- Published on
Pathology – Infective endocarditis
Definition
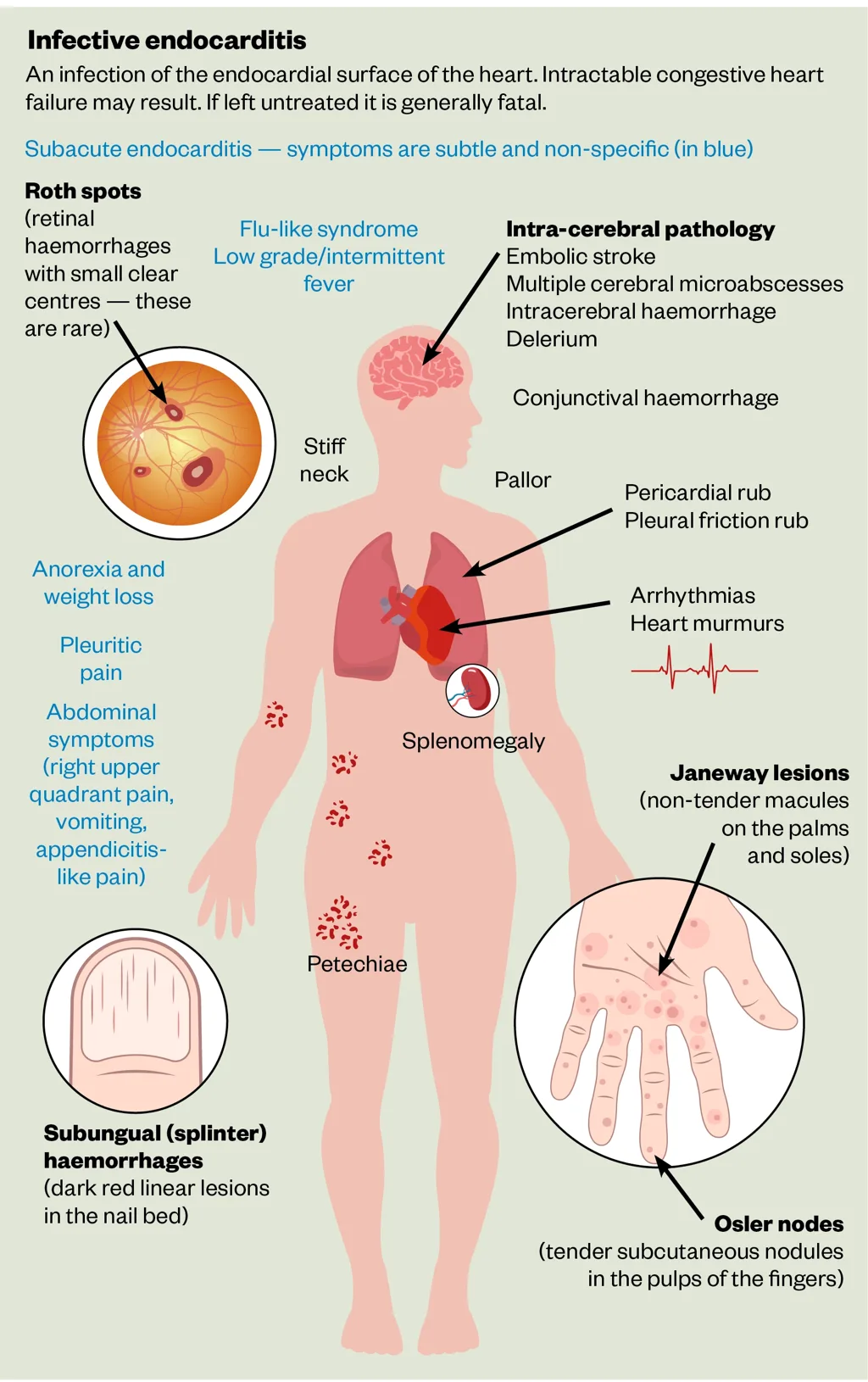
• An infection of the inner surface of the heart, typically involving a heart valve.
Classification
• Acute endocarditis is induced by pathogenic organisms infecting a structurally intact heart. Subacute endocarditis is a gradual sickness induced by mildly pathogenic organisms invading a structurally compromised heart. Epidemiology • Rare, yet crucial to identify.
Microbiology
• Acute endocarditis is typically caused by Staphylococcus aureus. Subacute endocarditis is predominantly caused by Streptococcus (S.) viridans or Enterococci.
Pathogenesis
S. aureus typically enters the bloodstream through the skin via indwelling vascular catheters or intravenous medication usage. S. viridans enters the bloodstream from the oropharynx subsequent to tooth brushing or dental procedures. Enterococci enter the bloodstream subsequent to intestinal instrumentation (endoscopy) or bladder instrumentation (cystoscopy or catheterization).
Presentation
Left-sided acute endocarditis manifests abruptly with fever and indications of valve impairment. Significant systemic embolic occurrences are prevalent; septic emboli may disseminate to several organs and induce abscess formation. Right-sided acute endocarditis manifests with fever, chills, and significant pulmonary symptoms resulting from many septic emboli in the lungs. Subacute endocarditis induces low-grade fever and systemic symptoms. The diagnosis may be challenging and readily disregarded.
Macroscopy
• The affected endocardial surface is adorned with fragile vegetations. • Acute cases may exhibit significant underlying tissue damage and abscess development.
Histopathology
Vegetations consist of a combination of fibrin, inflammatory cells, and bacterial colonies, predominantly comprising Gram-positive cocci in nearly all instances.
Prognosis • immediate endocarditis has a high death rate due to swift valve degradation and the onset of immediate heart failure. • Subacute endocarditis follows a more extended trajectory, although remains a grave condition if not recognized and treated.
Definition
• An infection of the inner surface of the heart, typically involving a heart valve.
Classification
• Acute endocarditis is induced by pathogenic organisms infecting a structurally intact heart. Subacute endocarditis is a gradual sickness induced by mildly pathogenic organisms invading a structurally compromised heart. Epidemiology • Rare, yet crucial to identify.
Microbiology
• Acute endocarditis is typically caused by Staphylococcus aureus. Subacute endocarditis is predominantly caused by Streptococcus (S.) viridans or Enterococci.
Pathogenesis
S. aureus typically enters the bloodstream through the skin via indwelling vascular catheters or intravenous medication usage. S. viridans enters the bloodstream from the oropharynx subsequent to tooth brushing or dental procedures. Enterococci enter the bloodstream subsequent to intestinal instrumentation (endoscopy) or bladder instrumentation (cystoscopy or catheterization).
Presentation
Left-sided acute endocarditis manifests abruptly with fever and indications of valve impairment. Significant systemic embolic occurrences are prevalent; septic emboli may disseminate to several organs and induce abscess formation. Right-sided acute endocarditis manifests with fever, chills, and significant pulmonary symptoms resulting from many septic emboli in the lungs. Subacute endocarditis induces low-grade fever and systemic symptoms. The diagnosis may be challenging and readily disregarded.
Macroscopy
• The affected endocardial surface is adorned with fragile vegetations. • Acute cases may exhibit significant underlying tissue damage and abscess development.
Histopathology
Vegetations consist of a combination of fibrin, inflammatory cells, and bacterial colonies, predominantly comprising Gram-positive cocci in nearly all instances.
Prognosis • immediate endocarditis has a high death rate due to swift valve degradation and the onset of immediate heart failure. • Subacute endocarditis follows a more extended trajectory, although remains a grave condition if not recognized and treated.
- Published on
Pathology - Right ventricular failure
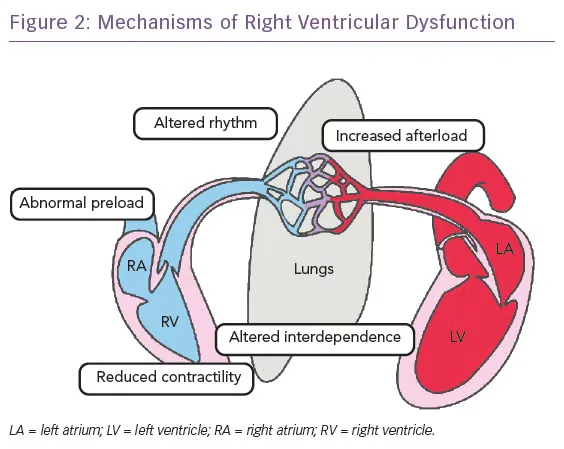
Definition: A syndrome caused by inadequate right ventricular output.
Epidemiology • Rare. • Observed far less often than LVF. Aetiology Most instances are attributable to chronic pulmonary conditions, including chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, bronchiectasis, and recurrent pulmonary emboli. Less common etiologies including ischemic heart disease impacting the right ventricle and right-sided valvular heart disease.
Pathogenesis • In the majority of instances, right ventricular failure (RVF) arises from pulmonary hypertension induced by chronic pulmonary conditions. • Pulmonary hypertension elevates the workload of the right ventricle by necessitating increased chamber pressure to sustain sufficient output. • Initially, right ventricular hypertrophy occurs, but ultimately, the chamber undergoes dilation and failure
.Presentation: • Deterioration of pre-existing dyspnea and onset of peripheral edema.
Macroscopy • The right ventricle exhibits hypertrophy and dilation. Histopathology • Histology is non-specific, typically exhibiting patchy myocyte hypertrophy or atrophy accompanied by interstitial fibrosis.
Prognosis • Elevated risk of mortality due to concurrent cardiac and respiratory failure. • Numerous patients experience abrupt death from a lethal ventricular arrhythmia originating in the compromised right ventricle.
Definition: A syndrome caused by inadequate right ventricular output.
Epidemiology • Rare. • Observed far less often than LVF. Aetiology Most instances are attributable to chronic pulmonary conditions, including chronic obstructive pulmonary disease (COPD), pulmonary fibrosis, bronchiectasis, and recurrent pulmonary emboli. Less common etiologies including ischemic heart disease impacting the right ventricle and right-sided valvular heart disease.
Pathogenesis • In the majority of instances, right ventricular failure (RVF) arises from pulmonary hypertension induced by chronic pulmonary conditions. • Pulmonary hypertension elevates the workload of the right ventricle by necessitating increased chamber pressure to sustain sufficient output. • Initially, right ventricular hypertrophy occurs, but ultimately, the chamber undergoes dilation and failure
.Presentation: • Deterioration of pre-existing dyspnea and onset of peripheral edema.
Macroscopy • The right ventricle exhibits hypertrophy and dilation. Histopathology • Histology is non-specific, typically exhibiting patchy myocyte hypertrophy or atrophy accompanied by interstitial fibrosis.
Prognosis • Elevated risk of mortality due to concurrent cardiac and respiratory failure. • Numerous patients experience abrupt death from a lethal ventricular arrhythmia originating in the compromised right ventricle.
- Published on
Pathology – left Ventricular Failure
Left ventricular failure
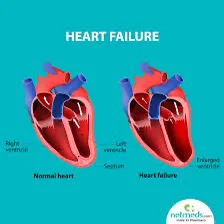
Definition: A syndrome caused by inadequate left ventricular output.
Epidemiology
• Extremely prevalent. • Occurs in approximately 1% of individuals beyond the age of 75 and 2% after 80 years.
Aetiology
• Ischemic heart disease. • Hypertensive cardiomyopathy. • Aortic or mitral valve pathology. 2 It is important to recognize that all of these are prevalent, and hence LVF frequently results from a combination of two or more of these illnesses.
Pathogenesis
Decreased cardiac output results in a reduction of blood pressure. Hypotension activates baroreceptors and diminishes renal perfusion. • This results in sympathetic overactivity and the stimulation of the renin-angiotensin-aldosterone system. • Blood pressure is reinstated at the cost of elevated heart rate, heightened peripheral vascular resistance (afterload), and augmented blood volume (preload). • Regrettably, this temporary remedy is detrimental in the long term, as it further exacerbates the workload of the heart.
• In reaction, the left ventricle experiences hypertrophy, which diminishes the capacity of the ventricular cavity and decreases the stroke volume. • Ultimately, the heart gets engorged with blood and suffers dilation. Presentation: Dyspnea, tiredness, palpitations. Peripheral edema and ascites typically manifest in advanced stages of the disease.
Macroscopy
• The heart exhibits increased weight, with hypertrophy and dilation of the left ventricle. • Potential underlying causes may be observable, such as coronary artery atherosclerosis or valve disease.
Histopathology
Histology is non-specific, typically exhibiting patchy myocyte enlargement and interstitial fibrosis due to persistent chamber damage.
Prognosis: • Dismal prognosis, with numerous individuals succumbing within three years of diagnosis. • Correlated with diminished quality of life and recurrent hospitalizations. • Lethal ventricular arrhythmias are a prevalent cause of abrupt mortality.
Left ventricular failure
Definition: A syndrome caused by inadequate left ventricular output.
Epidemiology
• Extremely prevalent. • Occurs in approximately 1% of individuals beyond the age of 75 and 2% after 80 years.
Aetiology
• Ischemic heart disease. • Hypertensive cardiomyopathy. • Aortic or mitral valve pathology. 2 It is important to recognize that all of these are prevalent, and hence LVF frequently results from a combination of two or more of these illnesses.
Pathogenesis
Decreased cardiac output results in a reduction of blood pressure. Hypotension activates baroreceptors and diminishes renal perfusion. • This results in sympathetic overactivity and the stimulation of the renin-angiotensin-aldosterone system. • Blood pressure is reinstated at the cost of elevated heart rate, heightened peripheral vascular resistance (afterload), and augmented blood volume (preload). • Regrettably, this temporary remedy is detrimental in the long term, as it further exacerbates the workload of the heart.
• In reaction, the left ventricle experiences hypertrophy, which diminishes the capacity of the ventricular cavity and decreases the stroke volume. • Ultimately, the heart gets engorged with blood and suffers dilation. Presentation: Dyspnea, tiredness, palpitations. Peripheral edema and ascites typically manifest in advanced stages of the disease.
Macroscopy
• The heart exhibits increased weight, with hypertrophy and dilation of the left ventricle. • Potential underlying causes may be observable, such as coronary artery atherosclerosis or valve disease.
Histopathology
Histology is non-specific, typically exhibiting patchy myocyte enlargement and interstitial fibrosis due to persistent chamber damage.
Prognosis: • Dismal prognosis, with numerous individuals succumbing within three years of diagnosis. • Correlated with diminished quality of life and recurrent hospitalizations. • Lethal ventricular arrhythmias are a prevalent cause of abrupt mortality.
- Published on
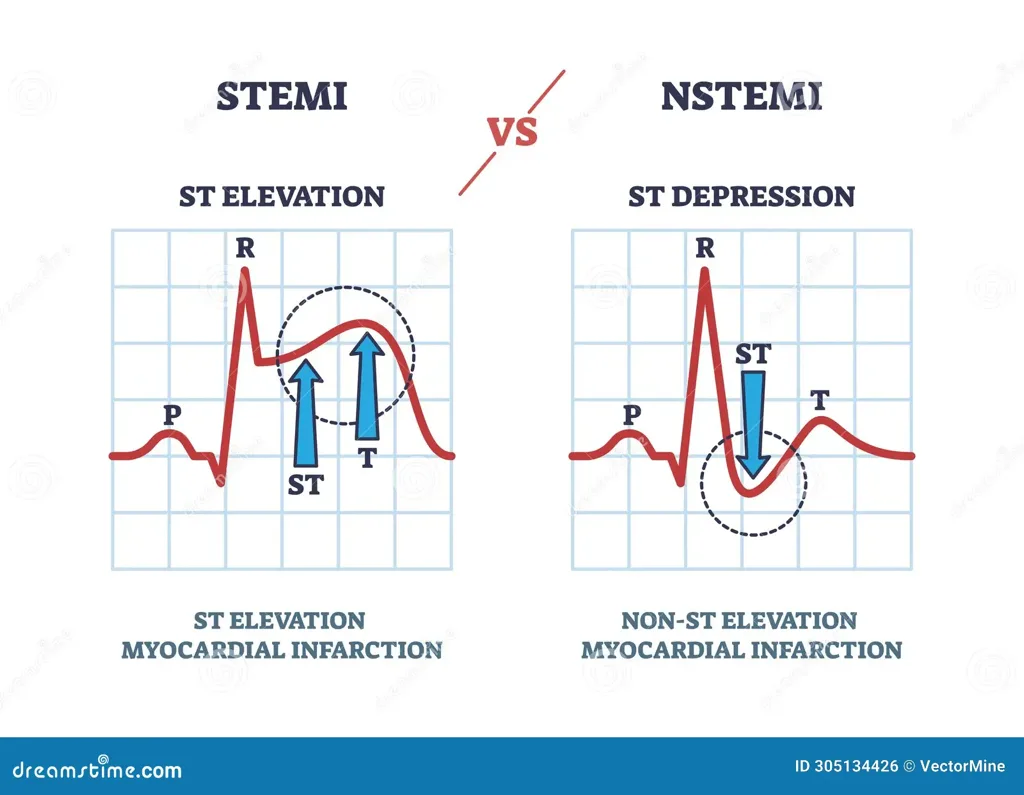
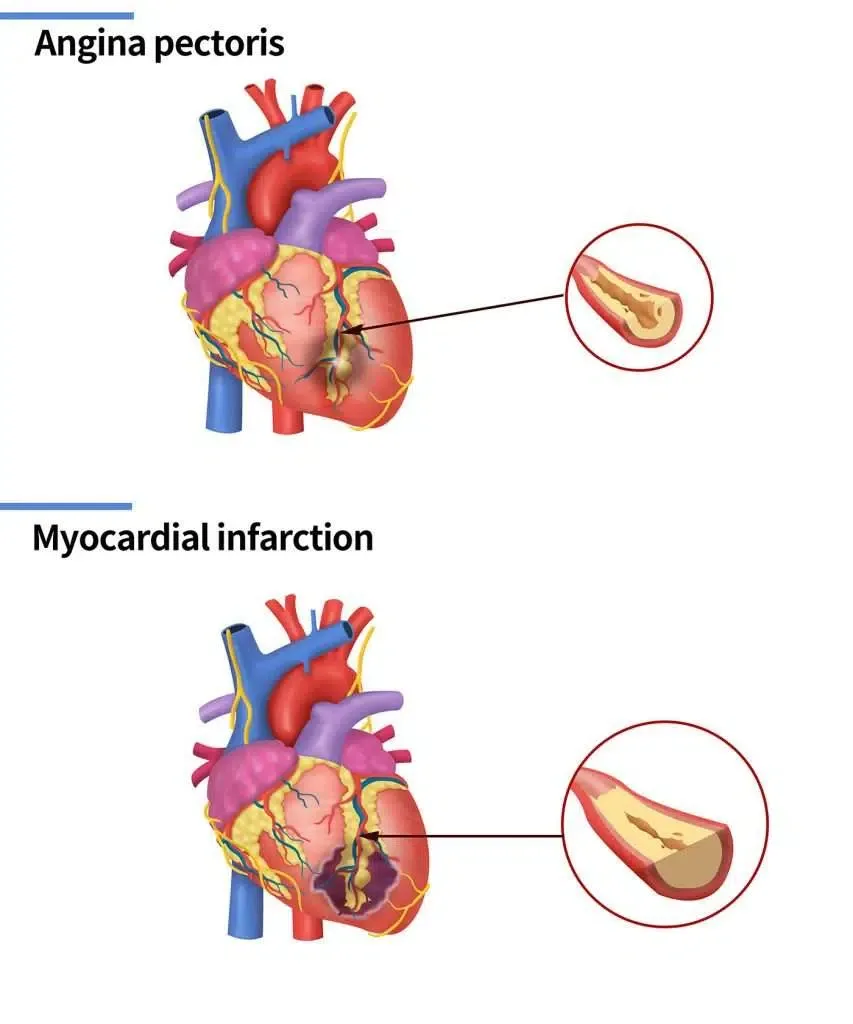
Pathology - ST-elevation myocardial infarction
Definition: Complete thickness necrosis of a region of the myocardium.
Epidemiology • Extremely prevalent.
Aetiology • Nearly invariably a consequence of coronary artery atherosclerosis.
Pathogenesis
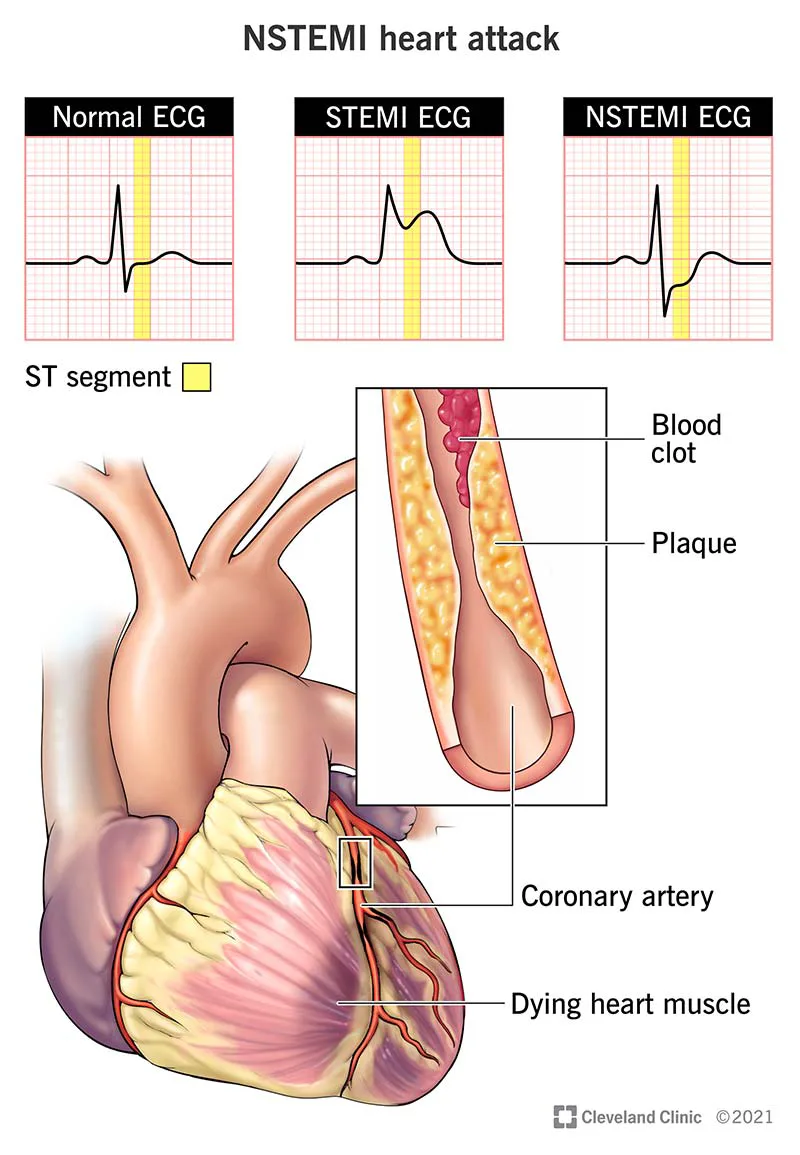
The rupture of an unstable atherosclerotic plaque in a coronary artery induces the creation of an occlusive thrombus rich in fibrin above the plaque. Complete closure of the coronary artery results in transmural necrosis of the myocardial region fed by that artery
Presentation • Persistent severe ischemic cardiac chest discomfort. • Patients frequently report a sensation akin to impending death. • The ECG displays ST-elevation or newly developed left bundle branch block. Biochemistry • Blood troponin concentrations are increased.
Macroscopy • The impacted coronary artery exhibits total obstruction due to a thrombus overlaying an atherosclerotic plaque. The infarcted myocardium becomes apparent approximately 15 hours post-event, presenting as mushy, enlarged, and exhibiting a darker red hue. • Within 24 to 48 hours, the infarct becomes yellow. Over weeks to months, the infarct is substituted by white scar tissue, resulting in a thinner ventricular wall.
Histopathology
The initial alteration in myocardial infarction is cytoplasmic eosinophilia and the loss of nuclei in the afflicted myocytes occurring approximately 8 to 12 hours post-infarction. • Within 24 hours, neutrophils infiltrate the necrotic region, and after several days, granulation tissue is established. • Over the course of weeks to months, the granulation tissue is supplanted by fibrous scar tissue.
Prognosis: Immediate problems encompass ventricular arrhythmias, which can be deadly, and abrupt heart failure in extreme instances. Rupture of the infarcted ventricular free wall results in hemopericardium, leading to fast cardiac tamponade and mortality. A thrombus that develops on akinetic myocardium may dislodge and result in systemic emboli. Subsequent difficulties encompass the creation of ventricular aneurysms and the emergence of left ventricular (LV) issues.
Definition: Complete thickness necrosis of a region of the myocardium.
Epidemiology • Extremely prevalent.
Aetiology • Nearly invariably a consequence of coronary artery atherosclerosis.
Pathogenesis
The rupture of an unstable atherosclerotic plaque in a coronary artery induces the creation of an occlusive thrombus rich in fibrin above the plaque. Complete closure of the coronary artery results in transmural necrosis of the myocardial region fed by that artery
Presentation • Persistent severe ischemic cardiac chest discomfort. • Patients frequently report a sensation akin to impending death. • The ECG displays ST-elevation or newly developed left bundle branch block. Biochemistry • Blood troponin concentrations are increased.
Macroscopy • The impacted coronary artery exhibits total obstruction due to a thrombus overlaying an atherosclerotic plaque. The infarcted myocardium becomes apparent approximately 15 hours post-event, presenting as mushy, enlarged, and exhibiting a darker red hue. • Within 24 to 48 hours, the infarct becomes yellow. Over weeks to months, the infarct is substituted by white scar tissue, resulting in a thinner ventricular wall.
Histopathology
The initial alteration in myocardial infarction is cytoplasmic eosinophilia and the loss of nuclei in the afflicted myocytes occurring approximately 8 to 12 hours post-infarction. • Within 24 hours, neutrophils infiltrate the necrotic region, and after several days, granulation tissue is established. • Over the course of weeks to months, the granulation tissue is supplanted by fibrous scar tissue.
Prognosis: Immediate problems encompass ventricular arrhythmias, which can be deadly, and abrupt heart failure in extreme instances. Rupture of the infarcted ventricular free wall results in hemopericardium, leading to fast cardiac tamponade and mortality. A thrombus that develops on akinetic myocardium may dislodge and result in systemic emboli. Subsequent difficulties encompass the creation of ventricular aneurysms and the emergence of left ventricular (LV) issues.
- Published on
Pathology - Non-ST-elevation myocardial infarction
Definition: Partial thickness necrosis of a region of the myocardium.
Epidemiology • Extremely prevalent.
Aetiology
• Primarily attributable to coronary artery atherosclerosis.
Pathogenesis
• The rupture or fissuring of an unstable atherosclerotic plaque triggers the development of a platelet-rich thrombus. • This thrombus results in considerable and protracted arterial constriction, leading to ischemic necrosis in a portion of the myocardium supplied by the affected artery.
Presentation
• Acute coronary syndrome characterized by prolonged ischemic cardiac chest discomfort at rest or with minimal exertion. • ECG reveals ischemic alterations without ST-elevation. Biochemistry • Elevated blood troponin levels are observed. Macroscopy • Notable narrowing of the affected coronary artery due to a complex atherosclerotic plaque.
Histopathology
• The initial alteration in myocardial infarction is heightened cytoplasmic eosinophilia and the absence of nuclei in the afflicted myocytes approximately 8–12 hours post-infarction. • Within 24 hours, neutrophils infiltrate the necrotic region, and after several days, granulation tissue is established. • Over the course of many weeks, the granulation tissue is substituted by scar tissue.
Prognosis: Patients have a significant risk of future acute coronary episodes and the subsequent development of left ventricular dysfunction.
Definition: Partial thickness necrosis of a region of the myocardium.
Epidemiology • Extremely prevalent.
Aetiology
• Primarily attributable to coronary artery atherosclerosis.
Pathogenesis
• The rupture or fissuring of an unstable atherosclerotic plaque triggers the development of a platelet-rich thrombus. • This thrombus results in considerable and protracted arterial constriction, leading to ischemic necrosis in a portion of the myocardium supplied by the affected artery.
Presentation
• Acute coronary syndrome characterized by prolonged ischemic cardiac chest discomfort at rest or with minimal exertion. • ECG reveals ischemic alterations without ST-elevation. Biochemistry • Elevated blood troponin levels are observed. Macroscopy • Notable narrowing of the affected coronary artery due to a complex atherosclerotic plaque.
Histopathology
• The initial alteration in myocardial infarction is heightened cytoplasmic eosinophilia and the absence of nuclei in the afflicted myocytes approximately 8–12 hours post-infarction. • Within 24 hours, neutrophils infiltrate the necrotic region, and after several days, granulation tissue is established. • Over the course of many weeks, the granulation tissue is substituted by scar tissue.
Prognosis: Patients have a significant risk of future acute coronary episodes and the subsequent development of left ventricular dysfunction.
- Published on
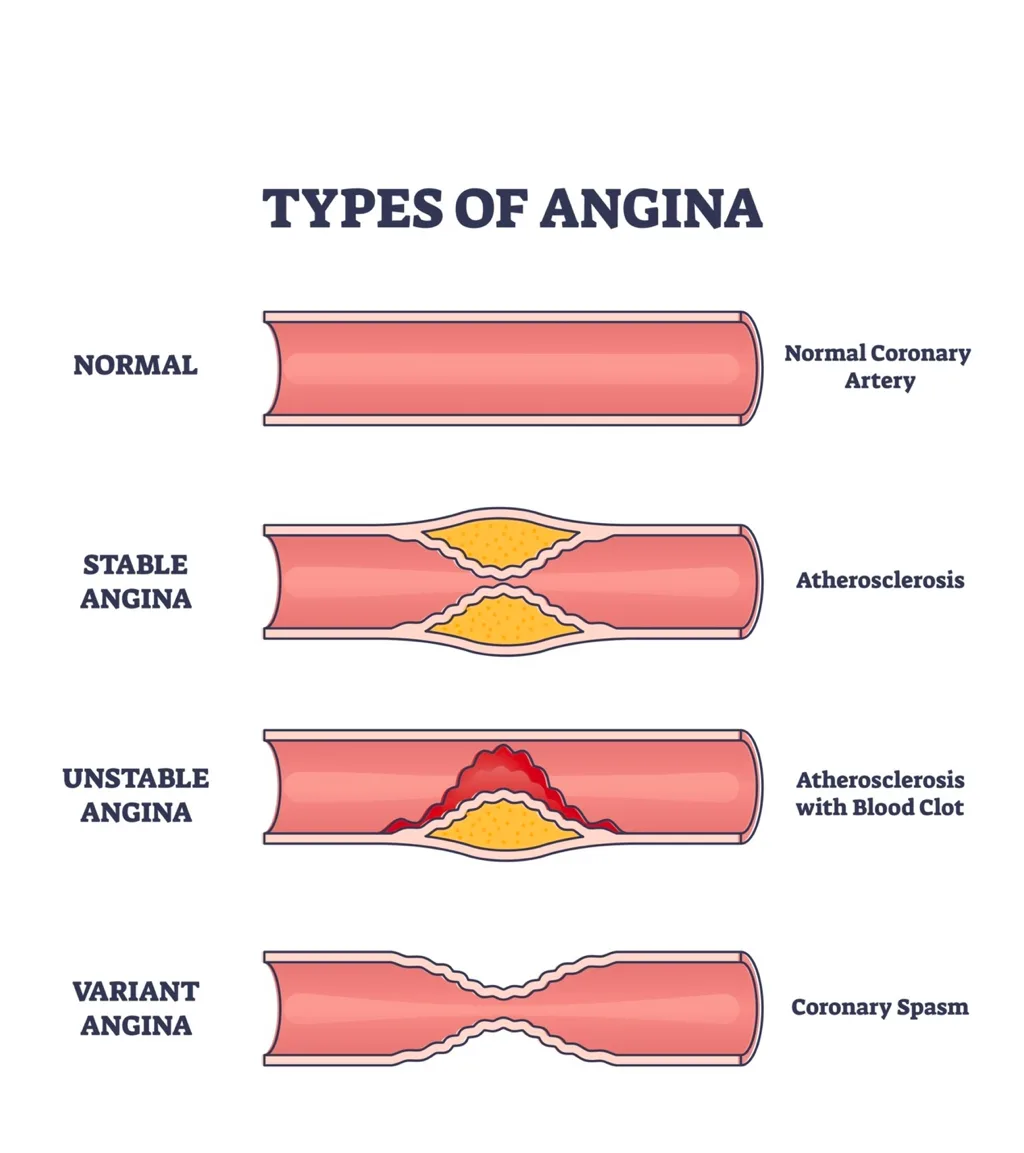
Pathology - Unstable angina
Definition: Severe acute myocardial ischemia without myocardial necrosis.
Epidemiology
• Extremely prevalent.
Aetiology
• Primarily attributable to coronary artery atherosclerosis.
Pathogenesis
• The erosion of the surface of an unstable atherosclerotic plaque prompts platelet aggregation on the plaque. • Platelet fragments may potentially dislodge and embolize downstream in the artery. The decrease in coronary blood flow results in acute ischemia of the afflicted myocardium, but does not lead to myocardial necrosis.
Presentation
• Acute coronary syndrome characterized by the abrupt onset of extended ischemic cardiac chest discomfort at rest or with modest exertion. • The electrocardiogram (ECG) reveals ischemia alterations, but lacks ST-elevation. Biochemistry • Blood troponin concentrations remain unchanged.
Macroscopy
• Significant narrowing of the affected coronary artery due to a complex atherosclerotic plaque. • No observable gross alterations in the myocardial. Histopathology • Absence of distinctive light microscopic characteristics in the myocardium.
Definition: Severe acute myocardial ischemia without myocardial necrosis.
Epidemiology
• Extremely prevalent.
Aetiology
• Primarily attributable to coronary artery atherosclerosis.
Pathogenesis
• The erosion of the surface of an unstable atherosclerotic plaque prompts platelet aggregation on the plaque. • Platelet fragments may potentially dislodge and embolize downstream in the artery. The decrease in coronary blood flow results in acute ischemia of the afflicted myocardium, but does not lead to myocardial necrosis.
Presentation
• Acute coronary syndrome characterized by the abrupt onset of extended ischemic cardiac chest discomfort at rest or with modest exertion. • The electrocardiogram (ECG) reveals ischemia alterations, but lacks ST-elevation. Biochemistry • Blood troponin concentrations remain unchanged.
Macroscopy
• Significant narrowing of the affected coronary artery due to a complex atherosclerotic plaque. • No observable gross alterations in the myocardial. Histopathology • Absence of distinctive light microscopic characteristics in the myocardium.
- Published on
Pathology -Angina pectoris
Definition: Recurrent transient bouts of thoracic discomfort resulting from myocardial ischemia.
Epidemiology • Highly prevalent.
Aetiology
• Almost often induced by coronary artery atherosclerosis.
• Principal risk factors include tobacco use, hypertension, diabetes, and hyperlipidemia. • Hypertension and aortic stenosis may also exacerbate the condition by inducing left ventricular hypertrophy and elevating myocardial oxygen demand.
Pathogenesis
Myocardial ischaemia arises when the demand for oxygen by the myocardium exceeds its supply. A substantial fixed stenosis of a coronary artery hinders coronary blood flow as myocardial oxygen demand escalates, such as during physical exertion.
Presentation
• Central chest discomfort frequently characterized as pressure, heaviness, tightness, or a squeezing sensation. • The discomfort frequently extends from the neck to the jaw and over the shoulders and upper arms. • It may be accompanied by nausea and diaphoresis. • Angina episodes are usually triggered by physical exertion or mental stress, persist for several minutes, and resolve with rest or medicine.
Macroscopy • Notable narrowing of a coronary artery due to atherosclerosis. • No significant alterations observed in the myocardium. Histopathology No distinct light microscopic characteristics in the myocardium.
Prognosis: Atherosclerosis is frequently widespread, placing patients at risk for various forms of ischemic heart disease (acute myocardial infarction, left ventricular failure), as well as abdominal aortic aneurysm, peripheral vascular disease, and stroke.
Definition: Recurrent transient bouts of thoracic discomfort resulting from myocardial ischemia.
Epidemiology • Highly prevalent.
Aetiology
• Almost often induced by coronary artery atherosclerosis.
• Principal risk factors include tobacco use, hypertension, diabetes, and hyperlipidemia. • Hypertension and aortic stenosis may also exacerbate the condition by inducing left ventricular hypertrophy and elevating myocardial oxygen demand.
Pathogenesis
Myocardial ischaemia arises when the demand for oxygen by the myocardium exceeds its supply. A substantial fixed stenosis of a coronary artery hinders coronary blood flow as myocardial oxygen demand escalates, such as during physical exertion.
Presentation
• Central chest discomfort frequently characterized as pressure, heaviness, tightness, or a squeezing sensation. • The discomfort frequently extends from the neck to the jaw and over the shoulders and upper arms. • It may be accompanied by nausea and diaphoresis. • Angina episodes are usually triggered by physical exertion or mental stress, persist for several minutes, and resolve with rest or medicine.
Macroscopy • Notable narrowing of a coronary artery due to atherosclerosis. • No significant alterations observed in the myocardium. Histopathology No distinct light microscopic characteristics in the myocardium.
Prognosis: Atherosclerosis is frequently widespread, placing patients at risk for various forms of ischemic heart disease (acute myocardial infarction, left ventricular failure), as well as abdominal aortic aneurysm, peripheral vascular disease, and stroke.
- Published on
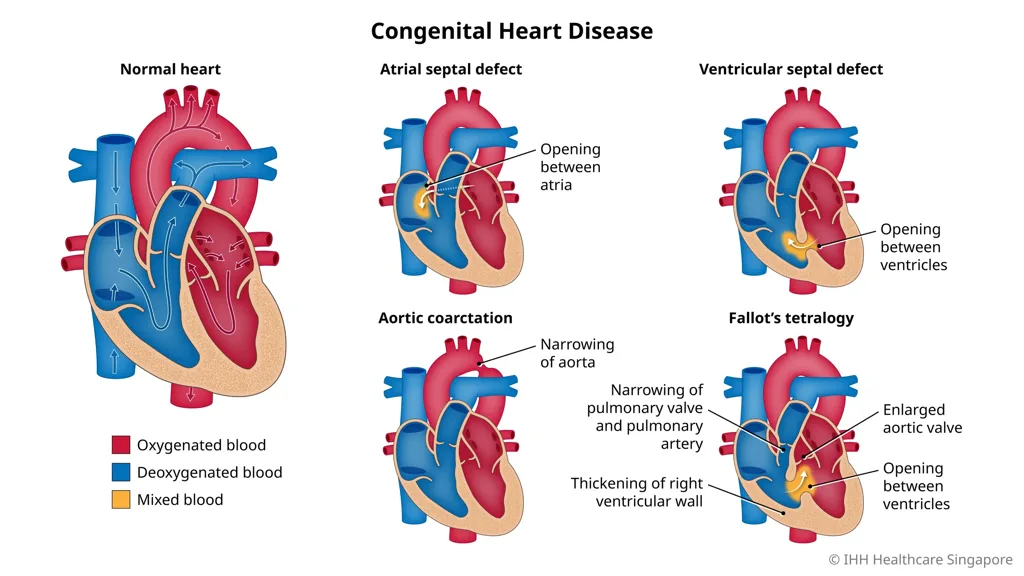
Pathology - Congenital Heart Disease
Ventricular septal defect
• The predominant form of congenital heart disease (CHD). • An atypical perforation in the interventricular septum. • May manifest anywhere inside the septum, albeit the majority are located in the superior region. A minor ventricular septal defect (VSD) may possess minimal functional significance and may close spontaneously as the infant matures. Nonetheless, there persists a risk of infective endocarditis. A significant VSD results in a left-to-right shunt, leading to augmented volume overload on the right ventricle, accompanied with manifestations of heart failure.
Patent ductus arteriosus
• Continuation of the ductus arteriosus beyond 10 days of life. • Systemic blood flows from the aorta to the pulmonary artery, resulting in a left-to-right shunt. Blood flow to the lungs is augmented twofold, as is the amount returning to the left side of the heart, resulting in left ventricular hypertrophy. • Infective endocarditis is a common complication.
Atrial septal defect
• An atypical orifice in the atrial septum. The most prevalent location is the central region of the septum, distant from the atrioventricular valves. • Blood circulates from the left atrium to the right atrium, resulting in enhanced pulmonary circulation. • May be asymptomatic or lead to increased fatigue during childhood. • Many individuals appear in maturity due to atrial arrhythmias.
Atrioventricular septal defect
• A defect at the intersection of the atrial and ventricular septa. • In a complete atrioventricular septal defect (AVSD), there exists a combination of a low atrial septal defect (ASD) and a high ventricular septal defect (VSD), effectively creating a central orifice in the heart. • Most function similarly to a VSD, resulting in volume overload to the right ventricle. • The most prevalent form of congenital heart disease (CHD) observed in children with Down syndrome.
Tetralogy of Fallot
• Includes pulmonary stenosis, ventricular septal defect (VSD), overriding aorta, and right ventricular hypertrophy. • Pulmonary stenosis induces a right-to-left shunt and diminishes pulmonary blood flow, leading to cyanosis. Transposition of the major arteries • Misplacement of the aorta to the right ventricle and the pulmonary artery to the left ventricle. • Typically accompanied with a defect that facilitates the mixing of blood from both circulations (e.g., ventricular septal defect [VSD] or patent ductus arteriosus [PDA]), otherwise the anomaly is incompatible with survival.
Coarctation of the aorta
• A localized constriction of the aortic arch lumen distal to the left subclavian artery's origin. • In the infantile variant, a patent ductus arteriosus distal to the coarctation facilitates cardiac output to the lower body; however, this predominantly consists of deoxygenated blood from the right heart, resulting in cyanosis of the lower body.
• In the adult variant, a patent ductus arteriosus is absent.
Enhanced blood flow to the upper body results in the majority of individuals experiencing upper extremity hypertension. This kind is frequently unacknowledged until adulthood. Bicuspid aortic valves typically function adequately at birth and sometimes remain undiagnosed. Most bicuspid valves ultimately progress to calcific aortic stenosis, occurring at an earlier age than the usual senile aortic stenosis, or aortic regurgitation. • Elevated risk of aortic dissection in adulthood
Ventricular septal defect
• The predominant form of congenital heart disease (CHD). • An atypical perforation in the interventricular septum. • May manifest anywhere inside the septum, albeit the majority are located in the superior region. A minor ventricular septal defect (VSD) may possess minimal functional significance and may close spontaneously as the infant matures. Nonetheless, there persists a risk of infective endocarditis. A significant VSD results in a left-to-right shunt, leading to augmented volume overload on the right ventricle, accompanied with manifestations of heart failure.
Patent ductus arteriosus
• Continuation of the ductus arteriosus beyond 10 days of life. • Systemic blood flows from the aorta to the pulmonary artery, resulting in a left-to-right shunt. Blood flow to the lungs is augmented twofold, as is the amount returning to the left side of the heart, resulting in left ventricular hypertrophy. • Infective endocarditis is a common complication.
Atrial septal defect
• An atypical orifice in the atrial septum. The most prevalent location is the central region of the septum, distant from the atrioventricular valves. • Blood circulates from the left atrium to the right atrium, resulting in enhanced pulmonary circulation. • May be asymptomatic or lead to increased fatigue during childhood. • Many individuals appear in maturity due to atrial arrhythmias.
Atrioventricular septal defect
• A defect at the intersection of the atrial and ventricular septa. • In a complete atrioventricular septal defect (AVSD), there exists a combination of a low atrial septal defect (ASD) and a high ventricular septal defect (VSD), effectively creating a central orifice in the heart. • Most function similarly to a VSD, resulting in volume overload to the right ventricle. • The most prevalent form of congenital heart disease (CHD) observed in children with Down syndrome.
Tetralogy of Fallot
• Includes pulmonary stenosis, ventricular septal defect (VSD), overriding aorta, and right ventricular hypertrophy. • Pulmonary stenosis induces a right-to-left shunt and diminishes pulmonary blood flow, leading to cyanosis. Transposition of the major arteries • Misplacement of the aorta to the right ventricle and the pulmonary artery to the left ventricle. • Typically accompanied with a defect that facilitates the mixing of blood from both circulations (e.g., ventricular septal defect [VSD] or patent ductus arteriosus [PDA]), otherwise the anomaly is incompatible with survival.
Coarctation of the aorta
• A localized constriction of the aortic arch lumen distal to the left subclavian artery's origin. • In the infantile variant, a patent ductus arteriosus distal to the coarctation facilitates cardiac output to the lower body; however, this predominantly consists of deoxygenated blood from the right heart, resulting in cyanosis of the lower body.
• In the adult variant, a patent ductus arteriosus is absent.
Enhanced blood flow to the upper body results in the majority of individuals experiencing upper extremity hypertension. This kind is frequently unacknowledged until adulthood. Bicuspid aortic valves typically function adequately at birth and sometimes remain undiagnosed. Most bicuspid valves ultimately progress to calcific aortic stenosis, occurring at an earlier age than the usual senile aortic stenosis, or aortic regurgitation. • Elevated risk of aortic dissection in adulthood
- Published on
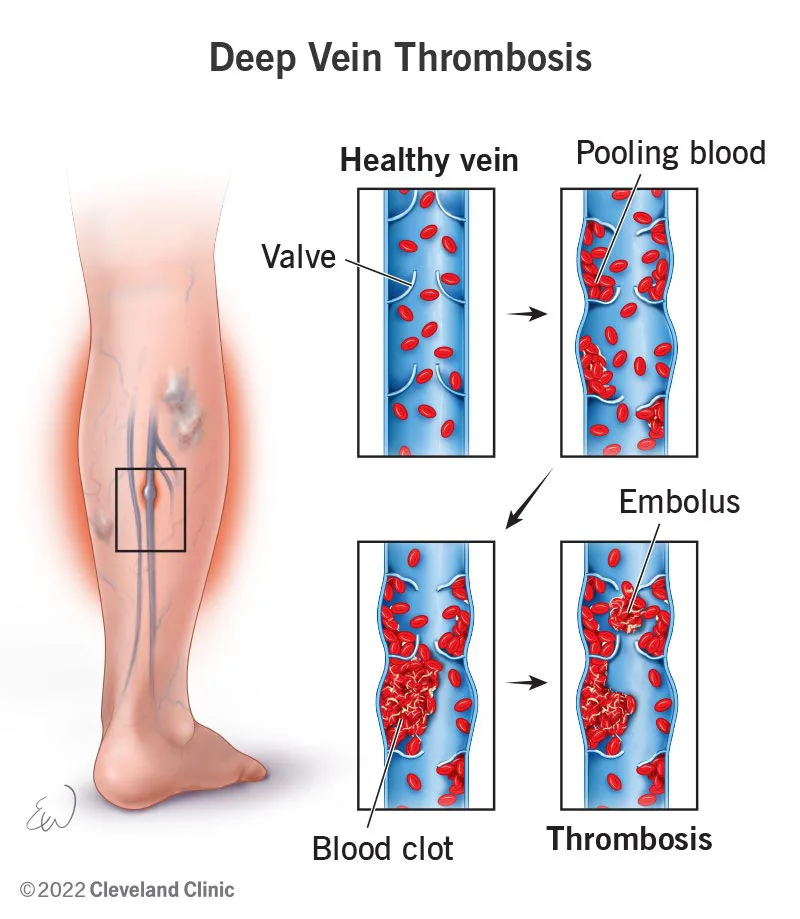
Pathology - Deep vein thrombosis
Definition
• Thrombosis occurring in the deep veins of the leg. Epidemiology: Approximately 1 in 1000 individuals annually.
Aetiology • Pertaining to blood stasis and/or heightened blood coagulability. • Risk factors encompass immobilization, pregnancy, recent surgery (especially to the lower limb or pelvic), cancer, long-haul flights, smoking, oral contraceptive use, hormone replacement therapy, and thrombophilia. 2 Various contributing components frequently function within an individual.
Pathogenesis
• Impaired blood flow and/or heightened blood coagulability surpasses the efficacy of natural anticoagulants, resulting in thrombus formation within the deep veins of the leg. • The thrombus may develop in size as it extends along the vein's lumen.
Presentation: • Inflamed, painful, and swollen lower limb with a warm red hue. • Certain cases may be asymptomatic.
Complications
Three Pulmonary thromboembolism
Definition
• Thrombosis occurring in the deep veins of the leg. Epidemiology: Approximately 1 in 1000 individuals annually.
Aetiology • Pertaining to blood stasis and/or heightened blood coagulability. • Risk factors encompass immobilization, pregnancy, recent surgery (especially to the lower limb or pelvic), cancer, long-haul flights, smoking, oral contraceptive use, hormone replacement therapy, and thrombophilia. 2 Various contributing components frequently function within an individual.
Pathogenesis
• Impaired blood flow and/or heightened blood coagulability surpasses the efficacy of natural anticoagulants, resulting in thrombus formation within the deep veins of the leg. • The thrombus may develop in size as it extends along the vein's lumen.
Presentation: • Inflamed, painful, and swollen lower limb with a warm red hue. • Certain cases may be asymptomatic.
Complications
Three Pulmonary thromboembolism
- Published on
Pathology – Varicose Veins
Definition: Tortuous and dilated superficial leg veins resulting from valvular incompetence.
Epidemiology
• Impact as much as 20% of the population. • Significant female predominance (5:4 ratio 9:1). Aetiology • The majority of cases are primary and idiopathic. • Secondary causes including pregnancy, substantial fibroids, and ovarian masses.
Mechanism of Disease Development
• Believed that valve cusps undergo degeneration and form perforations. • Valve incompetence elevates stress on the downstream valve. • Ultimately, a column of valves becomes inadequate, resulting in venous dilation.
Presentation
• The majority of patients present because of the unattractive appearance of the veins. • Discomfort, hurting, itching, and swelling may be present. • Symptoms may intensify towards the day's conclusion.
Complications
• Stasis dermatitis (varicose). • Varicose ulceration. • Lipodermatosclerosis. • Hemorrhaging. • Thrombosis (superficial thrombophlebitis)
Definition: Tortuous and dilated superficial leg veins resulting from valvular incompetence.
Epidemiology
• Impact as much as 20% of the population. • Significant female predominance (5:4 ratio 9:1). Aetiology • The majority of cases are primary and idiopathic. • Secondary causes including pregnancy, substantial fibroids, and ovarian masses.
Mechanism of Disease Development
• Believed that valve cusps undergo degeneration and form perforations. • Valve incompetence elevates stress on the downstream valve. • Ultimately, a column of valves becomes inadequate, resulting in venous dilation.
Presentation
• The majority of patients present because of the unattractive appearance of the veins. • Discomfort, hurting, itching, and swelling may be present. • Symptoms may intensify towards the day's conclusion.
Complications
• Stasis dermatitis (varicose). • Varicose ulceration. • Lipodermatosclerosis. • Hemorrhaging. • Thrombosis (superficial thrombophlebitis)

