- Published on
Pathology - Abdominal aortic aneurysm
Definition
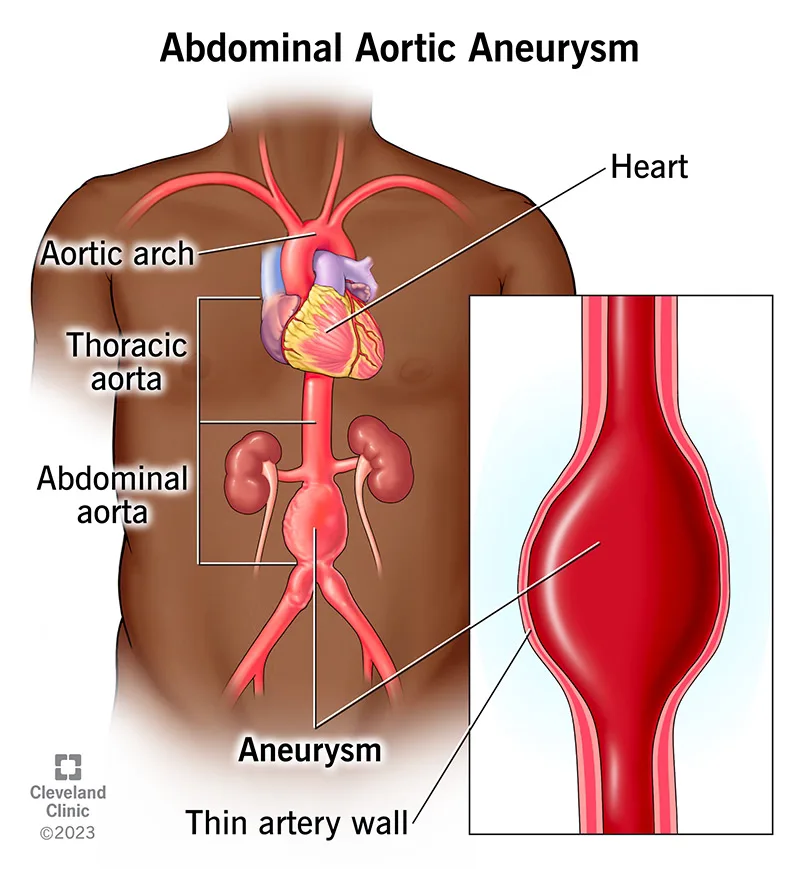
A permanent dilatation of the abdominal aorta exceeding 3 cm in diameter.
Epidemiology
The incidence is stated to be 5–10%.
Aetiology
Nearly all are attributable to aortic atherosclerosis.
Mechanism of disease development
Proteolytic enzymes compromise the aortic medium, resulting in aneurysmal alterations. Elevated concentrations of matrix metalloproteinases have been identified in aneurysmal aortas. These enzymes are recognized for their ability to breakdown elastin.
Pathology
Unruptured aneurysms are frequently asymptomatic; nonetheless, they may induce abdomen or back pain. Most are identified inadvertently during abdominal examination or imaging. Ruptured abdominal aortic aneurysms manifest as a surgical emergency characterized by abdominal discomfort and shock.
Macroscopy
The aorta exhibits dilation, typically occurring behind the renal arteries. Extensive atherosclerosis is consistently observed, frequently accompanied by secondary thrombosis and calcification.
Prognosis: The natural progression is characterized by gradual expansion. The risk of rupture is exponentially correlated with diameter. • Mortality following rupture surpasses 80%. Elective surgical intervention is recommended for aneurysms with a maximal diameter of 5.5 cm or greater.
Definition
A permanent dilatation of the abdominal aorta exceeding 3 cm in diameter.
Epidemiology
The incidence is stated to be 5–10%.
Aetiology
Nearly all are attributable to aortic atherosclerosis.
Mechanism of disease development
Proteolytic enzymes compromise the aortic medium, resulting in aneurysmal alterations. Elevated concentrations of matrix metalloproteinases have been identified in aneurysmal aortas. These enzymes are recognized for their ability to breakdown elastin.
Pathology
Unruptured aneurysms are frequently asymptomatic; nonetheless, they may induce abdomen or back pain. Most are identified inadvertently during abdominal examination or imaging. Ruptured abdominal aortic aneurysms manifest as a surgical emergency characterized by abdominal discomfort and shock.
Macroscopy
The aorta exhibits dilation, typically occurring behind the renal arteries. Extensive atherosclerosis is consistently observed, frequently accompanied by secondary thrombosis and calcification.
Prognosis: The natural progression is characterized by gradual expansion. The risk of rupture is exponentially correlated with diameter. • Mortality following rupture surpasses 80%. Elective surgical intervention is recommended for aneurysms with a maximal diameter of 5.5 cm or greater.
- Published on
Pathology - Aortic dissection
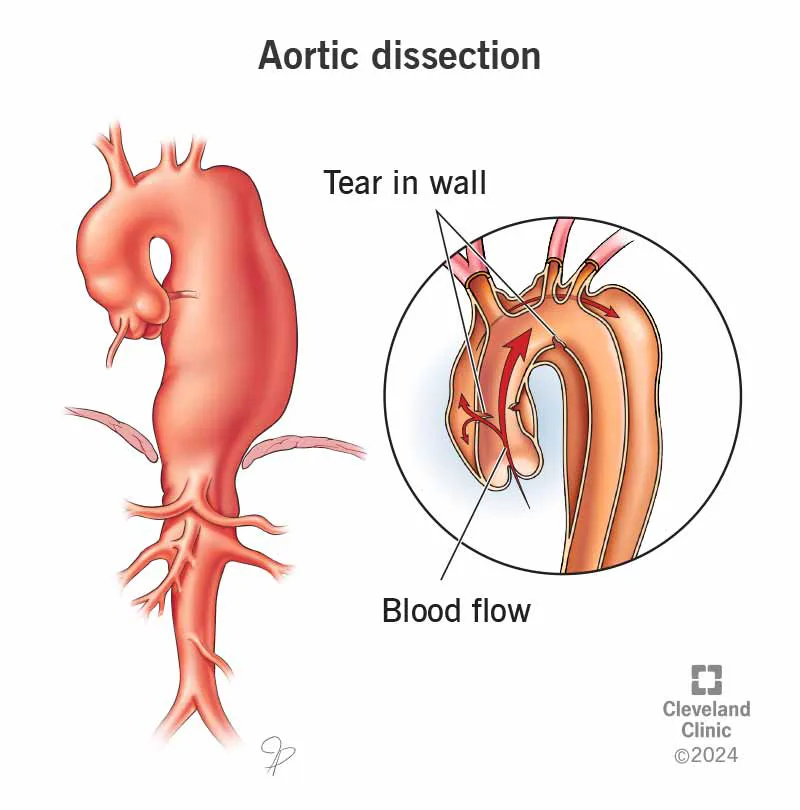
Definition: A rupture in the aortic wall allowing blood to flow through.
Epidemiology
• The majority of instances arise in persons aged 50 to 70 years. The 4:5 ratio equates to 2:1.
Aetiology
• The majority of instances are associated with hypertension. • Additional correlations include Marfan syndrome and congenital bicuspid aortic valve. The pathogenesis of aortic dissection in relation to hypertension remains contentious. • Suggested that the initial event is hemorrhage from a vasa vasorum into the media of the aorta. The intima experiences stress and ruptures, permitting blood to infiltrate the media and dissect along it. • Dissections may advance in the direction of the normal aortic blood flow (anterograde) or against it towards the aortic root (retrograde). • Dissections may re-enter the aortic lumen at a remote location, resulting in a 'double-barrelled' aorta, or may burst externally into the pericardial, pleural, or peritoneal cavities. Approximately 75% pertain to the ascending aorta or aortic arch (type A). Approximately 25% pertain to the descending aorta, without involvement of the ascending aorta or aortic arch (type B).
Presentation
• Intense, acute 'tearing' chest pain that may closely resemble acute myocardial infarction. • External rupture results in significant internal hemorrhage and shock.
Macroscopy
A rip is typically observable in the intima of the aorta at both the initiation and termination points of the dissection. • Should the dissection rupture externally, substantial volumes of blood clot will be present around the rupture site.
Histopathology
Microscopy offers limited insight into the reasons for dissection.
• The existence of significant degenerative alterations in the aorta wall of people under 60 years old suggests the potential for an inherited aortopathy, such as Marfan syndrome. Prognosis: Untreated cases have a significant death rate, with 50% succumbing within the first week.
• Treated cases exhibit favorable initial survival; but, they continue to be susceptible to mortality from rupture of the dissection or the emergence of a new dissection.
Definition: A rupture in the aortic wall allowing blood to flow through.
Epidemiology
• The majority of instances arise in persons aged 50 to 70 years. The 4:5 ratio equates to 2:1.
Aetiology
• The majority of instances are associated with hypertension. • Additional correlations include Marfan syndrome and congenital bicuspid aortic valve. The pathogenesis of aortic dissection in relation to hypertension remains contentious. • Suggested that the initial event is hemorrhage from a vasa vasorum into the media of the aorta. The intima experiences stress and ruptures, permitting blood to infiltrate the media and dissect along it. • Dissections may advance in the direction of the normal aortic blood flow (anterograde) or against it towards the aortic root (retrograde). • Dissections may re-enter the aortic lumen at a remote location, resulting in a 'double-barrelled' aorta, or may burst externally into the pericardial, pleural, or peritoneal cavities. Approximately 75% pertain to the ascending aorta or aortic arch (type A). Approximately 25% pertain to the descending aorta, without involvement of the ascending aorta or aortic arch (type B).
Presentation
• Intense, acute 'tearing' chest pain that may closely resemble acute myocardial infarction. • External rupture results in significant internal hemorrhage and shock.
Macroscopy
A rip is typically observable in the intima of the aorta at both the initiation and termination points of the dissection. • Should the dissection rupture externally, substantial volumes of blood clot will be present around the rupture site.
Histopathology
Microscopy offers limited insight into the reasons for dissection.
• The existence of significant degenerative alterations in the aorta wall of people under 60 years old suggests the potential for an inherited aortopathy, such as Marfan syndrome. Prognosis: Untreated cases have a significant death rate, with 50% succumbing within the first week.
• Treated cases exhibit favorable initial survival; but, they continue to be susceptible to mortality from rupture of the dissection or the emergence of a new dissection.
- Published on
Pathology - Acute lower limb ischemia
Definition
A quick and abrupt interruption of the artery flow to the lower leg.
Epidemiology
• Incidence documented at 14 per 100,000 individuals annually.
Aetiology
• 60% attributable to acute thrombosis in a vessel with pre-existing atherosclerosis. • 30% resulting from a thromboembolus originating from a distant region, typically the heart. Common cardiac connections include atrial fibrillation, acute myocardial infarction, and ventricular aneurysm. Typical locations of impaction include the popliteal artery, common femoral artery, and aortic bifurcation. Less frequent causes encompass aortic dissection, trauma, and iatrogenic injury. The incidence of iatrogenic injury is increasing due to the rising use of endovascular operations.
Pathogenesis
• Abrupt obstruction of the arterial supply to the leg results in ischaemia.
• In the absence of intervention, irreparable tissue damage transpires within 6 hours. Extensive muscular necrosis results in hyperkalemia, acidosis, abrupt renal failure, and cardiac arrest.
Presentation • Abrupt emergence of pain and sensory loss in the extremity. • Upon examination, the limb exhibits pallor and coolness, accompanied by diminished or absent pulses. Prognosis: Limb loss occurs in 40% of cases. • Mortality in 20% of cases
Definition
A quick and abrupt interruption of the artery flow to the lower leg.
Epidemiology
• Incidence documented at 14 per 100,000 individuals annually.
Aetiology
• 60% attributable to acute thrombosis in a vessel with pre-existing atherosclerosis. • 30% resulting from a thromboembolus originating from a distant region, typically the heart. Common cardiac connections include atrial fibrillation, acute myocardial infarction, and ventricular aneurysm. Typical locations of impaction include the popliteal artery, common femoral artery, and aortic bifurcation. Less frequent causes encompass aortic dissection, trauma, and iatrogenic injury. The incidence of iatrogenic injury is increasing due to the rising use of endovascular operations.
Pathogenesis
• Abrupt obstruction of the arterial supply to the leg results in ischaemia.
• In the absence of intervention, irreparable tissue damage transpires within 6 hours. Extensive muscular necrosis results in hyperkalemia, acidosis, abrupt renal failure, and cardiac arrest.
Presentation • Abrupt emergence of pain and sensory loss in the extremity. • Upon examination, the limb exhibits pallor and coolness, accompanied by diminished or absent pulses. Prognosis: Limb loss occurs in 40% of cases. • Mortality in 20% of cases

- Published on
Pathology - Chronic lower limb ischemia
Definition: Persistent impairment of arterial circulation to the lower extremities.
Epidemiology:
Prevalent
. • Impacts 7% of men over the age of 50. The 4:5 ratio equates to 2:1.
Aetiology
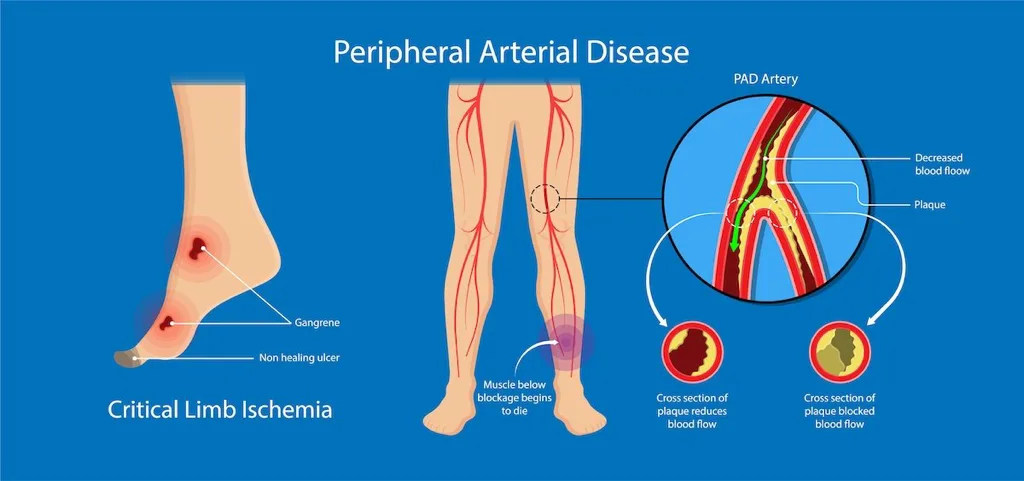
• The majority of cases are attributable to atherosclerosis impacting the aorto-iliac, femoral, or popliteal and calf arteries, either individually or collectively.
Pathogenesis
• Unifocal illness typically leads to intermittent claudication. • A two-level illness typically leads to critical limb ischemia.
Presentation
• Intermittent claudication is defined by pain in the calf or thigh induced by physical activity and alleviated by rest. Critical limb ischaemia is defined by rest pain, tissue necrosis (gangrene or ulceration), or a Doppler ankle pressure of less than 50 mmHg.
Prognosis: One-third experiences improvement, one-third maintains stability, and one-third experiences deterioration. • 4% necessitate intervention, and 1% culminate in amputation
Definition: Persistent impairment of arterial circulation to the lower extremities.
Epidemiology:
Prevalent
. • Impacts 7% of men over the age of 50. The 4:5 ratio equates to 2:1.
Aetiology
• The majority of cases are attributable to atherosclerosis impacting the aorto-iliac, femoral, or popliteal and calf arteries, either individually or collectively.
Pathogenesis
• Unifocal illness typically leads to intermittent claudication. • A two-level illness typically leads to critical limb ischemia.
Presentation
• Intermittent claudication is defined by pain in the calf or thigh induced by physical activity and alleviated by rest. Critical limb ischaemia is defined by rest pain, tissue necrosis (gangrene or ulceration), or a Doppler ankle pressure of less than 50 mmHg.
Prognosis: One-third experiences improvement, one-third maintains stability, and one-third experiences deterioration. • 4% necessitate intervention, and 1% culminate in amputation
- Published on
Pathology - Hypertension
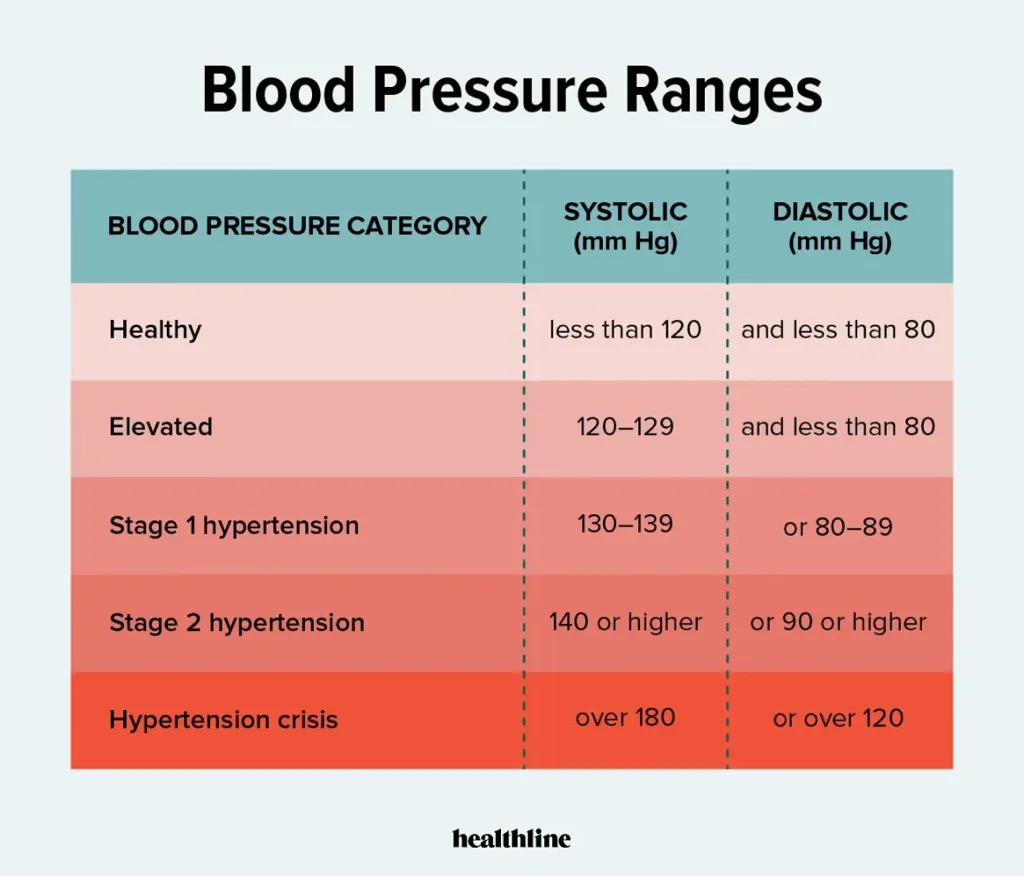
Definition • Consistently raised blood pressure at a threshold where the advantages of therapy are unequivocal for the individual.
All patients with blood pressure equal to or over 160/100 mmHg should receive treatment. The decision to manage blood pressure at 140/90 mmHg is contingent upon additional risk factors.
Epidemiology:
Highly prevalent.
• Significant geographical and racial heterogeneity. • The incidence is estimated to be as high as 25–30% in Western nations.
Aetiology
• Ninety-five percent are of indeterminate origin ('important'). Five percent of instances are attributed to chronic kidney illness, phaeochromocytoma, adrenal cortical adenoma,coarctation of the aorta, pregnancy, and the oral contraceptive pill.
Pathogenesis
• Highly intricate, involving numerous factors such as sodium consumption and genetic predisposition, which seem to interact to induce hypertension.
• Chronic hypertension facilitates atherosclerosis in medium and large systemic arteries and induces thickening of minor arteries (arteriosclerosis) and arterioles (arteriolosclerosis). Hypertension elevates the workload of the left ventricle, resulting in left ventricular hypertrophy and ultimately left ventricular failure.
Presentation
• The majority of patients are asymptomatic and are diagnosed during blood pressure assessment. • Individuals exhibit symptoms indicative of end-organ damage resulting from hypertension, such as intracerebral hemorrhage, left ventricular failure, and chronic renal disease.
Prognosis
• Inadequate treatment of the disease elevates the risk of left ventricular failure, intracerebral hemorrhage, chronic renal disease, and aortic dissection.
Definition • Consistently raised blood pressure at a threshold where the advantages of therapy are unequivocal for the individual.
All patients with blood pressure equal to or over 160/100 mmHg should receive treatment. The decision to manage blood pressure at 140/90 mmHg is contingent upon additional risk factors.
Epidemiology:
Highly prevalent.
• Significant geographical and racial heterogeneity. • The incidence is estimated to be as high as 25–30% in Western nations.
Aetiology
• Ninety-five percent are of indeterminate origin ('important'). Five percent of instances are attributed to chronic kidney illness, phaeochromocytoma, adrenal cortical adenoma,coarctation of the aorta, pregnancy, and the oral contraceptive pill.
Pathogenesis
• Highly intricate, involving numerous factors such as sodium consumption and genetic predisposition, which seem to interact to induce hypertension.
• Chronic hypertension facilitates atherosclerosis in medium and large systemic arteries and induces thickening of minor arteries (arteriosclerosis) and arterioles (arteriolosclerosis). Hypertension elevates the workload of the left ventricle, resulting in left ventricular hypertrophy and ultimately left ventricular failure.
Presentation
• The majority of patients are asymptomatic and are diagnosed during blood pressure assessment. • Individuals exhibit symptoms indicative of end-organ damage resulting from hypertension, such as intracerebral hemorrhage, left ventricular failure, and chronic renal disease.
Prognosis
• Inadequate treatment of the disease elevates the risk of left ventricular failure, intracerebral hemorrhage, chronic renal disease, and aortic dissection.
- Published on
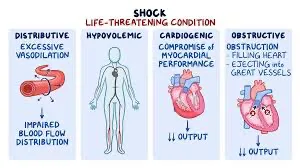
Shock
Defi nition
• A generalized failure of tissue perfusion.
Aetiology
• Pump failure, e.g. acute myocardial infarction.
• Peripheral circulation failure, e.g. hypovolaemia, sepsis, anaphylaxis
, tension pneumothorax,large pulmonary embolus
Pathogenesis
• Pump or peripheral circulation failure leads to cardiovascular collapse.
• Prolonged inadequate tissue perfusion risks the development of
multiple organ failure.
Presentation
• Tachycardia due to increased sympathetic drive.
• Urine output declines (only apparent if the patient is catheterized).
• Hypotension.
2 Note up to 15 % of circulating volume may be lost before any clinical signs
become apparent.
Prognosis
1 Shock is a serious condition which leads to the development of multiple
organ failure if not rapidly addressed
Defi nition
• A generalized failure of tissue perfusion.
Aetiology
• Pump failure, e.g. acute myocardial infarction.
• Peripheral circulation failure, e.g. hypovolaemia, sepsis, anaphylaxis
, tension pneumothorax,large pulmonary embolus
Pathogenesis
• Pump or peripheral circulation failure leads to cardiovascular collapse.
• Prolonged inadequate tissue perfusion risks the development of
multiple organ failure.
Presentation
• Tachycardia due to increased sympathetic drive.
• Urine output declines (only apparent if the patient is catheterized).
• Hypotension.
2 Note up to 15 % of circulating volume may be lost before any clinical signs
become apparent.
Prognosis
1 Shock is a serious condition which leads to the development of multiple
organ failure if not rapidly addressed
- Published on
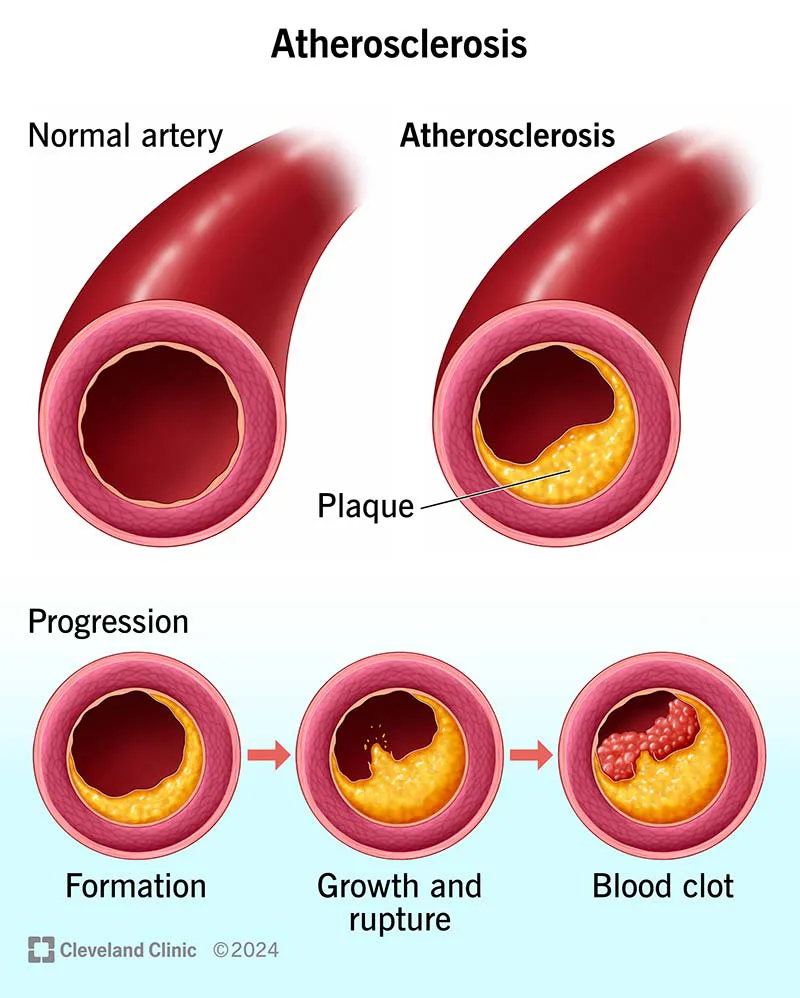
Pathology – Atherosclerosis
Definition
• An inflammatory condition affecting large and medium-sized systemic arteries, marked by the development of lipid-laden plaques within the arterial wall.
Epidemiology: Nearly universally observed to varying extents in all persons as they age.
Aetiology
Risk factors encompass age, male sex, diabetes mellitus, hypertension, tobacco use, and hyperlipidemia. Men who smoke exhibit a 70% elevated mortality rate from ischemic heart disease vs to non-smokers.
Pathogenesis
Endothelial injury induces an inflammatory and fibroproliferative response in the artery, resulting in atherosclerosis, as posited by the 'response to injury' hypothesis. • The endothelium can be compromised by various causes, including as smoking, hyperglycemia, and oxidized LDL. • Oxidized LDL is especially effective in promoting atherosclerosis due to its pro-inflammatory and pro-coagulant properties. Stable plaques characterized by a minimal presence of inflammatory cells and a robust fibrous cap constrict the arterial lumen, yet are less prone to precipitating acute problems. • Unstable plaques characterized by a higher concentration of inflammatory cells possess a thin fibrous cap susceptible to erosion, fissuring, or rupture. The exposure of the highly thrombogenic lipid core to the bloodstream induces an abrupt ischemic event in the organ supplied by the affected artery
Presentation
• Stable plaques induce signs of reversible ischemia in the affected organ, such as angina pectoris and chronic lower limb ischemia. • Unstable plaques precipitate acute ischemic events, including acute coronary syndromes, stroke, and acute lower limb ischemia.
Macroscopy
Atherosclerotic plaques are yellow, lipid-rich lesions located within the walls of big and medium-sized arteries. • Superimposed thrombus has a dark brown coloration. • Predilection sites include the coronary arteries, abdominal aorta, iliac arteries, and bifurcations of the carotid artery. Histopathology • The intima is enlarged by a plaque consisting of a lipid-dense core with an overlay of fibrous tissue. • In cases of superimposed thrombosis, a fibrin-rich clot may also be present, obstructing the artery.
Definition
• An inflammatory condition affecting large and medium-sized systemic arteries, marked by the development of lipid-laden plaques within the arterial wall.
Epidemiology: Nearly universally observed to varying extents in all persons as they age.
Aetiology
Risk factors encompass age, male sex, diabetes mellitus, hypertension, tobacco use, and hyperlipidemia. Men who smoke exhibit a 70% elevated mortality rate from ischemic heart disease vs to non-smokers.
Pathogenesis
Endothelial injury induces an inflammatory and fibroproliferative response in the artery, resulting in atherosclerosis, as posited by the 'response to injury' hypothesis. • The endothelium can be compromised by various causes, including as smoking, hyperglycemia, and oxidized LDL. • Oxidized LDL is especially effective in promoting atherosclerosis due to its pro-inflammatory and pro-coagulant properties. Stable plaques characterized by a minimal presence of inflammatory cells and a robust fibrous cap constrict the arterial lumen, yet are less prone to precipitating acute problems. • Unstable plaques characterized by a higher concentration of inflammatory cells possess a thin fibrous cap susceptible to erosion, fissuring, or rupture. The exposure of the highly thrombogenic lipid core to the bloodstream induces an abrupt ischemic event in the organ supplied by the affected artery
Presentation
• Stable plaques induce signs of reversible ischemia in the affected organ, such as angina pectoris and chronic lower limb ischemia. • Unstable plaques precipitate acute ischemic events, including acute coronary syndromes, stroke, and acute lower limb ischemia.
Macroscopy
Atherosclerotic plaques are yellow, lipid-rich lesions located within the walls of big and medium-sized arteries. • Superimposed thrombus has a dark brown coloration. • Predilection sites include the coronary arteries, abdominal aorta, iliac arteries, and bifurcations of the carotid artery. Histopathology • The intima is enlarged by a plaque consisting of a lipid-dense core with an overlay of fibrous tissue. • In cases of superimposed thrombosis, a fibrin-rich clot may also be present, obstructing the artery.
- Published on
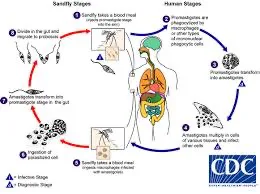
Pathology – Leishmaniasis
Leishmaniasis
pathogen: Leishmania protozoa.
Epidemiology • 1-2 million new cases annually worldwide. • Found in Africa, India, South America, Middle East, and the Mediterranean. Infection can be transmitted through a sandfly bite.
Pathogenesis: • The parasite enters the dermis and is phagocytosed by dermal macrophages. • The ability of each species to live within macrophages and avoid host immunity determines the clinical outcome.
Cutaneous leishmaniasis, caused by Leishmania (L.) tropica and L. Mexicana, typically results in a solitary nodule that ulcerates and heals with scarring.
• L. braziliensis causes mucocutaneous leishmaniasis, which causes skin lesions that can extend to the nose, mouth, and pharynx.
• Visceral leishmaniasis (kala-azar) caused by L. donovani causes fever, anemia, lymphadenopathy, and hepatosplenomegaly. The parasite spreads through macrophages and the reticuloendothelial system.
Diagnosis: Microscopy, culture, FISH, or PCR. Histopathology • Skin biopsies reveal a dense dermal immune infiltrate with lymphocytes, plasma cells, and parasitized macrophages. • The organisms are round to oval, 2-4 micrometers in size, and have an eccentric kinetoplast.
Prognosis: Cutaneous illness often cures spontaneously over months. • Early treatment is crucial for mucocutaneous illness, since mucosal involvement leads to poor outcomes. • Without therapy, visceral illness can lead to liver and bone marrow failure, which is deadly.
Leishmaniasis
pathogen: Leishmania protozoa.
Epidemiology • 1-2 million new cases annually worldwide. • Found in Africa, India, South America, Middle East, and the Mediterranean. Infection can be transmitted through a sandfly bite.
Pathogenesis: • The parasite enters the dermis and is phagocytosed by dermal macrophages. • The ability of each species to live within macrophages and avoid host immunity determines the clinical outcome.
Cutaneous leishmaniasis, caused by Leishmania (L.) tropica and L. Mexicana, typically results in a solitary nodule that ulcerates and heals with scarring.
• L. braziliensis causes mucocutaneous leishmaniasis, which causes skin lesions that can extend to the nose, mouth, and pharynx.
• Visceral leishmaniasis (kala-azar) caused by L. donovani causes fever, anemia, lymphadenopathy, and hepatosplenomegaly. The parasite spreads through macrophages and the reticuloendothelial system.
Diagnosis: Microscopy, culture, FISH, or PCR. Histopathology • Skin biopsies reveal a dense dermal immune infiltrate with lymphocytes, plasma cells, and parasitized macrophages. • The organisms are round to oval, 2-4 micrometers in size, and have an eccentric kinetoplast.
Prognosis: Cutaneous illness often cures spontaneously over months. • Early treatment is crucial for mucocutaneous illness, since mucosal involvement leads to poor outcomes. • Without therapy, visceral illness can lead to liver and bone marrow failure, which is deadly.
- Published on
Pathology – Lyme Disease
Lyme disease
Pathogen: Borrelia burgdorferi, a spirochete.
Epidemiology: Present in the temperate regions of Europe, North America, and Asia.
Transmission:
• An arthropod-borne infection conveyed through ticks of the genus Ixodes.
Pathogenesis
• Borrelia organisms are introduced into the dermis through the tick bite, where they initiate infection and multiply. • Subsequently, days to weeks later, Borrelia disseminates through the bloodstream to remote locations, particularly the joints, heart, and nervous system. Borrelia eludes the immune system by employing antigenic diversity of its surface proteins and by inactivating complement components.
Presentation
• The initial indication is a radially widening erythematous rash at the location of the tick bite, referred to as erythema migrans. Numerous sufferers do not exhibit or remember the rash. Subsequent manifestations encompass arthralgia, myalgia, neuropathies, cognitive alterations, and palpitations.
The existence of nonspecific characteristics across various bodily systems might render diagnosis exceedingly difficult.
Diagnosis: • Western blot, ELISA, or PCR examination of blood or cerebrospinal fluid (CSF). Prognosis: Most individuals identified and treated achieve complete recovery without problems.
Lyme disease
Pathogen: Borrelia burgdorferi, a spirochete.
Epidemiology: Present in the temperate regions of Europe, North America, and Asia.
Transmission:
• An arthropod-borne infection conveyed through ticks of the genus Ixodes.
Pathogenesis
• Borrelia organisms are introduced into the dermis through the tick bite, where they initiate infection and multiply. • Subsequently, days to weeks later, Borrelia disseminates through the bloodstream to remote locations, particularly the joints, heart, and nervous system. Borrelia eludes the immune system by employing antigenic diversity of its surface proteins and by inactivating complement components.
Presentation
• The initial indication is a radially widening erythematous rash at the location of the tick bite, referred to as erythema migrans. Numerous sufferers do not exhibit or remember the rash. Subsequent manifestations encompass arthralgia, myalgia, neuropathies, cognitive alterations, and palpitations.
The existence of nonspecific characteristics across various bodily systems might render diagnosis exceedingly difficult.
Diagnosis: • Western blot, ELISA, or PCR examination of blood or cerebrospinal fluid (CSF). Prognosis: Most individuals identified and treated achieve complete recovery without problems.

- Published on
Pathology - Syphilis
Pathogen
• Treponema pallidum, a helical spirochete.
Epidemiology
• Global prevalence.
• Rising incidence since the 1990s.
Transmission occurs predominantly by sexual contact with an infected individual.
• Can be transmitted from mother to infant, resulting in congenital syphilis.
Pathogenesis
Organisms infiltrate the body through tiny epithelial abrasions.
• The organism generates a non-antigenic mucin coat that promotes rapid dissemination throughout the body via the bloodstream and lymphatic system.
Presentation
• Primary syphilis results in a firm, painless skin ulcer ('chancre') that manifests approximately three weeks post-exposure. The chancre manifests at the site of touch and is typically located in the genital or perianal region. There may be some regional lymphadenopathy.
• Secondary syphilis manifests 1–2 months post-chancre with a rash, malaise, lymphadenopathy, and fever.
Tertiary syphilis manifests years post-exposure with gummas in the skin, mucosa, bone, joints, lungs, and testes.
Gummas are inflammatory lesions resulting from a granulomatous response to the pathogen.
Quaternary syphilis induces ascending aortic aneurysms, cranial nerve palsies, dementia, and tabes dorsalis.
Diagnosis • In primary syphilis, the organisms can be observed through microscopy of the chancre fluid. At this time, serology is frequently negative. In secondary syphilis, the pathogens may be observed in the lesions, and serological tests are typically positive. Organisms are typically absent in the later stages of syphilis, but serological tests generally stay positive.
Prognosis: Antibiotic therapy in the primary or secondary stages is typically curative and mitigates the risk of long-term problems associated with advanced disease.
Pathogen
• Treponema pallidum, a helical spirochete.
Epidemiology
• Global prevalence.
• Rising incidence since the 1990s.
Transmission occurs predominantly by sexual contact with an infected individual.
• Can be transmitted from mother to infant, resulting in congenital syphilis.
Pathogenesis
Organisms infiltrate the body through tiny epithelial abrasions.
• The organism generates a non-antigenic mucin coat that promotes rapid dissemination throughout the body via the bloodstream and lymphatic system.
Presentation
• Primary syphilis results in a firm, painless skin ulcer ('chancre') that manifests approximately three weeks post-exposure. The chancre manifests at the site of touch and is typically located in the genital or perianal region. There may be some regional lymphadenopathy.
• Secondary syphilis manifests 1–2 months post-chancre with a rash, malaise, lymphadenopathy, and fever.
Tertiary syphilis manifests years post-exposure with gummas in the skin, mucosa, bone, joints, lungs, and testes.
Gummas are inflammatory lesions resulting from a granulomatous response to the pathogen.
Quaternary syphilis induces ascending aortic aneurysms, cranial nerve palsies, dementia, and tabes dorsalis.
Diagnosis • In primary syphilis, the organisms can be observed through microscopy of the chancre fluid. At this time, serology is frequently negative. In secondary syphilis, the pathogens may be observed in the lesions, and serological tests are typically positive. Organisms are typically absent in the later stages of syphilis, but serological tests generally stay positive.
Prognosis: Antibiotic therapy in the primary or secondary stages is typically curative and mitigates the risk of long-term problems associated with advanced disease.

