- Published on
Pathology – Leishmaniasis
Leishmaniasis
pathogen: Leishmania protozoa.
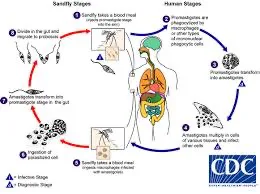
Epidemiology • 1-2 million new cases annually worldwide. • Found in Africa, India, South America, Middle East, and the Mediterranean. Infection can be transmitted through a sandfly bite.
Pathogenesis: • The parasite enters the dermis and is phagocytosed by dermal macrophages. • The ability of each species to live within macrophages and avoid host immunity determines the clinical outcome.
Cutaneous leishmaniasis, caused by Leishmania (L.) tropica and L. Mexicana, typically results in a solitary nodule that ulcerates and heals with scarring.
• L. braziliensis causes mucocutaneous leishmaniasis, which causes skin lesions that can extend to the nose, mouth, and pharynx.
• Visceral leishmaniasis (kala-azar) caused by L. donovani causes fever, anemia, lymphadenopathy, and hepatosplenomegaly. The parasite spreads through macrophages and the reticuloendothelial system.
Diagnosis: Microscopy, culture, FISH, or PCR. Histopathology • Skin biopsies reveal a dense dermal immune infiltrate with lymphocytes, plasma cells, and parasitized macrophages. • The organisms are round to oval, 2-4 micrometers in size, and have an eccentric kinetoplast.
Prognosis: Cutaneous illness often cures spontaneously over months. • Early treatment is crucial for mucocutaneous illness, since mucosal involvement leads to poor outcomes. • Without therapy, visceral illness can lead to liver and bone marrow failure, which is deadly.
Leishmaniasis
pathogen: Leishmania protozoa.
Epidemiology • 1-2 million new cases annually worldwide. • Found in Africa, India, South America, Middle East, and the Mediterranean. Infection can be transmitted through a sandfly bite.
Pathogenesis: • The parasite enters the dermis and is phagocytosed by dermal macrophages. • The ability of each species to live within macrophages and avoid host immunity determines the clinical outcome.
Cutaneous leishmaniasis, caused by Leishmania (L.) tropica and L. Mexicana, typically results in a solitary nodule that ulcerates and heals with scarring.
• L. braziliensis causes mucocutaneous leishmaniasis, which causes skin lesions that can extend to the nose, mouth, and pharynx.
• Visceral leishmaniasis (kala-azar) caused by L. donovani causes fever, anemia, lymphadenopathy, and hepatosplenomegaly. The parasite spreads through macrophages and the reticuloendothelial system.
Diagnosis: Microscopy, culture, FISH, or PCR. Histopathology • Skin biopsies reveal a dense dermal immune infiltrate with lymphocytes, plasma cells, and parasitized macrophages. • The organisms are round to oval, 2-4 micrometers in size, and have an eccentric kinetoplast.
Prognosis: Cutaneous illness often cures spontaneously over months. • Early treatment is crucial for mucocutaneous illness, since mucosal involvement leads to poor outcomes. • Without therapy, visceral illness can lead to liver and bone marrow failure, which is deadly.
- Published on
Pathology – Lyme Disease
Lyme disease
Pathogen: Borrelia burgdorferi, a spirochete.
Epidemiology: Present in the temperate regions of Europe, North America, and Asia.
Transmission:
• An arthropod-borne infection conveyed through ticks of the genus Ixodes.
Pathogenesis
• Borrelia organisms are introduced into the dermis through the tick bite, where they initiate infection and multiply. • Subsequently, days to weeks later, Borrelia disseminates through the bloodstream to remote locations, particularly the joints, heart, and nervous system. Borrelia eludes the immune system by employing antigenic diversity of its surface proteins and by inactivating complement components.
Presentation
• The initial indication is a radially widening erythematous rash at the location of the tick bite, referred to as erythema migrans. Numerous sufferers do not exhibit or remember the rash. Subsequent manifestations encompass arthralgia, myalgia, neuropathies, cognitive alterations, and palpitations.
The existence of nonspecific characteristics across various bodily systems might render diagnosis exceedingly difficult.
Diagnosis: • Western blot, ELISA, or PCR examination of blood or cerebrospinal fluid (CSF). Prognosis: Most individuals identified and treated achieve complete recovery without problems.
Lyme disease
Pathogen: Borrelia burgdorferi, a spirochete.
Epidemiology: Present in the temperate regions of Europe, North America, and Asia.
Transmission:
• An arthropod-borne infection conveyed through ticks of the genus Ixodes.
Pathogenesis
• Borrelia organisms are introduced into the dermis through the tick bite, where they initiate infection and multiply. • Subsequently, days to weeks later, Borrelia disseminates through the bloodstream to remote locations, particularly the joints, heart, and nervous system. Borrelia eludes the immune system by employing antigenic diversity of its surface proteins and by inactivating complement components.
Presentation
• The initial indication is a radially widening erythematous rash at the location of the tick bite, referred to as erythema migrans. Numerous sufferers do not exhibit or remember the rash. Subsequent manifestations encompass arthralgia, myalgia, neuropathies, cognitive alterations, and palpitations.
The existence of nonspecific characteristics across various bodily systems might render diagnosis exceedingly difficult.
Diagnosis: • Western blot, ELISA, or PCR examination of blood or cerebrospinal fluid (CSF). Prognosis: Most individuals identified and treated achieve complete recovery without problems.

- Published on
Pathology - Syphilis
Pathogen
• Treponema pallidum, a helical spirochete.
Epidemiology
• Global prevalence.
• Rising incidence since the 1990s.
Transmission occurs predominantly by sexual contact with an infected individual.
• Can be transmitted from mother to infant, resulting in congenital syphilis.
Pathogenesis
Organisms infiltrate the body through tiny epithelial abrasions.
• The organism generates a non-antigenic mucin coat that promotes rapid dissemination throughout the body via the bloodstream and lymphatic system.
Presentation
• Primary syphilis results in a firm, painless skin ulcer ('chancre') that manifests approximately three weeks post-exposure. The chancre manifests at the site of touch and is typically located in the genital or perianal region. There may be some regional lymphadenopathy.
• Secondary syphilis manifests 1–2 months post-chancre with a rash, malaise, lymphadenopathy, and fever.
Tertiary syphilis manifests years post-exposure with gummas in the skin, mucosa, bone, joints, lungs, and testes.
Gummas are inflammatory lesions resulting from a granulomatous response to the pathogen.
Quaternary syphilis induces ascending aortic aneurysms, cranial nerve palsies, dementia, and tabes dorsalis.
Diagnosis • In primary syphilis, the organisms can be observed through microscopy of the chancre fluid. At this time, serology is frequently negative. In secondary syphilis, the pathogens may be observed in the lesions, and serological tests are typically positive. Organisms are typically absent in the later stages of syphilis, but serological tests generally stay positive.
Prognosis: Antibiotic therapy in the primary or secondary stages is typically curative and mitigates the risk of long-term problems associated with advanced disease.
Pathogen
• Treponema pallidum, a helical spirochete.
Epidemiology
• Global prevalence.
• Rising incidence since the 1990s.
Transmission occurs predominantly by sexual contact with an infected individual.
• Can be transmitted from mother to infant, resulting in congenital syphilis.
Pathogenesis
Organisms infiltrate the body through tiny epithelial abrasions.
• The organism generates a non-antigenic mucin coat that promotes rapid dissemination throughout the body via the bloodstream and lymphatic system.
Presentation
• Primary syphilis results in a firm, painless skin ulcer ('chancre') that manifests approximately three weeks post-exposure. The chancre manifests at the site of touch and is typically located in the genital or perianal region. There may be some regional lymphadenopathy.
• Secondary syphilis manifests 1–2 months post-chancre with a rash, malaise, lymphadenopathy, and fever.
Tertiary syphilis manifests years post-exposure with gummas in the skin, mucosa, bone, joints, lungs, and testes.
Gummas are inflammatory lesions resulting from a granulomatous response to the pathogen.
Quaternary syphilis induces ascending aortic aneurysms, cranial nerve palsies, dementia, and tabes dorsalis.
Diagnosis • In primary syphilis, the organisms can be observed through microscopy of the chancre fluid. At this time, serology is frequently negative. In secondary syphilis, the pathogens may be observed in the lesions, and serological tests are typically positive. Organisms are typically absent in the later stages of syphilis, but serological tests generally stay positive.
Prognosis: Antibiotic therapy in the primary or secondary stages is typically curative and mitigates the risk of long-term problems associated with advanced disease.

- Published on
Pathology – Tuberculosis
Pathogen
• Mycobacterium tuberculosis, an acid-fast bacillus with a rod form. Epidemiology • The most prevalent infectious disease globally. • Causes the demise of 2 million individuals annually.
Transmission
• Respiratory transmission from an infectious individual with active pulmonary tuberculosis (TB).
Immunopathogenesis
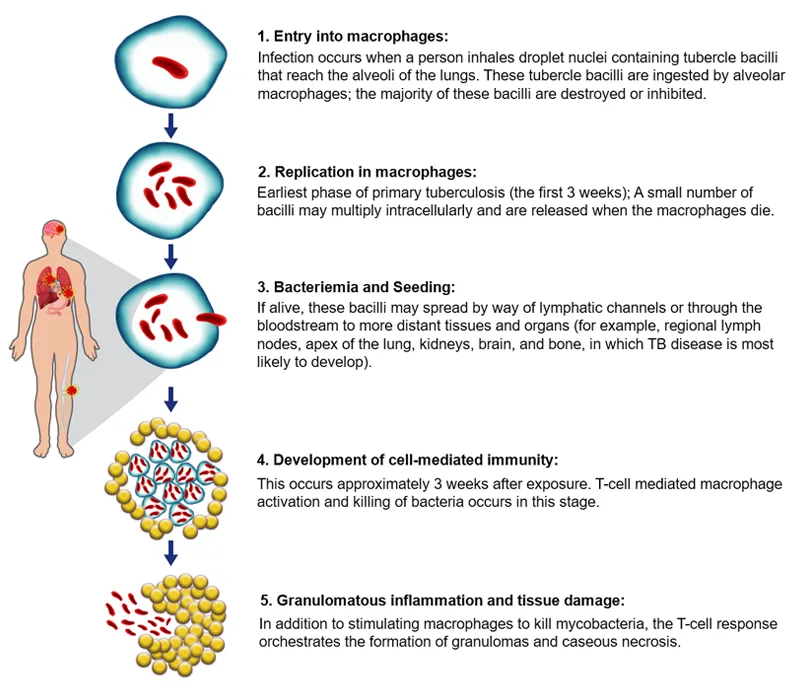
• Inhaled bacilli are phagocytosed by alveolar macrophages, however they can persist and proliferate within these cells. Mycobacteria disseminate within macrophages in the bloodstream to oxygenated regions of the body, including the lung apices, kidneys, bones, and meninges. • Subsequent to many weeks, mycobacteria-specific CD4+ helper T-cells are activated upon MHC class II antigen presentation by macrophages. • Th1 subset helper T-cells generate IFN-γ, which activates macrophages into epithelioid macrophages that aggregate into granulomas, isolating the mycobacteria in an anoxic and acidic milieu.
• The majority of immunocompetent hosts retain the infection, resulting in scarring.
Active disease typically manifests in the elderly, malnourished, diabetic, immunosuppressed, or alcoholic individuals. Active disease may manifest as pulmonary (75%) or extrapulmonary (25%).
Presentation
• Pulmonary tuberculosis manifests as a chronic pneumonia characterized by a persistent cough, fever, night sweats, weight loss, and anorexia.
• Extrapulmonary tuberculosis may appear with meningitis, lymphadenopathy, genitourinary symptoms, or discomfort in bones or joints
.Diagnosis • Acid-fast bacilli may be detected in sputum, pleural fluid, or bronchoalveolar lavage (BAL) fluid. • Culture is the definitive inquiry, although it may require up to 12 weeks for results. Polymerase chain reaction (PCR) is applicable for the diagnosis and identification of drug-resistant strains.
Histopathology
The histopathological characteristic is necrotizing granulomatous inflammation.
Prognosis: • Following antituberculous therapy, the majority of individuals achieve complete recovery. • If left untreated, approximately fifty percent of individuals will ultimately succumb to the virus.
• Prognosis is poorer in the presence of concurrent HIV or organisms exhibiting multidrug resistance.
Pathogen
• Mycobacterium tuberculosis, an acid-fast bacillus with a rod form. Epidemiology • The most prevalent infectious disease globally. • Causes the demise of 2 million individuals annually.
Transmission
• Respiratory transmission from an infectious individual with active pulmonary tuberculosis (TB).
Immunopathogenesis
• Inhaled bacilli are phagocytosed by alveolar macrophages, however they can persist and proliferate within these cells. Mycobacteria disseminate within macrophages in the bloodstream to oxygenated regions of the body, including the lung apices, kidneys, bones, and meninges. • Subsequent to many weeks, mycobacteria-specific CD4+ helper T-cells are activated upon MHC class II antigen presentation by macrophages. • Th1 subset helper T-cells generate IFN-γ, which activates macrophages into epithelioid macrophages that aggregate into granulomas, isolating the mycobacteria in an anoxic and acidic milieu.
• The majority of immunocompetent hosts retain the infection, resulting in scarring.
Active disease typically manifests in the elderly, malnourished, diabetic, immunosuppressed, or alcoholic individuals. Active disease may manifest as pulmonary (75%) or extrapulmonary (25%).
Presentation
• Pulmonary tuberculosis manifests as a chronic pneumonia characterized by a persistent cough, fever, night sweats, weight loss, and anorexia.
• Extrapulmonary tuberculosis may appear with meningitis, lymphadenopathy, genitourinary symptoms, or discomfort in bones or joints
.Diagnosis • Acid-fast bacilli may be detected in sputum, pleural fluid, or bronchoalveolar lavage (BAL) fluid. • Culture is the definitive inquiry, although it may require up to 12 weeks for results. Polymerase chain reaction (PCR) is applicable for the diagnosis and identification of drug-resistant strains.
Histopathology
The histopathological characteristic is necrotizing granulomatous inflammation.
Prognosis: • Following antituberculous therapy, the majority of individuals achieve complete recovery. • If left untreated, approximately fifty percent of individuals will ultimately succumb to the virus.
• Prognosis is poorer in the presence of concurrent HIV or organisms exhibiting multidrug resistance.
- Published on
Pathology – Malaria
Malaria
Pathogen
• Plasmodia protozoa: Plasmodium (P.) falciparum, P. vivax, P. ovale, P. malariae.
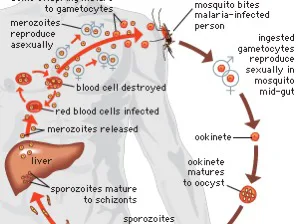
Epidemiology: Endemic in tropical regions of Africa, Asia, and South America. Approximately 10 million new infections annually. Approximately 1 million fatalities annually, predominantly due to P. falciparum. Transmission • Female Anopheles mosquitoes inject Plasmodium sporozoites during a blood meal.
Pathogenesis
• Sporozoites invade hepatocytes and grow into merozoites. • Merozoites infect and replicate within erythrocytes, resulting in hemolytic anemia. Sequestration of red blood cells significantly infected by P. falciparum results in acute renal failure and cerebral malaria.
Presentation
• A non-specific influenza-like disease characterized initially by headache, malaise, and myalgia. • Subsequently, fevers and chills ensue. Cerebral malaria manifests with confusion, seizures, and coma.
Diagnosis: Parasitized erythrocytes may be observed upon inspection of blood smears. Prognosis: Non-falciparum malaria exhibits a minimal death rate. Severe falciparum malaria can be fatal.
Adverse prognostic indicators encompass elevated parasitaemia, hypoglycaemia, disseminated intravascular coagulation (DIC), and renal dysfunction.
Malaria
Pathogen
• Plasmodia protozoa: Plasmodium (P.) falciparum, P. vivax, P. ovale, P. malariae.
Epidemiology: Endemic in tropical regions of Africa, Asia, and South America. Approximately 10 million new infections annually. Approximately 1 million fatalities annually, predominantly due to P. falciparum. Transmission • Female Anopheles mosquitoes inject Plasmodium sporozoites during a blood meal.
Pathogenesis
• Sporozoites invade hepatocytes and grow into merozoites. • Merozoites infect and replicate within erythrocytes, resulting in hemolytic anemia. Sequestration of red blood cells significantly infected by P. falciparum results in acute renal failure and cerebral malaria.
Presentation
• A non-specific influenza-like disease characterized initially by headache, malaise, and myalgia. • Subsequently, fevers and chills ensue. Cerebral malaria manifests with confusion, seizures, and coma.
Diagnosis: Parasitized erythrocytes may be observed upon inspection of blood smears. Prognosis: Non-falciparum malaria exhibits a minimal death rate. Severe falciparum malaria can be fatal.
Adverse prognostic indicators encompass elevated parasitaemia, hypoglycaemia, disseminated intravascular coagulation (DIC), and renal dysfunction.
- Published on
Pathology – Neoplasia
Definitions
A neoplasm is an abnormal tissue mass characterized by unregulated growth and lacking any beneficial function. The term is frequently employed interchangeably with the term tumor, which denotes a swelling.
Benign neoplasms typically have a gradual development rate and remain localized to their site of origin. While benign neoplasms typically follow a harmless trajectory, they may pose risks if they exert pressure on essential adjacent structures or if they emit hormones indiscriminately.
Malignant neoplasms possess the ability to disseminate or metastasis to remote locations, resulting in new tumors known as metastases, which can proliferate independently of the initial tumor.
Cancer is an overarching word for any malignant neoplasm.
Nomenclature of neoplasms
Epithelial neoplasms
Benign neoplasms of squamous epithelium are termed acanthomas when flat and papillomas when exhibiting branching fronds.
Benign neoplasms of glandular epithelium are referred to as adenomas.
Epithelial malignancies are classified as carcinomas.
Carcinomas exhibiting squamous differentiation are termed squamous cell carcinomas. Carcinomas exhibiting glandular differentiation are termed adenocarcinomas. Carcinomas frequently follow a stage of epithelial dysplasia, characterized by the presence of neoplastic cells inside the epithelium, without penetration beyond the epithelial boundaries.
Neoplasms of connective tissue Lipoma is a benign adipose tissue tumor. • Leiomyoma is a benign neoplasm of smooth muscle. • Rhabdomyoma is a benign neoplasm of skeletal muscle. • Angioma is a benign vascular neoplasm. • Osteoma is a benign osseous neoplasm. Liposarcoma is a malignant tumor of adipose tissue. Leiomyosarcoma is a malignant neoplasm of smooth muscle tissue. • Rhabdomyosarcoma is a malignant neoplasm of skeletal muscle. • Angiosarcoma is a malignant neoplasm of vascular tissue. • Osteosarcoma is a malignant neoplasm of bone.
Alternative neoplasm classifications Lymphomas, leukemias, and myeloma are hematological malignancies originating from blood or bone marrow cells.
Malignant melanoma is a tumor of malignant melanocytes. Malignant mesothelioma is a neoplastic mesothelial tumor. Germ cell tumors constitute a heterogeneous category of neoplasms that typically originate in the testes or ovaries. Embryonal tumors are a category of malignant neoplasms primarily observed in children, characterized by highly undifferentiated cells, such as neuroblastoma and nephroblastoma.
Definitions
A neoplasm is an abnormal tissue mass characterized by unregulated growth and lacking any beneficial function. The term is frequently employed interchangeably with the term tumor, which denotes a swelling.
Benign neoplasms typically have a gradual development rate and remain localized to their site of origin. While benign neoplasms typically follow a harmless trajectory, they may pose risks if they exert pressure on essential adjacent structures or if they emit hormones indiscriminately.
Malignant neoplasms possess the ability to disseminate or metastasis to remote locations, resulting in new tumors known as metastases, which can proliferate independently of the initial tumor.
Cancer is an overarching word for any malignant neoplasm.
Nomenclature of neoplasms
Epithelial neoplasms
Benign neoplasms of squamous epithelium are termed acanthomas when flat and papillomas when exhibiting branching fronds.
Benign neoplasms of glandular epithelium are referred to as adenomas.
Epithelial malignancies are classified as carcinomas.
Carcinomas exhibiting squamous differentiation are termed squamous cell carcinomas. Carcinomas exhibiting glandular differentiation are termed adenocarcinomas. Carcinomas frequently follow a stage of epithelial dysplasia, characterized by the presence of neoplastic cells inside the epithelium, without penetration beyond the epithelial boundaries.
Neoplasms of connective tissue Lipoma is a benign adipose tissue tumor. • Leiomyoma is a benign neoplasm of smooth muscle. • Rhabdomyoma is a benign neoplasm of skeletal muscle. • Angioma is a benign vascular neoplasm. • Osteoma is a benign osseous neoplasm. Liposarcoma is a malignant tumor of adipose tissue. Leiomyosarcoma is a malignant neoplasm of smooth muscle tissue. • Rhabdomyosarcoma is a malignant neoplasm of skeletal muscle. • Angiosarcoma is a malignant neoplasm of vascular tissue. • Osteosarcoma is a malignant neoplasm of bone.
Alternative neoplasm classifications Lymphomas, leukemias, and myeloma are hematological malignancies originating from blood or bone marrow cells.
Malignant melanoma is a tumor of malignant melanocytes. Malignant mesothelioma is a neoplastic mesothelial tumor. Germ cell tumors constitute a heterogeneous category of neoplasms that typically originate in the testes or ovaries. Embryonal tumors are a category of malignant neoplasms primarily observed in children, characterized by highly undifferentiated cells, such as neuroblastoma and nephroblastoma.
- Published on
Pathology - Carcinogenesis
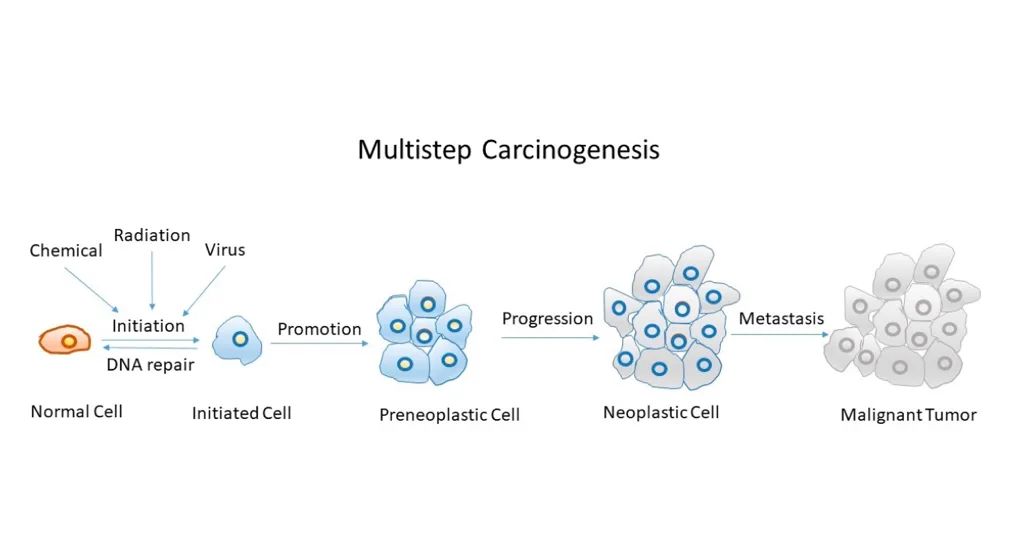
Definition • The series of events culminating in the formation of a malignant tumor.
Aetiology
• Radiation or chemicals that impair DNA, such as sunlight in skin carcinomas and cigarette smoke in lung carcinomas. Chronic inflammatory illnesses that induce sustained cellular proliferation, such as ulcerative colitis, increase the risk of colonic cancer
.• Elevated hormone levels induce the proliferation of hormonally responsive tissues, such as estrogens in breast and endometrial carcinomas. Oncogenic viruses synthesize proteins that facilitate unregulated cell proliferation, such as HPV in cervical cancer. Pathogenesis DNA damage to genes encoding proteins that govern cell division permits uncontrolled cellular proliferation. Genes regulating cell division are categorized into oncogenes and tumor suppressor genes. Oncogenes are mutated genes that facilitate cell division. Mutations typically lead to the overexpression of the gene product or the constitutive activation of the protein product. Examples of oncogenes frequently mutated in malignancies are KIT, RAS, and MYC.
Tumor suppressor genes
• Genes that encode proteins which typically decrease cellular proliferation. • Typically, the inactivation of both alleles is necessary for a tumorigenic impact. Examples of frequently altered tumour suppressor genes in malignancies include P53, CDKN2A, and RB
Metastasis
• The attainment of metastatic capability is a crucial occurrence in the progression of a neoplasm; dissemination to remote locations is a primary factor contributing to the mortality associated with malignant tumors. Malignant neoplasms disseminate through three primary pathways: hematogenous spread to distant organs (e.g., lungs, liver, bone, brain), lymphatic spread to regional lymph nodes (e.g., axillary lymph nodes in breast carcinomas), and transcoelomic spread, wherein malignant tumors adjacent to body cavities, such as the pleura or peritoneum, can infiltrate these spaces and propagate to other organs. Successful metastasis necessitates the malignant cells to surmount several obstacles: detachment from adjacent cells, degradation of the extracellular matrix, invasion of a vessel lumen, endurance in circulation while reaching a distant location, egress from the vessel, and effective implantation and proliferation at the new site.
Definition • The series of events culminating in the formation of a malignant tumor.
Aetiology
• Radiation or chemicals that impair DNA, such as sunlight in skin carcinomas and cigarette smoke in lung carcinomas. Chronic inflammatory illnesses that induce sustained cellular proliferation, such as ulcerative colitis, increase the risk of colonic cancer
.• Elevated hormone levels induce the proliferation of hormonally responsive tissues, such as estrogens in breast and endometrial carcinomas. Oncogenic viruses synthesize proteins that facilitate unregulated cell proliferation, such as HPV in cervical cancer. Pathogenesis DNA damage to genes encoding proteins that govern cell division permits uncontrolled cellular proliferation. Genes regulating cell division are categorized into oncogenes and tumor suppressor genes. Oncogenes are mutated genes that facilitate cell division. Mutations typically lead to the overexpression of the gene product or the constitutive activation of the protein product. Examples of oncogenes frequently mutated in malignancies are KIT, RAS, and MYC.
Tumor suppressor genes
• Genes that encode proteins which typically decrease cellular proliferation. • Typically, the inactivation of both alleles is necessary for a tumorigenic impact. Examples of frequently altered tumour suppressor genes in malignancies include P53, CDKN2A, and RB
Metastasis
• The attainment of metastatic capability is a crucial occurrence in the progression of a neoplasm; dissemination to remote locations is a primary factor contributing to the mortality associated with malignant tumors. Malignant neoplasms disseminate through three primary pathways: hematogenous spread to distant organs (e.g., lungs, liver, bone, brain), lymphatic spread to regional lymph nodes (e.g., axillary lymph nodes in breast carcinomas), and transcoelomic spread, wherein malignant tumors adjacent to body cavities, such as the pleura or peritoneum, can infiltrate these spaces and propagate to other organs. Successful metastasis necessitates the malignant cells to surmount several obstacles: detachment from adjacent cells, degradation of the extracellular matrix, invasion of a vessel lumen, endurance in circulation while reaching a distant location, egress from the vessel, and effective implantation and proliferation at the new site.
- Published on
Pathology – Microbes
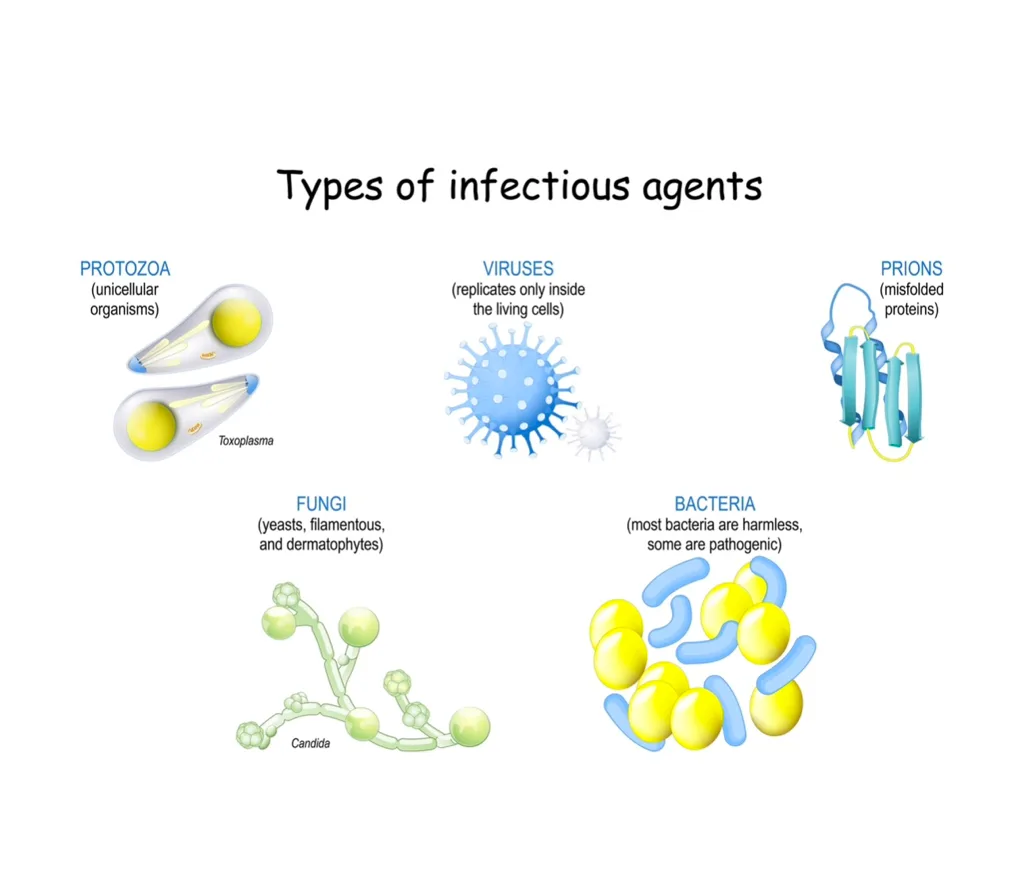
Bacteria • Unicellular entities possessing double-stranded DNA that resides freely in the cytoplasm, encased by a cell membrane and cell wall. • Predominantly thrive in the presence of oxygen (aerobes), however are capable of growth in its absence (facultative anaerobes). Certain organisms proliferate exclusively under anoxic conditions (strict anaerobes). Gram-positive bacteria possess a robust cell wall comprised of peptidoglycan plus an additional polymer, frequently teichoic acid. Gram-negative bacteria possess a weaker peptidoglycan layer, which is covered by an outer lipid membrane consisting of lipopolysaccharide. Mycobacteria are a kind of bacteria characterized by a thick, waxy cell wall that can be stained using the Ziehl–Nielsen method.
Viruses are the smallest and most basic organisms, consisting of genetic material in the form of DNA or RNA encased within a protein shell known as a capsid. Certain viruses possess an external lipid membrane obtained from the host cell in which they originated. • Obligate intracellular entities that proliferate exclusively by infecting a host cell and commandeering its metabolic machinery. • Induce disease by damaging host cells (direct cytopathic effect) or as a result of the immunological response to the infection. • Certain viruses can induce latent infections, such as herpes simplex. • Some viruses are carcinogenic and contribute to the transformation of host cells and the onset of malignancy, for instance, HPV in cervical cancer and EBV in nasopharyngeal carcinoma.
Fungi possess DNA encased within a nucleus, feature a cell membrane that includes ergosterol, and have an external cell wall made of chitin. Yeasts are unicellular fungi that reproduce asexually through budding, such as Candida. • Moulds develop as branching filaments termed hyphae that intertwine to create a complex structure known as mycelium. Mycelia generate spores. • Certain fungi can survive in both yeast and mold forms, such as Histoplasma
Protozoa are unicellular creatures that can inhabit host cells or exist in the extracellular milieu. Intracellular protozoa obtain nourishment from the host cell (e.g., Plasmodium, Leishmania, Toxoplasma). Extracellular protozoa obtain nutrients through direct intake and/or the consumption of sloughed epithelial cells (e.g., Giardia, Trichomonas). Helminths • Complex multicellular parasitic worms that vary in size from tiny entities to colossal animals several meters long. • Numerous species possess intricate life cycles that involve multiple hosts. • Categorized as nematodes (roundworms), cestodes (tapeworms), and trematodes (flukes)
Bacteria • Unicellular entities possessing double-stranded DNA that resides freely in the cytoplasm, encased by a cell membrane and cell wall. • Predominantly thrive in the presence of oxygen (aerobes), however are capable of growth in its absence (facultative anaerobes). Certain organisms proliferate exclusively under anoxic conditions (strict anaerobes). Gram-positive bacteria possess a robust cell wall comprised of peptidoglycan plus an additional polymer, frequently teichoic acid. Gram-negative bacteria possess a weaker peptidoglycan layer, which is covered by an outer lipid membrane consisting of lipopolysaccharide. Mycobacteria are a kind of bacteria characterized by a thick, waxy cell wall that can be stained using the Ziehl–Nielsen method.
Viruses are the smallest and most basic organisms, consisting of genetic material in the form of DNA or RNA encased within a protein shell known as a capsid. Certain viruses possess an external lipid membrane obtained from the host cell in which they originated. • Obligate intracellular entities that proliferate exclusively by infecting a host cell and commandeering its metabolic machinery. • Induce disease by damaging host cells (direct cytopathic effect) or as a result of the immunological response to the infection. • Certain viruses can induce latent infections, such as herpes simplex. • Some viruses are carcinogenic and contribute to the transformation of host cells and the onset of malignancy, for instance, HPV in cervical cancer and EBV in nasopharyngeal carcinoma.
Fungi possess DNA encased within a nucleus, feature a cell membrane that includes ergosterol, and have an external cell wall made of chitin. Yeasts are unicellular fungi that reproduce asexually through budding, such as Candida. • Moulds develop as branching filaments termed hyphae that intertwine to create a complex structure known as mycelium. Mycelia generate spores. • Certain fungi can survive in both yeast and mold forms, such as Histoplasma
Protozoa are unicellular creatures that can inhabit host cells or exist in the extracellular milieu. Intracellular protozoa obtain nourishment from the host cell (e.g., Plasmodium, Leishmania, Toxoplasma). Extracellular protozoa obtain nutrients through direct intake and/or the consumption of sloughed epithelial cells (e.g., Giardia, Trichomonas). Helminths • Complex multicellular parasitic worms that vary in size from tiny entities to colossal animals several meters long. • Numerous species possess intricate life cycles that involve multiple hosts. • Categorized as nematodes (roundworms), cestodes (tapeworms), and trematodes (flukes)
- Published on
Pathology- Human Immunodeficiency Virus
Pathogen
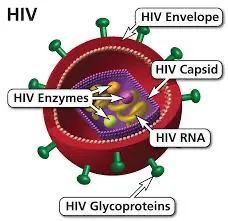
• Enveloped RNA virus with a single-stranded, positive-sense genome. • Belongs to the lentivirus genus within the retrovirus family.
Epidemiology
• Prevalent globally, particularly in Sub-Saharan Africa. • Designated as a pandemic by the World Health Organization (WHO).
Transmission
• Primary transmission pathways include unprotected sexual intercourse, infected needles, breast milk, and maternal transmission during childbirth
. • Transmission through transfused blood products has been nearly eradicated due to rigorous donor screening protocols.
Immunopathogenesis
• Infects CD4+ helper T lymphocytes, macrophages, and dendritic cells. • Extensive dissemination of lymphoid tissue transpires post-infection. • HIV-specific CD8+ cytotoxic T-cells initially manage the disease. • Subsequently, HIV evades immunological regulation via antigenic mutation. • Viral load escalates fast while CD4+ numbers decline sharply.
Presentation
• Acute seroconversion induces a flu-like disease characterized by fever, lymphadenopathy, pharyngitis, myalgia, rash, and oral ulcers. The latency phase subsequently ensues, typically remaining asymptomatic. The last phase is characterized by opportunistic infections and/or neoplasm. Common infections encompass bacterial pneumonia,pulmonary tuberculosis,Pneumocystis pneumonia, oesophageal candidiasis, cryptosporidiosis, Mycobacterium avium in the colon,cryptococcal meningitis, and cerebral toxoplasmosis.
Common neoplasms encompass cervical and anal warts, carcinoma, non-Hodgkin B-cell lymphomas, and Kaposi's sarcoma.
Histopathology
• Lymph nodes exhibit pronounced follicular proliferation accompanied by follicle lysis. Lymphomas are typically of the diffuse big B-cell variety.
• The bone marrow exhibits dysplasia characterized by disorganization of hematopoietic lineages and an elevated count of plasma cells.
• The skin may present with eosinophilic folliculitis, indicating infiltration of hair follicles by eosinophils. Cutaneous Kaposi's sarcoma exhibits an erratic proliferation of HHV-8-positive spindle cells inside the dermis, resulting in the formation of slit-like vascular gaps. Pneumocystis pneumonia is characterized by lymphocytic alveolitis accompanied by silver-positive organisms in the alveolar spaces. Prognosis: With contemporary anti-HIV medicine, numerous individuals can anticipate a lifespan approaching normalcy, resulting in death with HIV rather than from it.
Pathogen
• Enveloped RNA virus with a single-stranded, positive-sense genome. • Belongs to the lentivirus genus within the retrovirus family.
Epidemiology
• Prevalent globally, particularly in Sub-Saharan Africa. • Designated as a pandemic by the World Health Organization (WHO).
Transmission
• Primary transmission pathways include unprotected sexual intercourse, infected needles, breast milk, and maternal transmission during childbirth
. • Transmission through transfused blood products has been nearly eradicated due to rigorous donor screening protocols.
Immunopathogenesis
• Infects CD4+ helper T lymphocytes, macrophages, and dendritic cells. • Extensive dissemination of lymphoid tissue transpires post-infection. • HIV-specific CD8+ cytotoxic T-cells initially manage the disease. • Subsequently, HIV evades immunological regulation via antigenic mutation. • Viral load escalates fast while CD4+ numbers decline sharply.
Presentation
• Acute seroconversion induces a flu-like disease characterized by fever, lymphadenopathy, pharyngitis, myalgia, rash, and oral ulcers. The latency phase subsequently ensues, typically remaining asymptomatic. The last phase is characterized by opportunistic infections and/or neoplasm. Common infections encompass bacterial pneumonia,pulmonary tuberculosis,Pneumocystis pneumonia, oesophageal candidiasis, cryptosporidiosis, Mycobacterium avium in the colon,cryptococcal meningitis, and cerebral toxoplasmosis.
Common neoplasms encompass cervical and anal warts, carcinoma, non-Hodgkin B-cell lymphomas, and Kaposi's sarcoma.
Histopathology
• Lymph nodes exhibit pronounced follicular proliferation accompanied by follicle lysis. Lymphomas are typically of the diffuse big B-cell variety.
• The bone marrow exhibits dysplasia characterized by disorganization of hematopoietic lineages and an elevated count of plasma cells.
• The skin may present with eosinophilic folliculitis, indicating infiltration of hair follicles by eosinophils. Cutaneous Kaposi's sarcoma exhibits an erratic proliferation of HHV-8-positive spindle cells inside the dermis, resulting in the formation of slit-like vascular gaps. Pneumocystis pneumonia is characterized by lymphocytic alveolitis accompanied by silver-positive organisms in the alveolar spaces. Prognosis: With contemporary anti-HIV medicine, numerous individuals can anticipate a lifespan approaching normalcy, resulting in death with HIV rather than from it.
- Published on
Pathology- Antimicrobial agents
Antibacterial agents
Inhibitors of cellular wall biosynthesis • Disrupt peptidoglycan production. • Beta-lactams, such as penicillins and cephalosporins. • Glycopeptides, such as vancomycin and teicoplanin.
Protein synthesis inhibitors
• Bind to bacterial ribosomes and inhibit the elongation of protein chains. Aminoglycosides, such as gentamicin. • Tetracyclines, such as doxycycline. • Macrolides, such as erythromycin and clarithromycin.
Nucleic acid synthesis inhibitors
• Disrupt the production of DNA precursors or the process of DNA replication. • Sulfonamides, such as sulfamethoxazole. • Trimethoprim. • Quinolones, such as ciprofloxacin. • Rifamycins, such as rifampicin. • Nitroimidazoles, such as metronidazole.
Antiviral medications
Aciclovir is a guanosine analogue that undergoes phosphorylation by viral thymidine kinase. Aciclovir triphosphate is integrated into viral DNA, resulting in the cessation of chain replication. Ganciclovir is analogous to acyclovir, although exhibits more efficacy against cytomegalovirus (CMV). Contemporary HIV treatment employs a mix of reverse transcriptase inhibitors and protease inhibitors.
Antifungal medications
Azoles inhibit the formation of ergosterol, such as fluconazole. Polyenes disrupt the functionality of fungal cell membranes, such as amphotericin and nystatin.
Antibacterial agents
Inhibitors of cellular wall biosynthesis • Disrupt peptidoglycan production. • Beta-lactams, such as penicillins and cephalosporins. • Glycopeptides, such as vancomycin and teicoplanin.
Protein synthesis inhibitors
• Bind to bacterial ribosomes and inhibit the elongation of protein chains. Aminoglycosides, such as gentamicin. • Tetracyclines, such as doxycycline. • Macrolides, such as erythromycin and clarithromycin.
Nucleic acid synthesis inhibitors
• Disrupt the production of DNA precursors or the process of DNA replication. • Sulfonamides, such as sulfamethoxazole. • Trimethoprim. • Quinolones, such as ciprofloxacin. • Rifamycins, such as rifampicin. • Nitroimidazoles, such as metronidazole.
Antiviral medications
Aciclovir is a guanosine analogue that undergoes phosphorylation by viral thymidine kinase. Aciclovir triphosphate is integrated into viral DNA, resulting in the cessation of chain replication. Ganciclovir is analogous to acyclovir, although exhibits more efficacy against cytomegalovirus (CMV). Contemporary HIV treatment employs a mix of reverse transcriptase inhibitors and protease inhibitors.
Antifungal medications
Azoles inhibit the formation of ergosterol, such as fluconazole. Polyenes disrupt the functionality of fungal cell membranes, such as amphotericin and nystatin.