- Published on
Emergency And Acute Medicine: Hyperparathyroidism
Basics
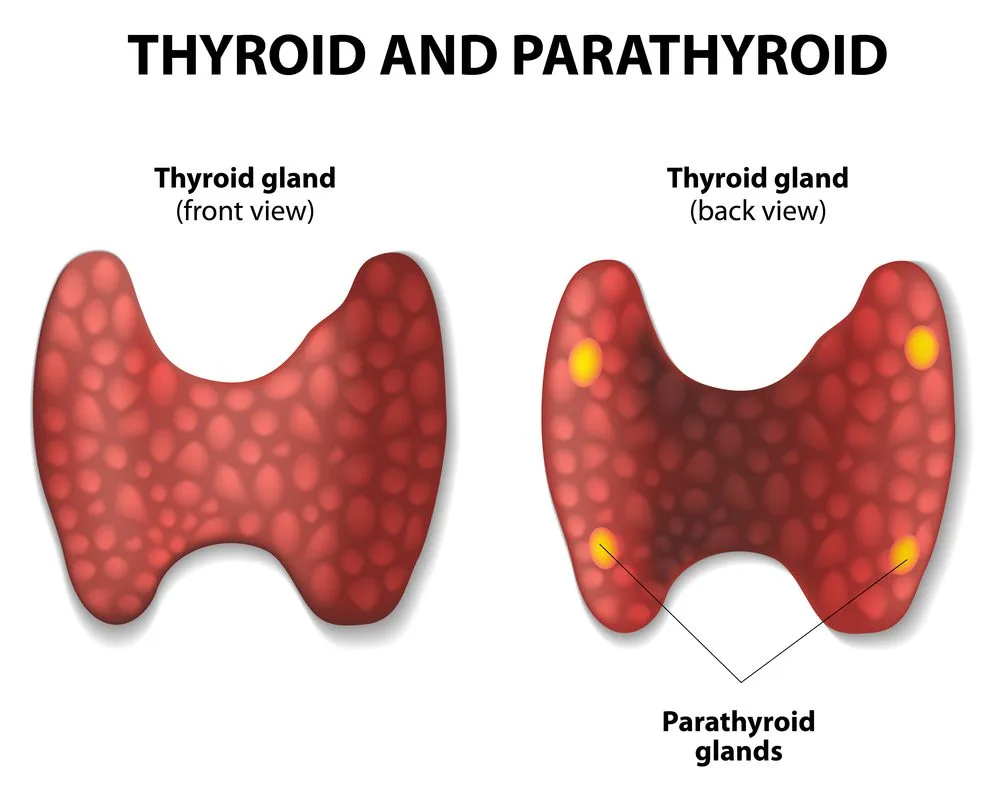
Description Hyperparathyroidism is characterized by excess parathyroid hormone (PTH) leading to metabolic effects including decreased urinary calcium excretion, increased urinary phosphate loss, increased renal conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, and increased calcium and phosphate release from bone. Hypercalcemia is the primary metabolic abnormality. Despite reduced renal calcium excretion, hypercalciuria occurs due to elevated serum calcium, often accompanied by urinary magnesium loss. Magnesium is essential for both PTH secretion and peripheral PTH action; hypomagnesemia may blunt PTH effects. Genetic associations include multiple endocrine neoplasia (MEN) syndromes: MEN 1 (hyperparathyroidism, pancreatic islet tumors, pituitary disease) and MEN 2 (hyperparathyroidism in MEN 2A, medullary thyroid carcinoma, pheochromocytoma, and mucosal neuromas in MEN 2B).
Etiology Primary hyperparathyroidism results from parathyroid adenoma (≈85%), hyperplasia (≈14%), or rarely carcinoma (<1%). Secondary hyperparathyroidism is a compensatory response to vitamin D deficiency or chronic kidney disease with hyperphosphatemia; calcium levels are low or normal with elevated PTH.
Diagnosis
Signs and symptoms Classic features include renal stones, bone pain, gastrointestinal complaints, and neuropsychiatric changes. Alert Hypercalcemic crisis presents with anorexia, nausea, vomiting, and progressive mental status depression.
History Symptoms correlate with severity and rapidity of hypercalcemia.
Pediatric considerations Neonates born to hypoparathyroid mothers may present with hypotonia, weakness, and lethargy; hypercalcemic infants may have distinctive facial features including broad forehead, epicanthal folds, underdeveloped nasal bridge, and prominent upper lip.
Physical exam Findings may include dehydration, hypertension despite volume depletion, cardiac conduction abnormalities (bradyarrhythmias, bundle branch block, complete heart block, asystole), shortened QT interval, potentiation of digoxin toxicity, neurologic deficits (decreased reflexes, proximal weakness, lethargy, coma), psychiatric symptoms (depression, anxiety, psychosis), gastrointestinal symptoms (anorexia, constipation, peptic ulcer disease, pancreatitis), musculoskeletal pain, gout or pseudogout, and renal manifestations including nephrolithiasis and nephrocalcinosis.
Essential workup Measure serum calcium and albumin to assess corrected calcium. Evaluate for symptoms of severe hypercalcemia or impending parathyroid crisis. If asymptomatic with normal ECG and corrected calcium <14 mg/dL, no further ED testing is required. If symptomatic or calcium ≥14 mg/dL, obtain ionized calcium, electrolytes, BUN/creatinine, phosphorus, magnesium, alkaline phosphatase, ESR, TSH, CBC, and chest radiograph.
Diagnosis tests and interpretation
Laboratory Correct calcium for albumin: corrected Ca (mg/dL) = measured Ca + 0.8 × (4 − albumin). Acidosis increases ionized calcium by reducing albumin binding. Phosphorus is typically low in primary hyperparathyroidism and elevated in secondary disease. Chloride-to-phosphate ratio >33 favors hyperparathyroidism; <30 suggests malignancy. Alkaline phosphatase is elevated in ~50% of cases. ESR and anemia are usually normal in hyperparathyroidism but elevated in malignancy or granulomatous disease. Magnesium is often low or low-normal. PTH is elevated in primary and secondary hyperparathyroidism. PTH-related peptide suggests malignancy-associated hypercalcemia.
Imaging Chest radiograph evaluates volume status and screens for malignancy or granulomatous disease.
Diagnostic procedures Definitive diagnosis and treatment are established with parathyroidectomy.
Differential diagnosis PTH-mediated causes include primary or secondary hyperparathyroidism and familial hypocalciuric hypercalcemia. Non-PTH causes include malignancy, vitamin D excess or granulomatous disease, immobilization (e.g., Paget disease), and drug-induced hypercalcemia (thiazides, lithium, vitamin A, aluminum antacids, estrogens, androgens, tamoxifen).
Treatment
Prehospital May present primarily with psychiatric manifestations.
Initial stabilization/therapy Place on cardiac monitor if symptomatic or calcium >14 mg/dL. Begin IV hydration with 0.9% normal saline and correct acidosis.
Emergency department management Treat hypercalcemia with aggressive isotonic saline hydration (≥250 mL/hr unless limited by heart failure) targeting urine output ≥100 mL/hr. After adequate hydration, add loop diuretics to enhance calciuresis; avoid thiazides. Consider glucocorticoids in vitamin D–mediated or granulomatous disease. Initiate bisphosphonates in coordination with endocrinology. Treat dysrhythmias conventionally and use extreme caution with digoxin. Stop contributing medications and monitor closely for heart failure and electrolyte disturbances. Use calcitonin when hydration is contraindicated and initiate dialysis for refractory hypercalcemia with renal failure.
Medication First line Normal saline infusion; furosemide 40 mg IV q2–4h after rehydration; prednisone 40–60 mg PO or hydrocortisone 100 mg IV. Second line (with endocrinology) Calcitonin salmon 4 U/kg SC q12h; pamidronate 60–90 mg IV depending on calcium level; zoledronic acid 4 mg IV; cinacalcet 30 mg PO daily or BID for secondary hyperparathyroidism or carcinoma.
Follow-up and disposition
Admission criteria Corrected calcium >14 mg/dL, symptomatic hypercalcemia, or cardiac conduction abnormalities.
Discharge criteria Asymptomatic patients with calcium <14 mg/dL who can maintain hydration.
Issues for referral Endocrinology referral for PTH evaluation and definitive management.
Follow-up recommendations Arrange outpatient PTH testing, reinforce hydration, and discontinue medications that increase calcium levels.
Key points Hyperparathyroid-related hypercalcemia is often mild and rarely exceeds 14 mg/dL; higher levels suggest malignancy. Measure ionized or albumin-corrected calcium. Administering loop diuretics before adequate hydration worsens hypercalcemia and is a common management error.
Basics
Description Hyperparathyroidism is characterized by excess parathyroid hormone (PTH) leading to metabolic effects including decreased urinary calcium excretion, increased urinary phosphate loss, increased renal conversion of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, and increased calcium and phosphate release from bone. Hypercalcemia is the primary metabolic abnormality. Despite reduced renal calcium excretion, hypercalciuria occurs due to elevated serum calcium, often accompanied by urinary magnesium loss. Magnesium is essential for both PTH secretion and peripheral PTH action; hypomagnesemia may blunt PTH effects. Genetic associations include multiple endocrine neoplasia (MEN) syndromes: MEN 1 (hyperparathyroidism, pancreatic islet tumors, pituitary disease) and MEN 2 (hyperparathyroidism in MEN 2A, medullary thyroid carcinoma, pheochromocytoma, and mucosal neuromas in MEN 2B).
Etiology Primary hyperparathyroidism results from parathyroid adenoma (≈85%), hyperplasia (≈14%), or rarely carcinoma (<1%). Secondary hyperparathyroidism is a compensatory response to vitamin D deficiency or chronic kidney disease with hyperphosphatemia; calcium levels are low or normal with elevated PTH.
Diagnosis
Signs and symptoms Classic features include renal stones, bone pain, gastrointestinal complaints, and neuropsychiatric changes. Alert Hypercalcemic crisis presents with anorexia, nausea, vomiting, and progressive mental status depression.
History Symptoms correlate with severity and rapidity of hypercalcemia.
Pediatric considerations Neonates born to hypoparathyroid mothers may present with hypotonia, weakness, and lethargy; hypercalcemic infants may have distinctive facial features including broad forehead, epicanthal folds, underdeveloped nasal bridge, and prominent upper lip.
Physical exam Findings may include dehydration, hypertension despite volume depletion, cardiac conduction abnormalities (bradyarrhythmias, bundle branch block, complete heart block, asystole), shortened QT interval, potentiation of digoxin toxicity, neurologic deficits (decreased reflexes, proximal weakness, lethargy, coma), psychiatric symptoms (depression, anxiety, psychosis), gastrointestinal symptoms (anorexia, constipation, peptic ulcer disease, pancreatitis), musculoskeletal pain, gout or pseudogout, and renal manifestations including nephrolithiasis and nephrocalcinosis.
Essential workup Measure serum calcium and albumin to assess corrected calcium. Evaluate for symptoms of severe hypercalcemia or impending parathyroid crisis. If asymptomatic with normal ECG and corrected calcium <14 mg/dL, no further ED testing is required. If symptomatic or calcium ≥14 mg/dL, obtain ionized calcium, electrolytes, BUN/creatinine, phosphorus, magnesium, alkaline phosphatase, ESR, TSH, CBC, and chest radiograph.
Diagnosis tests and interpretation
Laboratory Correct calcium for albumin: corrected Ca (mg/dL) = measured Ca + 0.8 × (4 − albumin). Acidosis increases ionized calcium by reducing albumin binding. Phosphorus is typically low in primary hyperparathyroidism and elevated in secondary disease. Chloride-to-phosphate ratio >33 favors hyperparathyroidism; <30 suggests malignancy. Alkaline phosphatase is elevated in ~50% of cases. ESR and anemia are usually normal in hyperparathyroidism but elevated in malignancy or granulomatous disease. Magnesium is often low or low-normal. PTH is elevated in primary and secondary hyperparathyroidism. PTH-related peptide suggests malignancy-associated hypercalcemia.
Imaging Chest radiograph evaluates volume status and screens for malignancy or granulomatous disease.
Diagnostic procedures Definitive diagnosis and treatment are established with parathyroidectomy.
Differential diagnosis PTH-mediated causes include primary or secondary hyperparathyroidism and familial hypocalciuric hypercalcemia. Non-PTH causes include malignancy, vitamin D excess or granulomatous disease, immobilization (e.g., Paget disease), and drug-induced hypercalcemia (thiazides, lithium, vitamin A, aluminum antacids, estrogens, androgens, tamoxifen).
Treatment
Prehospital May present primarily with psychiatric manifestations.
Initial stabilization/therapy Place on cardiac monitor if symptomatic or calcium >14 mg/dL. Begin IV hydration with 0.9% normal saline and correct acidosis.
Emergency department management Treat hypercalcemia with aggressive isotonic saline hydration (≥250 mL/hr unless limited by heart failure) targeting urine output ≥100 mL/hr. After adequate hydration, add loop diuretics to enhance calciuresis; avoid thiazides. Consider glucocorticoids in vitamin D–mediated or granulomatous disease. Initiate bisphosphonates in coordination with endocrinology. Treat dysrhythmias conventionally and use extreme caution with digoxin. Stop contributing medications and monitor closely for heart failure and electrolyte disturbances. Use calcitonin when hydration is contraindicated and initiate dialysis for refractory hypercalcemia with renal failure.
Medication First line Normal saline infusion; furosemide 40 mg IV q2–4h after rehydration; prednisone 40–60 mg PO or hydrocortisone 100 mg IV. Second line (with endocrinology) Calcitonin salmon 4 U/kg SC q12h; pamidronate 60–90 mg IV depending on calcium level; zoledronic acid 4 mg IV; cinacalcet 30 mg PO daily or BID for secondary hyperparathyroidism or carcinoma.
Follow-up and disposition
Admission criteria Corrected calcium >14 mg/dL, symptomatic hypercalcemia, or cardiac conduction abnormalities.
Discharge criteria Asymptomatic patients with calcium <14 mg/dL who can maintain hydration.
Issues for referral Endocrinology referral for PTH evaluation and definitive management.
Follow-up recommendations Arrange outpatient PTH testing, reinforce hydration, and discontinue medications that increase calcium levels.
Key points Hyperparathyroid-related hypercalcemia is often mild and rarely exceeds 14 mg/dL; higher levels suggest malignancy. Measure ionized or albumin-corrected calcium. Administering loop diuretics before adequate hydration worsens hypercalcemia and is a common management error.
- Published on
Emergency And Acute Medicine: Hypertensive Emergencies
Basics
Description Hypertensive crisis refers to severe blood pressure elevation, typically SBP >179 mm Hg or DBP >109 mm Hg. Hypertensive urgency is severe BP elevation without acute end-organ injury. Hypertensive emergency is severe BP elevation with acute target-organ damage. In hypertensive emergency, autoregulation fails: arterioles initially constrict to protect capillary beds, but extreme pressures overwhelm this response, causing endothelial injury, increased permeability, platelet and coagulation activation, and fibrin deposition. Sympathetic and renin–angiotensin activation further increase vasoconstriction and inflammation, worsening ischemia and perpetuating a vicious cycle. Commonly affected organs include brain (encephalopathy, ischemic stroke, intracerebral hemorrhage), retina (hemorrhage, papilledema), heart (ACS, acute heart failure, aortic dissection), kidneys (acute renal failure), and placenta (preeclampsia/eclampsia).
Etiology Causes include essential hypertension; renal vascular or parenchymal disease; coarctation of the aorta; CNS injury (head trauma, stroke/ICH, tumor, spinal cord injury); endocrine disorders (pheochromocytoma, Cushing syndrome, primary hyperaldosteronism, renin-secreting tumors); drugs and toxins (cocaine, PCP, amphetamines, erythropoietin, tacrolimus, cyclosporine, corticosteroids, oral contraceptives, MAOI interactions, lead); withdrawal of antihypertensives; autonomic hyperreactivity (Guillain–Barré, acute intermittent porphyria); postoperative pain or anesthetic complications; and pregnancy-related disease (preeclampsia/eclampsia).
Diagnosis
History Review prescribed and OTC medications, antihypertensive adherence or withdrawal, duration and control of baseline hypertension, prior end-organ disease, comorbidities (CAD, diabetes, obesity), and recreational drug use. Screen for end-organ injury, commonly dyspnea, chest pain, headache, confusion, and focal neurologic deficits.
Physical exam Measure BP in both arms using appropriate cuff size. Assess for neurologic deficits and mental status changes, perform funduscopic exam for hemorrhages or papilledema, evaluate cardiovascular status (JVP, crackles, S3, aortic regurg murmur), and check for pulse asymmetry.
Essential workup Obtain a 12-lead ECG for ischemia and LVH, and assess kidney function because acute renal failure may be clinically silent.
Diagnosis tests and interpretation
Laboratory CBC (anemia and thrombocytopenia may indicate thrombotic microangiopathy), BMP including BUN/creatinine and electrolytes (hypokalemia suggests mineralocorticoid excess), urinalysis (protein, blood, casts), urine toxicology when drug use is suspected, and pregnancy test when appropriate. Use standard chest pain protocols when indicated.
Imaging Chest radiograph for cardiopulmonary symptoms, head CT for headache, confusion, or focal deficits, and CTA chest/abdomen if aortic dissection is suspected.
Procedures Consider arterial line monitoring in unstable cases. Lumbar puncture may be used to evaluate for subarachnoid hemorrhage after appropriate imaging.
Differential diagnosis ACS, acute heart failure, aortic dissection, ischemic stroke, intracerebral hemorrhage, subarachnoid hemorrhage, preeclampsia/eclampsia, withdrawal syndromes (beta-blocker, clonidine), and catecholamine excess states (pheochromocytoma, sympathomimetic intoxication, tyramine reaction with MAOIs).
Treatment
Prehospital Support ABCs and consider cautious BP reduction only when clearly indicated.
Initial stabilization/therapy Provide oxygen as needed, establish IV access, monitor ECG and pulse oximetry.
Emergency department management Hypertensive urgency does not require IV reduction; give missed home medications, use oral agents only, and lower BP gradually over 24–48 hours with close follow-up. Hypertensive emergency requires IV therapy guided by the end-organ injury rather than the absolute BP. Reduce MAP by no more than 20–25% in the first hour, then target roughly SBP ~160 and DBP ~100 over 2–6 hours, transitioning to oral agents within 6–12 hours once stable. Lower more gradually in acute CNS injury, but more rapidly in aortic dissection. Hypertensive encephalopathy: lower MAP up to 20% or DBP to 100–110 within the first hour, then normalize over 48–72 hours using nicardipine, clevidipine, or labetalol. Ischemic stroke: treat only if SBP >220 or DBP >120, or if thrombolysis planned (target <185/110 pre-tPA, then <180/105); avoid reducing MAP more than 15–20% in the first 24 hours; preferred agents are nicardipine, clevidipine, or labetalol. ICH/SAH: treat if SBP >180 or DBP >100; aim SBP 140–160 or MAP down 20–25% in the first hour; avoid nitroglycerin and nitroprusside due to cerebral vasodilation and ICP effects; use nicardipine, clevidipine, or labetalol. ACS: target MAP 60–100 using labetalol or esmolol with nitroglycerin; avoid hydralazine and nitroprusside. Acute heart failure: target MAP 60–100 with nitroprusside or nitroglycerin plus ACE inhibitor and/or loop diuretic. Acute renal failure or microangiopathy: reduce MAP 20–25% in the first hour using nicardipine, clevidipine, or fenoldopam; ACE inhibitors are preferred for scleroderma renal crisis. Aortic dissection: reduce shear force by lowering HR and BP; beta-blockade must come first; target SBP 100–120 and HR <65 within 20 minutes using esmolol plus a vasodilator (dihydropyridine CCB or nitroprusside); obtain urgent surgical consultation for type A.
Sympathomimetic crisis: avoid pure beta-blockade; use phentolamine or calcium channel blocker plus benzodiazepines; use clonidine for clonidine withdrawal.
Pregnancy considerations Preeclampsia is SBP >140 or DBP >90 with proteinuria after 20 weeks to 4 weeks postpartum, often with headache, visual changes, edema, or RUQ pain; target SBP 130–150 and DBP 80–100 using labetalol, nicardipine, hydralazine, and magnesium, with obstetric consultation.
Medication Clevidipine 1–16 mg/h infusion; nicardipine 2–15 mg/h infusion; labetalol 20–80 mg IV q10 min (max 300 mg) or 0.5–2 mg/min infusion; esmolol 80 mg IV bolus then 150 μg/kg/min infusion; nitroglycerin 5–100 μg/min infusion; nitroprusside 0.25–10 μg/kg/min infusion; hydralazine 10–20 mg IV bolus; fenoldopam 0.1–0.6 μg/kg/min infusion; enalaprilat 1.25–5 mg IV q6h; phentolamine 5–15 mg IV q5–15 min.
Follow-up and disposition
Admission criteria Any patient with acute end-organ injury requires admission; ICU monitoring is indicated for hypertensive emergency.
Discharge criteria No end-organ injury, reliable follow-up, known hypertension, reversible trigger such as medication nonadherence, and ability to resume a safe outpatient regimen; provide strict return precautions for chest pain, neurologic symptoms, or severe headache.
Follow-up recommendations Ensure timely primary care follow-up for medication initiation or adjustment and long-term BP control.
Key points Do not use IV agents for hypertensive urgency. In hypertensive emergency, the initial goal is controlled MAP reduction of 20–25% in the first hour, except for ischemic stroke and aortic dissection where targets differ. Avoid precipitous BP drops that can worsen ischemia. In aortic dissection prevent reflex tachycardia by starting beta-blockade first. In catecholamine excess avoid unopposed alpha stimulation by avoiding pure beta-blockers.
Basics
Description Hypertensive crisis refers to severe blood pressure elevation, typically SBP >179 mm Hg or DBP >109 mm Hg. Hypertensive urgency is severe BP elevation without acute end-organ injury. Hypertensive emergency is severe BP elevation with acute target-organ damage. In hypertensive emergency, autoregulation fails: arterioles initially constrict to protect capillary beds, but extreme pressures overwhelm this response, causing endothelial injury, increased permeability, platelet and coagulation activation, and fibrin deposition. Sympathetic and renin–angiotensin activation further increase vasoconstriction and inflammation, worsening ischemia and perpetuating a vicious cycle. Commonly affected organs include brain (encephalopathy, ischemic stroke, intracerebral hemorrhage), retina (hemorrhage, papilledema), heart (ACS, acute heart failure, aortic dissection), kidneys (acute renal failure), and placenta (preeclampsia/eclampsia).
Etiology Causes include essential hypertension; renal vascular or parenchymal disease; coarctation of the aorta; CNS injury (head trauma, stroke/ICH, tumor, spinal cord injury); endocrine disorders (pheochromocytoma, Cushing syndrome, primary hyperaldosteronism, renin-secreting tumors); drugs and toxins (cocaine, PCP, amphetamines, erythropoietin, tacrolimus, cyclosporine, corticosteroids, oral contraceptives, MAOI interactions, lead); withdrawal of antihypertensives; autonomic hyperreactivity (Guillain–Barré, acute intermittent porphyria); postoperative pain or anesthetic complications; and pregnancy-related disease (preeclampsia/eclampsia).
Diagnosis
History Review prescribed and OTC medications, antihypertensive adherence or withdrawal, duration and control of baseline hypertension, prior end-organ disease, comorbidities (CAD, diabetes, obesity), and recreational drug use. Screen for end-organ injury, commonly dyspnea, chest pain, headache, confusion, and focal neurologic deficits.
Physical exam Measure BP in both arms using appropriate cuff size. Assess for neurologic deficits and mental status changes, perform funduscopic exam for hemorrhages or papilledema, evaluate cardiovascular status (JVP, crackles, S3, aortic regurg murmur), and check for pulse asymmetry.
Essential workup Obtain a 12-lead ECG for ischemia and LVH, and assess kidney function because acute renal failure may be clinically silent.
Diagnosis tests and interpretation
Laboratory CBC (anemia and thrombocytopenia may indicate thrombotic microangiopathy), BMP including BUN/creatinine and electrolytes (hypokalemia suggests mineralocorticoid excess), urinalysis (protein, blood, casts), urine toxicology when drug use is suspected, and pregnancy test when appropriate. Use standard chest pain protocols when indicated.
Imaging Chest radiograph for cardiopulmonary symptoms, head CT for headache, confusion, or focal deficits, and CTA chest/abdomen if aortic dissection is suspected.
Procedures Consider arterial line monitoring in unstable cases. Lumbar puncture may be used to evaluate for subarachnoid hemorrhage after appropriate imaging.
Differential diagnosis ACS, acute heart failure, aortic dissection, ischemic stroke, intracerebral hemorrhage, subarachnoid hemorrhage, preeclampsia/eclampsia, withdrawal syndromes (beta-blocker, clonidine), and catecholamine excess states (pheochromocytoma, sympathomimetic intoxication, tyramine reaction with MAOIs).
Treatment
Prehospital Support ABCs and consider cautious BP reduction only when clearly indicated.
Initial stabilization/therapy Provide oxygen as needed, establish IV access, monitor ECG and pulse oximetry.
Emergency department management Hypertensive urgency does not require IV reduction; give missed home medications, use oral agents only, and lower BP gradually over 24–48 hours with close follow-up. Hypertensive emergency requires IV therapy guided by the end-organ injury rather than the absolute BP. Reduce MAP by no more than 20–25% in the first hour, then target roughly SBP ~160 and DBP ~100 over 2–6 hours, transitioning to oral agents within 6–12 hours once stable. Lower more gradually in acute CNS injury, but more rapidly in aortic dissection. Hypertensive encephalopathy: lower MAP up to 20% or DBP to 100–110 within the first hour, then normalize over 48–72 hours using nicardipine, clevidipine, or labetalol. Ischemic stroke: treat only if SBP >220 or DBP >120, or if thrombolysis planned (target <185/110 pre-tPA, then <180/105); avoid reducing MAP more than 15–20% in the first 24 hours; preferred agents are nicardipine, clevidipine, or labetalol. ICH/SAH: treat if SBP >180 or DBP >100; aim SBP 140–160 or MAP down 20–25% in the first hour; avoid nitroglycerin and nitroprusside due to cerebral vasodilation and ICP effects; use nicardipine, clevidipine, or labetalol. ACS: target MAP 60–100 using labetalol or esmolol with nitroglycerin; avoid hydralazine and nitroprusside. Acute heart failure: target MAP 60–100 with nitroprusside or nitroglycerin plus ACE inhibitor and/or loop diuretic. Acute renal failure or microangiopathy: reduce MAP 20–25% in the first hour using nicardipine, clevidipine, or fenoldopam; ACE inhibitors are preferred for scleroderma renal crisis. Aortic dissection: reduce shear force by lowering HR and BP; beta-blockade must come first; target SBP 100–120 and HR <65 within 20 minutes using esmolol plus a vasodilator (dihydropyridine CCB or nitroprusside); obtain urgent surgical consultation for type A.
Sympathomimetic crisis: avoid pure beta-blockade; use phentolamine or calcium channel blocker plus benzodiazepines; use clonidine for clonidine withdrawal.
Pregnancy considerations Preeclampsia is SBP >140 or DBP >90 with proteinuria after 20 weeks to 4 weeks postpartum, often with headache, visual changes, edema, or RUQ pain; target SBP 130–150 and DBP 80–100 using labetalol, nicardipine, hydralazine, and magnesium, with obstetric consultation.
Medication Clevidipine 1–16 mg/h infusion; nicardipine 2–15 mg/h infusion; labetalol 20–80 mg IV q10 min (max 300 mg) or 0.5–2 mg/min infusion; esmolol 80 mg IV bolus then 150 μg/kg/min infusion; nitroglycerin 5–100 μg/min infusion; nitroprusside 0.25–10 μg/kg/min infusion; hydralazine 10–20 mg IV bolus; fenoldopam 0.1–0.6 μg/kg/min infusion; enalaprilat 1.25–5 mg IV q6h; phentolamine 5–15 mg IV q5–15 min.
Follow-up and disposition
Admission criteria Any patient with acute end-organ injury requires admission; ICU monitoring is indicated for hypertensive emergency.
Discharge criteria No end-organ injury, reliable follow-up, known hypertension, reversible trigger such as medication nonadherence, and ability to resume a safe outpatient regimen; provide strict return precautions for chest pain, neurologic symptoms, or severe headache.
Follow-up recommendations Ensure timely primary care follow-up for medication initiation or adjustment and long-term BP control.
Key points Do not use IV agents for hypertensive urgency. In hypertensive emergency, the initial goal is controlled MAP reduction of 20–25% in the first hour, except for ischemic stroke and aortic dissection where targets differ. Avoid precipitous BP drops that can worsen ischemia. In aortic dissection prevent reflex tachycardia by starting beta-blockade first. In catecholamine excess avoid unopposed alpha stimulation by avoiding pure beta-blockers.

- Published on
Emergency And Acute Medicine: Hyperthermia
Basics
Description Hyperthermia represents a spectrum of heat-related illness caused by progressively overwhelming heat stress, ranging from dehydration and electrolyte abnormalities to thermoregulatory failure and multisystem organ dysfunction. Normal body temperature is maintained by balancing heat production and dissipation. At temperatures above 42°C (108°F), oxidative phosphorylation becomes uncoupled and critical enzymes fail. Heat stroke is defined by a core temperature >105°F (40.5°C) with failure of thermoregulation, severe CNS dysfunction, and multisystem organ failure. Classic heat stroke is nonexertional, typically affecting the elderly, very young, or debilitated patients who cannot escape a hot environment; it develops over days to weeks and is associated with severe dehydration and hot, often dry skin. Exertional heat stroke occurs in younger, healthy individuals under intense physical exertion, develops over hours, and may occur despite ongoing sweating. Heat exhaustion involves moderate temperature elevation, usually <104°F (40°C), preserved thermoregulation and CNS function, and fluid or salt depletion; without treatment it may progress to heat stroke.
Etiology Predisposing factors impair heat dissipation or increase heat production. Medical conditions include extremes of age, dehydration, cardiovascular disease, obesity, diabetes, hyperthyroidism, pheochromocytoma, febrile illness, and skin disorders limiting sweating. Pharmacologic contributors include sympathomimetics, cocaine, PCP, LSD, MAO inhibitors, antipsychotics, anxiolytics, anticholinergics, antihistamines, beta-blockers, diuretics, laxatives, and drug or alcohol withdrawal. Environmental risks include high heat and humidity, prolonged exertion, immobility, lack of air conditioning, poor acclimatization, and occlusive clothing.
Pediatric considerations Children are at increased risk due to higher body surface area–to–mass ratio and reduced sweating capacity.
Diagnosis
Signs and symptoms Heat stroke presents with the classic triad of hyperthermia, CNS dysfunction, and hot skin. Core temperature exceeds 105°F (40.5°C). Neurologic findings include delirium, coma, seizures, ataxia, and confusion. Cardiovascular findings include tachycardia, hypotension, wide pulse pressure, and conduction abnormalities. Pulmonary findings include tachypnea, respiratory alkalosis, hypoxemia, and noncardiogenic pulmonary edema. GI symptoms include nausea, vomiting, and diarrhea. Renal failure, rhabdomyolysis, hepatic failure with extreme transaminase elevation, and coagulopathy including DIC may occur and indicate poor prognosis. Heat exhaustion causes headache, fatigue, malaise, impaired judgment, nausea, vomiting, tachycardia, dehydration, tachypnea, and profuse sweating without severe CNS dysfunction. Heat cramps cause painful muscle cramps after heavy sweating and hypotonic fluid replacement, leading to hyponatremia. Heat edema presents as dependent lower-extremity swelling in nonacclimatized individuals. Heat syncope presents as transient loss of consciousness during heat exposure, especially in the elderly. Prickly heat causes a pruritic maculopapular or vesicular rash due to sweat duct obstruction.
Essential workup Measure accurate core temperature using a rectal or esophageal probe. Establish history of heat exposure. Heat exhaustion is a diagnosis of exclusion. Heat stroke requires both core temperature >40.5°C and severe CNS dysfunction.
Diagnosis tests and interpretation
Laboratory Obtain CBC (leukocytosis, hemoconcentration), electrolytes, BUN, creatinine, glucose, urinalysis (myoglobin), creatine kinase for rhabdomyolysis, ABG (acidosis and elevated lactate common in exertional heat stroke), blood and urine cultures if sepsis is considered, toxicology screen, PT/PTT and DIC panel, liver function tests, and troponin (elevation suggests poor prognosis).
Imaging ECG in elderly or cardiac risk patients. Chest radiograph for ARDS or aspiration. Head CT for altered mental status. Lumbar puncture may be required to exclude CNS infection.
Differential diagnosis Sepsis, thyroid storm, pheochromocytoma, stimulant or anticholinergic toxicity, meningitis or encephalitis, cerebral malaria, delirium tremens, neuroleptic malignant syndrome, malignant hyperthermia, and serotonin syndrome.
Treatment
Prehospital Remove patient from heat source, disrobe, and initiate cooling with wet sheets.
Initial stabilization/therapy Ensure airway, breathing, and circulation. Begin continuous core temperature monitoring. Initiate rapid cooling if temperature >104°F (40°C). Give IV 0.9% normal saline bolus if hypotensive. For altered mental status, administer glucose, thiamine, and naloxone as indicated.
Emergency department management Cooling is the priority. Use evaporative cooling with misted warm water and high airflow; combine with ice packs to groin and axilla. Cold-water immersion is effective but often impractical. Advanced techniques such as cold peritoneal lavage, extracorporeal circulation, or cold dialysis may be considered for refractory cases. Stop cooling at 102°F (39°C) to prevent hypothermia. Antipyretics are ineffective and alcohol sponge baths should be avoided. Supportive care includes aggressive isotonic fluid resuscitation while avoiding fluid overload. Insert Foley catheter to monitor urine output; target >2 mL/kg/hr if rhabdomyolysis is present. Treat seizures, agitation, and shivering with benzodiazepines. Avoid vasopressors and antiarrhythmics until adequate cooling, as many arrhythmias resolve with temperature normalization. Treat associated heat syndromes with appropriate hydration, electrolyte replacement, elevation or compression, and topical therapy as indicated.
Medication Benzodiazepines such as diazepam or lorazepam for seizures or agitation; naloxone when opioid toxicity is suspected.
Follow-up and disposition
Admission criteria All patients with heat stroke require ICU admission. Heat exhaustion requires admission if severe electrolyte abnormalities, renal failure, rhabdomyolysis, or advanced age are present.
Discharge criteria Patients without heat stroke or severe heat exhaustion who normalize clinically after treatment may be discharged with counseling.
Key points Heat stroke cannot be diagnosed without both core temperature >40.5°C and severe CNS dysfunction. Rapid cooling and supportive care are the cornerstones of management. Continuous core temperature monitoring is standard of care, and evaporative cooling is the preferred first-line method.
Basics
Description Hyperthermia represents a spectrum of heat-related illness caused by progressively overwhelming heat stress, ranging from dehydration and electrolyte abnormalities to thermoregulatory failure and multisystem organ dysfunction. Normal body temperature is maintained by balancing heat production and dissipation. At temperatures above 42°C (108°F), oxidative phosphorylation becomes uncoupled and critical enzymes fail. Heat stroke is defined by a core temperature >105°F (40.5°C) with failure of thermoregulation, severe CNS dysfunction, and multisystem organ failure. Classic heat stroke is nonexertional, typically affecting the elderly, very young, or debilitated patients who cannot escape a hot environment; it develops over days to weeks and is associated with severe dehydration and hot, often dry skin. Exertional heat stroke occurs in younger, healthy individuals under intense physical exertion, develops over hours, and may occur despite ongoing sweating. Heat exhaustion involves moderate temperature elevation, usually <104°F (40°C), preserved thermoregulation and CNS function, and fluid or salt depletion; without treatment it may progress to heat stroke.
Etiology Predisposing factors impair heat dissipation or increase heat production. Medical conditions include extremes of age, dehydration, cardiovascular disease, obesity, diabetes, hyperthyroidism, pheochromocytoma, febrile illness, and skin disorders limiting sweating. Pharmacologic contributors include sympathomimetics, cocaine, PCP, LSD, MAO inhibitors, antipsychotics, anxiolytics, anticholinergics, antihistamines, beta-blockers, diuretics, laxatives, and drug or alcohol withdrawal. Environmental risks include high heat and humidity, prolonged exertion, immobility, lack of air conditioning, poor acclimatization, and occlusive clothing.
Pediatric considerations Children are at increased risk due to higher body surface area–to–mass ratio and reduced sweating capacity.
Diagnosis
Signs and symptoms Heat stroke presents with the classic triad of hyperthermia, CNS dysfunction, and hot skin. Core temperature exceeds 105°F (40.5°C). Neurologic findings include delirium, coma, seizures, ataxia, and confusion. Cardiovascular findings include tachycardia, hypotension, wide pulse pressure, and conduction abnormalities. Pulmonary findings include tachypnea, respiratory alkalosis, hypoxemia, and noncardiogenic pulmonary edema. GI symptoms include nausea, vomiting, and diarrhea. Renal failure, rhabdomyolysis, hepatic failure with extreme transaminase elevation, and coagulopathy including DIC may occur and indicate poor prognosis. Heat exhaustion causes headache, fatigue, malaise, impaired judgment, nausea, vomiting, tachycardia, dehydration, tachypnea, and profuse sweating without severe CNS dysfunction. Heat cramps cause painful muscle cramps after heavy sweating and hypotonic fluid replacement, leading to hyponatremia. Heat edema presents as dependent lower-extremity swelling in nonacclimatized individuals. Heat syncope presents as transient loss of consciousness during heat exposure, especially in the elderly. Prickly heat causes a pruritic maculopapular or vesicular rash due to sweat duct obstruction.
Essential workup Measure accurate core temperature using a rectal or esophageal probe. Establish history of heat exposure. Heat exhaustion is a diagnosis of exclusion. Heat stroke requires both core temperature >40.5°C and severe CNS dysfunction.
Diagnosis tests and interpretation
Laboratory Obtain CBC (leukocytosis, hemoconcentration), electrolytes, BUN, creatinine, glucose, urinalysis (myoglobin), creatine kinase for rhabdomyolysis, ABG (acidosis and elevated lactate common in exertional heat stroke), blood and urine cultures if sepsis is considered, toxicology screen, PT/PTT and DIC panel, liver function tests, and troponin (elevation suggests poor prognosis).
Imaging ECG in elderly or cardiac risk patients. Chest radiograph for ARDS or aspiration. Head CT for altered mental status. Lumbar puncture may be required to exclude CNS infection.
Differential diagnosis Sepsis, thyroid storm, pheochromocytoma, stimulant or anticholinergic toxicity, meningitis or encephalitis, cerebral malaria, delirium tremens, neuroleptic malignant syndrome, malignant hyperthermia, and serotonin syndrome.
Treatment
Prehospital Remove patient from heat source, disrobe, and initiate cooling with wet sheets.
Initial stabilization/therapy Ensure airway, breathing, and circulation. Begin continuous core temperature monitoring. Initiate rapid cooling if temperature >104°F (40°C). Give IV 0.9% normal saline bolus if hypotensive. For altered mental status, administer glucose, thiamine, and naloxone as indicated.
Emergency department management Cooling is the priority. Use evaporative cooling with misted warm water and high airflow; combine with ice packs to groin and axilla. Cold-water immersion is effective but often impractical. Advanced techniques such as cold peritoneal lavage, extracorporeal circulation, or cold dialysis may be considered for refractory cases. Stop cooling at 102°F (39°C) to prevent hypothermia. Antipyretics are ineffective and alcohol sponge baths should be avoided. Supportive care includes aggressive isotonic fluid resuscitation while avoiding fluid overload. Insert Foley catheter to monitor urine output; target >2 mL/kg/hr if rhabdomyolysis is present. Treat seizures, agitation, and shivering with benzodiazepines. Avoid vasopressors and antiarrhythmics until adequate cooling, as many arrhythmias resolve with temperature normalization. Treat associated heat syndromes with appropriate hydration, electrolyte replacement, elevation or compression, and topical therapy as indicated.
Medication Benzodiazepines such as diazepam or lorazepam for seizures or agitation; naloxone when opioid toxicity is suspected.
Follow-up and disposition
Admission criteria All patients with heat stroke require ICU admission. Heat exhaustion requires admission if severe electrolyte abnormalities, renal failure, rhabdomyolysis, or advanced age are present.
Discharge criteria Patients without heat stroke or severe heat exhaustion who normalize clinically after treatment may be discharged with counseling.
Key points Heat stroke cannot be diagnosed without both core temperature >40.5°C and severe CNS dysfunction. Rapid cooling and supportive care are the cornerstones of management. Continuous core temperature monitoring is standard of care, and evaporative cooling is the preferred first-line method.
- Published on
Emergency And Acute Medicine: Hyperthyroidism
Basics
Description Hyperthyroidism is caused by excessive thyroid hormone production, producing a continuum of disease due to direct metabolic effects of thyroid hormones and increased sensitivity to catecholamines. Clinical states range from subclinical or mild hyperthyroidism to thyrotoxicosis and, in 1–2% of cases, life-threatening thyroid storm. Thyroid regulation occurs through hypothalamic TRH stimulating pituitary TSH release, which increases thyroidal secretion of T4 and T3. Most circulating hormone is T4, which is peripherally converted to the more biologically active T3. Genetic predisposition plays a role, particularly in Graves disease, which is associated with HLA-B8 and HLA-DR3, and in some familial cases of nontoxic goiter with autosomal dominant inheritance.
Etiology Primary hyperthyroidism includes Graves disease, toxic multinodular or uninodular goiter, iodine-induced hyperthyroidism, and thyroiditis (postpartum, radiation, subacute de Quervain, and chronic lymphocytic). Other causes include metastatic thyroid cancer, ectopic thyroid tissue such as struma ovarii, pituitary adenoma, drug-induced hyperthyroidism (amiodarone, lithium, interferon, interleukin-2, iodinated contrast), factitious thyrotoxicosis from excess hormone ingestion, and aspirin overdose.
Diagnosis
Alert Thyroid storm is a medical emergency and may be precipitated by infection, trauma, surgery, diabetic ketoacidosis, myocardial infarction, stroke, chemotherapy, organophosphate intoxication, or abrupt withdrawal of antithyroid medications.
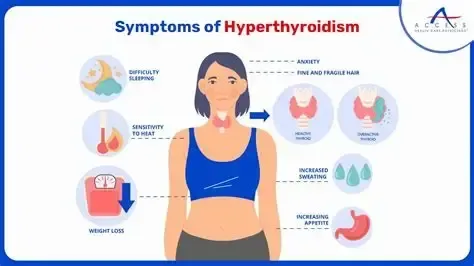
Signs and symptoms Findings reflect heightened end-organ responsiveness to thyroid hormone. Common signs include fever, tachycardia with widened pulse pressure, diaphoresis, tremor, hyperreflexia, goiter, thyromegaly, thyroid bruit, exophthalmos, lid lag, pretibial myxedema, congestive heart failure, shock, and psychosis. Symptoms include weight loss despite increased appetite, palpitations, chest pain, heat intolerance, diarrhea, vomiting, weakness, anxiety, insomnia, menstrual irregularities, and fatigue. Thyroid storm presents with exaggerated manifestations including extreme tachyarrhythmias, heart failure, shock, delirium, coma, seizures, and thromboembolic events.
Geriatric considerations Apathetic hyperthyroidism often presents with subtle findings such as refractory atrial fibrillation, heart failure, weight loss, depression, tremor, and emotional lability rather than classic hyperadrenergic features.
History Typically reveals gradual onset of symptoms.
Physical exam May show fever, tachycardia, systolic hypertension with widened pulse pressure, tachypnea, alopecia, fine diaphoretic skin, irregularly irregular rhythm, lung rales, RUQ tenderness, jaundice, proximal muscle weakness, tremor, and altered mental status.
Essential workup Identify underlying cause and precipitating factors. Plasma TSH is the preferred initial test; a normal TSH generally excludes hyperthyroidism. Low TSH with normal T4 requires T3 measurement to rule out T3 thyrotoxicosis. If laboratory testing is delayed or unavailable, strong clinical suspicion should prompt treatment.
Diagnosis tests and interpretation
Laboratory TSH is typically suppressed, with elevated free T4. Approximately 5% of patients have isolated T3 thyrotoxicosis. Additional testing may include CBC, chemistry panel, liver enzymes, ABG, glucose, and cardiac markers to evaluate complications or precipitants.
Imaging Chest radiograph is useful in heart failure or infection.
Diagnostic procedures ECG commonly shows sinus tachycardia or new-onset atrial fibrillation and helps identify ischemia as a precipitating factor.
Differential diagnosis Pheochromocytoma, sepsis, sympathomimetic intoxication, psychosis, heat stroke, delirium tremens, malignant hyperthermia, neuroleptic malignant syndrome, serotonin syndrome, hypothalamic stroke, hypothyroidism with apathetic presentation, and factitious thyrotoxicosis.
Treatment
Prehospital Supportive care and stabilization.
Initial stabilization/therapy Manage airway, breathing, and circulation. Initiate cardiac monitoring, provide oxygen and IV fluids, and begin cooling measures. Use acetaminophen for fever and avoid aspirin, which increases free thyroid hormone levels.
Emergency department management Identify and treat precipitating causes. In suspected thyroid storm, initiate treatment based on clinical suspicion without delay. Inhibit hormone synthesis with thioamides, preferably propylthiouracil, which also reduces peripheral T4-to-T3 conversion; methimazole is an alternative. Block hormone release with iodine preparations only after thioamide administration and at least one hour later. Block peripheral effects using beta-blockers, with propranolol preferred due to inhibition of T4-to-T3 conversion; esmolol may be used when beta-1 selectivity is needed. Reduce peripheral conversion with corticosteroids. Adjunctive therapies include cholestyramine to reduce enterohepatic circulation of thyroid hormone and lithium if iodine is contraindicated. Manage heart failure, dehydration, hyperthermia, and associated conditions concurrently.
Medication Propylthiouracil, propranolol, iodine solutions (Lugol), methimazole, esmolol, hydrocortisone or dexamethasone, cholestyramine, lithium, guanethidine, and reserpine as indicated based on clinical context.
Pregnancy considerations Physiologic changes may mimic hyperthyroidism. Poorly controlled disease increases risks of hyperemesis gravidarum, preeclampsia, preterm labor, low birth weight, miscarriage, and stillbirth. PTU is preferred at the lowest effective dose; propranolol may be used cautiously. Radioactive iodine is contraindicated. Thyroidectomy is an option when medications are not tolerated. Postpartum thyroiditis occurs in up to 10% of patients and often resolves within one year.
Follow-up and disposition
Admission criteria Thyroid storm, need for IV rate control, or significant instability.
Discharge criteria Mild symptoms responsive to oral therapy with reliable follow-up.
Follow-up recommendations Arrange timely primary care or endocrinology follow-up.
Key points Thyroid storm is highly lethal without prompt treatment and often requires empiric therapy. Never administer iodine before blocking hormone synthesis with a thioamide. Radioactive iodine is contraindicated in pregnancy.
Basics
Description Hyperthyroidism is caused by excessive thyroid hormone production, producing a continuum of disease due to direct metabolic effects of thyroid hormones and increased sensitivity to catecholamines. Clinical states range from subclinical or mild hyperthyroidism to thyrotoxicosis and, in 1–2% of cases, life-threatening thyroid storm. Thyroid regulation occurs through hypothalamic TRH stimulating pituitary TSH release, which increases thyroidal secretion of T4 and T3. Most circulating hormone is T4, which is peripherally converted to the more biologically active T3. Genetic predisposition plays a role, particularly in Graves disease, which is associated with HLA-B8 and HLA-DR3, and in some familial cases of nontoxic goiter with autosomal dominant inheritance.
Etiology Primary hyperthyroidism includes Graves disease, toxic multinodular or uninodular goiter, iodine-induced hyperthyroidism, and thyroiditis (postpartum, radiation, subacute de Quervain, and chronic lymphocytic). Other causes include metastatic thyroid cancer, ectopic thyroid tissue such as struma ovarii, pituitary adenoma, drug-induced hyperthyroidism (amiodarone, lithium, interferon, interleukin-2, iodinated contrast), factitious thyrotoxicosis from excess hormone ingestion, and aspirin overdose.
Diagnosis
Alert Thyroid storm is a medical emergency and may be precipitated by infection, trauma, surgery, diabetic ketoacidosis, myocardial infarction, stroke, chemotherapy, organophosphate intoxication, or abrupt withdrawal of antithyroid medications.
Signs and symptoms Findings reflect heightened end-organ responsiveness to thyroid hormone. Common signs include fever, tachycardia with widened pulse pressure, diaphoresis, tremor, hyperreflexia, goiter, thyromegaly, thyroid bruit, exophthalmos, lid lag, pretibial myxedema, congestive heart failure, shock, and psychosis. Symptoms include weight loss despite increased appetite, palpitations, chest pain, heat intolerance, diarrhea, vomiting, weakness, anxiety, insomnia, menstrual irregularities, and fatigue. Thyroid storm presents with exaggerated manifestations including extreme tachyarrhythmias, heart failure, shock, delirium, coma, seizures, and thromboembolic events.
Geriatric considerations Apathetic hyperthyroidism often presents with subtle findings such as refractory atrial fibrillation, heart failure, weight loss, depression, tremor, and emotional lability rather than classic hyperadrenergic features.
History Typically reveals gradual onset of symptoms.
Physical exam May show fever, tachycardia, systolic hypertension with widened pulse pressure, tachypnea, alopecia, fine diaphoretic skin, irregularly irregular rhythm, lung rales, RUQ tenderness, jaundice, proximal muscle weakness, tremor, and altered mental status.
Essential workup Identify underlying cause and precipitating factors. Plasma TSH is the preferred initial test; a normal TSH generally excludes hyperthyroidism. Low TSH with normal T4 requires T3 measurement to rule out T3 thyrotoxicosis. If laboratory testing is delayed or unavailable, strong clinical suspicion should prompt treatment.
Diagnosis tests and interpretation
Laboratory TSH is typically suppressed, with elevated free T4. Approximately 5% of patients have isolated T3 thyrotoxicosis. Additional testing may include CBC, chemistry panel, liver enzymes, ABG, glucose, and cardiac markers to evaluate complications or precipitants.
Imaging Chest radiograph is useful in heart failure or infection.
Diagnostic procedures ECG commonly shows sinus tachycardia or new-onset atrial fibrillation and helps identify ischemia as a precipitating factor.
Differential diagnosis Pheochromocytoma, sepsis, sympathomimetic intoxication, psychosis, heat stroke, delirium tremens, malignant hyperthermia, neuroleptic malignant syndrome, serotonin syndrome, hypothalamic stroke, hypothyroidism with apathetic presentation, and factitious thyrotoxicosis.
Treatment
Prehospital Supportive care and stabilization.
Initial stabilization/therapy Manage airway, breathing, and circulation. Initiate cardiac monitoring, provide oxygen and IV fluids, and begin cooling measures. Use acetaminophen for fever and avoid aspirin, which increases free thyroid hormone levels.
Emergency department management Identify and treat precipitating causes. In suspected thyroid storm, initiate treatment based on clinical suspicion without delay. Inhibit hormone synthesis with thioamides, preferably propylthiouracil, which also reduces peripheral T4-to-T3 conversion; methimazole is an alternative. Block hormone release with iodine preparations only after thioamide administration and at least one hour later. Block peripheral effects using beta-blockers, with propranolol preferred due to inhibition of T4-to-T3 conversion; esmolol may be used when beta-1 selectivity is needed. Reduce peripheral conversion with corticosteroids. Adjunctive therapies include cholestyramine to reduce enterohepatic circulation of thyroid hormone and lithium if iodine is contraindicated. Manage heart failure, dehydration, hyperthermia, and associated conditions concurrently.
Medication Propylthiouracil, propranolol, iodine solutions (Lugol), methimazole, esmolol, hydrocortisone or dexamethasone, cholestyramine, lithium, guanethidine, and reserpine as indicated based on clinical context.
Pregnancy considerations Physiologic changes may mimic hyperthyroidism. Poorly controlled disease increases risks of hyperemesis gravidarum, preeclampsia, preterm labor, low birth weight, miscarriage, and stillbirth. PTU is preferred at the lowest effective dose; propranolol may be used cautiously. Radioactive iodine is contraindicated. Thyroidectomy is an option when medications are not tolerated. Postpartum thyroiditis occurs in up to 10% of patients and often resolves within one year.
Follow-up and disposition
Admission criteria Thyroid storm, need for IV rate control, or significant instability.
Discharge criteria Mild symptoms responsive to oral therapy with reliable follow-up.
Follow-up recommendations Arrange timely primary care or endocrinology follow-up.
Key points Thyroid storm is highly lethal without prompt treatment and often requires empiric therapy. Never administer iodine before blocking hormone synthesis with a thioamide. Radioactive iodine is contraindicated in pregnancy.
- Published on
Emergency And Acute Medicine: Hypokalemia
Basics
Description
Hypokalemia is defined as a serum potassium <3.5 meq />. Mild 3–3.5 mEq/L, moderate 2.5–3 mEq/L, severe <2.5 meq />. Occurs in up to 20% of inpatients and 14% of outpatients, commonly from diuretics or GI losses. Potassium is the major intracellular cation (98% intracellular) maintained by Na–K ATPase, insulin, β-agonists, and mineralocorticoids. Hypokalemia increases the intracellular–extracellular potassium gradient, alters depolarization thresholds, prolongs action potentials, and disrupts cellular function.
Etiology
Renal losses Diuretics, renal tubular disorders (RTA I and II), interstitial nephritis, drug toxicity (amphotericin, cisplatin), myeloma kidney, hyperaldosteronism (primary, secondary, exogenous), hypomagnesemia, osmotic diuresis, Bartter and Gitelman syndromes, Liddle syndrome, delivery of nonreabsorbable anions (bicarbonate, ketones, hippurate, penicillins).
GI losses Diarrhea, villous adenomas, laxative abuse, vomiting or NG suction, ureterosigmoidostomy, intestinal fistulae, ileostomy, cystic fibrosis.
Intracellular shift Alkalosis, insulin administration or refeeding, adrenergic excess (stress, β-agonists, theophylline), stimulants, hypokalemic periodic paralysis (familial or thyrotoxic), hypothermia.
Poor intake Rare alone; seen with malnutrition, eating disorders, dementia, or esophageal disease.
Diagnosis
Signs And Symptoms Neuromuscular weakness beginning in lower extremities and progressing proximally, paralysis with rapid severe hypokalemia, muscle cramps, tetany, rhabdomyolysis, paresthesias, fatigue. GI ileus and constipation. Cardiac dysrhythmias including PACs, PVCs, AV block, atrial or junctional tachycardias, VT/VF, and potentiation of digoxin toxicity. Renal concentrating defect causing polyuria and polydipsia.
Physical Exam Hypertension suggests mineralocorticoid excess or renal artery stenosis. Hypotension suggests GI loss or diuretics. Decreased reflexes and muscle tenderness may be present.
Diagnosis Tests And Interpretation
Lab Electrolytes, BUN, creatinine, glucose. Elevated bicarbonate suggests diuretics, vomiting, or mineralocorticoid excess; low bicarbonate suggests RTA or diarrhea. Urine potassium <20 meq /> suggests nonrenal loss or intracellular shift; >20 mEq/L suggests renal loss. Urine potassium–creatinine ratio <13 meq /> favors nonrenal loss; >13 mEq/g favors renal loss. Urine sodium <20 meq /> with high urine potassium suggests secondary hyperaldosteronism. Plasma renin differentiates primary vs secondary hyperaldosteronism. Check TSH and free T4 if indicated.
ECG Flattened T waves, ST depression, prominent U waves mimicking QT prolongation, small P waves, atrial and ventricular dysrhythmias.
Differential Diagnosis Primary cardiac disease, neuromuscular junction disorders, spinal cord disease, polyneuropathies, acute myopathies, cataplexy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, cardiac monitoring.
Emergency Department Treatment/Procedures Replace potassium based on severity, symptoms, and comorbidities. Oral replacement preferred when possible. Identify and stop ongoing losses, treat vomiting or diarrhea, avoid glucose-containing fluids, and correct volume depletion and hypochloremia.
Medications
Oral potassium chloride Preferred. Mild to moderate: 10–20 mEq q6–12h. Moderate to severe: 40–60 mEq q8–12h.
Oral potassium citrate or gluconate Use in acidosis; less effective in alkalosis.
IV potassium chloride Indicated for severe hypokalemia, dysrhythmias, paralysis, or ongoing losses. Typical rate 10 mEq/h via peripheral line; higher rates require central access and close monitoring. Avoid dextrose solutions.
Adjuncts Magnesium sulfate 2 g IV if hypomagnesemia present. Correct volume and chloride deficits with normal saline.
Follow-Up And Disposition
Admission Criteria Need for IV potassium, dysrhythmias, profound weakness, ongoing losses, K <2.5 meq />, significant hypotension or hypertension, major comorbidities.
Discharge Criteria Asymptomatic, able to take oral potassium, reliable follow-up. Recheck electrolytes in 2–3 days.
Follow-Up Recommendations Continue replacement until potassium remains ≥3–3.5 mEq/L. Refer to nephrology if renal wasting suspected.
Pearls And Pitfalls
Correct hypokalemia before treating acidosis to prevent dangerous intracellular shifts. Avoid glucose during replacement. Check and correct magnesium if hypokalemia is refractory. Small potassium doses are sufficient in periodic paralysis or adrenergic states; excessive replacement risks rebound hyperkalemia.
Basics
Description
Hypokalemia is defined as a serum potassium <3.5 meq />. Mild 3–3.5 mEq/L, moderate 2.5–3 mEq/L, severe <2.5 meq />. Occurs in up to 20% of inpatients and 14% of outpatients, commonly from diuretics or GI losses. Potassium is the major intracellular cation (98% intracellular) maintained by Na–K ATPase, insulin, β-agonists, and mineralocorticoids. Hypokalemia increases the intracellular–extracellular potassium gradient, alters depolarization thresholds, prolongs action potentials, and disrupts cellular function.
Etiology
Renal losses Diuretics, renal tubular disorders (RTA I and II), interstitial nephritis, drug toxicity (amphotericin, cisplatin), myeloma kidney, hyperaldosteronism (primary, secondary, exogenous), hypomagnesemia, osmotic diuresis, Bartter and Gitelman syndromes, Liddle syndrome, delivery of nonreabsorbable anions (bicarbonate, ketones, hippurate, penicillins).
GI losses Diarrhea, villous adenomas, laxative abuse, vomiting or NG suction, ureterosigmoidostomy, intestinal fistulae, ileostomy, cystic fibrosis.
Intracellular shift Alkalosis, insulin administration or refeeding, adrenergic excess (stress, β-agonists, theophylline), stimulants, hypokalemic periodic paralysis (familial or thyrotoxic), hypothermia.
Poor intake Rare alone; seen with malnutrition, eating disorders, dementia, or esophageal disease.
Diagnosis
Signs And Symptoms Neuromuscular weakness beginning in lower extremities and progressing proximally, paralysis with rapid severe hypokalemia, muscle cramps, tetany, rhabdomyolysis, paresthesias, fatigue. GI ileus and constipation. Cardiac dysrhythmias including PACs, PVCs, AV block, atrial or junctional tachycardias, VT/VF, and potentiation of digoxin toxicity. Renal concentrating defect causing polyuria and polydipsia.
Physical Exam Hypertension suggests mineralocorticoid excess or renal artery stenosis. Hypotension suggests GI loss or diuretics. Decreased reflexes and muscle tenderness may be present.
Diagnosis Tests And Interpretation
Lab Electrolytes, BUN, creatinine, glucose. Elevated bicarbonate suggests diuretics, vomiting, or mineralocorticoid excess; low bicarbonate suggests RTA or diarrhea. Urine potassium <20 meq /> suggests nonrenal loss or intracellular shift; >20 mEq/L suggests renal loss. Urine potassium–creatinine ratio <13 meq /> favors nonrenal loss; >13 mEq/g favors renal loss. Urine sodium <20 meq /> with high urine potassium suggests secondary hyperaldosteronism. Plasma renin differentiates primary vs secondary hyperaldosteronism. Check TSH and free T4 if indicated.
ECG Flattened T waves, ST depression, prominent U waves mimicking QT prolongation, small P waves, atrial and ventricular dysrhythmias.
Differential Diagnosis Primary cardiac disease, neuromuscular junction disorders, spinal cord disease, polyneuropathies, acute myopathies, cataplexy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, cardiac monitoring.
Emergency Department Treatment/Procedures Replace potassium based on severity, symptoms, and comorbidities. Oral replacement preferred when possible. Identify and stop ongoing losses, treat vomiting or diarrhea, avoid glucose-containing fluids, and correct volume depletion and hypochloremia.
Medications
Oral potassium chloride Preferred. Mild to moderate: 10–20 mEq q6–12h. Moderate to severe: 40–60 mEq q8–12h.
Oral potassium citrate or gluconate Use in acidosis; less effective in alkalosis.
IV potassium chloride Indicated for severe hypokalemia, dysrhythmias, paralysis, or ongoing losses. Typical rate 10 mEq/h via peripheral line; higher rates require central access and close monitoring. Avoid dextrose solutions.
Adjuncts Magnesium sulfate 2 g IV if hypomagnesemia present. Correct volume and chloride deficits with normal saline.
Follow-Up And Disposition
Admission Criteria Need for IV potassium, dysrhythmias, profound weakness, ongoing losses, K <2.5 meq />, significant hypotension or hypertension, major comorbidities.
Discharge Criteria Asymptomatic, able to take oral potassium, reliable follow-up. Recheck electrolytes in 2–3 days.
Follow-Up Recommendations Continue replacement until potassium remains ≥3–3.5 mEq/L. Refer to nephrology if renal wasting suspected.
Pearls And Pitfalls
Correct hypokalemia before treating acidosis to prevent dangerous intracellular shifts. Avoid glucose during replacement. Check and correct magnesium if hypokalemia is refractory. Small potassium doses are sufficient in periodic paralysis or adrenergic states; excessive replacement risks rebound hyperkalemia.
- Published on
Emergency And Acute Medicine: Hyperventilation Syndrome
Basics
Description Hyperventilation syndrome is a clinical constellation of symptoms most commonly including dyspnea, chest pain, lightheadedness, and paresthesias. Symptoms result from a nonphysiologic increase in minute ventilation due to increased respiratory rate and/or increased tidal volume such as frequent sighing. The diagnosis can only be made after excluding physiologic and pathologic causes of hyperventilation. It affects approximately 10–15% of the general population and is more common in women, possibly related to progesterone effects.
Etiology The precise mechanism is unclear. Episodes are most often triggered by psychological stressors. Proposed contributing mechanisms include hypocapnia, hypophosphatemia, and hypocalcemia, although their exact roles remain controversial.
Diagnosis
Signs and symptoms
History Patients often report prior similar episodes, identifiable triggers, duration of symptoms, time of onset during the day, and response to previous treatments.
Cardiac Chest pain, dyspnea, air hunger, palpitations.
Neurologic Dizziness, lightheadedness, syncope, paresthesias, headache, carpopedal spasm, tetany.
Psychiatric Anxiety, intense fear, giddiness, depersonalization, sense of unreality.
General Fatigue, weakness, malaise.
Physical exam Findings are often minimal. Tachypnea is common but not universal, as some patients hyperventilate by increasing tidal volume rather than respiratory rate. Carpopedal spasm may be prominent, and Chvostek sign may be present.
Essential workup Hyperventilation syndrome is a diagnosis of exclusion. A careful history and physical examination are essential. Vital signs including pulse oximetry should be obtained; oxygen saturation is normal in isolated hyperventilation syndrome.
Diagnosis tests and interpretation
Laboratory Obtain arterial blood gas analysis if hypoxia is present. Check electrolytes, BUN, creatinine, and glucose when metabolic acidosis or diabetic ketoacidosis is suspected.
ECG Perform when chest pain or palpitations are present.
Imaging Chest radiograph is indicated in patients with hypoxia or focal lung findings.
Diagnostic procedures A hyperventilation provocation test may be attempted after symptom resolution by voluntary overbreathing for three minutes. Reproduction of symptoms may help patient understanding, though diagnostic accuracy is debated.
Differential diagnosis
Pathologic Asthma, congestive heart failure, pulmonary embolism, pneumonia, severe pain, CNS lesions, metabolic acidosis including DKA, pulmonary hypertension, hypoglycemia, drug intoxication such as salicylates, and withdrawal syndromes including alcohol or benzodiazepines.
Physiologic Pregnancy, fever, altitude exposure.
Treatment
Prehospital Patients with abnormal vital signs require IV access and pulse oximetry. Provide supplemental oxygen only if hypoxic.
Initial stabilization/therapy Establish monitoring and initiate evaluation and treatment for suspected physiologic or pathologic causes.
Emergency department management If evaluation excludes organic causes and history is consistent, initiate treatment for hyperventilation syndrome. Reassurance, calm explanation, and coaching often result in rapid symptom resolution. Paper bag rebreathing should not be used, as it is unsupported by evidence and may be dangerous in patients with hypoxia or occult pathology. Address underlying psychological stressors and assess for psychiatric risk including suicidal ideation. Short-acting anxiolytics may be used to interrupt the anxiety–hyperventilation cycle when symptoms persist.
Medication Benzodiazepines such as alprazolam 0.25–0.5 mg PO, lorazepam 1–2 mg PO or IV, or diazepam 2–5 mg PO or IV. Outpatient options include buspirone 5 mg PO three times daily or diazepam 2–5 mg PO two to four times daily for selected patients.
Follow-up and disposition
Admission criteria Hyperventilation syndrome alone does not require hospital admission.
Discharge criteria Pathologic and physiologic causes have been excluded or treated, no acute psychiatric concerns are present, and reliable follow-up is available.
Follow-up recommendations Arrange primary care follow-up and assess the need for psychiatric referral.
Key points Always exclude organic causes before diagnosing hyperventilation syndrome. Isolated hyperventilation syndrome does not cause hypoxia. Avoid paper bag rebreathing due to potential harm.
Basics
Description Hyperventilation syndrome is a clinical constellation of symptoms most commonly including dyspnea, chest pain, lightheadedness, and paresthesias. Symptoms result from a nonphysiologic increase in minute ventilation due to increased respiratory rate and/or increased tidal volume such as frequent sighing. The diagnosis can only be made after excluding physiologic and pathologic causes of hyperventilation. It affects approximately 10–15% of the general population and is more common in women, possibly related to progesterone effects.
Etiology The precise mechanism is unclear. Episodes are most often triggered by psychological stressors. Proposed contributing mechanisms include hypocapnia, hypophosphatemia, and hypocalcemia, although their exact roles remain controversial.
Diagnosis
Signs and symptoms
History Patients often report prior similar episodes, identifiable triggers, duration of symptoms, time of onset during the day, and response to previous treatments.
Cardiac Chest pain, dyspnea, air hunger, palpitations.
Neurologic Dizziness, lightheadedness, syncope, paresthesias, headache, carpopedal spasm, tetany.
Psychiatric Anxiety, intense fear, giddiness, depersonalization, sense of unreality.
General Fatigue, weakness, malaise.
Physical exam Findings are often minimal. Tachypnea is common but not universal, as some patients hyperventilate by increasing tidal volume rather than respiratory rate. Carpopedal spasm may be prominent, and Chvostek sign may be present.
Essential workup Hyperventilation syndrome is a diagnosis of exclusion. A careful history and physical examination are essential. Vital signs including pulse oximetry should be obtained; oxygen saturation is normal in isolated hyperventilation syndrome.
Diagnosis tests and interpretation
Laboratory Obtain arterial blood gas analysis if hypoxia is present. Check electrolytes, BUN, creatinine, and glucose when metabolic acidosis or diabetic ketoacidosis is suspected.
ECG Perform when chest pain or palpitations are present.
Imaging Chest radiograph is indicated in patients with hypoxia or focal lung findings.
Diagnostic procedures A hyperventilation provocation test may be attempted after symptom resolution by voluntary overbreathing for three minutes. Reproduction of symptoms may help patient understanding, though diagnostic accuracy is debated.
Differential diagnosis
Pathologic Asthma, congestive heart failure, pulmonary embolism, pneumonia, severe pain, CNS lesions, metabolic acidosis including DKA, pulmonary hypertension, hypoglycemia, drug intoxication such as salicylates, and withdrawal syndromes including alcohol or benzodiazepines.
Physiologic Pregnancy, fever, altitude exposure.
Treatment
Prehospital Patients with abnormal vital signs require IV access and pulse oximetry. Provide supplemental oxygen only if hypoxic.
Initial stabilization/therapy Establish monitoring and initiate evaluation and treatment for suspected physiologic or pathologic causes.
Emergency department management If evaluation excludes organic causes and history is consistent, initiate treatment for hyperventilation syndrome. Reassurance, calm explanation, and coaching often result in rapid symptom resolution. Paper bag rebreathing should not be used, as it is unsupported by evidence and may be dangerous in patients with hypoxia or occult pathology. Address underlying psychological stressors and assess for psychiatric risk including suicidal ideation. Short-acting anxiolytics may be used to interrupt the anxiety–hyperventilation cycle when symptoms persist.
Medication Benzodiazepines such as alprazolam 0.25–0.5 mg PO, lorazepam 1–2 mg PO or IV, or diazepam 2–5 mg PO or IV. Outpatient options include buspirone 5 mg PO three times daily or diazepam 2–5 mg PO two to four times daily for selected patients.
Follow-up and disposition
Admission criteria Hyperventilation syndrome alone does not require hospital admission.
Discharge criteria Pathologic and physiologic causes have been excluded or treated, no acute psychiatric concerns are present, and reliable follow-up is available.
Follow-up recommendations Arrange primary care follow-up and assess the need for psychiatric referral.
Key points Always exclude organic causes before diagnosing hyperventilation syndrome. Isolated hyperventilation syndrome does not cause hypoxia. Avoid paper bag rebreathing due to potential harm.
- Published on
Emergency And Acute Medicine: Hyperviscosity Syndrome
Basics
Description Hyperviscosity syndrome is the clinical consequence of increased blood viscosity leading to impaired microcirculatory flow and reduced tissue oxygen delivery. As viscosity rises, greater cardiac output is required to maintain perfusion, yet oxygen delivery worsens because blood transit through the microcirculation slows. The classic clinical presentation is a triad of mucosal bleeding, visual disturbances, and neurologic symptoms.
Etiology Hyperviscosity results from elevation of cellular or acellular blood components. Acellular (protein) hyperviscosity is the most common cause (85–90%) and is usually due to increased gamma globulins from monoclonal gammopathies such as Waldenström macroglobulinemia and multiple myeloma; polyclonal gammopathies from rheumatologic disease are rare. Cellular hyperviscosity (10–15%) occurs with markedly increased blood cells, including erythrocytosis in polycythemia vera, extreme leukocytosis (>100,000) in acute or chronic leukemia, and severe thrombocytosis.
Diagnosis
Signs and symptoms The classic triad includes bleeding, visual changes, and neurologic dysfunction. Hematologic manifestations are most common and include epistaxis, gingival, rectal, or uterine bleeding, prolonged postprocedural bleeding, and pruritus. Ocular findings include blurred vision, diplopia, visual loss, and characteristic funduscopic changes such as the “link-sausage” appearance of retinal veins, retinal hemorrhages, exudates, microaneurysms, and papilledema. Neurologic symptoms include headache, dizziness, vertigo, ataxia, tinnitus, hearing loss, paresthesias, peripheral neuropathy, seizures, altered mental status, coma, and intracranial hemorrhage. Renal manifestations include hematuria, sterile pyuria, and nephritic or nephrotic syndromes. Cardiovascular findings may include angina, myocardial infarction, dysrhythmias, and heart failure. Dermatologic features include Raynaud phenomenon, livedo reticularis, palpable purpura, digital infarcts, and peripheral gangrene.
History Suspect hyperviscosity syndrome in patients with the classic triad, known immunoglobulin-producing disorders, or hypercellular hematologic diseases presenting with microvascular ischemia or cardiac decompensation.
Physical exam No pathognomonic findings exist; exam reflects end-organ involvement such as mucosal bleeding, petechiae, focal neurologic deficits, heart failure signs, or abnormal funduscopic findings.
Essential workup Assess for bleeding and end-organ ischemia. Measure serum or whole blood viscosity when available. Suspect the diagnosis when laboratory processing is difficult due to serum stasis or analyzer obstruction from viscous samples.
Diagnosis tests and interpretation
Laboratory Obtain CBC with differential to assess anemia, erythrocytosis, leukocytosis, or thrombocytosis; normocytic normochromic anemia is common. Peripheral smear may show rouleaux formation, a key diagnostic clue. Check electrolytes, BUN, creatinine, and glucose; renal dysfunction is common, and pseudohyponatremia or hypercalcemia may occur in multiple myeloma. Urinalysis may show proteinuria or hematuria. Obtain coagulation studies. Perform serum and urine protein electrophoresis. Serum viscosity measurement (when available) is diagnostic; normal relative viscosity is 1.4–1.8, and symptoms usually develop at ≥4 centipoise.
Imaging Head CT is indicated in patients with neurologic symptoms to exclude intracranial hemorrhage.
Differential diagnosis Platelet disorders, inherited or acquired coagulation factor deficiencies, liver disease, vitamin K deficiency, and disseminated intravascular coagulation.
Treatment
Prehospital Initiate IV fluid resuscitation in patients with bleeding or suspected hypovolemia.
Initial stabilization/therapy Rehydrate with isotonic saline. Bleeding or ischemia often does not respond to routine therapy and requires viscosity reduction. In patients with anemia and leukemia, avoid transfusion before plasmapheresis as it may worsen viscosity.
Emergency department management Provide supportive care and obtain early hematology consultation. Phlebotomy is a temporizing measure in severe cases with coma or seizures when plasmapheresis is not immediately available; remove 100–200 mL of whole blood and replace with isotonic saline, ideally after consultation, and is first-line in polycythemia vera. Plasmapheresis or leukapheresis is definitive therapy; typical volumes are 40 mL/kg in stable patients and up to 60 mL/kg in critically ill patients. Multiple sessions are often required. Monitor for hypocalcemia from citrate anticoagulation and rare dysrhythmias. Leukapheresis is preferred for hyperleukocytosis. ED clinicians may assist by establishing large-bore central access with caution due to bleeding risk.
Follow-up and disposition
Admission criteria Admit all patients with symptomatic hyperviscosity or evidence of bleeding or end-organ ischemia; ICU admission is indicated for hemorrhage, altered mental status, or acute myocardial infarction.
Discharge criteria Discharge only after definitive treatment of the underlying disorder and symptom resolution.
Issues for referral All patients require hematology consultation.
Key points Avoid diuretics as they can worsen viscosity. The hallmark triad consists of visual disturbances, bleeding, and neurologic symptoms. Early recognition and rapid viscosity reduction are critical to prevent irreversible end-organ damage.
Basics
Description Hyperviscosity syndrome is the clinical consequence of increased blood viscosity leading to impaired microcirculatory flow and reduced tissue oxygen delivery. As viscosity rises, greater cardiac output is required to maintain perfusion, yet oxygen delivery worsens because blood transit through the microcirculation slows. The classic clinical presentation is a triad of mucosal bleeding, visual disturbances, and neurologic symptoms.
Etiology Hyperviscosity results from elevation of cellular or acellular blood components. Acellular (protein) hyperviscosity is the most common cause (85–90%) and is usually due to increased gamma globulins from monoclonal gammopathies such as Waldenström macroglobulinemia and multiple myeloma; polyclonal gammopathies from rheumatologic disease are rare. Cellular hyperviscosity (10–15%) occurs with markedly increased blood cells, including erythrocytosis in polycythemia vera, extreme leukocytosis (>100,000) in acute or chronic leukemia, and severe thrombocytosis.
Diagnosis
Signs and symptoms The classic triad includes bleeding, visual changes, and neurologic dysfunction. Hematologic manifestations are most common and include epistaxis, gingival, rectal, or uterine bleeding, prolonged postprocedural bleeding, and pruritus. Ocular findings include blurred vision, diplopia, visual loss, and characteristic funduscopic changes such as the “link-sausage” appearance of retinal veins, retinal hemorrhages, exudates, microaneurysms, and papilledema. Neurologic symptoms include headache, dizziness, vertigo, ataxia, tinnitus, hearing loss, paresthesias, peripheral neuropathy, seizures, altered mental status, coma, and intracranial hemorrhage. Renal manifestations include hematuria, sterile pyuria, and nephritic or nephrotic syndromes. Cardiovascular findings may include angina, myocardial infarction, dysrhythmias, and heart failure. Dermatologic features include Raynaud phenomenon, livedo reticularis, palpable purpura, digital infarcts, and peripheral gangrene.
History Suspect hyperviscosity syndrome in patients with the classic triad, known immunoglobulin-producing disorders, or hypercellular hematologic diseases presenting with microvascular ischemia or cardiac decompensation.
Physical exam No pathognomonic findings exist; exam reflects end-organ involvement such as mucosal bleeding, petechiae, focal neurologic deficits, heart failure signs, or abnormal funduscopic findings.
Essential workup Assess for bleeding and end-organ ischemia. Measure serum or whole blood viscosity when available. Suspect the diagnosis when laboratory processing is difficult due to serum stasis or analyzer obstruction from viscous samples.
Diagnosis tests and interpretation
Laboratory Obtain CBC with differential to assess anemia, erythrocytosis, leukocytosis, or thrombocytosis; normocytic normochromic anemia is common. Peripheral smear may show rouleaux formation, a key diagnostic clue. Check electrolytes, BUN, creatinine, and glucose; renal dysfunction is common, and pseudohyponatremia or hypercalcemia may occur in multiple myeloma. Urinalysis may show proteinuria or hematuria. Obtain coagulation studies. Perform serum and urine protein electrophoresis. Serum viscosity measurement (when available) is diagnostic; normal relative viscosity is 1.4–1.8, and symptoms usually develop at ≥4 centipoise.
Imaging Head CT is indicated in patients with neurologic symptoms to exclude intracranial hemorrhage.
Differential diagnosis Platelet disorders, inherited or acquired coagulation factor deficiencies, liver disease, vitamin K deficiency, and disseminated intravascular coagulation.
Treatment
Prehospital Initiate IV fluid resuscitation in patients with bleeding or suspected hypovolemia.
Initial stabilization/therapy Rehydrate with isotonic saline. Bleeding or ischemia often does not respond to routine therapy and requires viscosity reduction. In patients with anemia and leukemia, avoid transfusion before plasmapheresis as it may worsen viscosity.
Emergency department management Provide supportive care and obtain early hematology consultation. Phlebotomy is a temporizing measure in severe cases with coma or seizures when plasmapheresis is not immediately available; remove 100–200 mL of whole blood and replace with isotonic saline, ideally after consultation, and is first-line in polycythemia vera. Plasmapheresis or leukapheresis is definitive therapy; typical volumes are 40 mL/kg in stable patients and up to 60 mL/kg in critically ill patients. Multiple sessions are often required. Monitor for hypocalcemia from citrate anticoagulation and rare dysrhythmias. Leukapheresis is preferred for hyperleukocytosis. ED clinicians may assist by establishing large-bore central access with caution due to bleeding risk.
Follow-up and disposition
Admission criteria Admit all patients with symptomatic hyperviscosity or evidence of bleeding or end-organ ischemia; ICU admission is indicated for hemorrhage, altered mental status, or acute myocardial infarction.
Discharge criteria Discharge only after definitive treatment of the underlying disorder and symptom resolution.
Issues for referral All patients require hematology consultation.
Key points Avoid diuretics as they can worsen viscosity. The hallmark triad consists of visual disturbances, bleeding, and neurologic symptoms. Early recognition and rapid viscosity reduction are critical to prevent irreversible end-organ damage.
- Published on
Emergency And Acute Medicine: Hyphema
Basics
Description Blood in the anterior chamber of the eye between the iris and cornea. Hyphema refers to grossly visible layered blood. Microhyphema refers to suspended red blood cells seen only on slit-lamp exam. Genetic predisposition is related to hereditary blood dyscrasias.
Etiology Blunt trauma is the most common cause (70–80%) due to anteroposterior compression with equatorial globe expansion causing rupture of iris or ciliary body vessels. Penetrating trauma causes direct vessel injury or sudden ocular decompression. Spontaneous causes include ocular tumors (melanoma, retinoblastoma, xanthogranuloma, metastatic tumors), blood dyscrasias (hemophilia, leukemia, thrombocytopenia, von Willebrand disease), anticoagulant or antiplatelet use (aspirin, warfarin, heparin), iris neovascularization (proliferative diabetic retinopathy, retinal vein occlusion, carotid stenosis), and postsurgical causes such as cataract extraction, trabeculectomy, or vitrectomy. In children without trauma, suspect nonaccidental injury.
Diagnosis
Signs And Symptoms Photophobia, blurred vision, decreased visual acuity, ocular pain, nausea, and vomiting.
History Assess prior visual acuity, prior ocular surgery or glaucoma treatment, bleeding disorders including sickle cell disease, mechanism and timing of injury, onset of visual loss, and history of excessive tearing (suggestive of open globe injury).
Physical Exam Perform full trauma exam. Look for periorbital ecchymosis, eyelid lacerations, enophthalmos, limited ocular movement with diplopia, or proptosis. Ocular exam includes visual acuity, exclusion of open globe injury before tonometry, pupillary response, slit-lamp exam, and dilated fundus exam without pressure on the globe. Hyphema grading: Grade I <1/3 AC, Grade II 1/3–1/2 AC, Grade III >1/2 AC, Grade IV total (“8-ball” hyphema). Higher grades have increased risk of rebleeding, glaucoma, corneal staining, and poor visual recovery.
Diagnosis Tests And Interpretation
Lab Obtain platelet count, PT/PTT if bleeding disorder or anticoagulant use is suspected. Screen for sickle cell disease when indicated.
Imaging CT orbits for suspected open globe, intraocular foreign body, or orbital fracture. B-scan ultrasound only if globe integrity is confirmed and posterior structures cannot be visualized.
Essential Workup Visual acuity, globe integrity, intraocular pressure, assessment for associated injuries, targeted labs, and imaging when indicated.
Differential Diagnosis Uveitis, endophthalmitis.
Treatment
Prehospital Place eye shield if open globe is suspected.
Initial Stabilization/Therapy Keep head elevated, limit activity, avoid straining, place rigid eye shield, and avoid eye patching.
Emergency Department Treatment/Procedures Provide mild analgesia (avoid NSAIDs) and antiemetics. Use cycloplegics (atropine 1% or cyclopentolate 1%) and topical steroids (prednisolone acetate 1%). Aminocaproic acid may be used in consultation with ophthalmology. Oral prednisone may be indicated in selected high-risk cases. Manage elevated intraocular pressure with topical beta-blockers first, then alpha-agonists, carbonic anhydrase inhibitors, and systemic agents if needed. Avoid carbonic anhydrase inhibitors and mannitol in sickle cell disease. Surgical evacuation is indicated for uncontrolled intraocular pressure.
Medications
First Line Atropine 1% TID, prednisolone acetate 1% QID.
Second Line Timolol or levobunolol, brimonidine or apraclonidine, dorzolamide or brinzolamide, acetazolamide.
Follow-Up And Disposition
Admission Criteria Uncontrolled intraocular pressure, open globe injury, noncompliance, associated injuries, children <7 years, or high-risk conditions such as sickle cell disease or hemophilia.
Discharge Criteria Controlled intraocular pressure and absence of admission criteria.
Follow-Up Recommendations Daily ophthalmology follow-up for the first 3 days to monitor for rebleeding, corneal staining, and pressure elevation.
Pearls And Pitfalls Always exclude ruptured globe before tonometry or treatment. Intraocular pressure reduction is not immediate. Screen for sickle cell disease in at-risk populations.
Basics
Description Blood in the anterior chamber of the eye between the iris and cornea. Hyphema refers to grossly visible layered blood. Microhyphema refers to suspended red blood cells seen only on slit-lamp exam. Genetic predisposition is related to hereditary blood dyscrasias.
Etiology Blunt trauma is the most common cause (70–80%) due to anteroposterior compression with equatorial globe expansion causing rupture of iris or ciliary body vessels. Penetrating trauma causes direct vessel injury or sudden ocular decompression. Spontaneous causes include ocular tumors (melanoma, retinoblastoma, xanthogranuloma, metastatic tumors), blood dyscrasias (hemophilia, leukemia, thrombocytopenia, von Willebrand disease), anticoagulant or antiplatelet use (aspirin, warfarin, heparin), iris neovascularization (proliferative diabetic retinopathy, retinal vein occlusion, carotid stenosis), and postsurgical causes such as cataract extraction, trabeculectomy, or vitrectomy. In children without trauma, suspect nonaccidental injury.
Diagnosis
Signs And Symptoms Photophobia, blurred vision, decreased visual acuity, ocular pain, nausea, and vomiting.
History Assess prior visual acuity, prior ocular surgery or glaucoma treatment, bleeding disorders including sickle cell disease, mechanism and timing of injury, onset of visual loss, and history of excessive tearing (suggestive of open globe injury).
Physical Exam Perform full trauma exam. Look for periorbital ecchymosis, eyelid lacerations, enophthalmos, limited ocular movement with diplopia, or proptosis. Ocular exam includes visual acuity, exclusion of open globe injury before tonometry, pupillary response, slit-lamp exam, and dilated fundus exam without pressure on the globe. Hyphema grading: Grade I <1/3 AC, Grade II 1/3–1/2 AC, Grade III >1/2 AC, Grade IV total (“8-ball” hyphema). Higher grades have increased risk of rebleeding, glaucoma, corneal staining, and poor visual recovery.
Diagnosis Tests And Interpretation
Lab Obtain platelet count, PT/PTT if bleeding disorder or anticoagulant use is suspected. Screen for sickle cell disease when indicated.
Imaging CT orbits for suspected open globe, intraocular foreign body, or orbital fracture. B-scan ultrasound only if globe integrity is confirmed and posterior structures cannot be visualized.
Essential Workup Visual acuity, globe integrity, intraocular pressure, assessment for associated injuries, targeted labs, and imaging when indicated.
Differential Diagnosis Uveitis, endophthalmitis.
Treatment
Prehospital Place eye shield if open globe is suspected.
Initial Stabilization/Therapy Keep head elevated, limit activity, avoid straining, place rigid eye shield, and avoid eye patching.
Emergency Department Treatment/Procedures Provide mild analgesia (avoid NSAIDs) and antiemetics. Use cycloplegics (atropine 1% or cyclopentolate 1%) and topical steroids (prednisolone acetate 1%). Aminocaproic acid may be used in consultation with ophthalmology. Oral prednisone may be indicated in selected high-risk cases. Manage elevated intraocular pressure with topical beta-blockers first, then alpha-agonists, carbonic anhydrase inhibitors, and systemic agents if needed. Avoid carbonic anhydrase inhibitors and mannitol in sickle cell disease. Surgical evacuation is indicated for uncontrolled intraocular pressure.
Medications
First Line Atropine 1% TID, prednisolone acetate 1% QID.
Second Line Timolol or levobunolol, brimonidine or apraclonidine, dorzolamide or brinzolamide, acetazolamide.
Follow-Up And Disposition
Admission Criteria Uncontrolled intraocular pressure, open globe injury, noncompliance, associated injuries, children <7 years, or high-risk conditions such as sickle cell disease or hemophilia.
Discharge Criteria Controlled intraocular pressure and absence of admission criteria.
Follow-Up Recommendations Daily ophthalmology follow-up for the first 3 days to monitor for rebleeding, corneal staining, and pressure elevation.
Pearls And Pitfalls Always exclude ruptured globe before tonometry or treatment. Intraocular pressure reduction is not immediate. Screen for sickle cell disease in at-risk populations.
- Published on
Emergency And Acute Medicine – Idiopathic Thrombocytopenic Purpura
Basics
Description Idiopathic thrombocytopenic purpura (ITP) is isolated thrombocytopenia without an identifiable cause and with normal other cell lines. Incidence is approximately 2–5 per 100,000 per year. Acute ITP commonly affects children, with about 80% recovering within 8 weeks with or without therapy. Chronic ITP occurs mainly in adults, particularly young women, and often requires treatment to achieve remission. Refractory chronic ITP is characterized by fluctuating platelet counts and poor response to therapy.
Etiology
Immune-mediated platelet destruction due to autoantibodies, primarily IgG, leading to splenic and hepatic macrophage clearance. Some patients lack detectable autoantibodies, suggesting T-cell–mediated cytotoxicity. Complement activation may contribute. Decreased platelet production may occur in chronic or refractory disease. Eradication of Helicobacter pylori has been associated with platelet recovery in some patients.
Diagnosis
Signs And Symptoms
History: Mucocutaneous bleeding is most common, including epistaxis, gingival bleeding, menorrhagia, and conjunctival hemorrhage. Gastrointestinal bleeding, hemarthrosis, hematuria, and hematomas are uncommon. Pediatric cases often follow viral illness by 2–3 weeks. Adults typically have insidious onset; up to one-quarter are asymptomatic.
Physical exam: Petechiae and nonpalpable purpura are common. Spleen size is normal; splenomegaly suggests an alternate diagnosis. Intracranial hemorrhage is the most serious complication and leading cause of death, with risk increasing with age.
Essential Workup
Diagnosis of exclusion. CBC with differential and peripheral smear. PT and PTT if bleeding. Renal and liver function tests. Type and screen if bleeding. Pregnancy test when appropriate. Consider HIV testing.
Diagnosis Tests And Interpretation
Labs: Isolated thrombocytopenia with increased mean platelet volume. Normal RBC and WBC morphology. Normal coagulation studies and liver function.
Imaging: Noncontrast CT head if headache, neurologic deficits, trauma, or concern for intracranial hemorrhage.
Procedures: Bone marrow biopsy in patients >60 years, atypical cases, refractory disease, or prior to splenectomy. Antibody testing is not clinically useful.
Differential Diagnosis
Bone marrow failure or infiltration, splenic sequestration, thrombotic microangiopathies, disseminated intravascular coagulation, HELLP syndrome, valvular disease, and drug-induced thrombocytopenia.
Treatment
Prehospital And Initial Stabilization ABCs with attention to airway in severe mucosal bleeding or CNS hemorrhage. Establish IV access. Control bleeding with direct pressure.
Emergency Department Management Management depends on platelet count, bleeding severity, duration, age, and comorbidities. Observation is appropriate for children without bleeding or profound thrombocytopenia. Life-threatening bleeding requires high-dose IV corticosteroids, IVIG, and platelet transfusions (given after steroids or IVIG). Platelet transfusions alone are often ineffective. Aminocaproic acid may be considered for mucosal bleeding.
Medication
First line: High-dose glucocorticoids (dexamethasone 40 mg daily or prednisone 1–2 mg/kg/day), IVIG 1–2 g/kg for critical bleeding or urgent platelet rise, Anti-D immunoglobulin in Rh-positive patients.
Second line: Immunosuppressive agents, rituximab, thrombopoietin receptor agonists, or splenectomy for refractory disease.
Pregnancy Considerations
Differentiate from gestational thrombocytopenia and HELLP syndrome. Maternal platelet count does not predict neonatal thrombocytopenia. Mode of delivery is based on obstetric indications. Neonates should be screened and treated if thrombocytopenic.
Follow-Up And Disposition
Admission Criteria Life-threatening bleeding, any bleeding with platelets <20,000 />micro;L, asymptomatic patients with platelets <20,000 />micro;L and unreliable follow-up.
Discharge Criteria Asymptomatic patients or minor bleeding with platelets >30,000/µL.
Follow-Up Recommendations Hematology follow-up is required in all cases.
Key Points And Cautions
Exclude pseudothrombocytopenia before diagnosis. Spontaneous bleeding is uncommon until platelets fall below 10,000/µL. Intracranial hemorrhage risk increases with age and mandates urgent evaluation.
Basics
Description Idiopathic thrombocytopenic purpura (ITP) is isolated thrombocytopenia without an identifiable cause and with normal other cell lines. Incidence is approximately 2–5 per 100,000 per year. Acute ITP commonly affects children, with about 80% recovering within 8 weeks with or without therapy. Chronic ITP occurs mainly in adults, particularly young women, and often requires treatment to achieve remission. Refractory chronic ITP is characterized by fluctuating platelet counts and poor response to therapy.
Etiology
Immune-mediated platelet destruction due to autoantibodies, primarily IgG, leading to splenic and hepatic macrophage clearance. Some patients lack detectable autoantibodies, suggesting T-cell–mediated cytotoxicity. Complement activation may contribute. Decreased platelet production may occur in chronic or refractory disease. Eradication of Helicobacter pylori has been associated with platelet recovery in some patients.
Diagnosis
Signs And Symptoms
History: Mucocutaneous bleeding is most common, including epistaxis, gingival bleeding, menorrhagia, and conjunctival hemorrhage. Gastrointestinal bleeding, hemarthrosis, hematuria, and hematomas are uncommon. Pediatric cases often follow viral illness by 2–3 weeks. Adults typically have insidious onset; up to one-quarter are asymptomatic.
Physical exam: Petechiae and nonpalpable purpura are common. Spleen size is normal; splenomegaly suggests an alternate diagnosis. Intracranial hemorrhage is the most serious complication and leading cause of death, with risk increasing with age.
Essential Workup
Diagnosis of exclusion. CBC with differential and peripheral smear. PT and PTT if bleeding. Renal and liver function tests. Type and screen if bleeding. Pregnancy test when appropriate. Consider HIV testing.
Diagnosis Tests And Interpretation
Labs: Isolated thrombocytopenia with increased mean platelet volume. Normal RBC and WBC morphology. Normal coagulation studies and liver function.
Imaging: Noncontrast CT head if headache, neurologic deficits, trauma, or concern for intracranial hemorrhage.
Procedures: Bone marrow biopsy in patients >60 years, atypical cases, refractory disease, or prior to splenectomy. Antibody testing is not clinically useful.
Differential Diagnosis
Bone marrow failure or infiltration, splenic sequestration, thrombotic microangiopathies, disseminated intravascular coagulation, HELLP syndrome, valvular disease, and drug-induced thrombocytopenia.
Treatment
Prehospital And Initial Stabilization ABCs with attention to airway in severe mucosal bleeding or CNS hemorrhage. Establish IV access. Control bleeding with direct pressure.
Emergency Department Management Management depends on platelet count, bleeding severity, duration, age, and comorbidities. Observation is appropriate for children without bleeding or profound thrombocytopenia. Life-threatening bleeding requires high-dose IV corticosteroids, IVIG, and platelet transfusions (given after steroids or IVIG). Platelet transfusions alone are often ineffective. Aminocaproic acid may be considered for mucosal bleeding.
Medication
First line: High-dose glucocorticoids (dexamethasone 40 mg daily or prednisone 1–2 mg/kg/day), IVIG 1–2 g/kg for critical bleeding or urgent platelet rise, Anti-D immunoglobulin in Rh-positive patients.
Second line: Immunosuppressive agents, rituximab, thrombopoietin receptor agonists, or splenectomy for refractory disease.
Pregnancy Considerations
Differentiate from gestational thrombocytopenia and HELLP syndrome. Maternal platelet count does not predict neonatal thrombocytopenia. Mode of delivery is based on obstetric indications. Neonates should be screened and treated if thrombocytopenic.
Follow-Up And Disposition
Admission Criteria Life-threatening bleeding, any bleeding with platelets <20,000 />micro;L, asymptomatic patients with platelets <20,000 />micro;L and unreliable follow-up.
Discharge Criteria Asymptomatic patients or minor bleeding with platelets >30,000/µL.
Follow-Up Recommendations Hematology follow-up is required in all cases.
Key Points And Cautions
Exclude pseudothrombocytopenia before diagnosis. Spontaneous bleeding is uncommon until platelets fall below 10,000/µL. Intracranial hemorrhage risk increases with age and mandates urgent evaluation.
- Published on
Emergency And Acute Medicine – Hypothermia
Basics
Description Core body temperature <35°c. risk factors include impaired thermoregulation (infants, elderly), comorbid illness, intoxication, and environmental exposure. heat loss occurs via radiation (most significant), conduction, convection, evaporation, respiration. production relies on shivering, nonshivering thermogenesis, increased thyroxine epinephrine.< />pan>
Etiology
Dermal disease (burns, exfoliative dermatitis, severe psoriasis). Drug induced (ethanol, phenothiazines, sedative–hypnotics). Environmental exposure (immersion, nonimmersion). Iatrogenic causes (aggressive fluid resuscitation, heat stroke treatment). Metabolic disorders (hypothyroidism, hypopituitarism, hypoadrenalism). Neurologic conditions (spinal cord injury, head trauma, stroke, tumor, Wernicke disease). Neuromuscular inefficiency (extremes of age, impaired shivering, lack of acclimatization). Sepsis. Pediatric patients are at higher risk because of increased surface area to mass ratio; consider nonaccidental trauma.
Diagnosis
Signs And Symptoms
Mild (35–32.2°C): Hypertension, shivering, tachycardia progressing to bradycardia, tachypnea, vasoconstriction, apathy, ataxia, cold diuresis, impaired judgment.
Moderate (32.2–28°C): Atrial dysrhythmias, bradycardia refractory to atropine, decreased level of consciousness, hypoventilation with CO₂ retention, dilated pupils, diminished gag reflex, cessation of shivering, hyporeflexia, hypotension, J (Osborn) waves.
Severe (<28°c): apnea, coma, minimal eeg activity, nonreactive pupils, oliguria, pulmonary edema, ventricular dysrhythmias or asystole.< />pan>
History Duration and circumstances of cold exposure or submersion.
Physical Exam Pulse and blood pressure may be difficult to detect; pupils often dilated at very low temperatures.
Essential Workup Accurate core temperature measurement.
Diagnosis Tests And Interpretation
Lab Fingerstick glucose, ABG (no temperature correction), CBC (hemoconcentration), electrolytes, BUN/creatinine, potassium, CPK, lactate, coagulation studies, toxicology screen.
Imaging CXR for pneumonia.
ECG Bradyarrhythmias, atrial fibrillation, ventricular fibrillation, prolonged PR/QRS/QT, Osborn waves.
Differential Diagnosis Environmental exposure, sepsis, CNS pathology, metabolic disorders, drug toxicity.
Treatment
Prehospital Patient is not dead until “warm and dead.” Prolonged pulse checks (30–45 s). CPR during transport if indicated.
Initial Stabilization/Therapy ABCs, supplemental oxygen, safe intubation if needed, cardiac monitoring, warmed IV fluids (D5NS preferred), remove wet clothing, passive rewarming, naloxone, dextrose, and thiamine for altered mental status, stress-dose steroids if adrenal insufficiency suspected.
Emergency Department Treatment/Procedures Handle gently to avoid precipitating ventricular fibrillation. Most dysrhythmias resolve with rewarming alone. Defibrillate up to 1–3 times below 28–30°C, then defer until rewarmed. Active rewarming is required for core temperature <32°c. use passive external rewarming for mild cases, active (forced warm air, trunk first) moderate and core (humidified oxygen, warmed iv fluids, peritoneal or pleural lavage, extracorporeal including hemodialysis cardiopulmonary bypass) severe hypothermia cardiac arrest. faster rates (1–2°c />r) are associated with better outcomes.
Medication Amiodarone for persistent ventricular dysrhythmias after rewarming, dextrose for hypoglycemia, hydrocortisone or methylprednisolone if adrenal insufficiency suspected, levothyroxine only for myxedema coma, naloxone, thiamine.
Follow-Up And Disposition
Admission Criteria Moderate to severe hypothermia (<32°c).< />pan>
Discharge Criteria Young, healthy patients with very mild hypothermia who normalize and have a safe, warm environment.
Follow-Up Recommendations Social services involvement for patients at risk of recurrent cold exposure.
Key Points And Cautions Defibrillation is rarely effective below 28–30°C. Atrial fibrillation often resolves with rewarming alone. Beware afterdrop and rewarming shock. Gentle handling and adequate volume resuscitation are essential.
Basics
Description Core body temperature <35°c. risk factors include impaired thermoregulation (infants, elderly), comorbid illness, intoxication, and environmental exposure. heat loss occurs via radiation (most significant), conduction, convection, evaporation, respiration. production relies on shivering, nonshivering thermogenesis, increased thyroxine epinephrine.< />pan>
Etiology
Dermal disease (burns, exfoliative dermatitis, severe psoriasis). Drug induced (ethanol, phenothiazines, sedative–hypnotics). Environmental exposure (immersion, nonimmersion). Iatrogenic causes (aggressive fluid resuscitation, heat stroke treatment). Metabolic disorders (hypothyroidism, hypopituitarism, hypoadrenalism). Neurologic conditions (spinal cord injury, head trauma, stroke, tumor, Wernicke disease). Neuromuscular inefficiency (extremes of age, impaired shivering, lack of acclimatization). Sepsis. Pediatric patients are at higher risk because of increased surface area to mass ratio; consider nonaccidental trauma.
Diagnosis
Signs And Symptoms
Mild (35–32.2°C): Hypertension, shivering, tachycardia progressing to bradycardia, tachypnea, vasoconstriction, apathy, ataxia, cold diuresis, impaired judgment.
Moderate (32.2–28°C): Atrial dysrhythmias, bradycardia refractory to atropine, decreased level of consciousness, hypoventilation with CO₂ retention, dilated pupils, diminished gag reflex, cessation of shivering, hyporeflexia, hypotension, J (Osborn) waves.
Severe (<28°c): apnea, coma, minimal eeg activity, nonreactive pupils, oliguria, pulmonary edema, ventricular dysrhythmias or asystole.< />pan>
History Duration and circumstances of cold exposure or submersion.
Physical Exam Pulse and blood pressure may be difficult to detect; pupils often dilated at very low temperatures.
Essential Workup Accurate core temperature measurement.
Diagnosis Tests And Interpretation
Lab Fingerstick glucose, ABG (no temperature correction), CBC (hemoconcentration), electrolytes, BUN/creatinine, potassium, CPK, lactate, coagulation studies, toxicology screen.
Imaging CXR for pneumonia.
ECG Bradyarrhythmias, atrial fibrillation, ventricular fibrillation, prolonged PR/QRS/QT, Osborn waves.
Differential Diagnosis Environmental exposure, sepsis, CNS pathology, metabolic disorders, drug toxicity.
Treatment
Prehospital Patient is not dead until “warm and dead.” Prolonged pulse checks (30–45 s). CPR during transport if indicated.
Initial Stabilization/Therapy ABCs, supplemental oxygen, safe intubation if needed, cardiac monitoring, warmed IV fluids (D5NS preferred), remove wet clothing, passive rewarming, naloxone, dextrose, and thiamine for altered mental status, stress-dose steroids if adrenal insufficiency suspected.
Emergency Department Treatment/Procedures Handle gently to avoid precipitating ventricular fibrillation. Most dysrhythmias resolve with rewarming alone. Defibrillate up to 1–3 times below 28–30°C, then defer until rewarmed. Active rewarming is required for core temperature <32°c. use passive external rewarming for mild cases, active (forced warm air, trunk first) moderate and core (humidified oxygen, warmed iv fluids, peritoneal or pleural lavage, extracorporeal including hemodialysis cardiopulmonary bypass) severe hypothermia cardiac arrest. faster rates (1–2°c />r) are associated with better outcomes.
Medication Amiodarone for persistent ventricular dysrhythmias after rewarming, dextrose for hypoglycemia, hydrocortisone or methylprednisolone if adrenal insufficiency suspected, levothyroxine only for myxedema coma, naloxone, thiamine.
Follow-Up And Disposition
Admission Criteria Moderate to severe hypothermia (<32°c).< />pan>
Discharge Criteria Young, healthy patients with very mild hypothermia who normalize and have a safe, warm environment.
Follow-Up Recommendations Social services involvement for patients at risk of recurrent cold exposure.
Key Points And Cautions Defibrillation is rarely effective below 28–30°C. Atrial fibrillation often resolves with rewarming alone. Beware afterdrop and rewarming shock. Gentle handling and adequate volume resuscitation are essential.

