is an indication for direct surgical exploration. - Hemodynamically stable patients with abdominal trauma
If the patient is stable and there are no definitive signs of perforation on physical exam, the correct study is an abdominal CT scan, not DPL.
Findings That Make DPL Positive
A DPL is considered positive when any of the following are found in the aspirated fluid:
- Red blood cells >100,000/mm³
- White blood cells >500/mm³
- Presence of bile
- Presence of feces
Any of these findings indicates significant intra-abdominal injury requiring surgical intervention.
What DPL Misses
A major limitation of DPL is that it is inadequate for detecting retroperitoneal injuries. Injuries to retroperitoneal structures such as the pancreas, kidneys, duodenum, or great vessels may be missed, making CT imaging superior in stable patients.

- Published on
Diagnostic Tests: Pelvic Laparoscopy
Overview — What This Test Is
Pelvic laparoscopy is a minimally invasive surgical procedure that allows direct visualization of pelvic structures through small abdominal incisions using a laparoscope. Because it provides real-time, direct inspection, pelvic laparoscopy is considered the most accurate diagnostic test for several gynecologic conditions, particularly when noninvasive imaging is inconclusive.
It can also be diagnostic and therapeutic, allowing for immediate intervention during the same procedure.
Conditions Best Diagnosed With Pelvic Laparoscopy
Pelvic laparoscopy is the most accurate test for diagnosing:
When Pelvic Laparoscopy Is the Correct Answer
Choose pelvic laparoscopy in high-risk or unclear cases where rapid, definitive diagnosis is required:
In these scenarios, laparoscopy allows immediate confirmation and management of potentially life-threatening or refractory pelvic conditions.
Overview — What This Test Is
Pelvic laparoscopy is a minimally invasive surgical procedure that allows direct visualization of pelvic structures through small abdominal incisions using a laparoscope. Because it provides real-time, direct inspection, pelvic laparoscopy is considered the most accurate diagnostic test for several gynecologic conditions, particularly when noninvasive imaging is inconclusive.
It can also be diagnostic and therapeutic, allowing for immediate intervention during the same procedure.
Conditions Best Diagnosed With Pelvic Laparoscopy
Pelvic laparoscopy is the most accurate test for diagnosing:
- Ectopic pregnancy
- Pelvic inflammatory disease (PID), especially complicated or refractory cases
- Endometriosis
- Ovarian or pelvic cysts
- Chronic pelvic pain of unclear etiology
When Pelvic Laparoscopy Is the Correct Answer
Choose pelvic laparoscopy in high-risk or unclear cases where rapid, definitive diagnosis is required:
- Pelvic pain with vaginal bleeding and a positive β-hCG, particularly when:
- The β-hCG level is lower than expected for the estimated gestational age
- There is concern for ectopic pregnancy
- Persistent lower abdominal pain in a woman treated for PID who shows an incomplete response to antibiotics, and pregnancy has been excluded
In these scenarios, laparoscopy allows immediate confirmation and management of potentially life-threatening or refractory pelvic conditions.

- Published on
Diagnostic Tests: Anti–Basement Membrane (Anti-BM) Antibodies
Overview — What This Is
Anti–basement membrane (anti-BM) antibodies are autoantibodies directed against the glomerular basement membrane (GBM), specifically type IV collagen. Their presence is characteristic of Goodpasture’s syndrome, an autoimmune disorder in which antibodies attack basement membranes in the kidneys and lungs, leading to rapidly progressive disease in both organs.
When This Is the Correct Answer
You should answer anti-BM antibodies when the clinical presentation suggests Goodpasture’s syndrome, classically involving both renal and pulmonary symptoms. Typical findings include:
• Hematuria and hypertension
• Renal insufficiency
• Red blood cells or red cell casts on urinalysis
• Pulmonary symptoms, such as:
• Cough
• Shortness of breath
• Hemoptysis
This combination of glomerulonephritis plus pulmonary hemorrhage is the classic high-yield scenario for anti-BM antibodies.
Most Accurate Diagnostic Test
The most accurate diagnostic test for Goodpasture’s syndrome is a tissue biopsy, either:
• Kidney biopsy, or
• Lung biopsy
Biopsy typically shows linear deposition of IgG along the basement membrane on immunofluorescence, which is diagnostic. While anti-BM antibody testing is highly suggestive, biopsy provides definitive confirmation.
Overview — What This Is
Anti–basement membrane (anti-BM) antibodies are autoantibodies directed against the glomerular basement membrane (GBM), specifically type IV collagen. Their presence is characteristic of Goodpasture’s syndrome, an autoimmune disorder in which antibodies attack basement membranes in the kidneys and lungs, leading to rapidly progressive disease in both organs.
When This Is the Correct Answer
You should answer anti-BM antibodies when the clinical presentation suggests Goodpasture’s syndrome, classically involving both renal and pulmonary symptoms. Typical findings include:
• Hematuria and hypertension
• Renal insufficiency
• Red blood cells or red cell casts on urinalysis
• Pulmonary symptoms, such as:
• Cough
• Shortness of breath
• Hemoptysis
This combination of glomerulonephritis plus pulmonary hemorrhage is the classic high-yield scenario for anti-BM antibodies.
Most Accurate Diagnostic Test
The most accurate diagnostic test for Goodpasture’s syndrome is a tissue biopsy, either:
• Kidney biopsy, or
• Lung biopsy
Biopsy typically shows linear deposition of IgG along the basement membrane on immunofluorescence, which is diagnostic. While anti-BM antibody testing is highly suggestive, biopsy provides definitive confirmation.
- Published on
Diagnostic Tests: Total Complement Level (CH50)
When to Choose CH50 as the Correct Answer
The total complement level (CH50) assay is used to evaluate the functional integrity of the complement system, particularly the classical complement pathway. You should select CH50 when a patient—most often young—presents with recurrent, unexplained bacterial infections despite having otherwise normal immune function.
Typical clinical scenarios include:
An abnormal (low) CH50 indicates an inherited or acquired complement deficiency, prompting further evaluation of specific complement components.
When to Choose CH50 as the Correct Answer
The total complement level (CH50) assay is used to evaluate the functional integrity of the complement system, particularly the classical complement pathway. You should select CH50 when a patient—most often young—presents with recurrent, unexplained bacterial infections despite having otherwise normal immune function.
Typical clinical scenarios include:
- Recurrent pneumonia, meningitis, or sinusitis
- Infections caused by encapsulated organisms, especially:
- Neisseria species
- Streptococcus pneumoniae
- Haemophilus influenzae
- Normal lymphocyte counts
- Normal immunoglobulin levels
An abnormal (low) CH50 indicates an inherited or acquired complement deficiency, prompting further evaluation of specific complement components.

- Published on
Diagnostic Tests: Water Deprivation Test
Overview — What This Test Is For
The water deprivation test is used to evaluate disorders of water balance, specifically to distinguish among the causes of diabetes insipidus (DI). It also provides an objective assessment of patients who present with hypernatremia and excessive urine output, helping determine whether the kidneys are able to appropriately concentrate urine in response to rising serum osmolality.
How the Test Is Performed
In the water deprivation test, all fluid intake is restricted for 12–24 hours under close medical supervision. During this period, clinicians carefully monitor:
As dehydration progresses, normal kidneys should conserve water by producing less, more concentrated urine. If urine remains dilute and high in volume despite increasing serum osmolality, diabetes insipidus is present.
After dehydration, vasopressin (ADH) is administered:
When the Water Deprivation Test Is the Correct Answer
Choose the water deprivation test when a patient presents with:
In such cases, this test is the best initial diagnostic step to confirm diabetes insipidus and determine whether it is central or nephrogenic in origin.
Overview — What This Test Is For
The water deprivation test is used to evaluate disorders of water balance, specifically to distinguish among the causes of diabetes insipidus (DI). It also provides an objective assessment of patients who present with hypernatremia and excessive urine output, helping determine whether the kidneys are able to appropriately concentrate urine in response to rising serum osmolality.
How the Test Is Performed
In the water deprivation test, all fluid intake is restricted for 12–24 hours under close medical supervision. During this period, clinicians carefully monitor:
- Urine volume
- Urine osmolality
- Serum osmolality
- Body weight
As dehydration progresses, normal kidneys should conserve water by producing less, more concentrated urine. If urine remains dilute and high in volume despite increasing serum osmolality, diabetes insipidus is present.
After dehydration, vasopressin (ADH) is administered:
- A decrease in urine volume with increased urine osmolality indicates central DI (ADH deficiency).
- No response to vasopressin indicates nephrogenic DI (renal resistance to ADH).
When the Water Deprivation Test Is the Correct Answer
Choose the water deprivation test when a patient presents with:
- Hypernatremia
- Polyuria (high urine output)
- Inappropriately dilute urine
In such cases, this test is the best initial diagnostic step to confirm diabetes insipidus and determine whether it is central or nephrogenic in origin.

