- Published on
Pathology - Bacterial pneumonia
Definition: An infection of the lung parenchyma induced by bacterial pathogens.
Classification • Acquired inside the community. • Nosocomial. • Aspiration. • Immunosuppression.
Epidemiology • Extremely prevalent.
Microbiology • Community-acquired pathogens: Streptococcus pneumoniae, Mycoplasma pneumoniae, Haemophilus influenzae, Legionella pneumophila. • Hospital-acquired: Gram-negative bacteria, such as Klebsiella, Escherichia coli, and Pseudomonas. • Aspiration: a combination of aerobic and anaerobic bacteria. • Immunosuppression: all previously stated possibilities, including viral, mycobacterial, and Pneumocystis infections. Coexisting infections frequently occur in immunosuppressed individuals.
Pathogenesis Bacterial bypass the lung's defenses and initiate infection within the alveoli.
Presentation: • Productive cough, dyspnea, thoracic discomfort, and pyrexia. Macroscopy • The infected lung parenchyma exhibits a firm texture and a yellowish hue. • Purulent exudate may be expelled from minor air passages. The superficial pleura may exhibit signs of pleuritis. Histopathology The alveolar gaps are occupied by an inflammatory infiltrate abundant in neutrophils. Bacterial colonies are frequently discernible within the exudate. • In instances of aspiration pneumonia, alimentary substances may be found within the lung parenchyma. • Severe instances compounded by abscess formation exhibit loss of lung tissue, replaced by confluent sheets of neutrophils.
Prognosis • Recovery is typically anticipated with suitable antibiotic therapy in an otherwise healthy individual.
Complications encompass respiratory failure, septicaemia, pleural effusion, empyema, and lung abscess. These occurrences are more probable with pathogenic organisms or in people with concurrent cardiac and pulmonary conditions.
Definition: An infection of the lung parenchyma induced by bacterial pathogens.
Classification • Acquired inside the community. • Nosocomial. • Aspiration. • Immunosuppression.
Epidemiology • Extremely prevalent.
Microbiology • Community-acquired pathogens: Streptococcus pneumoniae, Mycoplasma pneumoniae, Haemophilus influenzae, Legionella pneumophila. • Hospital-acquired: Gram-negative bacteria, such as Klebsiella, Escherichia coli, and Pseudomonas. • Aspiration: a combination of aerobic and anaerobic bacteria. • Immunosuppression: all previously stated possibilities, including viral, mycobacterial, and Pneumocystis infections. Coexisting infections frequently occur in immunosuppressed individuals.
Pathogenesis Bacterial bypass the lung's defenses and initiate infection within the alveoli.
Presentation: • Productive cough, dyspnea, thoracic discomfort, and pyrexia. Macroscopy • The infected lung parenchyma exhibits a firm texture and a yellowish hue. • Purulent exudate may be expelled from minor air passages. The superficial pleura may exhibit signs of pleuritis. Histopathology The alveolar gaps are occupied by an inflammatory infiltrate abundant in neutrophils. Bacterial colonies are frequently discernible within the exudate. • In instances of aspiration pneumonia, alimentary substances may be found within the lung parenchyma. • Severe instances compounded by abscess formation exhibit loss of lung tissue, replaced by confluent sheets of neutrophils.
Prognosis • Recovery is typically anticipated with suitable antibiotic therapy in an otherwise healthy individual.
Complications encompass respiratory failure, septicaemia, pleural effusion, empyema, and lung abscess. These occurrences are more probable with pathogenic organisms or in people with concurrent cardiac and pulmonary conditions.

- Published on
Pathology - Chronic obstructive pulmonary disease (COPD)
Definition: A chronic pulmonary ailment marked by dyspnea resulting from poorly reversible and increasing airflow restriction.
Epidemiology • Extremely prevalent. Primarily a condition affecting middle-aged to older adult smokers.
Aetiology • The majority of instances are attributable to smoking. • Instances in younger individuals may result from A-1-antitrypsin deficiency. Pathogenesis Inflammation and scarring of tiny bronchioles are considered the primary cause of airflow obstruction. • An imbalance between proteases and antiproteases leads to the degradation of lung parenchyma, resulting in the dilatation of terminal airspaces (emphysema) and air trapping. • Hyperplasia of mucous glands and the irritative effects of smoking contribute to a productive cough (chronic bronchitis).
Presentation • Abrupt emergence of dyspnea during exertion, occurring against a history of chronic cough and sputum expectoration. • Spirometric analysis generally reveals a diminished FEV1 and a reduced FEV1/FVC ratio (Fig. 5.1). Macroscopy • The lungs exhibit hyperinflation, characterized by thick mucus in the airways and dilated terminal airspaces. • Bullae may be observed.
Histopathology • Persistent inflammation and fibrosis of tiny bronchioles (chronic obstructive bronchiolitis). • Highly pigmented macrophages in respiratory bronchioles (respiratory bronchiolitis). • Enlarged terminal airspaces (emphysema). Larger airways may exhibit mucus gland hyperplasia
.
Prognosis • Progressive deterioration of lung function accompanied by bouts of acute exacerbation resulting from infection, pneumothorax, or pulmonary embolism. • Subsequently, pulmonary hypertension and right ventricular failure manifest. Left ventricular failure frequently coexists with ischemic heart disease. • Mortality frequently associated with a conjunction of respiratory and heart failure
Definition: A chronic pulmonary ailment marked by dyspnea resulting from poorly reversible and increasing airflow restriction.
Epidemiology • Extremely prevalent. Primarily a condition affecting middle-aged to older adult smokers.
Aetiology • The majority of instances are attributable to smoking. • Instances in younger individuals may result from A-1-antitrypsin deficiency. Pathogenesis Inflammation and scarring of tiny bronchioles are considered the primary cause of airflow obstruction. • An imbalance between proteases and antiproteases leads to the degradation of lung parenchyma, resulting in the dilatation of terminal airspaces (emphysema) and air trapping. • Hyperplasia of mucous glands and the irritative effects of smoking contribute to a productive cough (chronic bronchitis).
Presentation • Abrupt emergence of dyspnea during exertion, occurring against a history of chronic cough and sputum expectoration. • Spirometric analysis generally reveals a diminished FEV1 and a reduced FEV1/FVC ratio (Fig. 5.1). Macroscopy • The lungs exhibit hyperinflation, characterized by thick mucus in the airways and dilated terminal airspaces. • Bullae may be observed.
Histopathology • Persistent inflammation and fibrosis of tiny bronchioles (chronic obstructive bronchiolitis). • Highly pigmented macrophages in respiratory bronchioles (respiratory bronchiolitis). • Enlarged terminal airspaces (emphysema). Larger airways may exhibit mucus gland hyperplasia
.
Prognosis • Progressive deterioration of lung function accompanied by bouts of acute exacerbation resulting from infection, pneumothorax, or pulmonary embolism. • Subsequently, pulmonary hypertension and right ventricular failure manifest. Left ventricular failure frequently coexists with ischemic heart disease. • Mortality frequently associated with a conjunction of respiratory and heart failure

- Published on
Pathology – Asthma
Definition
• A chronic inflammatory condition of the major airways marked by recurring episodes of reversible airway constriction.
Epidemiology: Highly prevalent, impacting over 10% of children and 5% of adults.
Aetiology • The majority of cases are linked to atopy, a hereditary predisposition of the immune system to generate IgE in reaction to prevalent environmental allergens. • The aetiology of non-atopic asthma remains ambiguous; nevertheless, some propose a connection with gastro-oesophageal reflux syndrome.
Pathogenesis: Atopic individuals react to prevalent environmental allergens by generating substantial quantities of allergen-specific IgE, which attaches to the surface of mast cells. • Subsequent exposure to the allergen results in the cross-linking of allergen-specific IgE antibodies and the degranulation of mast cells. Degranulated mast cells provoke airway inflammation and bronchospasm. Chronic inflammation leads to hypersensitive airways that respond to many stimuli, such as physical exertion, cold air, and tobacco smoke. Presentation: Intermittent episodes of dyspnea, wheezing, and chest constriction. Coughing, especially during nocturnal hours, is prevalent.
Macroscopy • The lungs of the majority of asthmatics may appear macroscopically normal. • In severe illness, thick mucus plugs may be observed in the airways.
Histopathology • The airways exhibit signs of inflammatory activity characterized by the presence of eosinophils, which are typically absent in normal airways. • Additionally, there may be thickening of the basement membrane, hyperplasia of goblet cells, and pronounced smooth muscle.
Prognosis: Generally favorable with suitable treatment. • A minor fatality rate is linked to severe acute asthma.
Definition
• A chronic inflammatory condition of the major airways marked by recurring episodes of reversible airway constriction.
Epidemiology: Highly prevalent, impacting over 10% of children and 5% of adults.
Aetiology • The majority of cases are linked to atopy, a hereditary predisposition of the immune system to generate IgE in reaction to prevalent environmental allergens. • The aetiology of non-atopic asthma remains ambiguous; nevertheless, some propose a connection with gastro-oesophageal reflux syndrome.
Pathogenesis: Atopic individuals react to prevalent environmental allergens by generating substantial quantities of allergen-specific IgE, which attaches to the surface of mast cells. • Subsequent exposure to the allergen results in the cross-linking of allergen-specific IgE antibodies and the degranulation of mast cells. Degranulated mast cells provoke airway inflammation and bronchospasm. Chronic inflammation leads to hypersensitive airways that respond to many stimuli, such as physical exertion, cold air, and tobacco smoke. Presentation: Intermittent episodes of dyspnea, wheezing, and chest constriction. Coughing, especially during nocturnal hours, is prevalent.
Macroscopy • The lungs of the majority of asthmatics may appear macroscopically normal. • In severe illness, thick mucus plugs may be observed in the airways.
Histopathology • The airways exhibit signs of inflammatory activity characterized by the presence of eosinophils, which are typically absent in normal airways. • Additionally, there may be thickening of the basement membrane, hyperplasia of goblet cells, and pronounced smooth muscle.
Prognosis: Generally favorable with suitable treatment. • A minor fatality rate is linked to severe acute asthma.

- Published on
Pathology - Pulmonary thromboembolism
Definition: Occlusion of a pulmonary artery by an embolic thrombus.
Epidemiology: Highly prevalent and frequently underdiagnosed.
Aetiology • Pulmonary emboli arise from deep vein thromboses, thus sharing identical risk factors, including immobility, acute medical conditions, recent surgical procedures, malignancy, pregnancy, and both inherited and acquired thrombotic diseases.
Pathogenesis: A piece of a detached thrombus from deep vein thrombosis embolizes via the right side of the heart into the pulmonary arterial circulation and becomes lodged in a pulmonary artery.
The clinical presentation is contingent upon the size of the pulmonary artery obstructed by the embolus. • Blockage of a large pulmonary artery usually leads to rapid death due to a sudden massive rise in pulmonary arterial pressure, acute right ventricular failure, and cardiac arrest. • Occlusion of medium-sized arteries results in a region of ventilation-perfusion imbalance in the lungs, leading to dyspnea. • Minor pulmonary emboli may produce mild manifestations of dyspnea, thoracic discomfort, and vertigo; these symptoms can often remain undetected.
Macroscopy
• Emboli appear as thrombi pieces within pulmonary arteries. • Thrombi are solid and brown, with the sliced surface potentially displaying discernible bands (lines of Zahn). Histopathology: Fresh thromboemboli consist of a composite of fibrin and interwoven blood cells, frequently organized in alternating linear bands that align with the macroscopic lines of Zahn. • Thromboemboli undergo organization after 2–3 days, characterized by the proliferation of granulation tissue consisting of fibroblasts and capillaries derived from the vessel wall. • Aged thromboemboli may manifest as fibrous nodules protruding from the vessel wall or as fibrous bands traversing the lumen of a pulmonary artery.
Prognosis
• Approximately 30% of all patients succumb to pulmonary embolism. • The mortalityz risk significantly increases if the diagnosis is not promptly established.
Definition: Occlusion of a pulmonary artery by an embolic thrombus.
Epidemiology: Highly prevalent and frequently underdiagnosed.
Aetiology • Pulmonary emboli arise from deep vein thromboses, thus sharing identical risk factors, including immobility, acute medical conditions, recent surgical procedures, malignancy, pregnancy, and both inherited and acquired thrombotic diseases.
Pathogenesis: A piece of a detached thrombus from deep vein thrombosis embolizes via the right side of the heart into the pulmonary arterial circulation and becomes lodged in a pulmonary artery.
The clinical presentation is contingent upon the size of the pulmonary artery obstructed by the embolus. • Blockage of a large pulmonary artery usually leads to rapid death due to a sudden massive rise in pulmonary arterial pressure, acute right ventricular failure, and cardiac arrest. • Occlusion of medium-sized arteries results in a region of ventilation-perfusion imbalance in the lungs, leading to dyspnea. • Minor pulmonary emboli may produce mild manifestations of dyspnea, thoracic discomfort, and vertigo; these symptoms can often remain undetected.
Macroscopy
• Emboli appear as thrombi pieces within pulmonary arteries. • Thrombi are solid and brown, with the sliced surface potentially displaying discernible bands (lines of Zahn). Histopathology: Fresh thromboemboli consist of a composite of fibrin and interwoven blood cells, frequently organized in alternating linear bands that align with the macroscopic lines of Zahn. • Thromboemboli undergo organization after 2–3 days, characterized by the proliferation of granulation tissue consisting of fibroblasts and capillaries derived from the vessel wall. • Aged thromboemboli may manifest as fibrous nodules protruding from the vessel wall or as fibrous bands traversing the lumen of a pulmonary artery.
Prognosis
• Approximately 30% of all patients succumb to pulmonary embolism. • The mortalityz risk significantly increases if the diagnosis is not promptly established.


- Published on
Cystic fibrosis
Definition: An hereditary condition resulting from a mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.
Epidemiology • The predominant fatal genetic disorder among European people. Approximately 1 in 2,500 infants born in the United Kingdom (UK) are diagnosed with cystic fibrosis (CF). Genetics: Inherited in an autosomal recessive fashion. The CFTR gene is located on chromosome 7q and encodes a chloride ion channel. More than 1,400 variants have been identified, with the most prevalent being a deletion at position 508 that results in the loss of a phenylalanine amino acid (the ZF508 mutation). The ZF508 mutation induces improper folding of the CFTR protein, leading to its breakdown within the cell. • Alternative mutations may yield a properly situated protein, however with dysfunctional activity. The absence of normal CFTR leads to impaired electrolyte transport across epithelial cell membranes, leading in the production of viscous mucus discharges.
Presentation • The majority of patients exhibit lung illness resulting from recurrent infections. Initially, typical bacteria inhabit the lungs; nevertheless, Pseudomonas aeruginosa frequently emerges as the predominant organism. Additionally, pancreatic insufficiency is prevalent. • Bowel obstruction might arise during the newborn period due to thick meconium (meconium ileus) or manifest later in childhood. • Liver illness manifests at a later stage. • Certain cases may be identified when elevated serum immunoreactive trypsin is detected during newborn screening.
Macroscopy • Lungs from older children typically have extensive bronchiectasis. • The liver may present with steatosis and, in severe instances, may be cirrhotic. Histopathology The lungs exhibit bronchiectatic airways filled with viscous mucus. Acute inflammation may occur in the presence of an active infection. The liver has thickened bile within the intrahepatic bile ducts. Periportal fibrosis may occur, which can advance to cirrhosis in more severe instances.
Prognosis: The average lifespan is presently approximately 35 years. • The majority of individuals succumb to pulmonary illness.
Definition: An hereditary condition resulting from a mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.
Epidemiology • The predominant fatal genetic disorder among European people. Approximately 1 in 2,500 infants born in the United Kingdom (UK) are diagnosed with cystic fibrosis (CF). Genetics: Inherited in an autosomal recessive fashion. The CFTR gene is located on chromosome 7q and encodes a chloride ion channel. More than 1,400 variants have been identified, with the most prevalent being a deletion at position 508 that results in the loss of a phenylalanine amino acid (the ZF508 mutation). The ZF508 mutation induces improper folding of the CFTR protein, leading to its breakdown within the cell. • Alternative mutations may yield a properly situated protein, however with dysfunctional activity. The absence of normal CFTR leads to impaired electrolyte transport across epithelial cell membranes, leading in the production of viscous mucus discharges.
Presentation • The majority of patients exhibit lung illness resulting from recurrent infections. Initially, typical bacteria inhabit the lungs; nevertheless, Pseudomonas aeruginosa frequently emerges as the predominant organism. Additionally, pancreatic insufficiency is prevalent. • Bowel obstruction might arise during the newborn period due to thick meconium (meconium ileus) or manifest later in childhood. • Liver illness manifests at a later stage. • Certain cases may be identified when elevated serum immunoreactive trypsin is detected during newborn screening.
Macroscopy • Lungs from older children typically have extensive bronchiectasis. • The liver may present with steatosis and, in severe instances, may be cirrhotic. Histopathology The lungs exhibit bronchiectatic airways filled with viscous mucus. Acute inflammation may occur in the presence of an active infection. The liver has thickened bile within the intrahepatic bile ducts. Periportal fibrosis may occur, which can advance to cirrhosis in more severe instances.
Prognosis: The average lifespan is presently approximately 35 years. • The majority of individuals succumb to pulmonary illness.

- Published on
Pathology – Bronchiectasis
Definition • A pathological, irreversible dilatation of the bronchi, characterized by inflammation in the bronchial walls and surrounding lung tissue. Epidemiology • Rare in developed nations. • Continues to be a significant source of morbidity in developing nations.
Aetiology
• A structural condition stemming from a variety of diverse causes. • In industrialized countries, bronchiectasis is frequently connected to obstruction to a region of lung (e.g. tumour or foreign body) or in conjunction with cystic fi brosis. Numerous instances are determined to be idiopathic. In less developed nations, serious pulmonary infections are a significant cause.
Pathogenesis
• Believed to be a consequence of the deterioration of bronchial walls due to chronic inflammation. Scarring in the surrounding lung parenchyma exerts traction on the compromised bronchi, resulting in their permanent dilation.
Presentation: • Chronic productive cough and hemoptysis, potentially severe.
Macroscopy • The affected lung regions exhibit obviously dilated airways filled with mucopurulent material, extending to the pleural surface. • In obstructive instances, the etiology may be observed proximally, such as a neoplasm. Histopathology: Bronchial dilatation accompanied by significant chronic inflammation in the wall, frequently with lymphoid clusters and germinal centers. • Neighboring alveoli may exhibit acute and organizing pneumonia. Complications include pulmonary hypertension and right ventricular failure. • Accumulation of serum amyloid A protein in B-pleated sheets throughout many organs (AA amyloidosis)
Definition • A pathological, irreversible dilatation of the bronchi, characterized by inflammation in the bronchial walls and surrounding lung tissue. Epidemiology • Rare in developed nations. • Continues to be a significant source of morbidity in developing nations.
Aetiology
• A structural condition stemming from a variety of diverse causes. • In industrialized countries, bronchiectasis is frequently connected to obstruction to a region of lung (e.g. tumour or foreign body) or in conjunction with cystic fi brosis. Numerous instances are determined to be idiopathic. In less developed nations, serious pulmonary infections are a significant cause.
Pathogenesis
• Believed to be a consequence of the deterioration of bronchial walls due to chronic inflammation. Scarring in the surrounding lung parenchyma exerts traction on the compromised bronchi, resulting in their permanent dilation.
Presentation: • Chronic productive cough and hemoptysis, potentially severe.
Macroscopy • The affected lung regions exhibit obviously dilated airways filled with mucopurulent material, extending to the pleural surface. • In obstructive instances, the etiology may be observed proximally, such as a neoplasm. Histopathology: Bronchial dilatation accompanied by significant chronic inflammation in the wall, frequently with lymphoid clusters and germinal centers. • Neighboring alveoli may exhibit acute and organizing pneumonia. Complications include pulmonary hypertension and right ventricular failure. • Accumulation of serum amyloid A protein in B-pleated sheets throughout many organs (AA amyloidosis)

- Published on
Pathology - Acute Respiratory Distress Syndrome
Definition: A critical form of acute lung injury characterized by a PaO2:FiO2 ratio of less than 200 mmHg, accompanied by bilateral alveolar infiltrates on chest X-ray, and occurring in the absence of left ventricular failure.
Epidemiology: Rare occurrence.
Aetiology • Any significant lung injury may result in acute respiratory distress syndrome (ARDS). • Frequent etiologies encompass acute pneumonia, shock, trauma, numerous transfusions, and near-drowning. Pathogenesis • Significant lung injury results in extensive alveolar necrosis, severely disrupting normal gas exchange.
Presentation
• Intense dyspnea accompanied by indications of the underlying etiology. Macroscopy • Both lungs are generally significantly heavy and fluid-filled, frequently exceeding 1000g each (a normal lung weighs 730–400g). Histopathology • The histopathological signature is diffuse alveolar destruction, defined by hyaline membranes lining the alveolar spaces. • Hyaline membranes consist of a mixture of fibrin and necrotic alveolar epithelial cells.
Prognosis: A grave condition with fatality rates ranging from 30% to 50%, contingent upon the underlying etiology. • Survivors typically exhibit persistent pulmonary functional impairments.
Definition: A critical form of acute lung injury characterized by a PaO2:FiO2 ratio of less than 200 mmHg, accompanied by bilateral alveolar infiltrates on chest X-ray, and occurring in the absence of left ventricular failure.
Epidemiology: Rare occurrence.
Aetiology • Any significant lung injury may result in acute respiratory distress syndrome (ARDS). • Frequent etiologies encompass acute pneumonia, shock, trauma, numerous transfusions, and near-drowning. Pathogenesis • Significant lung injury results in extensive alveolar necrosis, severely disrupting normal gas exchange.
Presentation
• Intense dyspnea accompanied by indications of the underlying etiology. Macroscopy • Both lungs are generally significantly heavy and fluid-filled, frequently exceeding 1000g each (a normal lung weighs 730–400g). Histopathology • The histopathological signature is diffuse alveolar destruction, defined by hyaline membranes lining the alveolar spaces. • Hyaline membranes consist of a mixture of fibrin and necrotic alveolar epithelial cells.
Prognosis: A grave condition with fatality rates ranging from 30% to 50%, contingent upon the underlying etiology. • Survivors typically exhibit persistent pulmonary functional impairments.

- Published on
Pathology - Respiratory failure
Definition: Arterial pO2
Definition: Arterial pO2
- Published on
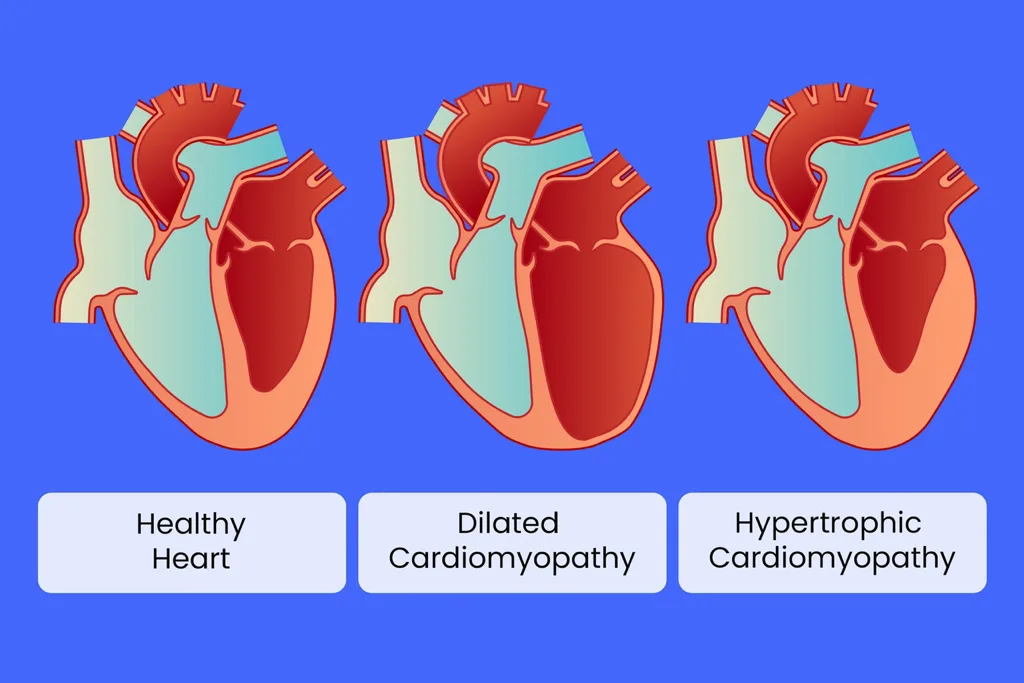
Pathology – Cardiomyopathies
Hypertrophic cardiomyopathy
• Rare, having an incidence of 0.5%. • 770% of cases have been associated with mutations in genes that encode sarcomeric proteins, including β-myosin heavy chain, troponin T, myosin binding protein, and α-tropomyosin. • A broad range of manifestations, including dyspnea, angina pectoris, syncope, palpitations, and abrupt mortality.
Macroscopically, the majority of patients exhibit asymmetric left ventricular hypertrophy, primarily affecting the septum. Associated systolic anterior motion of the mitral valve frequently results in a localized area of endocardial fibrosis on the septum, referred to as the sub-aortic mitral impact lesion. In many instances, this condition induces symmetric left ventricular hypertrophy that is indistinguishable from that resulting from hypertension or aortic stenosis. • The histological characteristic of HCM is the presence of myocyte enlargement, myocyte disorganization, and interstitial fibrosis. Myocyte disarray denotes the disruption of the typical parallel alignment of myocytes, which instead assume random oblique configurations.
Idiopathic dilated cardiomyopathy
• Rare, having an incidence of 0.2%. • The modes of inheritance encompass autosomal dominant, X-linked, autosomal recessive, and mitochondrial inheritance. • Numerous gene mutations have been identified, including those in cardiac actin, desmin, sarcoglycan, troponin, and tropomyosin.
• Clinical manifestations include dyspnea, fatigue, and palpitations. Thrombus formation on the akinetic myocardium may lead to systemic emboli. The heart exhibits increased mass with dilatation and thinning of the cardiac chambers, with no identifiable reason such as coronary artery disease, valve disease, hypertension, or alcohol misuse.
Microscopic findings are nonspecific but may exhibit myocyte attenuation and myofibril loss, accompanied by enlarged myocyte nuclei and interstitial fibrosis.
Arrhythmogenic right ventricular cardiomyopathy
The precise incidence and prevalence within the general population are undetermined. • Mutations in genes that encode cell adhesion molecules are delineated. Mutations result in the separation and apoptosis of myocytes under mechanical stress, followed by fat replacement and scarring. • Exhibits palpitations or experiences abrupt death.
Macroscopically, the right ventricle exhibits thinning, particularly in the right ventricular outflow tract, characterized by a yellow hue attributed to fat replacement.
• Microscopically, the normal right ventricular myocardium is replaced by adipose tissue and fibrosis. The illness process typically initiates in the epicardial region and progresses toward the endocardial surface.
Hypertrophic cardiomyopathy
• Rare, having an incidence of 0.5%. • 770% of cases have been associated with mutations in genes that encode sarcomeric proteins, including β-myosin heavy chain, troponin T, myosin binding protein, and α-tropomyosin. • A broad range of manifestations, including dyspnea, angina pectoris, syncope, palpitations, and abrupt mortality.
Macroscopically, the majority of patients exhibit asymmetric left ventricular hypertrophy, primarily affecting the septum. Associated systolic anterior motion of the mitral valve frequently results in a localized area of endocardial fibrosis on the septum, referred to as the sub-aortic mitral impact lesion. In many instances, this condition induces symmetric left ventricular hypertrophy that is indistinguishable from that resulting from hypertension or aortic stenosis. • The histological characteristic of HCM is the presence of myocyte enlargement, myocyte disorganization, and interstitial fibrosis. Myocyte disarray denotes the disruption of the typical parallel alignment of myocytes, which instead assume random oblique configurations.
Idiopathic dilated cardiomyopathy
• Rare, having an incidence of 0.2%. • The modes of inheritance encompass autosomal dominant, X-linked, autosomal recessive, and mitochondrial inheritance. • Numerous gene mutations have been identified, including those in cardiac actin, desmin, sarcoglycan, troponin, and tropomyosin.
• Clinical manifestations include dyspnea, fatigue, and palpitations. Thrombus formation on the akinetic myocardium may lead to systemic emboli. The heart exhibits increased mass with dilatation and thinning of the cardiac chambers, with no identifiable reason such as coronary artery disease, valve disease, hypertension, or alcohol misuse.
Microscopic findings are nonspecific but may exhibit myocyte attenuation and myofibril loss, accompanied by enlarged myocyte nuclei and interstitial fibrosis.
Arrhythmogenic right ventricular cardiomyopathy
The precise incidence and prevalence within the general population are undetermined. • Mutations in genes that encode cell adhesion molecules are delineated. Mutations result in the separation and apoptosis of myocytes under mechanical stress, followed by fat replacement and scarring. • Exhibits palpitations or experiences abrupt death.
Macroscopically, the right ventricle exhibits thinning, particularly in the right ventricular outflow tract, characterized by a yellow hue attributed to fat replacement.
• Microscopically, the normal right ventricular myocardium is replaced by adipose tissue and fibrosis. The illness process typically initiates in the epicardial region and progresses toward the endocardial surface.
- Published on
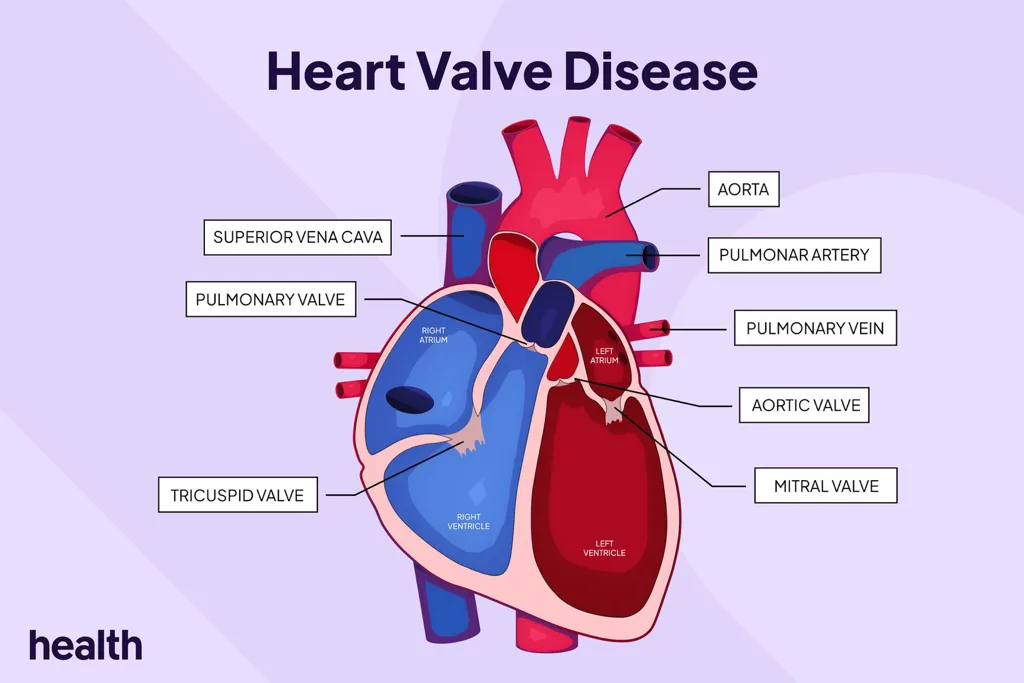
Pathology - Valvular cardiac pathology
Aortic stenosis
• The predominant valve pathology. • Primarily results from calcification of a structurally normal tricuspid valve in the elderly (senile calcific aortic stenosis). Bicuspid aortic valves undergo calcification at an earlier age. Chronic rheumatic illness can potentially lead to aortic stenosis. • Prolonged turbulent blood flow through the valve is believed to result in damage, subsequently leading to calcification. • Exhibits chest discomfort, syncope, and dyspnea.
Aortic regurgitation
• Aortic regurgitation (AR) can result from disorders that induce dilation of the aortic root, such as Marfan syndrome and ankylosing spondylitis. • Congenital anomalies of the valve leaflets may also contribute to AR. • Dilation of the aortic root exerts tension on the annulus of the aortic valve, hindering complete closure of the leaflets. • Symptoms include dyspnea and palpitations.
Mitral Stenosis
Mitral stenosis is typically a consequence of persistent rheumatic valvular heart disease. • The constriction of the valve obstructs the unobstructed flow of blood from the left atrium to the left ventricle during ventricular diastole. • The increase in left atrial pressure is conveyed to the pulmonary venous system, resulting in pulmonary edema and dyspnea. • The left atrium enlarges and becomes susceptible to atrial fibrillation. • Stenotic mitral valves exhibit significant thickening of the valve leaflets and the associated chordae tendineae. The fusion of the leaflets results in the characteristic 'fish mouth' appearance.
Mitral regurgitation
• Typically results from mitral valve prolapse or ischemic heart disease. • In mitral valve prolapse, the abnormal valve leaflets bulge into the left atrium during ventricular systole. • In ischemic heart disease, regurgitation arises from a combination of ischemic papillary dysfunction and the dilation of the mitral valve annulus due to left ventricular enlargement. • Patients may stay asymptomatic for a period as the left ventricle and left atrium hypertrophy to accommodate the additional volume; however, decompensation and the onset of left ventricular failure will ultimately occur.
Aortic stenosis
• The predominant valve pathology. • Primarily results from calcification of a structurally normal tricuspid valve in the elderly (senile calcific aortic stenosis). Bicuspid aortic valves undergo calcification at an earlier age. Chronic rheumatic illness can potentially lead to aortic stenosis. • Prolonged turbulent blood flow through the valve is believed to result in damage, subsequently leading to calcification. • Exhibits chest discomfort, syncope, and dyspnea.
Aortic regurgitation
• Aortic regurgitation (AR) can result from disorders that induce dilation of the aortic root, such as Marfan syndrome and ankylosing spondylitis. • Congenital anomalies of the valve leaflets may also contribute to AR. • Dilation of the aortic root exerts tension on the annulus of the aortic valve, hindering complete closure of the leaflets. • Symptoms include dyspnea and palpitations.
Mitral Stenosis
Mitral stenosis is typically a consequence of persistent rheumatic valvular heart disease. • The constriction of the valve obstructs the unobstructed flow of blood from the left atrium to the left ventricle during ventricular diastole. • The increase in left atrial pressure is conveyed to the pulmonary venous system, resulting in pulmonary edema and dyspnea. • The left atrium enlarges and becomes susceptible to atrial fibrillation. • Stenotic mitral valves exhibit significant thickening of the valve leaflets and the associated chordae tendineae. The fusion of the leaflets results in the characteristic 'fish mouth' appearance.
Mitral regurgitation
• Typically results from mitral valve prolapse or ischemic heart disease. • In mitral valve prolapse, the abnormal valve leaflets bulge into the left atrium during ventricular systole. • In ischemic heart disease, regurgitation arises from a combination of ischemic papillary dysfunction and the dilation of the mitral valve annulus due to left ventricular enlargement. • Patients may stay asymptomatic for a period as the left ventricle and left atrium hypertrophy to accommodate the additional volume; however, decompensation and the onset of left ventricular failure will ultimately occur.