- Published on
KembaraXtra-Medicine- Anovulatory Uterine Bleeding
Definition
Anovulatory uterine bleeding refers to abnormal uterine bleeding that results from disruption of normal ovulation. It is characterized by noncyclic, irregular, and unpredictable bleeding in both timing and volume due to dysfunction of the hypothalamic–pituitary–ovarian (HPO) axis. Because ovulation does not occur consistently, normal hormonal feedback and endometrial stability are lost, leading to abnormal shedding of the endometrium. This condition is also referred to as abnormal uterine bleeding associated with ovulatory dysfunction (AUB-O).
Epidemiology and Demographics
Anovulatory uterine bleeding is common among reproductive-age women, with an estimated prevalence of approximately 53 per 1000 women in the United States and 3% to 30% internationally. It occurs most frequently at times of physiologic hormonal transition. During puberty, immaturity of the HPO axis commonly results in irregular and anovulatory cycles, particularly within the first two to three years after menarche. In perimenopause, declining ovarian reserve and erratic follicular recruitment lead to frequent anovulatory cycles. Anovulation is also common during pregnancy and lactation.
Risk Factors
Any condition that disrupts the normal function of the HPO axis increases the risk of anovulatory bleeding. Extremes of body weight, including obesity and underweight states, are significant risk factors. Chronic stress, excessive exercise, eating disorders, and systemic illness may also impair ovulation and contribute to abnormal bleeding patterns.
Clinical Presentation and Physical Findings
Patients with anovulatory uterine bleeding often report irregular menstrual cycles with variable cycle length and inconsistent bleeding volume. Unlike ovulatory cycles, these patients may lack premenstrual symptoms such as breast tenderness, cramping, bloating, or vaginal discharge. Underweight patients or those with eating disorders or high levels of physical activity may show signs of hypogonadotropic hypogonadism. Obesity may be associated with excessive estrogen production. Hyperandrogenic features such as acne, hirsutism, or male-pattern hair growth suggest conditions such as polycystic ovary syndrome (PCOS), congenital adrenal hyperplasia, Cushing syndrome, or androgen-secreting tumors.
Etiology and Pathophysiology
Anovulatory uterine bleeding arises from a breakdown in the normal hormonal relationship between the HPO axis and the endometrium. In a normal menstrual cycle, estrogen stimulates endometrial proliferation during the follicular phase, followed by ovulation and progesterone secretion during the luteal phase. Progesterone stabilizes the endometrium, and its withdrawal leads to orderly menstruation. In anovulatory cycles, progesterone is absent or insufficient, resulting in unopposed estrogen exposure. This causes continued endometrial proliferation with unpredictable breakdown, irregular shedding, and abnormal bleeding.
Disorders of the HPO axis include hypogonadotropic hypogonadism due to genetic conditions, functional causes such as eating disorders or excessive exercise, or hypothalamic–pituitary tumors. Hypergonadotropic hypogonadism may result from conditions such as Turner syndrome, chemotherapy, autoimmune oophoritis, or gonadal dysgenesis. Hyperprolactinemia may be caused by medications, prolactinomas, hypothyroidism, malignancy, or infiltrative disease. Polycystic ovary syndrome is a particularly common cause, characterized by chronic anovulation, androgen excess, and prolonged unopposed estrogen exposure.
Diagnosis and Differential Diagnosis
The differential diagnosis of anovulatory uterine bleeding includes pregnancy, thyroid disease, hyperprolactinemia, hyperandrogenic disorders, premature ovarian insufficiency, excessive exercise, stress, anorexia, and medication effects. Pregnancy must always be excluded first. Diagnosis is based on clinical history, physical examination, and targeted laboratory and imaging evaluation.
Diagnostic Workup
Laboratory evaluation typically includes human chorionic gonadotropin testing to exclude pregnancy, thyroid-stimulating hormone, prolactin, follicle-stimulating hormone, luteinizing hormone, estradiol, testosterone, and 17-hydroxyprogesterone levels. Pelvic ultrasound is useful when PCOS or ovarian tumors are suspected. Brain MRI is indicated in cases of unexplained hyperprolactinemia or hypothalamic amenorrhea, while abdominal imaging may be required if an adrenal tumor is suspected.
Management and Treatment
Treatment is directed at both controlling abnormal bleeding and addressing the underlying cause of anovulation. Nonpharmacologic management includes weight loss and increased physical activity for obese patients, as well as improved nutrition and reduction in excessive exercise for underweight patients or those with hypothalamic dysfunction.
For patients who are not pregnant, a withdrawal bleed can be induced with medroxyprogesterone acetate given for 7 to 10 days. Management of specific etiologies includes thyroid replacement for hypothyroidism, dopamine agonists or medication adjustment for hyperprolactinemia, and hormonal regulation for PCOS. Combined oral contraceptives are particularly effective in PCOS, as estrogen increases sex hormone–binding globulin and reduces free androgen levels while providing endometrial protection. Progestin-only therapy is also effective for endometrial protection. Metformin improves insulin sensitivity and may induce ovulation in PCOS but is less effective than ovulation-induction agents.
Hypothalamic dysfunction is treated with nutritional rehabilitation, reduced exercise intensity, treatment of eating disorders, and estrogen replacement when indicated. Premature ovarian insufficiency is managed with estrogen replacement therapy, with the addition of progestin if the uterus is present to protect the endometrium.
Fertility Considerations
Ovulation induction is an option for patients desiring fertility. Injectable gonadotropins are typically required for hypogonadotropic hypogonadism. In PCOS, letrozole or clomiphene citrate are first-line agents for ovulation induction. Nonclassical congenital adrenal hyperplasia may be treated with glucocorticoids combined with ovulation-induction agents. Patients with premature ovarian insufficiency have a very low chance of spontaneous conception and often require donor oocytes or embryos.
Pearls and Clinical Considerations
Polycystic ovary syndrome is the most common cause of anovulation, affecting approximately 6% to 10% of women. Patients with PCOS should be screened for metabolic complications, including insulin resistance, diabetes, dyslipidemia, hypertension, cardiovascular disease, and nonalcoholic fatty liver disease. Chronic unopposed estrogen exposure increases the risk of endometrial hyperplasia and carcinoma, making cycle regulation or regular progestin withdrawal essential. In patients requiring estrogen replacement, concurrent progestin therapy is mandatory if the uterus is present.
Patient and Family Education
Counseling should emphasize the importance of optimal nutrition and healthy body weight. Bone health should be addressed in patients with hypothalamic dysfunction due to low estrogen levels. Patients with PCOS should be educated about metabolic and endometrial cancer risks. Fertility goals and future reproductive options should be discussed with all patients.
Definition
Anovulatory uterine bleeding refers to abnormal uterine bleeding that results from disruption of normal ovulation. It is characterized by noncyclic, irregular, and unpredictable bleeding in both timing and volume due to dysfunction of the hypothalamic–pituitary–ovarian (HPO) axis. Because ovulation does not occur consistently, normal hormonal feedback and endometrial stability are lost, leading to abnormal shedding of the endometrium. This condition is also referred to as abnormal uterine bleeding associated with ovulatory dysfunction (AUB-O).
Epidemiology and Demographics
Anovulatory uterine bleeding is common among reproductive-age women, with an estimated prevalence of approximately 53 per 1000 women in the United States and 3% to 30% internationally. It occurs most frequently at times of physiologic hormonal transition. During puberty, immaturity of the HPO axis commonly results in irregular and anovulatory cycles, particularly within the first two to three years after menarche. In perimenopause, declining ovarian reserve and erratic follicular recruitment lead to frequent anovulatory cycles. Anovulation is also common during pregnancy and lactation.
Risk Factors
Any condition that disrupts the normal function of the HPO axis increases the risk of anovulatory bleeding. Extremes of body weight, including obesity and underweight states, are significant risk factors. Chronic stress, excessive exercise, eating disorders, and systemic illness may also impair ovulation and contribute to abnormal bleeding patterns.
Clinical Presentation and Physical Findings
Patients with anovulatory uterine bleeding often report irregular menstrual cycles with variable cycle length and inconsistent bleeding volume. Unlike ovulatory cycles, these patients may lack premenstrual symptoms such as breast tenderness, cramping, bloating, or vaginal discharge. Underweight patients or those with eating disorders or high levels of physical activity may show signs of hypogonadotropic hypogonadism. Obesity may be associated with excessive estrogen production. Hyperandrogenic features such as acne, hirsutism, or male-pattern hair growth suggest conditions such as polycystic ovary syndrome (PCOS), congenital adrenal hyperplasia, Cushing syndrome, or androgen-secreting tumors.
Etiology and Pathophysiology
Anovulatory uterine bleeding arises from a breakdown in the normal hormonal relationship between the HPO axis and the endometrium. In a normal menstrual cycle, estrogen stimulates endometrial proliferation during the follicular phase, followed by ovulation and progesterone secretion during the luteal phase. Progesterone stabilizes the endometrium, and its withdrawal leads to orderly menstruation. In anovulatory cycles, progesterone is absent or insufficient, resulting in unopposed estrogen exposure. This causes continued endometrial proliferation with unpredictable breakdown, irregular shedding, and abnormal bleeding.
Disorders of the HPO axis include hypogonadotropic hypogonadism due to genetic conditions, functional causes such as eating disorders or excessive exercise, or hypothalamic–pituitary tumors. Hypergonadotropic hypogonadism may result from conditions such as Turner syndrome, chemotherapy, autoimmune oophoritis, or gonadal dysgenesis. Hyperprolactinemia may be caused by medications, prolactinomas, hypothyroidism, malignancy, or infiltrative disease. Polycystic ovary syndrome is a particularly common cause, characterized by chronic anovulation, androgen excess, and prolonged unopposed estrogen exposure.
Diagnosis and Differential Diagnosis
The differential diagnosis of anovulatory uterine bleeding includes pregnancy, thyroid disease, hyperprolactinemia, hyperandrogenic disorders, premature ovarian insufficiency, excessive exercise, stress, anorexia, and medication effects. Pregnancy must always be excluded first. Diagnosis is based on clinical history, physical examination, and targeted laboratory and imaging evaluation.
Diagnostic Workup
Laboratory evaluation typically includes human chorionic gonadotropin testing to exclude pregnancy, thyroid-stimulating hormone, prolactin, follicle-stimulating hormone, luteinizing hormone, estradiol, testosterone, and 17-hydroxyprogesterone levels. Pelvic ultrasound is useful when PCOS or ovarian tumors are suspected. Brain MRI is indicated in cases of unexplained hyperprolactinemia or hypothalamic amenorrhea, while abdominal imaging may be required if an adrenal tumor is suspected.
Management and Treatment
Treatment is directed at both controlling abnormal bleeding and addressing the underlying cause of anovulation. Nonpharmacologic management includes weight loss and increased physical activity for obese patients, as well as improved nutrition and reduction in excessive exercise for underweight patients or those with hypothalamic dysfunction.
For patients who are not pregnant, a withdrawal bleed can be induced with medroxyprogesterone acetate given for 7 to 10 days. Management of specific etiologies includes thyroid replacement for hypothyroidism, dopamine agonists or medication adjustment for hyperprolactinemia, and hormonal regulation for PCOS. Combined oral contraceptives are particularly effective in PCOS, as estrogen increases sex hormone–binding globulin and reduces free androgen levels while providing endometrial protection. Progestin-only therapy is also effective for endometrial protection. Metformin improves insulin sensitivity and may induce ovulation in PCOS but is less effective than ovulation-induction agents.
Hypothalamic dysfunction is treated with nutritional rehabilitation, reduced exercise intensity, treatment of eating disorders, and estrogen replacement when indicated. Premature ovarian insufficiency is managed with estrogen replacement therapy, with the addition of progestin if the uterus is present to protect the endometrium.
Fertility Considerations
Ovulation induction is an option for patients desiring fertility. Injectable gonadotropins are typically required for hypogonadotropic hypogonadism. In PCOS, letrozole or clomiphene citrate are first-line agents for ovulation induction. Nonclassical congenital adrenal hyperplasia may be treated with glucocorticoids combined with ovulation-induction agents. Patients with premature ovarian insufficiency have a very low chance of spontaneous conception and often require donor oocytes or embryos.
Pearls and Clinical Considerations
Polycystic ovary syndrome is the most common cause of anovulation, affecting approximately 6% to 10% of women. Patients with PCOS should be screened for metabolic complications, including insulin resistance, diabetes, dyslipidemia, hypertension, cardiovascular disease, and nonalcoholic fatty liver disease. Chronic unopposed estrogen exposure increases the risk of endometrial hyperplasia and carcinoma, making cycle regulation or regular progestin withdrawal essential. In patients requiring estrogen replacement, concurrent progestin therapy is mandatory if the uterus is present.
Patient and Family Education
Counseling should emphasize the importance of optimal nutrition and healthy body weight. Bone health should be addressed in patients with hypothalamic dysfunction due to low estrogen levels. Patients with PCOS should be educated about metabolic and endometrial cancer risks. Fertility goals and future reproductive options should be discussed with all patients.

- Published on
KembaraXtra-Medicine- Anorexia–Cachexia Syndrome Associated with Malignancy
Basic Information and Definition
Anorexia–cachexia syndrome is a complex metabolic condition associated with underlying malignancy, characterized by reduced appetite and a progressive loss of skeletal muscle mass, with or without loss of fat mass. Unlike simple starvation, this syndrome cannot be fully reversed by conventional nutritional support alone. It reflects a multifactorial process involving metabolic, inflammatory, and neurohormonal alterations. The condition is commonly referred to as cancer cachexia and is coded as ICD-10-CM R64.
Epidemiology and Demographics
The prevalence of cancer cachexia varies widely due to differences in diagnostic criteria across studies, with reported incidence ranging from 12% to as high as 85% depending on the definition used. The syndrome is particularly common in patients with lung and gastrointestinal malignancies. In several studies, more than half of patients with advanced cancer met criteria for cachexia when defined by anorexia and weight loss exceeding 5%. Cachexia contributes significantly to morbidity and mortality in oncology patients.
Genetic and Inflammatory Factors
Genetic susceptibility appears to influence the development and severity of cancer cachexia. Certain polymorphisms, particularly those associated with elevated inflammatory markers and vitamin D receptor variants, may predispose patients to a more aggressive cachectic phenotype. Although no single nucleotide polymorphism has been definitively linked to cancer cachexia, variants associated with increased inflammatory cytokine production, loss of lean and fat mass, and reduced survival are thought to increase vulnerability.
Etiology and Pathophysiology
Among patients with malignancy, anorexia is common and leads to decreased caloric intake and malnutrition. Cancer cachexia is driven by a systemic inflammatory response mediated by cytokines such as interleukin-6, interleukin-1, interferon-gamma, and tumor necrosis factor-alpha. These cytokines activate the ubiquitin–proteasome pathway via nuclear factor kappa B, leading to accelerated muscle protein degradation. Simultaneously, protein synthesis is suppressed through downregulation of myogenic differentiation factors such as MyoD. The inflammatory milieu also induces a hypermetabolic state, shifting the balance toward catabolism with increased lipolysis and muscle wasting.
Diagnosis and Differential Diagnosis
The differential diagnosis of anorexia–cachexia syndrome includes starvation, malabsorption syndromes, hyperthyroidism, anorexia nervosa, and major depressive disorder. Accurate diagnosis requires exclusion of these conditions and recognition of cachexia as a distinct metabolic process related to malignancy rather than inadequate intake alone.
Clinical Assessment and Staging
Patients with cancer cachexia can be categorized into three stages: precachexia, cachexia, and refractory cachexia. Assessment involves evaluation across multiple domains, including food intake, catabolic and inflammatory changes, functional impairment, psychosocial impact, and body composition, particularly muscle and adipose tissue stores. Diagnostic criteria include unintentional weight loss greater than 5% in the absence of starvation, a body mass index below 20 with weight loss exceeding 2%, or evidence of sarcopenia with more than 2% weight loss.
Laboratory and Imaging Evaluation
Laboratory assessment typically includes a complete blood count, comprehensive metabolic panel, serum albumin and prealbumin levels, and inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein. Endocrine evaluation may include thyroid-stimulating hormone, cortisol, adrenocorticotropic hormone, and testosterone levels. Imaging with computed tomography or magnetic resonance imaging can be used to assess body composition and quantify sarcopenia by measuring muscle mass.
Treatment Overview
Management of anorexia–cachexia syndrome is multimodal and focuses on aggressive nutritional support, symptom control, and treatment of the underlying malignancy. Functional causes of malabsorption or gastrointestinal obstruction should be identified and addressed early. A structured, comprehensive approach that includes education, early recognition, exercise, nutritional optimization, and targeted pharmacologic therapy is recommended.
Nonpharmacologic Therapy
Nutritional intervention emphasizes frequent, small, calorie-dense meals, often supplemented with liquid nutritional formulations, under the guidance of a nutritionist. Physical activity, when feasible, plays a crucial role by modulating muscle metabolism, improving insulin sensitivity, reducing inflammation, preserving muscle mass, and enhancing functional performance. Exercise also contributes to improved quality of life and overall well-being.
Pharmacologic and Acute Management
Pharmacologic therapy is primarily aimed at appetite stimulation and modulation of inflammation. Glucocorticoids such as prednisone or dexamethasone can transiently improve appetite but are limited by significant side effects, including immunosuppression, muscle weakness, and adrenal insufficiency. Megestrol acetate may improve appetite and body weight but does not significantly enhance lean body mass and carries risks such as thromboembolism and hormonal suppression. Cannabinoids, including dronabinol, have not demonstrated consistent benefit in appetite or weight gain. Other agents, such as mirtazapine and olanzapine, may be beneficial in selected patients, particularly those undergoing chemotherapy with associated nausea and weight loss. Nonsteroidal antiinflammatory drugs, including celecoxib, have shown modest benefits in weight and quality of life in some studies, especially when used as part of combination therapy.
Emerging and Investigational Therapies
Anamorelin, a ghrelin receptor agonist, has demonstrated increases in lean body mass in patients with advanced non–small cell lung cancer, although functional outcomes such as muscle strength have not consistently improved. Multimodal strategies combining nutritional support, antiinflammatory therapy, and structured exercise programs are under investigation, including large randomized trials evaluating comprehensive interventions in advanced cancers.
Chronic Management and Supportive Care
Long-term management includes continued nutritional supplementation, rehabilitation, and exercise programs. The benefits of amino acids, omega-3 fatty acids, and docosahexaenoic acid remain inconclusive. Ongoing reassessment and adjustment of care plans are essential as the disease progresses.
Referral and Prognostic Considerations
Referral to nutrition specialists, dedicated cachexia clinics, and palliative care services is strongly recommended. Cancer cachexia is frequently underrecognized and contributes directly to mortality in a significant proportion of patients with advanced malignancy. Early identification and intervention, particularly in the precachexia stage, may improve outcomes. Enrollment in clinical trials should be considered whenever available to advance understanding and management of this challenging syndrome.
Basic Information and Definition
Anorexia–cachexia syndrome is a complex metabolic condition associated with underlying malignancy, characterized by reduced appetite and a progressive loss of skeletal muscle mass, with or without loss of fat mass. Unlike simple starvation, this syndrome cannot be fully reversed by conventional nutritional support alone. It reflects a multifactorial process involving metabolic, inflammatory, and neurohormonal alterations. The condition is commonly referred to as cancer cachexia and is coded as ICD-10-CM R64.
Epidemiology and Demographics
The prevalence of cancer cachexia varies widely due to differences in diagnostic criteria across studies, with reported incidence ranging from 12% to as high as 85% depending on the definition used. The syndrome is particularly common in patients with lung and gastrointestinal malignancies. In several studies, more than half of patients with advanced cancer met criteria for cachexia when defined by anorexia and weight loss exceeding 5%. Cachexia contributes significantly to morbidity and mortality in oncology patients.
Genetic and Inflammatory Factors
Genetic susceptibility appears to influence the development and severity of cancer cachexia. Certain polymorphisms, particularly those associated with elevated inflammatory markers and vitamin D receptor variants, may predispose patients to a more aggressive cachectic phenotype. Although no single nucleotide polymorphism has been definitively linked to cancer cachexia, variants associated with increased inflammatory cytokine production, loss of lean and fat mass, and reduced survival are thought to increase vulnerability.
Etiology and Pathophysiology
Among patients with malignancy, anorexia is common and leads to decreased caloric intake and malnutrition. Cancer cachexia is driven by a systemic inflammatory response mediated by cytokines such as interleukin-6, interleukin-1, interferon-gamma, and tumor necrosis factor-alpha. These cytokines activate the ubiquitin–proteasome pathway via nuclear factor kappa B, leading to accelerated muscle protein degradation. Simultaneously, protein synthesis is suppressed through downregulation of myogenic differentiation factors such as MyoD. The inflammatory milieu also induces a hypermetabolic state, shifting the balance toward catabolism with increased lipolysis and muscle wasting.
Diagnosis and Differential Diagnosis
The differential diagnosis of anorexia–cachexia syndrome includes starvation, malabsorption syndromes, hyperthyroidism, anorexia nervosa, and major depressive disorder. Accurate diagnosis requires exclusion of these conditions and recognition of cachexia as a distinct metabolic process related to malignancy rather than inadequate intake alone.
Clinical Assessment and Staging
Patients with cancer cachexia can be categorized into three stages: precachexia, cachexia, and refractory cachexia. Assessment involves evaluation across multiple domains, including food intake, catabolic and inflammatory changes, functional impairment, psychosocial impact, and body composition, particularly muscle and adipose tissue stores. Diagnostic criteria include unintentional weight loss greater than 5% in the absence of starvation, a body mass index below 20 with weight loss exceeding 2%, or evidence of sarcopenia with more than 2% weight loss.
Laboratory and Imaging Evaluation
Laboratory assessment typically includes a complete blood count, comprehensive metabolic panel, serum albumin and prealbumin levels, and inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein. Endocrine evaluation may include thyroid-stimulating hormone, cortisol, adrenocorticotropic hormone, and testosterone levels. Imaging with computed tomography or magnetic resonance imaging can be used to assess body composition and quantify sarcopenia by measuring muscle mass.
Treatment Overview
Management of anorexia–cachexia syndrome is multimodal and focuses on aggressive nutritional support, symptom control, and treatment of the underlying malignancy. Functional causes of malabsorption or gastrointestinal obstruction should be identified and addressed early. A structured, comprehensive approach that includes education, early recognition, exercise, nutritional optimization, and targeted pharmacologic therapy is recommended.
Nonpharmacologic Therapy
Nutritional intervention emphasizes frequent, small, calorie-dense meals, often supplemented with liquid nutritional formulations, under the guidance of a nutritionist. Physical activity, when feasible, plays a crucial role by modulating muscle metabolism, improving insulin sensitivity, reducing inflammation, preserving muscle mass, and enhancing functional performance. Exercise also contributes to improved quality of life and overall well-being.
Pharmacologic and Acute Management
Pharmacologic therapy is primarily aimed at appetite stimulation and modulation of inflammation. Glucocorticoids such as prednisone or dexamethasone can transiently improve appetite but are limited by significant side effects, including immunosuppression, muscle weakness, and adrenal insufficiency. Megestrol acetate may improve appetite and body weight but does not significantly enhance lean body mass and carries risks such as thromboembolism and hormonal suppression. Cannabinoids, including dronabinol, have not demonstrated consistent benefit in appetite or weight gain. Other agents, such as mirtazapine and olanzapine, may be beneficial in selected patients, particularly those undergoing chemotherapy with associated nausea and weight loss. Nonsteroidal antiinflammatory drugs, including celecoxib, have shown modest benefits in weight and quality of life in some studies, especially when used as part of combination therapy.
Emerging and Investigational Therapies
Anamorelin, a ghrelin receptor agonist, has demonstrated increases in lean body mass in patients with advanced non–small cell lung cancer, although functional outcomes such as muscle strength have not consistently improved. Multimodal strategies combining nutritional support, antiinflammatory therapy, and structured exercise programs are under investigation, including large randomized trials evaluating comprehensive interventions in advanced cancers.
Chronic Management and Supportive Care
Long-term management includes continued nutritional supplementation, rehabilitation, and exercise programs. The benefits of amino acids, omega-3 fatty acids, and docosahexaenoic acid remain inconclusive. Ongoing reassessment and adjustment of care plans are essential as the disease progresses.
Referral and Prognostic Considerations
Referral to nutrition specialists, dedicated cachexia clinics, and palliative care services is strongly recommended. Cancer cachexia is frequently underrecognized and contributes directly to mortality in a significant proportion of patients with advanced malignancy. Early identification and intervention, particularly in the precachexia stage, may improve outcomes. Enrollment in clinical trials should be considered whenever available to advance understanding and management of this challenging syndrome.

- Published on
KembaraXtra-Medicine- Anorexia Nervosa
Basic Information and Definition
Anorexia nervosa is a serious psychiatric disorder characterized by abnormal eating behaviors, intense fear of weight gain, severe self-induced weight loss, and a distinct disturbance in body image and self-perception. The disorder involves both psychological and physiological components and can affect nearly every organ system. It is classified into restricting type and binge-eating/purging type. ICD-10-CM codes include F50.00 (unspecified), F50.01 (restricting type), and F50.02 (binge-eating/purging type).
Epidemiology and Demographics
In the United States, anorexia nervosa affects approximately 0.2% to 1.3% of the general population, with an annual incidence of 5 to 10 cases per 100,000 individuals. The disorder is strongly associated with activities that emphasize thinness, such as competitive athletics and modeling. Females are disproportionately affected, with a female-to-male ratio of approximately 20:1. About 0.5% to 1% of women aged 15 to 30 years and up to 1.5% of teenage girls are affected. Adolescence to young adulthood is the most common age of onset, with a mean onset around 17 years.
Physical Findings and Clinical Presentation
Eating disorders can present with subtle, nonspecific symptoms in early or mild cases, including fatigue, cold intolerance, dizziness, and low energy, making early recognition challenging. Children and adolescents are particularly vulnerable due to ongoing growth and development. In moderate to severe anorexia nervosa, patients often appear markedly emaciated and may wear layered clothing to conceal weight loss. The skin is typically dry, may exhibit lanugo hair, and can appear yellowish due to carotenodermia. Hair thinning, brittle nails, bradycardia, hypotension, hypothermia, and bradypnea are common. Peripheral edema may occur. In females, normal fat distribution is lost, although axillary and pubic hair are usually preserved.
Etiology and Pathophysiology
The etiology of anorexia nervosa is multifactorial and incompletely understood, involving sociocultural pressures, psychological vulnerabilities, familial dynamics, and genetic predisposition. A history of sexual abuse has been reported in up to half of affected individuals. Psychologically, patients often struggle with low self-esteem, impaired identity formation, and a strong need for control. Body weight and food intake may become central mechanisms through which individuals attempt to exert control over their environment and emotions.
Diagnostic Criteria
Diagnosis is based on clinical assessment and DSM-5 criteria. These include restriction of energy intake leading to significantly low body weight for age, sex, and developmental stage; intense fear of gaining weight or persistent behavior interfering with weight gain; and disturbance in body image or lack of recognition of the seriousness of low body weight. Subtypes include the restricting type, characterized by dieting, fasting, or excessive exercise without bingeing or purging, and the binge-eating/purging type, which includes recurrent binge eating or purging behaviors. Amenorrhea, although historically emphasized, may be absent in younger adolescents and is no longer required for diagnosis.
Differential Diagnosis
Conditions that may mimic or coexist with anorexia nervosa include other eating disorders such as bulimia nervosa and binge eating disorder, substance use disorders, major depressive disorder, obsessive-compulsive disorder, schizophrenia, and conversion disorder. Medical causes of weight loss must also be considered, including malignancy, endocrine disorders (such as Addison disease, diabetes mellitus, thyroid disorders, or panhypopituitarism), gastrointestinal diseases (celiac disease, Crohn disease, parasitic infections), and chronic infections such as tuberculosis or HIV.
Workup and Screening
Screening for eating disorders should be incorporated into routine psychosocial assessments, especially in adolescents. Patients may minimize symptoms; therefore, collateral history from parents or caregivers is essential. The SCOFF questionnaire is a useful screening tool, with high sensitivity for anorexia and bulimia when two or more responses are positive. Baseline electrocardiography is recommended for all patients to assess for QT interval prolongation, which is associated with increased risk of sudden cardiac death. A dual-energy x-ray absorptiometry (DEXA) scan should be considered after six months of amenorrhea to evaluate for osteopenia or osteoporosis.
Laboratory Findings
Laboratory results may be normal in mild cases. Common abnormalities include endocrine changes such as decreased gonadotropins, estrogens, and thyroid hormones, with normal thyroid-stimulating hormone and elevated cortisol. Hematologic abnormalities may include leukopenia, anemia, thrombocytopenia, and reduced inflammatory markers. Electrolyte disturbances such as hypokalemia, hypomagnesemia, hypocalcemia, hypophosphatemia, metabolic alkalosis, and hypercholesterolemia may occur. Elevated plasma beta-carotene levels can help distinguish anorexia nervosa from other causes of starvation.
Treatment and Nonpharmacologic Management
Management requires a multidisciplinary approach involving medical, nutritional, and psychological care. A target weight should be established, aiming for 100% of ideal body weight in adolescents and 90% to 100% in adults. Weight restoration should proceed gradually, with initial caloric intake of 800 to 1200 kcal per day in small, frequent meals, advancing to 1500 to 3000 kcal as tolerated. Electrolytes must be monitored closely to prevent refeeding syndrome. In severe cases, enteral or parenteral nutrition may be necessary. Mealtimes should emphasize support rather than confrontation, and post-meal supervision may be required to prevent purging or excessive exercise.
Acute Management and Severity Assessment
Severity is categorized by body mass index in adults or BMI percentile in children and adolescents. Mild disease corresponds to a BMI of 17 kg/m² or higher, moderate disease to BMI 16–16.99, severe disease to BMI 15–15.99, and extreme disease to BMI below 15. Most patients can be managed as outpatients; however, inpatient care is indicated for medical instability, severe electrolyte disturbances, significant bradycardia or hypotension, prolonged QT interval, rapid weight loss, failure of outpatient treatment, or suicidal ideation. Pharmacologic therapy generally has limited benefit unless comorbid depression, anxiety, or obsessive-compulsive symptoms are present.
Chronic Management and Psychotherapy
Long-term psychotherapy is central to recovery and may need to continue for years. Treatment focuses on body image, self-esteem, interpersonal relationships, and relapse prevention. Family-based therapy is particularly effective in children and adolescents and is strongly recommended.
Disposition and Prognosis
The long-term prognosis of anorexia nervosa is guarded, with many patients experiencing relapses or persistent disordered eating and body image distortion. Menstrual function typically returns within six months of achieving 90% of ideal body weight, although pregnancy can occur even in the presence of amenorrhea. Mortality rates range from 5% to 20%, significantly higher than in age-matched peers, with common causes including electrolyte imbalance, starvation, and suicide. Favorable prognostic factors include early diagnosis, prompt treatment initiation, strong family support, and positive therapeutic relationships.
Referral and Indications for Hospitalization
Hospitalization should be considered for severe dehydration, electrolyte abnormalities, cardiac arrhythmias, significant physiologic instability, intractable purging, suicidal thoughts, weight loss exceeding 30% of ideal body weight, rapid ongoing weight loss, or failure of outpatient nutritional rehabilitation. Early involvement of mental health specialists is essential to optimize outcomes.
Basic Information and Definition
Anorexia nervosa is a serious psychiatric disorder characterized by abnormal eating behaviors, intense fear of weight gain, severe self-induced weight loss, and a distinct disturbance in body image and self-perception. The disorder involves both psychological and physiological components and can affect nearly every organ system. It is classified into restricting type and binge-eating/purging type. ICD-10-CM codes include F50.00 (unspecified), F50.01 (restricting type), and F50.02 (binge-eating/purging type).
Epidemiology and Demographics
In the United States, anorexia nervosa affects approximately 0.2% to 1.3% of the general population, with an annual incidence of 5 to 10 cases per 100,000 individuals. The disorder is strongly associated with activities that emphasize thinness, such as competitive athletics and modeling. Females are disproportionately affected, with a female-to-male ratio of approximately 20:1. About 0.5% to 1% of women aged 15 to 30 years and up to 1.5% of teenage girls are affected. Adolescence to young adulthood is the most common age of onset, with a mean onset around 17 years.
Physical Findings and Clinical Presentation
Eating disorders can present with subtle, nonspecific symptoms in early or mild cases, including fatigue, cold intolerance, dizziness, and low energy, making early recognition challenging. Children and adolescents are particularly vulnerable due to ongoing growth and development. In moderate to severe anorexia nervosa, patients often appear markedly emaciated and may wear layered clothing to conceal weight loss. The skin is typically dry, may exhibit lanugo hair, and can appear yellowish due to carotenodermia. Hair thinning, brittle nails, bradycardia, hypotension, hypothermia, and bradypnea are common. Peripheral edema may occur. In females, normal fat distribution is lost, although axillary and pubic hair are usually preserved.
Etiology and Pathophysiology
The etiology of anorexia nervosa is multifactorial and incompletely understood, involving sociocultural pressures, psychological vulnerabilities, familial dynamics, and genetic predisposition. A history of sexual abuse has been reported in up to half of affected individuals. Psychologically, patients often struggle with low self-esteem, impaired identity formation, and a strong need for control. Body weight and food intake may become central mechanisms through which individuals attempt to exert control over their environment and emotions.
Diagnostic Criteria
Diagnosis is based on clinical assessment and DSM-5 criteria. These include restriction of energy intake leading to significantly low body weight for age, sex, and developmental stage; intense fear of gaining weight or persistent behavior interfering with weight gain; and disturbance in body image or lack of recognition of the seriousness of low body weight. Subtypes include the restricting type, characterized by dieting, fasting, or excessive exercise without bingeing or purging, and the binge-eating/purging type, which includes recurrent binge eating or purging behaviors. Amenorrhea, although historically emphasized, may be absent in younger adolescents and is no longer required for diagnosis.
Differential Diagnosis
Conditions that may mimic or coexist with anorexia nervosa include other eating disorders such as bulimia nervosa and binge eating disorder, substance use disorders, major depressive disorder, obsessive-compulsive disorder, schizophrenia, and conversion disorder. Medical causes of weight loss must also be considered, including malignancy, endocrine disorders (such as Addison disease, diabetes mellitus, thyroid disorders, or panhypopituitarism), gastrointestinal diseases (celiac disease, Crohn disease, parasitic infections), and chronic infections such as tuberculosis or HIV.
Workup and Screening
Screening for eating disorders should be incorporated into routine psychosocial assessments, especially in adolescents. Patients may minimize symptoms; therefore, collateral history from parents or caregivers is essential. The SCOFF questionnaire is a useful screening tool, with high sensitivity for anorexia and bulimia when two or more responses are positive. Baseline electrocardiography is recommended for all patients to assess for QT interval prolongation, which is associated with increased risk of sudden cardiac death. A dual-energy x-ray absorptiometry (DEXA) scan should be considered after six months of amenorrhea to evaluate for osteopenia or osteoporosis.
Laboratory Findings
Laboratory results may be normal in mild cases. Common abnormalities include endocrine changes such as decreased gonadotropins, estrogens, and thyroid hormones, with normal thyroid-stimulating hormone and elevated cortisol. Hematologic abnormalities may include leukopenia, anemia, thrombocytopenia, and reduced inflammatory markers. Electrolyte disturbances such as hypokalemia, hypomagnesemia, hypocalcemia, hypophosphatemia, metabolic alkalosis, and hypercholesterolemia may occur. Elevated plasma beta-carotene levels can help distinguish anorexia nervosa from other causes of starvation.
Treatment and Nonpharmacologic Management
Management requires a multidisciplinary approach involving medical, nutritional, and psychological care. A target weight should be established, aiming for 100% of ideal body weight in adolescents and 90% to 100% in adults. Weight restoration should proceed gradually, with initial caloric intake of 800 to 1200 kcal per day in small, frequent meals, advancing to 1500 to 3000 kcal as tolerated. Electrolytes must be monitored closely to prevent refeeding syndrome. In severe cases, enteral or parenteral nutrition may be necessary. Mealtimes should emphasize support rather than confrontation, and post-meal supervision may be required to prevent purging or excessive exercise.
Acute Management and Severity Assessment
Severity is categorized by body mass index in adults or BMI percentile in children and adolescents. Mild disease corresponds to a BMI of 17 kg/m² or higher, moderate disease to BMI 16–16.99, severe disease to BMI 15–15.99, and extreme disease to BMI below 15. Most patients can be managed as outpatients; however, inpatient care is indicated for medical instability, severe electrolyte disturbances, significant bradycardia or hypotension, prolonged QT interval, rapid weight loss, failure of outpatient treatment, or suicidal ideation. Pharmacologic therapy generally has limited benefit unless comorbid depression, anxiety, or obsessive-compulsive symptoms are present.
Chronic Management and Psychotherapy
Long-term psychotherapy is central to recovery and may need to continue for years. Treatment focuses on body image, self-esteem, interpersonal relationships, and relapse prevention. Family-based therapy is particularly effective in children and adolescents and is strongly recommended.
Disposition and Prognosis
The long-term prognosis of anorexia nervosa is guarded, with many patients experiencing relapses or persistent disordered eating and body image distortion. Menstrual function typically returns within six months of achieving 90% of ideal body weight, although pregnancy can occur even in the presence of amenorrhea. Mortality rates range from 5% to 20%, significantly higher than in age-matched peers, with common causes including electrolyte imbalance, starvation, and suicide. Favorable prognostic factors include early diagnosis, prompt treatment initiation, strong family support, and positive therapeutic relationships.
Referral and Indications for Hospitalization
Hospitalization should be considered for severe dehydration, electrolyte abnormalities, cardiac arrhythmias, significant physiologic instability, intractable purging, suicidal thoughts, weight loss exceeding 30% of ideal body weight, rapid ongoing weight loss, or failure of outpatient nutritional rehabilitation. Early involvement of mental health specialists is essential to optimize outcomes.


- Published on
KembaraXtra-Medicine- Anorectal Stricture
Basic Information and Definition
An anorectal stricture, also referred to as anal stenosis, is an abnormal narrowing of the anal canal. Strictures are classified according to both severity and location. Severity ranges from mild, in which a well-lubricated finger or medium Hill-Ferguson retractor can pass easily, to moderate, where passage is possible only with forceful dilation, and severe, where no passage is possible. Location is described as low (at least 0.5 cm distal to the dentate line), middle (within 0.5 cm on either side of the dentate line), or high (at least 0.5 cm proximal to the dentate line).
Synonyms and Coding
Anorectal stricture is also known as anal stenosis or Küss disease. The ICD-10-CM code used is K62.4, which denotes stenosis of the anus and rectum.
Epidemiology and Risk Factors
Hemorrhoid surgery is the most common overall cause of anorectal stricture, occurring in approximately 5% to 10% of patients after radical hemorrhoidectomy, particularly for grade III and IV hemorrhoidal disease. The risk of developing a stricture is directly related to the extent of anoderm resection. Other important risk factors include prior anorectal surgery, inflammatory bowel disease, previous pelvic radiation, and chronic hemorrhoidal disease.
Physical Findings and Clinical Presentation
Pain with defecation is the most common presenting symptom. Patients may also report rectal bleeding, narrowing of stools, severe constipation, outlet obstruction, fecal incontinence, tenesmus, or urgency. A careful history should assess prior anorectal surgery, Crohn disease, radiation exposure, or perianal trauma. On physical examination, visual inspection may reveal skin tags or chronic fissures. Digital rectal examination typically demonstrates a narrowed anal canal with difficulty passing a lubricated finger. In severe cases, examination under anesthesia may be required to adequately assess the stricture.
Etiology
Anorectal strictures are broadly divided into congenital, primary, and secondary causes. Congenital strictures are pediatric conditions related to abnormal embryologic development, including anal atresia and imperforate anus. Primary strictures usually occur in elderly patients due to fibrous involution of perianal tissues. Secondary strictures are the most common and are typically iatrogenic, most often following hemorrhoidectomy or other anorectal surgeries such as low anterior resection, ileal pouch–anal anastomosis, anopexy, or excision of perianal skin lesions. Other secondary causes include fibrosis of the anoderm or distal rectal mucosa, anal canal muscle hypertrophy or spasm, neoplastic conditions (such as Bowen disease, Paget disease, anal squamous cell carcinoma, rectal adenocarcinoma, or condyloma acuminata), inflammatory diseases (including anal fissure, Crohn disease, tuberculosis, actinomycosis, lymphogranuloma venereum, and chronic suppuration), traumatic causes (radiation therapy, perineal burns, hot water enemas, ibuprofen suppositories, and chronic laxative abuse), and sexually transmitted infections.
Diagnosis and Differential Diagnosis
Anorectal stricture is primarily a clinical diagnosis. The differential diagnosis includes anorectal or rectal neoplasm, inflammatory bowel disease, and traumatic injury. Any suspicious lesions identified during examination should be biopsied to exclude malignancy or inflammatory pathology.
Workup
Although the diagnosis is clinical, evaluation should ensure that secondary causes such as neoplasm or inflammatory disease are excluded. Regardless of etiology, hydration, fiber supplementation, and stool softeners should be initiated in all patients to reduce symptoms and prevent further injury.
Treatment
Management depends on severity and underlying cause. Nonpharmacologic therapy includes manual dilation using digital techniques or commercial dilators, which may be initiated in the clinic or operating room and continued on an outpatient basis for mild to moderate strictures. Surgical options include resection of neoplasm, stricturoplasty, or anoplasty. While multiple operative techniques have been described, there is no consensus on a single superior approach; all aim to replace scar tissue with healthy, pliable anoderm within the anal canal.
Chronic Management
For mild disease, conservative measures such as stool softeners, fiber supplementation, adequate hydration, and dietary modification may be sufficient to control symptoms without the need for procedural intervention.
Prevention and Complementary Considerations
The most effective management of postsurgical anorectal stricture is prevention. Proper surgical technique during anorectal procedures, including preservation of anoderm and, in some cases, internal sphincterotomy, can significantly reduce the risk of developing stenosis.
Disposition and Referral
Mild strictures can usually be managed on an outpatient basis. Moderate to severe strictures require evaluation by a colorectal surgeon. Referral is also indicated when there is concern for neoplasm, failure of conservative management, or inability of the clinician to pass a lubricated finger into the rectum during examination.
Basic Information and Definition
An anorectal stricture, also referred to as anal stenosis, is an abnormal narrowing of the anal canal. Strictures are classified according to both severity and location. Severity ranges from mild, in which a well-lubricated finger or medium Hill-Ferguson retractor can pass easily, to moderate, where passage is possible only with forceful dilation, and severe, where no passage is possible. Location is described as low (at least 0.5 cm distal to the dentate line), middle (within 0.5 cm on either side of the dentate line), or high (at least 0.5 cm proximal to the dentate line).
Synonyms and Coding
Anorectal stricture is also known as anal stenosis or Küss disease. The ICD-10-CM code used is K62.4, which denotes stenosis of the anus and rectum.
Epidemiology and Risk Factors
Hemorrhoid surgery is the most common overall cause of anorectal stricture, occurring in approximately 5% to 10% of patients after radical hemorrhoidectomy, particularly for grade III and IV hemorrhoidal disease. The risk of developing a stricture is directly related to the extent of anoderm resection. Other important risk factors include prior anorectal surgery, inflammatory bowel disease, previous pelvic radiation, and chronic hemorrhoidal disease.
Physical Findings and Clinical Presentation
Pain with defecation is the most common presenting symptom. Patients may also report rectal bleeding, narrowing of stools, severe constipation, outlet obstruction, fecal incontinence, tenesmus, or urgency. A careful history should assess prior anorectal surgery, Crohn disease, radiation exposure, or perianal trauma. On physical examination, visual inspection may reveal skin tags or chronic fissures. Digital rectal examination typically demonstrates a narrowed anal canal with difficulty passing a lubricated finger. In severe cases, examination under anesthesia may be required to adequately assess the stricture.
Etiology
Anorectal strictures are broadly divided into congenital, primary, and secondary causes. Congenital strictures are pediatric conditions related to abnormal embryologic development, including anal atresia and imperforate anus. Primary strictures usually occur in elderly patients due to fibrous involution of perianal tissues. Secondary strictures are the most common and are typically iatrogenic, most often following hemorrhoidectomy or other anorectal surgeries such as low anterior resection, ileal pouch–anal anastomosis, anopexy, or excision of perianal skin lesions. Other secondary causes include fibrosis of the anoderm or distal rectal mucosa, anal canal muscle hypertrophy or spasm, neoplastic conditions (such as Bowen disease, Paget disease, anal squamous cell carcinoma, rectal adenocarcinoma, or condyloma acuminata), inflammatory diseases (including anal fissure, Crohn disease, tuberculosis, actinomycosis, lymphogranuloma venereum, and chronic suppuration), traumatic causes (radiation therapy, perineal burns, hot water enemas, ibuprofen suppositories, and chronic laxative abuse), and sexually transmitted infections.
Diagnosis and Differential Diagnosis
Anorectal stricture is primarily a clinical diagnosis. The differential diagnosis includes anorectal or rectal neoplasm, inflammatory bowel disease, and traumatic injury. Any suspicious lesions identified during examination should be biopsied to exclude malignancy or inflammatory pathology.
Workup
Although the diagnosis is clinical, evaluation should ensure that secondary causes such as neoplasm or inflammatory disease are excluded. Regardless of etiology, hydration, fiber supplementation, and stool softeners should be initiated in all patients to reduce symptoms and prevent further injury.
Treatment
Management depends on severity and underlying cause. Nonpharmacologic therapy includes manual dilation using digital techniques or commercial dilators, which may be initiated in the clinic or operating room and continued on an outpatient basis for mild to moderate strictures. Surgical options include resection of neoplasm, stricturoplasty, or anoplasty. While multiple operative techniques have been described, there is no consensus on a single superior approach; all aim to replace scar tissue with healthy, pliable anoderm within the anal canal.
Chronic Management
For mild disease, conservative measures such as stool softeners, fiber supplementation, adequate hydration, and dietary modification may be sufficient to control symptoms without the need for procedural intervention.
Prevention and Complementary Considerations
The most effective management of postsurgical anorectal stricture is prevention. Proper surgical technique during anorectal procedures, including preservation of anoderm and, in some cases, internal sphincterotomy, can significantly reduce the risk of developing stenosis.
Disposition and Referral
Mild strictures can usually be managed on an outpatient basis. Moderate to severe strictures require evaluation by a colorectal surgeon. Referral is also indicated when there is concern for neoplasm, failure of conservative management, or inability of the clinician to pass a lubricated finger into the rectum during examination.


- Published on
KembaraXtra-Medicine- Anorectal Fistula
Basic Information and Definition
An anorectal fistula is an inflammatory tract that connects the anal canal to the perianal skin. It has a primary (internal) opening in the anal canal at the dentate line and a secondary (external) opening on the perianal skin. Most fistulae develop as a complication of a perianal abscess that begins with infection of an anal crypt gland; if the abscess ruptures and the tract becomes epithelialized, a chronic fistula forms.
Classification by Relationship to the Anal Sphincter Complex
Intersphincteric fistulas are the most common and travel within the intersphincteric plane to the perianal skin. Transsphincteric fistulas are frequent and pass from the internal opening through both internal and external sphincters into the ischiorectal fossa and then to the perianal skin. Suprasphincteric fistulas are uncommon; after traversing the internal sphincter, the tract courses above the puborectalis and then descends lateral to the external sphincter into the ischiorectal space, sometimes associated with a supralevator abscess if the cavity extends upward. Extrasphincteric fistulas are rare and pass from the rectum above the levators, through the levator muscles, and into the ischiorectal space and perianal skin. Submucosal fistulas originate at the dentate line from an infected crypt without involving the sphincter muscles. Horseshoe fistulas extend from one ischiorectal fossa to the other behind the rectum. (Fistulotomy is not appropriate for extrasphincteric fistulas because of the high risk of incontinence.)
Synonyms
Fistula-in-ano and anal fistula.
ICD-10-CM Codes
K60.5 (Anorectal fistula) and K60.3 (Anal fistula).
Epidemiology and Demographics
Anorectal fistulas occur across all ages, with an average age around 39 years. They are about twice as common in men as in women. They are associated with inflammatory bowel disease and constipation. In pediatrics, they are more common in infants, with boys affected more than girls.
Physical Findings and Clinical Presentation
In the acute stage, patients may have perianal swelling, pain with defecation and sitting, and fever. In the chronic stage, symptoms include persistent pain, malodorous perianal drainage or bleeding, and anal pruritus. The external opening is often tender and inflamed, typically within 2–3 cm of the anal verge, and may express purulent or serosanguineous drainage with compression. A greater distance from the anal margin increases the likelihood of a more complex fistula with upward extension. Recurrent perianal abscess strongly suggests an underlying fistula.
Goodsall Rule
The likely course of the fistula tract can often be estimated from the external opening location. If the external opening is anterior to an imaginary transverse line through the midpoint of the anus, the tract usually runs radially to the anal canal. If the opening is posterior to that line, the tract is usually curved and enters the anal canal at the posterior midline. An important exception is an anterior external opening more than 3 cm from the anus, which may still curve posteriorly and open in the posterior midline.
Etiology
The most common cause is a nonspecific infection of an anal crypt gland involving skin or intestinal flora, and fistulas are more likely when intestinal microorganisms are cultured from the initial abscess. Other infectious causes include tuberculosis, lymphogranuloma venereum, and actinomycosis. Inflammatory bowel disease (especially Crohn disease, and less commonly ulcerative colitis) is an important cause. Trauma can lead to fistulas, including after surgery (e.g., episiotomy, prostatectomy), foreign bodies, or anal intercourse. Malignancy (carcinoma, leukemia, lymphoma) and malignancy treatment (surgery, radiation) can also cause fistula formation.
Diagnosis
Diagnosis is commonly established by history and physical examination, especially in simple fistulas, supported by anoscopy and/or further evaluation when needed.
Differential Diagnosis
Anal abscess, anal ulcer or fissure, hidradenitis suppurativa, pilonidal sinus, Bartholin gland abscess or sinus, and infected perianal sebaceous cysts.
Workup
Digital rectal examination is performed to assess sphincter tone and voluntary squeeze pressure, detect an extraluminal mass, identify an indurated tract, and attempt to palpate an internal opening or pit. Gentle probing of the external opening may be performed but should be done carefully to avoid creating a false tract; about half of patients may not have a clinically detectable internal opening. Exam alone may be sufficient for many simple fistulas. Anoscopy is used to evaluate the anal canal. Proctosigmoidoscopy is recommended to exclude inflammatory or neoplastic disease. When extensive evaluation or procedures are required, studies should be done under adequate anesthesia.
Laboratory Tests
A complete blood count may be obtained. Rectal biopsy is appropriate if inflammatory bowel disease or malignancy is suspected; biopsy of the external orifice is not useful.
Imaging Studies
Transanal endosonography (EUS) can help estimate how much sphincter would be divided during fistulotomy and can detect undrained sepsis, complex anatomy, and high blind tracts. MRI is useful for identifying suprasphincteric or extrasphincteric tracts, and MRI/EUS are generally more accurate than clinical exam in mapping fistula anatomy. CT is limited because it lacks the resolution to define tract relationships to sphincters and levators. Fistulography is rarely needed now. Colonoscopy or barium enema should be considered when IBD or malignancy is suspected, when fistulas are recurrent or multiple, or in patients younger than 25 years. A small bowel series may occasionally be obtained for similar indications.
Treatment: Nonpharmacologic
Sitz baths can provide symptomatic relief and improve comfort.
Pharmacologic Therapy
Medications are rarely recommended as primary therapy. Immunomodulators such as infliximab may be used in selected cases, particularly when fistulas are related to Crohn disease.
Acute General Management
Surgery is the treatment of choice. Broad-spectrum antibiotics are used when cellulitis is present, when the patient is immunocompromised, or when valvular heart disease or prosthetic devices are present. Stool softeners or laxatives may be used to reduce straining and discomfort.
Chronic Management and Surgical Options
Definitive management is typically surgical, tailored to fistula type and complexity. The main goals are to eradicate the fistula, prevent recurrence, preserve sphincter function, and minimize healing time. Surgical and procedural options include fistulotomy, fistulectomy, seton placement (to maintain drainage while healing occurs), fibrin glue, fistula plugs, LIFT procedure (ligation of the intersphincteric fistula tract), rectal advancement flaps, and, in select complex situations, colostomy. Strategy varies by classification; superficial/intersphincteric and low transsphincteric fistulas are often candidates for fistulotomy, while higher or more complex fistulas more often require sphincter-sparing approaches such as setons, LIFT, advancement flaps, glue, or plugs. Extrasphincteric disease requires addressing any intraabdominal or pelvic source and is not managed with fistulotomy due to incontinence risk.
Disposition
Most patients are managed with outpatient surgery.
Referral
Referral to a surgeon experienced in anorectal fistula management is recommended.
Pearls and Considerations
HIV-positive and diabetic patients who develop perirectal abscesses or fistulas should be treated as true surgical emergencies. The risk of septicemia, Fournier gangrene, and other severe septic complications makes rapid evaluation and drainage imperative.
Basic Information and Definition
An anorectal fistula is an inflammatory tract that connects the anal canal to the perianal skin. It has a primary (internal) opening in the anal canal at the dentate line and a secondary (external) opening on the perianal skin. Most fistulae develop as a complication of a perianal abscess that begins with infection of an anal crypt gland; if the abscess ruptures and the tract becomes epithelialized, a chronic fistula forms.
Classification by Relationship to the Anal Sphincter Complex
Intersphincteric fistulas are the most common and travel within the intersphincteric plane to the perianal skin. Transsphincteric fistulas are frequent and pass from the internal opening through both internal and external sphincters into the ischiorectal fossa and then to the perianal skin. Suprasphincteric fistulas are uncommon; after traversing the internal sphincter, the tract courses above the puborectalis and then descends lateral to the external sphincter into the ischiorectal space, sometimes associated with a supralevator abscess if the cavity extends upward. Extrasphincteric fistulas are rare and pass from the rectum above the levators, through the levator muscles, and into the ischiorectal space and perianal skin. Submucosal fistulas originate at the dentate line from an infected crypt without involving the sphincter muscles. Horseshoe fistulas extend from one ischiorectal fossa to the other behind the rectum. (Fistulotomy is not appropriate for extrasphincteric fistulas because of the high risk of incontinence.)
Synonyms
Fistula-in-ano and anal fistula.
ICD-10-CM Codes
K60.5 (Anorectal fistula) and K60.3 (Anal fistula).
Epidemiology and Demographics
Anorectal fistulas occur across all ages, with an average age around 39 years. They are about twice as common in men as in women. They are associated with inflammatory bowel disease and constipation. In pediatrics, they are more common in infants, with boys affected more than girls.
Physical Findings and Clinical Presentation
In the acute stage, patients may have perianal swelling, pain with defecation and sitting, and fever. In the chronic stage, symptoms include persistent pain, malodorous perianal drainage or bleeding, and anal pruritus. The external opening is often tender and inflamed, typically within 2–3 cm of the anal verge, and may express purulent or serosanguineous drainage with compression. A greater distance from the anal margin increases the likelihood of a more complex fistula with upward extension. Recurrent perianal abscess strongly suggests an underlying fistula.
Goodsall Rule
The likely course of the fistula tract can often be estimated from the external opening location. If the external opening is anterior to an imaginary transverse line through the midpoint of the anus, the tract usually runs radially to the anal canal. If the opening is posterior to that line, the tract is usually curved and enters the anal canal at the posterior midline. An important exception is an anterior external opening more than 3 cm from the anus, which may still curve posteriorly and open in the posterior midline.
Etiology
The most common cause is a nonspecific infection of an anal crypt gland involving skin or intestinal flora, and fistulas are more likely when intestinal microorganisms are cultured from the initial abscess. Other infectious causes include tuberculosis, lymphogranuloma venereum, and actinomycosis. Inflammatory bowel disease (especially Crohn disease, and less commonly ulcerative colitis) is an important cause. Trauma can lead to fistulas, including after surgery (e.g., episiotomy, prostatectomy), foreign bodies, or anal intercourse. Malignancy (carcinoma, leukemia, lymphoma) and malignancy treatment (surgery, radiation) can also cause fistula formation.
Diagnosis
Diagnosis is commonly established by history and physical examination, especially in simple fistulas, supported by anoscopy and/or further evaluation when needed.
Differential Diagnosis
Anal abscess, anal ulcer or fissure, hidradenitis suppurativa, pilonidal sinus, Bartholin gland abscess or sinus, and infected perianal sebaceous cysts.
Workup
Digital rectal examination is performed to assess sphincter tone and voluntary squeeze pressure, detect an extraluminal mass, identify an indurated tract, and attempt to palpate an internal opening or pit. Gentle probing of the external opening may be performed but should be done carefully to avoid creating a false tract; about half of patients may not have a clinically detectable internal opening. Exam alone may be sufficient for many simple fistulas. Anoscopy is used to evaluate the anal canal. Proctosigmoidoscopy is recommended to exclude inflammatory or neoplastic disease. When extensive evaluation or procedures are required, studies should be done under adequate anesthesia.
Laboratory Tests
A complete blood count may be obtained. Rectal biopsy is appropriate if inflammatory bowel disease or malignancy is suspected; biopsy of the external orifice is not useful.
Imaging Studies
Transanal endosonography (EUS) can help estimate how much sphincter would be divided during fistulotomy and can detect undrained sepsis, complex anatomy, and high blind tracts. MRI is useful for identifying suprasphincteric or extrasphincteric tracts, and MRI/EUS are generally more accurate than clinical exam in mapping fistula anatomy. CT is limited because it lacks the resolution to define tract relationships to sphincters and levators. Fistulography is rarely needed now. Colonoscopy or barium enema should be considered when IBD or malignancy is suspected, when fistulas are recurrent or multiple, or in patients younger than 25 years. A small bowel series may occasionally be obtained for similar indications.
Treatment: Nonpharmacologic
Sitz baths can provide symptomatic relief and improve comfort.
Pharmacologic Therapy
Medications are rarely recommended as primary therapy. Immunomodulators such as infliximab may be used in selected cases, particularly when fistulas are related to Crohn disease.
Acute General Management
Surgery is the treatment of choice. Broad-spectrum antibiotics are used when cellulitis is present, when the patient is immunocompromised, or when valvular heart disease or prosthetic devices are present. Stool softeners or laxatives may be used to reduce straining and discomfort.
Chronic Management and Surgical Options
Definitive management is typically surgical, tailored to fistula type and complexity. The main goals are to eradicate the fistula, prevent recurrence, preserve sphincter function, and minimize healing time. Surgical and procedural options include fistulotomy, fistulectomy, seton placement (to maintain drainage while healing occurs), fibrin glue, fistula plugs, LIFT procedure (ligation of the intersphincteric fistula tract), rectal advancement flaps, and, in select complex situations, colostomy. Strategy varies by classification; superficial/intersphincteric and low transsphincteric fistulas are often candidates for fistulotomy, while higher or more complex fistulas more often require sphincter-sparing approaches such as setons, LIFT, advancement flaps, glue, or plugs. Extrasphincteric disease requires addressing any intraabdominal or pelvic source and is not managed with fistulotomy due to incontinence risk.
Disposition
Most patients are managed with outpatient surgery.
Referral
Referral to a surgeon experienced in anorectal fistula management is recommended.
Pearls and Considerations
HIV-positive and diabetic patients who develop perirectal abscesses or fistulas should be treated as true surgical emergencies. The risk of septicemia, Fournier gangrene, and other severe septic complications makes rapid evaluation and drainage imperative.


- Published on
KembaraXtra-Medicine- Ankylosing Spondylitis
Basic Information and Definition
Ankylosing spondylitis (AS) is a chronic inflammatory arthritis that primarily affects the sacroiliac joints and axial skeleton. It is characterized by ankylosis, which is abnormal joint stiffening, and enthesitis, inflammation at tendon and ligament insertion sites. Ankylosing spondylitis belongs to the family of seronegative spondyloarthropathies, which also includes reactive arthritis, psoriatic spondylitis, and enteropathic arthritis.
Synonyms
Ankylosing spondylitis is also known as Marie-Strümpell disease and Bechterew disease.
ICD-10-CM Codes
Ankylosing spondylitis is coded according to the region of spinal involvement, including unspecified spinal sites, juvenile ankylosing spondylitis, and specific cervical, thoracic, lumbar, lumbosacral, sacral, and occipito-atlanto-axial regions.
Epidemiology and Demographics
The prevalence of ankylosing spondylitis ranges from 0.1% to 1% of the general population and varies by ethnicity and the prevalence of the HLA-B27 allele. In populations with HLA-B27 positivity, prevalence is significantly higher, especially among individuals with a family history of spondyloarthropathy. The disease predominantly affects males, with approximately 70% of cases occurring in men. Symptoms typically begin between ages 15 and 35, and most patients develop symptoms before age 45.
Physical Findings and Clinical Presentation
Patients commonly present with chronic inflammatory back pain of insidious onset lasting longer than three months. Morning stiffness lasting at least 30 minutes is typical and improves with physical activity but worsens with rest. Bilateral sacroiliac joint tenderness is common, along with limited lumbar spine mobility. Enthesitis frequently affects the Achilles tendon and plantar fascia. Reduced chest expansion may occur due to costovertebral joint involvement. Peripheral arthritis, usually asymmetric and affecting the lower extremities, may be present. In advanced disease, patients may develop a characteristic posture with loss of lumbar lordosis, fixed hip flexion, knee flexion, and compensatory hyperextension of the neck. Extra-articular manifestations include acute anterior uveitis or iritis, seen in up to 40% of patients, as well as cardiovascular involvement such as aortic insufficiency, pulmonary fibrosis, and increased risk of osteoporosis.
Inflammatory Back Pain Characteristics
Inflammatory back pain in ankylosing spondylitis typically begins before age 45, persists for more than three months, and is localized to the lower back with possible alternating buttock pain. Symptoms often awaken patients during the second half of the night and improve with exercise or nonsteroidal anti-inflammatory drugs, but not with rest.
Etiology and Pathogenesis
The exact cause of ankylosing spondylitis remains incompletely understood. Genetic susceptibility plays a major role, with HLA-B27 being the strongest known predisposing factor. Immune dysregulation, environmental triggers, infections such as Klebsiella pneumoniae, and hormonal influences may contribute to disease development. Tumor necrosis factor (TNF) and other inflammatory cytokines are central mediators of the inflammatory process.
Diagnosis
Diagnosis is based on clinical features, laboratory findings, and imaging. Demonstration of inflammatory sacroiliitis on imaging is diagnostic in most patients, although some meet criteria for nonradiographic axial spondyloarthritis. Elevated erythrocyte sedimentation rate and C-reactive protein may be present, along with mild anemia. HLA-B27 testing supports the diagnosis in appropriate clinical contexts but is not diagnostic on its own, as it is present in a proportion of the healthy population.
Differential Diagnosis
The differential diagnosis includes diffuse idiopathic skeletal hyperostosis, mechanical or noninflammatory back pain, and other inflammatory spondyloarthropathies such as psoriatic arthritis, reactive arthritis, and enteropathic arthritis.
Imaging Studies
Pelvic radiographs classically demonstrate bilateral sacroiliitis and are part of the modified New York criteria. As disease progresses, vertebral bodies lose their normal concavity and become squared, with calcification of spinal ligaments leading to the characteristic bamboo spine appearance. Advanced disease may show diskovertebral erosions known as Andersson lesions. MRI is particularly useful in early disease and can detect active inflammation, bone marrow edema, erosions, and sacroiliitis before changes are visible on plain radiographs.
Nonpharmacologic Treatment
Regular exercise is a cornerstone of management, with emphasis on maintaining spinal mobility, posture, and aerobic fitness. Patients should be instructed in spinal extension and postural exercises to prevent flexion deformities. Sleeping supine on a firm mattress without pillows under the head or knees is recommended. Breathing exercises help preserve chest expansion.
Pharmacologic Therapy
Continuous full-dose NSAIDs are first-line therapy and are effective in controlling pain and stiffness; indomethacin may be particularly effective in some patients. Sulfasalazine may benefit patients with significant peripheral arthritis. Biologic therapies targeting TNF, such as etanercept, infliximab, and adalimumab, are highly effective for patients with inadequate response to NSAIDs and improve symptoms, spinal mobility, and quality of life. Etanercept is generally avoided in patients with recurrent uveitis. Interleukin-17 inhibitors, including secukinumab and ixekizumab, are approved alternatives for active disease.
Disposition and Prognosis
Most patients with ankylosing spondylitis have a normal life expectancy; however, many experience progressive loss of spinal mobility and functional impairment. Early diagnosis and appropriate therapy significantly improve long-term outcomes.
Referral
All patients with suspected or confirmed ankylosing spondylitis should be referred to a rheumatologist for comprehensive evaluation and long-term management.
Pearls and Considerations
A positive family history increases the diagnostic value of HLA-B27 testing. Selected patients with severe spinal deformities may benefit from corrective osteotomy. Emerging evidence suggests an increased risk of cardiovascular and vascular mortality, particularly in men with longstanding disease.
Basic Information and Definition
Ankylosing spondylitis (AS) is a chronic inflammatory arthritis that primarily affects the sacroiliac joints and axial skeleton. It is characterized by ankylosis, which is abnormal joint stiffening, and enthesitis, inflammation at tendon and ligament insertion sites. Ankylosing spondylitis belongs to the family of seronegative spondyloarthropathies, which also includes reactive arthritis, psoriatic spondylitis, and enteropathic arthritis.
Synonyms
Ankylosing spondylitis is also known as Marie-Strümpell disease and Bechterew disease.
ICD-10-CM Codes
Ankylosing spondylitis is coded according to the region of spinal involvement, including unspecified spinal sites, juvenile ankylosing spondylitis, and specific cervical, thoracic, lumbar, lumbosacral, sacral, and occipito-atlanto-axial regions.
Epidemiology and Demographics
The prevalence of ankylosing spondylitis ranges from 0.1% to 1% of the general population and varies by ethnicity and the prevalence of the HLA-B27 allele. In populations with HLA-B27 positivity, prevalence is significantly higher, especially among individuals with a family history of spondyloarthropathy. The disease predominantly affects males, with approximately 70% of cases occurring in men. Symptoms typically begin between ages 15 and 35, and most patients develop symptoms before age 45.
Physical Findings and Clinical Presentation
Patients commonly present with chronic inflammatory back pain of insidious onset lasting longer than three months. Morning stiffness lasting at least 30 minutes is typical and improves with physical activity but worsens with rest. Bilateral sacroiliac joint tenderness is common, along with limited lumbar spine mobility. Enthesitis frequently affects the Achilles tendon and plantar fascia. Reduced chest expansion may occur due to costovertebral joint involvement. Peripheral arthritis, usually asymmetric and affecting the lower extremities, may be present. In advanced disease, patients may develop a characteristic posture with loss of lumbar lordosis, fixed hip flexion, knee flexion, and compensatory hyperextension of the neck. Extra-articular manifestations include acute anterior uveitis or iritis, seen in up to 40% of patients, as well as cardiovascular involvement such as aortic insufficiency, pulmonary fibrosis, and increased risk of osteoporosis.
Inflammatory Back Pain Characteristics
Inflammatory back pain in ankylosing spondylitis typically begins before age 45, persists for more than three months, and is localized to the lower back with possible alternating buttock pain. Symptoms often awaken patients during the second half of the night and improve with exercise or nonsteroidal anti-inflammatory drugs, but not with rest.
Etiology and Pathogenesis
The exact cause of ankylosing spondylitis remains incompletely understood. Genetic susceptibility plays a major role, with HLA-B27 being the strongest known predisposing factor. Immune dysregulation, environmental triggers, infections such as Klebsiella pneumoniae, and hormonal influences may contribute to disease development. Tumor necrosis factor (TNF) and other inflammatory cytokines are central mediators of the inflammatory process.
Diagnosis
Diagnosis is based on clinical features, laboratory findings, and imaging. Demonstration of inflammatory sacroiliitis on imaging is diagnostic in most patients, although some meet criteria for nonradiographic axial spondyloarthritis. Elevated erythrocyte sedimentation rate and C-reactive protein may be present, along with mild anemia. HLA-B27 testing supports the diagnosis in appropriate clinical contexts but is not diagnostic on its own, as it is present in a proportion of the healthy population.
Differential Diagnosis
The differential diagnosis includes diffuse idiopathic skeletal hyperostosis, mechanical or noninflammatory back pain, and other inflammatory spondyloarthropathies such as psoriatic arthritis, reactive arthritis, and enteropathic arthritis.
Imaging Studies
Pelvic radiographs classically demonstrate bilateral sacroiliitis and are part of the modified New York criteria. As disease progresses, vertebral bodies lose their normal concavity and become squared, with calcification of spinal ligaments leading to the characteristic bamboo spine appearance. Advanced disease may show diskovertebral erosions known as Andersson lesions. MRI is particularly useful in early disease and can detect active inflammation, bone marrow edema, erosions, and sacroiliitis before changes are visible on plain radiographs.
Nonpharmacologic Treatment
Regular exercise is a cornerstone of management, with emphasis on maintaining spinal mobility, posture, and aerobic fitness. Patients should be instructed in spinal extension and postural exercises to prevent flexion deformities. Sleeping supine on a firm mattress without pillows under the head or knees is recommended. Breathing exercises help preserve chest expansion.
Pharmacologic Therapy
Continuous full-dose NSAIDs are first-line therapy and are effective in controlling pain and stiffness; indomethacin may be particularly effective in some patients. Sulfasalazine may benefit patients with significant peripheral arthritis. Biologic therapies targeting TNF, such as etanercept, infliximab, and adalimumab, are highly effective for patients with inadequate response to NSAIDs and improve symptoms, spinal mobility, and quality of life. Etanercept is generally avoided in patients with recurrent uveitis. Interleukin-17 inhibitors, including secukinumab and ixekizumab, are approved alternatives for active disease.
Disposition and Prognosis
Most patients with ankylosing spondylitis have a normal life expectancy; however, many experience progressive loss of spinal mobility and functional impairment. Early diagnosis and appropriate therapy significantly improve long-term outcomes.
Referral
All patients with suspected or confirmed ankylosing spondylitis should be referred to a rheumatologist for comprehensive evaluation and long-term management.
Pearls and Considerations
A positive family history increases the diagnostic value of HLA-B27 testing. Selected patients with severe spinal deformities may benefit from corrective osteotomy. Emerging evidence suggests an increased risk of cardiovascular and vascular mortality, particularly in men with longstanding disease.


- Published on
KembaraXtra-Medicine – ANCA-Associated Vasculitis
Basic Information Anti-neutrophil cytoplasmic antibody (ANCA)–associated vasculitis (AAV) is a group of small- to medium-vessel systemic vasculitides that includes granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA). These conditions share overlapping clinical manifestations and treatment strategies but differ in pathology and organ involvement. They are characterized by necrotizing, pauci-immune small-vessel vasculitis, with granulomatous inflammation present in GPA but absent in MPA. Most patients present with renal and pulmonary involvement, although the skin, nervous system, and gastrointestinal tract may also be affected. A limited form of GPA may be confined to the upper respiratory tract and can often be managed less aggressively.
Synonyms ANCA-associated vasculitis, ANCA-positive vasculitis, granulomatosis with polyangiitis (GPA), Wegener granulomatosis, microscopic polyangiitis (MPA), eosinophilic granulomatosis with polyangiitis (EGPA).
ICD-10-CM Codes I77.6 arteritis unspecified; M31.3 granulomatosis with polyangiitis; M31.7 microscopic polyangiitis; M30.1 eosinophilic granulomatosis with polyangiitis.
Epidemiology and Demographics The incidence is approximately 6–12 cases per million persons per year in Western Europe and Japan, with global variation. Prevalence ranges from 94 to 160 per million. There is a slight male predominance, and incidence increases with age, peaking between 60 and 70 years.
Risk Factors and Genetics Risk factors include infections such as Staphylococcus aureus, silica and hydrocarbon exposure, cigarette smoking, pesticides, and medications including hydralazine, minocycline, propylthiouracil, levamisole-adulterated cocaine, and allopurinol. Familial disease is rare. GPA is associated with SNPs in HLA-DP, PRTN3, and SERPINA1, whereas MPA is associated with HLA-DQ polymorphisms.
Physical Findings and Clinical Presentation Patients commonly have constitutional symptoms such as fever, fatigue, weight loss, myalgia, and arthralgia. Upper respiratory tract disease is prominent in GPA and includes chronic sinusitis, otitis media, mastoiditis, nasal crusting and epistaxis, septal perforation, subglottic or tracheal stenosis, and saddle-nose deformity. Ocular involvement includes conjunctivitis, episcleritis, scleritis, uveitis, optic neuropathy, and retinal vasculitis. Ear findings include sensorineural or conductive hearing loss and otorrhea. Oral findings may include chronic ulcerative lesions and “mulberry” gingivitis. Pulmonary disease presents with dyspnea, hemoptysis, pleuritic chest pain, nodules, cavitary lesions, infiltrates, effusions, or diffuse alveolar hemorrhage. Gastrointestinal involvement, more common in MPA, includes ischemic abdominal pain, bleeding, ulceration, or perforation. Renal disease is common in GPA and MPA and manifests as hypertension, edema, reduced urine output, rapidly progressive glomerulonephritis, microscopic hematuria, red cell casts, and proteinuria. Neurologic involvement includes mononeuritis multiplex, peripheral neuropathy, pachymeningitis, headaches, and rarely central nervous system disease. Cutaneous findings include palpable purpura, necrotic ulcers, nodules, urticaria, livedo reticularis, and digital gangrene.
Etiology The etiology is immune mediated and multifactorial. ANCAs directed against proteinase 3 (PR3) or myeloperoxidase (MPO) activate neutrophils, causing endothelial injury and tissue necrosis. Genetic susceptibility and environmental triggers contribute to disease development.
Diagnosis and Differential Diagnosis
Diagnosis is based on compatible clinical features supported by laboratory testing, imaging, and histopathology when feasible. Differential diagnoses include other systemic vasculitides, granulomatous lung diseases, anti–glomerular basement membrane disease, infections, malignancy, and drug- or cocaine-induced vasculitis.
Workup Evaluation
includes detailed history and physical examination, chest imaging, renal assessment, and targeted organ evaluation. ANCA serology typically shows PR3-ANCA in GPA and MPO-ANCA in MPA, though overlap exists and up to 15% of patients may be ANCA negative. Laboratory findings include anemia, leukocytosis, thrombocytosis, elevated inflammatory markers, impaired renal function, hematuria, and proteinuria. Tissue biopsy of affected organs, particularly kidney or lung, is recommended when safe to confirm diagnosis.
Treatment Management depends on disease severity and organ involvement. Induction therapy for moderate to severe disease includes systemic glucocorticoids combined with rituximab or cyclophosphamide. Reduced-dose steroid regimens may be used. Plasma exchange may be considered in select severe cases, though overall benefit is limited. Mild or limited disease may be treated with methotrexate-based regimens. Maintenance therapy commonly includes rituximab, azathioprine, methotrexate, or mycophenolate mofetil and is generally continued for 18–24 months. EGPA may additionally be treated with anti–interleukin-5 therapy such as mepolizumab. Prophylaxis against Pneumocystis jirovecii pneumonia is recommended during intensive immunosuppression.
Disposition and Referral
With prompt treatment, remission is achieved in most patients, though relapse is common. Renal failure and pulmonary involvement are major determinants of prognosis. Referral to rheumatology is essential, with multidisciplinary involvement from nephrology, pulmonology, ENT, dermatology, and neurology as indicated.
Pearls and Considerations
The goal of therapy is rapid induction of durable remission followed by maintenance treatment. Without treatment, mortality is high, and therapy is complicated by infection risk and progressive organ damage. Support and education resources are available through organizations such as the Vasculitis Foundation.
Basic Information Anti-neutrophil cytoplasmic antibody (ANCA)–associated vasculitis (AAV) is a group of small- to medium-vessel systemic vasculitides that includes granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA). These conditions share overlapping clinical manifestations and treatment strategies but differ in pathology and organ involvement. They are characterized by necrotizing, pauci-immune small-vessel vasculitis, with granulomatous inflammation present in GPA but absent in MPA. Most patients present with renal and pulmonary involvement, although the skin, nervous system, and gastrointestinal tract may also be affected. A limited form of GPA may be confined to the upper respiratory tract and can often be managed less aggressively.
Synonyms ANCA-associated vasculitis, ANCA-positive vasculitis, granulomatosis with polyangiitis (GPA), Wegener granulomatosis, microscopic polyangiitis (MPA), eosinophilic granulomatosis with polyangiitis (EGPA).
ICD-10-CM Codes I77.6 arteritis unspecified; M31.3 granulomatosis with polyangiitis; M31.7 microscopic polyangiitis; M30.1 eosinophilic granulomatosis with polyangiitis.
Epidemiology and Demographics The incidence is approximately 6–12 cases per million persons per year in Western Europe and Japan, with global variation. Prevalence ranges from 94 to 160 per million. There is a slight male predominance, and incidence increases with age, peaking between 60 and 70 years.
Risk Factors and Genetics Risk factors include infections such as Staphylococcus aureus, silica and hydrocarbon exposure, cigarette smoking, pesticides, and medications including hydralazine, minocycline, propylthiouracil, levamisole-adulterated cocaine, and allopurinol. Familial disease is rare. GPA is associated with SNPs in HLA-DP, PRTN3, and SERPINA1, whereas MPA is associated with HLA-DQ polymorphisms.
Physical Findings and Clinical Presentation Patients commonly have constitutional symptoms such as fever, fatigue, weight loss, myalgia, and arthralgia. Upper respiratory tract disease is prominent in GPA and includes chronic sinusitis, otitis media, mastoiditis, nasal crusting and epistaxis, septal perforation, subglottic or tracheal stenosis, and saddle-nose deformity. Ocular involvement includes conjunctivitis, episcleritis, scleritis, uveitis, optic neuropathy, and retinal vasculitis. Ear findings include sensorineural or conductive hearing loss and otorrhea. Oral findings may include chronic ulcerative lesions and “mulberry” gingivitis. Pulmonary disease presents with dyspnea, hemoptysis, pleuritic chest pain, nodules, cavitary lesions, infiltrates, effusions, or diffuse alveolar hemorrhage. Gastrointestinal involvement, more common in MPA, includes ischemic abdominal pain, bleeding, ulceration, or perforation. Renal disease is common in GPA and MPA and manifests as hypertension, edema, reduced urine output, rapidly progressive glomerulonephritis, microscopic hematuria, red cell casts, and proteinuria. Neurologic involvement includes mononeuritis multiplex, peripheral neuropathy, pachymeningitis, headaches, and rarely central nervous system disease. Cutaneous findings include palpable purpura, necrotic ulcers, nodules, urticaria, livedo reticularis, and digital gangrene.
Etiology The etiology is immune mediated and multifactorial. ANCAs directed against proteinase 3 (PR3) or myeloperoxidase (MPO) activate neutrophils, causing endothelial injury and tissue necrosis. Genetic susceptibility and environmental triggers contribute to disease development.
Diagnosis and Differential Diagnosis
Diagnosis is based on compatible clinical features supported by laboratory testing, imaging, and histopathology when feasible. Differential diagnoses include other systemic vasculitides, granulomatous lung diseases, anti–glomerular basement membrane disease, infections, malignancy, and drug- or cocaine-induced vasculitis.
Workup Evaluation
includes detailed history and physical examination, chest imaging, renal assessment, and targeted organ evaluation. ANCA serology typically shows PR3-ANCA in GPA and MPO-ANCA in MPA, though overlap exists and up to 15% of patients may be ANCA negative. Laboratory findings include anemia, leukocytosis, thrombocytosis, elevated inflammatory markers, impaired renal function, hematuria, and proteinuria. Tissue biopsy of affected organs, particularly kidney or lung, is recommended when safe to confirm diagnosis.
Treatment Management depends on disease severity and organ involvement. Induction therapy for moderate to severe disease includes systemic glucocorticoids combined with rituximab or cyclophosphamide. Reduced-dose steroid regimens may be used. Plasma exchange may be considered in select severe cases, though overall benefit is limited. Mild or limited disease may be treated with methotrexate-based regimens. Maintenance therapy commonly includes rituximab, azathioprine, methotrexate, or mycophenolate mofetil and is generally continued for 18–24 months. EGPA may additionally be treated with anti–interleukin-5 therapy such as mepolizumab. Prophylaxis against Pneumocystis jirovecii pneumonia is recommended during intensive immunosuppression.
Disposition and Referral
With prompt treatment, remission is achieved in most patients, though relapse is common. Renal failure and pulmonary involvement are major determinants of prognosis. Referral to rheumatology is essential, with multidisciplinary involvement from nephrology, pulmonology, ENT, dermatology, and neurology as indicated.
Pearls and Considerations
The goal of therapy is rapid induction of durable remission followed by maintenance treatment. Without treatment, mortality is high, and therapy is complicated by infection risk and progressive organ damage. Support and education resources are available through organizations such as the Vasculitis Foundation.

- Published on
KembaraXtra-Medicine- Angina Pectoris
Basic Information
Angina pectoris is a clinical syndrome of discomfort in the chest, jaw, shoulder, back, or arm caused by myocardial ischemia. Most commonly it is related to atherosclerotic (atheromatous) plaque in one or more large epicardial coronary arteries, but ischemia can also occur without obstructive coronary artery disease. Nonobstructive causes include uncontrolled hypertension, microvascular disease, valvular heart disease, hypertrophic cardiomyopathy, coronary spasm, and endothelial dysfunction. In general, any condition that creates an imbalance between myocardial oxygen supply and demand can produce an angina syndrome.
Classification of Angina
Chronic stable angina (also termed stable ischemic heart disease or chronic coronary artery disease) is typically predictable and follows a precipitating event such as climbing stairs, sexual intercourse, a heavy meal, emotional stress, or cold weather. Episodes usually resemble prior attacks in severity and are relieved by rest or the patient’s customary dose of sublingual nitroglycerin. It is usually caused by fixed coronary obstruction from atherosclerosis, commonly with one or more major coronary stenoses, often >70%. Unstable angina includes rest angina, recent-onset angina, and crescendo angina and is addressed under acute coronary syndrome. Rest angina occurs at rest, is usually prolonged (>20 minutes), and occurs within 1 week of presentation. Recent-onset angina is angina of at least Canadian Cardiovascular Society (CCS) Class III severity beginning within the past 2 months. Crescendo angina is previously diagnosed angina that becomes more frequent, lasts longer, or occurs at a lower threshold, defined as worsening by more than one CCS class within 2 months to at least CCS Class III severity.
Prinzmetal (variant) angina occurs at rest, is commonly triggered after cold exposure, and tends to be cyclical. It is associated with episodic ST-segment elevations on ECG and is due to coronary artery spasm with or without superimposed coronary artery disease; these patients are more prone to ventricular arrhythmias. Microvascular angina (syndrome X) refers to patients with angina symptoms, a positive exercise test, normal coronary angiograms, and no coronary spasm. In this condition, defective endothelium-dependent dilation in the coronary microcirculation contributes to abnormal regulation of myocardial perfusion and ischemic symptoms. Patients with chest pain and normal or nonobstructive coronary angiograms are predominantly women, and prognosis may be less benign than often assumed, with about a 2% risk of death or myocardial infarction at 30 days.
Refractory angina describes patients who, despite optimal medical therapy using at least maximal tolerated doses of two antianginal medications (plus aspirin and intensive risk-factor modification such as smoking cessation and tight control of hypertension, diabetes, and hyperlipidemia), continue to have angina along with objective evidence of ischemia. Other causes of angina syndromes include angina due to aortic stenosis, idiopathic hypertrophic subaortic stenosis, and cocaine-induced coronary vasoconstriction.
Functional Classification (Canadian Cardiovascular Society, CCS)
Class I: ordinary physical activity (walking, climbing stairs) does not cause angina; symptoms occur only with strenuous, rapid, or prolonged exertion at work or recreation. Class II: slight limitation of ordinary activity; angina occurs with walking or climbing stairs rapidly, walking uphill, activity after meals, exposure to cold or wind, emotional stress, or during the first few hours after awakening; angina occurs when walking more than two level blocks or climbing more than one flight of ordinary stairs at a normal pace in normal conditions. Class III: marked limitation of ordinary physical activity; angina occurs with walking one to two level blocks or climbing one flight of stairs in normal conditions at a normal pace. Class IV: inability to carry on any physical activity without discomfort; anginal symptoms may be present at rest.
ICD-10-CM Codes
I20.1 Angina pectoris with documented spasm; I20.8 Other forms of angina pectoris; I20.9 Angina pectoris, unspecified. I25.110 Atherosclerotic heart disease of native coronary artery with unstable angina pectoris; I25.111 Atherosclerotic heart disease of native coronary artery with angina pectoris with documented spasm; I25.118 Atherosclerotic heart disease of native coronary artery with other forms of angina pectoris; I25.119 Atherosclerotic heart disease of native coronary artery with unspecified angina pectoris. I25.700 Atherosclerosis of coronary artery bypass graft(s), unspecified, with unstable angina pectoris; I25.790 Atherosclerosis of other coronary artery bypass graft(s) with unstable angina pectoris; I25.791 Atherosclerosis of other coronary artery bypass graft(s) with angina pectoris with documented spasm; I25.798 Atherosclerosis of other coronary artery bypass graft(s) with other forms of angina pectoris; I25.799 Atherosclerosis of other coronary artery bypass graft(s) with unspecified angina pectoris.
Epidemiology and Demographics
Approximately one in three adults in the United States (about 81 million) has some form of cardiovascular disease. Based on NHANES 2007–2010, an estimated 15.4 million people have coronary heart disease, and about 7.8 million have angina. Angina is most common in middle-aged and elderly men. Among persons aged 60–79 years, roughly 25% of men and 16% of women have coronary heart disease; among those older than 80 years, the figures rise to about 37% for men and 23% for women. After menopause, the incidence of coronary heart disease and angina in women becomes similar to that in men. Even with improving survival over time, stable ischemic heart disease remains the leading cause of death in men and women (about 27% of deaths). Angina is the initial manifestation of ischemic heart disease in about 50% of cases, and about half of patients who present with acute coronary syndrome report preceding angina. Older population-based studies (Olmstead County, MN and Framingham, MA) reported an annual myocardial infarction rate of about 3%–3.5% per year among patients with symptomatic angina. Within 12 months of stable angina diagnosis, about 10%–20% progress to myocardial infarction or unstable angina.
Physical Findings and Clinical Presentation
Evaluating chest pain requires attention to quality, location, severity, duration, radiation, associated symptoms, provoking factors, and relieving factors. Anginal pain is often described as squeezing, griplike, suffocating, or heavy; it is rarely sharp or stabbing and typically does not change with position or respiration. The classic Levine sign is a clenched fist placed over the precordium. Many patients describe angina not as “pain” but as tightness, pressure, or discomfort. Atypical presentations are more common in women and older adults and may include nausea, vomiting, midepigastric discomfort, sharp (atypical) chest pain, dizziness, or syncope. Ischemic discomfort lasting longer than 20 minutes should raise concern for acute coronary syndrome. Women are more likely than men to report atypical chest pain or discomfort (reported by 65% in the WISE study). Elderly patients and those with diabetes may present with non–chest pain symptoms such as dyspnea, fatigue, or diaphoresis.
Etiology and Risk Factors
Key risk factors include advanced age, male sex, and genetic predisposition such as a family history of premature coronary artery disease in first-degree relatives (men <55 years, women <65 years). smoking increases the risk of first myocardial infarction nearly threefold. other major risks include hypertension, hyperlipidemia, impaired glucose tolerance or diabetes mellitus, prior stroke peripheral arterial disease, chronic kidney metabolic syndrome, physical inactivity, and obesity (bmi>30% over ideal). Higher childhood BMI is also associated with increased adult coronary heart disease risk.
Several conditions increase myocardial oxygen demand, including hyperthermia (especially with volume contraction), hyperthyroidism, and cocaine or methamphetamine use. Cocaine is used regularly by more than 5 million Americans and leads to over 64,000 emergency department evaluations yearly to rule out myocardial ischemia; it causes sympathomimetic toxicity, increases oxygen demand, induces coronary vasospasm, and can cause infarction in young patients, while long-term use accelerates stable ischemic heart disease. Severe uncontrolled hypertension increases myocardial oxygen demand and reduces subendocardial perfusion by increasing left ventricular wall tension; hypertrophic cardiomyopathy and aortic stenosis can produce even more severe hypertrophy and wall tension. Ventricular or supraventricular tachycardias can also raise oxygen demand and may require ambulatory monitoring for diagnosis.
Reduced oxygen supply can trigger angina as well. Anemia may cause angina when hemoglobin falls below about 9 g/dL, and ST–T changes (depression or inversion) can occur at hemoglobin levels below about 7 g/dL. Hypoxemia from pulmonary disease such as pneumonia, asthma, COPD, pulmonary hypertension, interstitial fibrosis, or obstructive sleep apnea can precipitate angina. Additional associated conditions and exposures include polycythemia, leukemia, thrombocytosis, hypergammaglobulinemia, oral contraceptive or hormone replacement therapy use, coronary artery calcium (linked to higher MI risk), long-term NSAID use, and traffic-related air pollution (dilute diesel exhaust), which promotes ischemia and adverse cardiovascular events. Low serum folate (needed to convert homocysteine to methionine) is associated with increased fatal coronary heart disease risk; hyperhomocysteinemia damages endothelium and promotes arterial smooth muscle proliferation and is an independent risk factor for coronary events, particularly in type 2 diabetes. Elevated high-sensitivity C-reactive protein (cardio-CRP) reflects systemic inflammation and is linked to accelerated atherosclerosis. Other noted associations include depression, vasculitis, elevated lipoprotein-associated phospholipase A2, elevated fibrinogen, low red blood cell glutathione peroxidase-1 activity, and prior radiation therapy.
Diagnosis: Differential Diagnosis
Nonischemic cardiovascular causes include aortic dissection and pericarditis. Pulmonary causes include pulmonary embolism, pneumothorax, pneumonia, and pleuritis. Gastrointestinal causes include esophageal disorders (esophagitis, spasm, reflux), biliary colic, cholecystitis, choledocholithiasis, cholangitis, peptic ulcer disease, pancreatitis, and other upper GI pathology. Chest wall causes include costochondritis, fibrositis, rib fracture, sternoclavicular arthritis, and herpes zoster before rash onset. Psychiatric causes include anxiety disorders, hyperventilation, panic disorder, primary anxiety, affective disorders (including depression), somatoform disorders, and thought disorders such as fixed delusions.
Workup and Clinical Risk Assessment
In patients with chest pain, estimate the probability of coronary artery disease based on age, sex, cardiovascular risk factors, and pain characteristics. History is the most important diagnostic element: exertional chest or left arm discomfort relieved by rest in a patient with risk factors strongly suggests coronary disease. Chest pain is categorized as typical angina, atypical angina, or noncardiac chest pain. Typical (definite) angina includes all three: substernal discomfort with characteristic quality and duration, provoked by exertion or emotional stress, and relieved by rest and/or sublingual nitroglycerin. Atypical (probable) angina has two of these features. Noncardiac chest pain has one or none.
Physical examination may be normal, but findings such as hypertension, arcus senilis, xanthelasma, carotid or peripheral bruits, and a prominent S4 increase suspicion for coronary artery disease. A mitral regurgitation murmur may indicate ischemic cardiomyopathy or transient ischemia, while murmurs of hypertrophic cardiomyopathy or aortic stenosis suggest non-CAD causes of angina. The overall evaluation aims to identify high-risk coronary disease while minimizing resource use. A practical approach considers (1) coronary risk assessment using classic risk factors, (2) functional capacity and stress test results, (3) left and right ventricular function, and (4) coronary anatomy, recognizing not every patient needs every modality. Patients without known coronary artery disease are typically stratified into low, intermediate, or high pretest probability after considering comorbidities and atherosclerotic risk; functional capacity and stress testing (exercise tolerance test, exercise testing with myocardial perfusion imaging, or stress echocardiography) are emphasized for low-to-intermediate probability groups. Exercise testing is preferred when feasible. Stress results help estimate annual mortality risk: <1% low risk, 1%–3% intermediate and>3% high risk.
Laboratory Tests and ECG/Imaging Basics
Screen for hypertension, diabetes, and hyperlipidemia per routine guidelines. Obtain an ECG during pain and when the patient is symptom-free; a normal resting ECG can occur in stable ischemic heart disease, and a small percentage of acute MI patients may have a normal or nondiagnostic ECG. Chest x-ray (PA and lateral) is considered when symptoms suggest heart failure, pericardial disease, or aortic aneurysm/dissection. High-sensitivity CRP (cardio-CRP) is a moderate predictor of coronary disease and adds prognostic value beyond the Framingham risk score.
Exercise Testing and Stress Imaging
Exercise testing is used for diagnosis and prognosis and provides important prognostic information via exercise performance and hemodynamic response. It is most useful in intermediate-likelihood patients because low-likelihood patients can have false positives and high-likelihood patients can have false negatives. The treadmill test is contraindicated when baseline ECG abnormalities make interpretation unreliable, including ST depression >0.5 mm, Wolff-Parkinson-White syndrome, left bundle branch block, or pacemaker rhythm. If baseline ECG abnormalities prevent interpretation, use stress echocardiography or myocardial perfusion imaging. Stress echocardiography tends to have higher specificity and lower cost, whereas radionuclide perfusion imaging has higher sensitivity (notably for single-vessel disease) and higher technical success. If the patient cannot exercise adequately, pharmacologic stress testing (e.g., dobutamine, adenosine, regadenoson) can be paired with these imaging modalities.
Risk Stratification From Noninvasive Testing
High risk (>3% annual risk of death or MI) includes severe resting LV dysfunction (LVEF <35%) not explained by noncoronary causes; resting perfusion abnormalities involving ≥10% of myocardium without prior mi; high-risk stress ecg findings such as ≥2 mm st depression at low workload or persisting into recovery, exercise-induced elevation, ventricular tachycardia />ibrillation; severe stress-induced LV dysfunction (peak exercise LVEF <45% or lvef drop ≥10%); stress-induced perfusion abnormalities involving ≥10% of myocardium multiple vascular territories; lv dilation; inducible wall motion abnormality>2 segments or two coronary beds; wall motion abnormality at low-dose dobutamine (≤10 mg/kg/min) or low heart rate (<120 bpm); and multivessel obstructive cad (≥70%) or left main stenosis (≥50%) on coronary cta.< />pan>
Intermediate risk (1%–3% annual risk) includes mild-to-moderate resting LV dysfunction (LVEF 35%–49%); resting perfusion abnormalities involving 5%–9.9% without prior MI; ≥1 mm ST depression with exertional symptoms; stress perfusion abnormalities involving 5%–9.9% or one vascular territory without LV dilation; small wall motion abnormality involving 1–2 segments and one coronary bed; and single-vessel CAD ≥70% or moderate stenosis (50%–69%) in ≥2 arteries on coronary CTA. Low risk (<1% annual risk) includes a low-risk treadmill score (≥5) or no new st changes exercise-induced chest pain at maximal exercise; normal small perfusion defect involving <5% of myocardium; stress change in limited resting wall motion abnormalities with stress; and coronary stenosis>50% on coronary CTA (noting these “low-risk” findings may not indicate truly low risk if a high-risk treadmill score or severe resting LV dysfunction is present). Coronary artery calcium assessment may also contribute to risk stratification.
A useful predictor in stable angina is the Duke treadmill score, combining exercise time/METS (Bruce protocol), ST-segment depression in millimeters, and an angina index; favorable scores (>5) are associated with >97% five-year survival independent of coronary anatomy and LV function.
Echocardiography, Coronary CTA, Calcium Scoring, Cardiac MRI, and Invasive Angiography
Echocardiography is indicated when murmurs suggest aortic stenosis, hypertrophic cardiomyopathy, mitral regurgitation, or mitral valve prolapse, and in patients with prior MI, pathologic Q waves, complex ventricular arrhythmias, heart failure, hypertension, diabetes, or abnormal ECG. Coronary CT angiography (CCTA) can detect subclinical CAD in asymptomatic patients with intermediate 10-year Framingham risk (10%–20%) and is recommended by 2021 ACC/AHA/ASE chest pain guidelines as a front-line imaging modality for stable angina. Studies comparing CCTA to invasive coronary angiography in stable angina show similar outcomes but fewer procedural complications and fewer invasive angiograms with an initial CCTA strategy. CCTA evaluates coronary calcium, lumen, and vessel wall; it can be first-line for risk assessment when a patient cannot exercise adequately, can clarify indeterminate functional tests, and can assess bypass graft or large stent patency (>3 mm). Cost and radiation limit routine broad use. CCTA has high negative predictive value to rule out severe CAD during ED chest pain evaluation (ROMICAT-II), and the SCOT-HEART trial (2018) showed coronary CTA lowered nonfatal MI risk compared with standard care alone in stable angina. Myocardial perfusion imaging and noninvasive fractional flow reserve can also be derived from cardiac CTA in selected settings.
Coronary artery calcium scoring provides strong predictive value beyond standard risk factors in low-to-intermediate pretest probability patients; a score <100 suggests low risk, while>400 suggests high risk. Cardiac MRI, beyond diagnosing arrhythmogenic right ventricular dysplasia, can assess perfusion, viability, and function in patients unable to exercise, though further cost-effectiveness data are needed in ischemic cardiomyopathy. Invasive coronary angiography remains the gold standard to define clinically significant CAD and is used to map location and extent of disease, especially in patients being considered for revascularization (CABG or angioplasty).
Treatment Overview: Core Strategies
Management involves five overlapping strategies: patient education and shared decision-making; management of comorbid conditions that worsen stable ischemic heart disease; aggressive modification of preventable risk factors (smoking cessation, weight loss in obesity, regular aerobic exercise 30–60 minutes/day for 5 days/week, folate deficiency correction, limiting saturated fat to <7% of calories and trans fats to <1%, low-sodium diet <2 g />ay, and emphasizing medication adherence); evidence-based pharmacologic therapy to improve symptoms and survival; and appropriate revascularization for selected patients to improve survival and long-term outcomes.
Pharmacologic Therapy (Prevention of MI/Death and Symptom Control)
Aspirin reduces cardiovascular mortality and morbidity by about 20%–25% in CAD; the usual dose is 75–162 mg/day if no contraindication. It inhibits cyclooxygenase and thromboxane A2 and reduces adverse cardiovascular events; patients intolerant of aspirin may use clopidogrel or undergo aspirin desensitization. Clopidogrel irreversibly blocks the P2Y12 ADP receptor, reducing platelet activation and aggregation; it can be used alone for aspirin intolerance or combined with aspirin in high-risk stable ischemic heart disease patients with low bleeding risk; dose is 75 mg/day. Ticagrelor (PEGASUS-TIMI 54) reduced death, cardiovascular MI, or stroke in patients after one year post-MI but increases bleeding risk versus placebo. Dipyridamole is not recommended as antiplatelet therapy in stable ischemic heart disease.
Beta-blockers are first-line for stable angina and have proven benefits in preventing MI and death. They reduce myocardial oxygen demand by lowering heart rate, blood pressure, AV nodal conduction, and contractility, raising the ischemic threshold and decreasing angina frequency. Doses are generally adjusted to achieve a resting heart rate of 55–60 bpm. Beta-blockers are recommended for at least 2–3 years after MI and lifelong for patients with LVEF <40% with heart failure or prior mi.< />pan>
Nitrates cause venodilation and vascular smooth muscle relaxation, decreasing preload (and myocardial oxygen consumption) and reducing resistance across obstructed segments, while redistributing coronary flow by augmenting collateral circulation and lowering LV diastolic pressure; they also have antithrombotic and antiplatelet effects. Sublingual nitroglycerin or spray should be prescribed for immediate angina relief in stable ischemic heart disease. Nitrate tolerance can be minimized with a daily nitrate-free interval (e.g., omit bedtime oral isosorbide dinitrate or use a 12-hour on/12-hour off transdermal schedule). Nitrates are relatively contraindicated in hypertrophic obstructive cardiomyopathy and should be avoided in severe aortic stenosis. They must not be used within 24 hours of sildenafil or vardenafil, or within 48 hours of tadalafil because of hypotension risk.
Calcium channel blockers improve oxygen supply by lowering coronary resistance and increasing arterial flow and reduce demand by lowering contractility and systemic vascular resistance; however, they have no proven mortality benefit in stable ischemic heart disease. They are first-line when beta-blockers are contraindicated, are key in coronary spasm, and are effective in microvascular angina. All classes reduce angina episodes, increase exercise duration, and reduce nitroglycerin use in effort-induced angina, but short-acting agents should be avoided. Nondihydropyridine calcium channel blockers should generally be avoided in systolic heart failure due to negative inotropy.
Ranolazine (studied in MARISA, CARISA, RAN080, ERICA; total ~1737 patients) inhibits the late inward sodium current, indirectly reducing sodium-dependent calcium influx during ischemia and improving diastolic tension and oxygen consumption. Its antianginal effects do not depend on heart rate or blood pressure reduction and it is used for chronic angina inadequately controlled by other agents, either as an alternative or in combination. It can prolong the QT interval, and low doses of diltiazem or verapamil should be used if combined.
ACE inhibitors may reduce LV/vascular hypertrophy, slow atherosclerosis progression, reduce plaque rupture/thrombosis risk, and improve hemodynamics and oxygen balance. They reduce cardiovascular death, MI, and stroke in at-risk patients or those with vascular disease, and are indicated in stable ischemic heart disease patients with hypertension, diabetes, LVEF <40%, or chronic kidney disease. arbs are alternatives for ace-intolerant patients who qualify.< />pan>
High-intensity statins are recommended for all patients with CAD. The ACC has recommended an LDL goal <70 mg />L for secondary prevention (no LDL goal for primary prevention). PCSK9 inhibitors (alirocumab, evolocumab) are approved for heterozygous familial hypercholesterolemia and are considered in very-high-risk atherosclerotic cardiovascular disease patients not at LDL goal despite high-intensity statin plus ezetimibe; ezetimibe should generally be tried before PCSK9 inhibitors due to cost. Inclisiran, evinacumab, and bempedoic acid are reasonable nonstatin options for patients unable to tolerate statins or reach LDL targets. Annual influenza vaccination is recommended in stable ischemic heart disease to reduce mortality, morbidity, and hospitalization. In type 2 diabetes, major trials (EMPA-REG OUTCOME, CANVAS, DECLARE-TIMI 58, CREDENCE) show SGLT2 inhibitors reduce cardiovascular events.
Newer and Adjunct Modalities for Chronic Stable Angina
Despite progress with PCI and CABG, some patients need additional therapies for symptom relief and quality of life, especially those with diffuse CAD unsuitable for revascularization, multiple prior PCIs/CABG, lack of bypass conduits, severe LV systolic dysfunction after revascularization, or comorbidities making procedures high risk. Pharmacologic agents explored as adjuncts to standard therapy (nitrates, beta-blockers, calcium channel blockers, ranolazine) include high-dose statins, trimetazidine, perhexiline, nicorandil, allopurinol, ivabradine, fasudil, and testosterone. Experimental nonpharmacologic options include stem cell therapy, therapeutic angiogenesis, and mechanical therapies such as enhanced external counterpulsation, spinal cord stimulation, transmyocardial laser revascularization, and coronary sinus reducing devices.
In TACT, EDTA chelation infusions reduced a composite outcome (including mortality, recurrent MI, stroke, revascularization, or angina hospitalization), leading chelation therapy to be upgraded from Class III (not recommended) to Class IIb in 2014 stable ischemic heart disease guidelines. Allopurinol (xanthine oxidase inhibitor) at 600 mg daily for 6 weeks in a small crossover study of 65 heart failure patients increased median time to ST depression (232 to 393 seconds), but larger studies are needed before recommending it routinely. Testosterone may improve endothelial dysfunction and potentially angina, but safety concerns require more trials. EECP was assessed in MUST-EECP (139 outpatients randomized to 35 hours active EECP), showing it was well tolerated; exercise duration rose in both groups; active EECP increased time to 1-mm ST depression while inactive did not; and more active EECP patients had fewer angina episodes. Professional society updates state EECP may be considered for refractory angina. Treatments not shown to reduce cardiovascular risk or improve outcomes include estrogen therapy; vitamin C, vitamin E, beta-carotene supplementation; folate/B6/B12 therapy solely to lower homocysteine; chelation therapy (outside its limited guideline context); garlic; coenzyme Q10; selenium; and chromium.
Referral and Revascularization
Revascularization strategy is chosen to improve survival and/or symptoms and includes PCI (balloon angioplasty and stenting) or CABG. While PCI is clearly beneficial in acute MI, its role in stable CAD is less clear; PCI use for stable CAD fell substantially from 2007 to 2011, especially in high-volume PCI hospitals.
To improve survival, CABG is recommended for significant left main stenosis (>50%), proximal LAD stenosis >70%, three-vessel disease with >70% stenosis, or two-vessel disease with severe/extensive ischemia, and for patients with mild-to-moderate LV systolic dysfunction (EF 35%–50%) with significant multivessel CAD. A left internal mammary artery graft to the LAD improves survival. CABG is preferred over PCI to improve survival in multivessel CAD with SYNTAX score >22 and in multivessel CAD with diabetes, particularly when LIMA-to-LAD grafting is used. PCI may be a reasonable alternative to CABG in selected stable patients with unprotected left main CAD when SYNTAX is low-to-intermediate and/or surgical risk is high (e.g., STS operative mortality risk >5%), PCI procedural complication risk is low, and likelihood of good long-term outcome is high.
To improve symptoms, CABG or PCI can be beneficial for patients with one or more significant (>70%) stenoses amenable to revascularization who have unacceptable angina despite maximal medical therapy, or when medications cannot be intensified due to contraindications, adverse effects, or patient preference. The ORBITA trial (2017) showed no significant improvement in angina score after PCI in optimally treated stable angina, though most placebo-group patients later underwent PCI. The ISCHEMIA trial (2020) showed no benefit of routine invasive therapy over conservative treatment in moderate-to-severe ischemia, but excluded patients with acute coronary syndrome, severe/frequent symptoms, EF <35%, and left main stenosis. hybrid revascularization (lima-to-lad grafting plus pci to non-lad vessels) may be used when the aorta is unfavorable, cabg targets are poor, conduits unsuitable, or lad anatomy unfavorable for pci. compared with pci, provides more effective angina relief fewer repeat procedures but carries a higher procedural stroke risk; 10-year survival similar.< />pan>
PCI is widely used for symptom relief but is not superior to intensive medical therapy in preventing MI or death in stable patients. Candidates for PCI should also be candidates for CABG. About 80% experience immediate symptom benefit after PCI. Stents are used in the majority of PCI cases and reduce restenosis when used electively in atheromatous lesions. Key limitations of stenting include subacute thrombosis, in-stent restenosis, bleeding risk from antiplatelet therapy, and higher cost. Dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor) prevents stent thrombosis; duration depends on stent type—about 4 weeks for bare metal stents and generally 6–12 months for drug-eluting stents due to delayed endothelialization. Newer drug-eluting stents with thin struts and limus-family drugs from durable polymers reduce stent thrombosis risk compared with early-generation sirolimus- or paclitaxel-eluting stents. Current evidence supports drug-eluting stents in most settings unless dual antiplatelet therapy is contraindicated.
Pearls and Considerations
Although nitrate responsiveness has traditionally been part of the diagnostic approach for stable ischemic heart disease, some evidence suggests that relief after nitroglycerin does not reliably predict active coronary artery disease in general chest pain admissions and should not be used alone to guide acute diagnosis. CABG offers higher long-term survival and fewer repeat revascularizations than PCI in some populations, but many patients prefer stenting because it is less invasive, involves shorter hospitalization, and has lower in-hospital mortality.
Basic Information
Angina pectoris is a clinical syndrome of discomfort in the chest, jaw, shoulder, back, or arm caused by myocardial ischemia. Most commonly it is related to atherosclerotic (atheromatous) plaque in one or more large epicardial coronary arteries, but ischemia can also occur without obstructive coronary artery disease. Nonobstructive causes include uncontrolled hypertension, microvascular disease, valvular heart disease, hypertrophic cardiomyopathy, coronary spasm, and endothelial dysfunction. In general, any condition that creates an imbalance between myocardial oxygen supply and demand can produce an angina syndrome.
Classification of Angina
Chronic stable angina (also termed stable ischemic heart disease or chronic coronary artery disease) is typically predictable and follows a precipitating event such as climbing stairs, sexual intercourse, a heavy meal, emotional stress, or cold weather. Episodes usually resemble prior attacks in severity and are relieved by rest or the patient’s customary dose of sublingual nitroglycerin. It is usually caused by fixed coronary obstruction from atherosclerosis, commonly with one or more major coronary stenoses, often >70%. Unstable angina includes rest angina, recent-onset angina, and crescendo angina and is addressed under acute coronary syndrome. Rest angina occurs at rest, is usually prolonged (>20 minutes), and occurs within 1 week of presentation. Recent-onset angina is angina of at least Canadian Cardiovascular Society (CCS) Class III severity beginning within the past 2 months. Crescendo angina is previously diagnosed angina that becomes more frequent, lasts longer, or occurs at a lower threshold, defined as worsening by more than one CCS class within 2 months to at least CCS Class III severity.
Prinzmetal (variant) angina occurs at rest, is commonly triggered after cold exposure, and tends to be cyclical. It is associated with episodic ST-segment elevations on ECG and is due to coronary artery spasm with or without superimposed coronary artery disease; these patients are more prone to ventricular arrhythmias. Microvascular angina (syndrome X) refers to patients with angina symptoms, a positive exercise test, normal coronary angiograms, and no coronary spasm. In this condition, defective endothelium-dependent dilation in the coronary microcirculation contributes to abnormal regulation of myocardial perfusion and ischemic symptoms. Patients with chest pain and normal or nonobstructive coronary angiograms are predominantly women, and prognosis may be less benign than often assumed, with about a 2% risk of death or myocardial infarction at 30 days.
Refractory angina describes patients who, despite optimal medical therapy using at least maximal tolerated doses of two antianginal medications (plus aspirin and intensive risk-factor modification such as smoking cessation and tight control of hypertension, diabetes, and hyperlipidemia), continue to have angina along with objective evidence of ischemia. Other causes of angina syndromes include angina due to aortic stenosis, idiopathic hypertrophic subaortic stenosis, and cocaine-induced coronary vasoconstriction.
Functional Classification (Canadian Cardiovascular Society, CCS)
Class I: ordinary physical activity (walking, climbing stairs) does not cause angina; symptoms occur only with strenuous, rapid, or prolonged exertion at work or recreation. Class II: slight limitation of ordinary activity; angina occurs with walking or climbing stairs rapidly, walking uphill, activity after meals, exposure to cold or wind, emotional stress, or during the first few hours after awakening; angina occurs when walking more than two level blocks or climbing more than one flight of ordinary stairs at a normal pace in normal conditions. Class III: marked limitation of ordinary physical activity; angina occurs with walking one to two level blocks or climbing one flight of stairs in normal conditions at a normal pace. Class IV: inability to carry on any physical activity without discomfort; anginal symptoms may be present at rest.
ICD-10-CM Codes
I20.1 Angina pectoris with documented spasm; I20.8 Other forms of angina pectoris; I20.9 Angina pectoris, unspecified. I25.110 Atherosclerotic heart disease of native coronary artery with unstable angina pectoris; I25.111 Atherosclerotic heart disease of native coronary artery with angina pectoris with documented spasm; I25.118 Atherosclerotic heart disease of native coronary artery with other forms of angina pectoris; I25.119 Atherosclerotic heart disease of native coronary artery with unspecified angina pectoris. I25.700 Atherosclerosis of coronary artery bypass graft(s), unspecified, with unstable angina pectoris; I25.790 Atherosclerosis of other coronary artery bypass graft(s) with unstable angina pectoris; I25.791 Atherosclerosis of other coronary artery bypass graft(s) with angina pectoris with documented spasm; I25.798 Atherosclerosis of other coronary artery bypass graft(s) with other forms of angina pectoris; I25.799 Atherosclerosis of other coronary artery bypass graft(s) with unspecified angina pectoris.
Epidemiology and Demographics
Approximately one in three adults in the United States (about 81 million) has some form of cardiovascular disease. Based on NHANES 2007–2010, an estimated 15.4 million people have coronary heart disease, and about 7.8 million have angina. Angina is most common in middle-aged and elderly men. Among persons aged 60–79 years, roughly 25% of men and 16% of women have coronary heart disease; among those older than 80 years, the figures rise to about 37% for men and 23% for women. After menopause, the incidence of coronary heart disease and angina in women becomes similar to that in men. Even with improving survival over time, stable ischemic heart disease remains the leading cause of death in men and women (about 27% of deaths). Angina is the initial manifestation of ischemic heart disease in about 50% of cases, and about half of patients who present with acute coronary syndrome report preceding angina. Older population-based studies (Olmstead County, MN and Framingham, MA) reported an annual myocardial infarction rate of about 3%–3.5% per year among patients with symptomatic angina. Within 12 months of stable angina diagnosis, about 10%–20% progress to myocardial infarction or unstable angina.
Physical Findings and Clinical Presentation
Evaluating chest pain requires attention to quality, location, severity, duration, radiation, associated symptoms, provoking factors, and relieving factors. Anginal pain is often described as squeezing, griplike, suffocating, or heavy; it is rarely sharp or stabbing and typically does not change with position or respiration. The classic Levine sign is a clenched fist placed over the precordium. Many patients describe angina not as “pain” but as tightness, pressure, or discomfort. Atypical presentations are more common in women and older adults and may include nausea, vomiting, midepigastric discomfort, sharp (atypical) chest pain, dizziness, or syncope. Ischemic discomfort lasting longer than 20 minutes should raise concern for acute coronary syndrome. Women are more likely than men to report atypical chest pain or discomfort (reported by 65% in the WISE study). Elderly patients and those with diabetes may present with non–chest pain symptoms such as dyspnea, fatigue, or diaphoresis.
Etiology and Risk Factors
Key risk factors include advanced age, male sex, and genetic predisposition such as a family history of premature coronary artery disease in first-degree relatives (men <55 years, women <65 years). smoking increases the risk of first myocardial infarction nearly threefold. other major risks include hypertension, hyperlipidemia, impaired glucose tolerance or diabetes mellitus, prior stroke peripheral arterial disease, chronic kidney metabolic syndrome, physical inactivity, and obesity (bmi>30% over ideal). Higher childhood BMI is also associated with increased adult coronary heart disease risk.
Several conditions increase myocardial oxygen demand, including hyperthermia (especially with volume contraction), hyperthyroidism, and cocaine or methamphetamine use. Cocaine is used regularly by more than 5 million Americans and leads to over 64,000 emergency department evaluations yearly to rule out myocardial ischemia; it causes sympathomimetic toxicity, increases oxygen demand, induces coronary vasospasm, and can cause infarction in young patients, while long-term use accelerates stable ischemic heart disease. Severe uncontrolled hypertension increases myocardial oxygen demand and reduces subendocardial perfusion by increasing left ventricular wall tension; hypertrophic cardiomyopathy and aortic stenosis can produce even more severe hypertrophy and wall tension. Ventricular or supraventricular tachycardias can also raise oxygen demand and may require ambulatory monitoring for diagnosis.
Reduced oxygen supply can trigger angina as well. Anemia may cause angina when hemoglobin falls below about 9 g/dL, and ST–T changes (depression or inversion) can occur at hemoglobin levels below about 7 g/dL. Hypoxemia from pulmonary disease such as pneumonia, asthma, COPD, pulmonary hypertension, interstitial fibrosis, or obstructive sleep apnea can precipitate angina. Additional associated conditions and exposures include polycythemia, leukemia, thrombocytosis, hypergammaglobulinemia, oral contraceptive or hormone replacement therapy use, coronary artery calcium (linked to higher MI risk), long-term NSAID use, and traffic-related air pollution (dilute diesel exhaust), which promotes ischemia and adverse cardiovascular events. Low serum folate (needed to convert homocysteine to methionine) is associated with increased fatal coronary heart disease risk; hyperhomocysteinemia damages endothelium and promotes arterial smooth muscle proliferation and is an independent risk factor for coronary events, particularly in type 2 diabetes. Elevated high-sensitivity C-reactive protein (cardio-CRP) reflects systemic inflammation and is linked to accelerated atherosclerosis. Other noted associations include depression, vasculitis, elevated lipoprotein-associated phospholipase A2, elevated fibrinogen, low red blood cell glutathione peroxidase-1 activity, and prior radiation therapy.
Diagnosis: Differential Diagnosis
Nonischemic cardiovascular causes include aortic dissection and pericarditis. Pulmonary causes include pulmonary embolism, pneumothorax, pneumonia, and pleuritis. Gastrointestinal causes include esophageal disorders (esophagitis, spasm, reflux), biliary colic, cholecystitis, choledocholithiasis, cholangitis, peptic ulcer disease, pancreatitis, and other upper GI pathology. Chest wall causes include costochondritis, fibrositis, rib fracture, sternoclavicular arthritis, and herpes zoster before rash onset. Psychiatric causes include anxiety disorders, hyperventilation, panic disorder, primary anxiety, affective disorders (including depression), somatoform disorders, and thought disorders such as fixed delusions.
Workup and Clinical Risk Assessment
In patients with chest pain, estimate the probability of coronary artery disease based on age, sex, cardiovascular risk factors, and pain characteristics. History is the most important diagnostic element: exertional chest or left arm discomfort relieved by rest in a patient with risk factors strongly suggests coronary disease. Chest pain is categorized as typical angina, atypical angina, or noncardiac chest pain. Typical (definite) angina includes all three: substernal discomfort with characteristic quality and duration, provoked by exertion or emotional stress, and relieved by rest and/or sublingual nitroglycerin. Atypical (probable) angina has two of these features. Noncardiac chest pain has one or none.
Physical examination may be normal, but findings such as hypertension, arcus senilis, xanthelasma, carotid or peripheral bruits, and a prominent S4 increase suspicion for coronary artery disease. A mitral regurgitation murmur may indicate ischemic cardiomyopathy or transient ischemia, while murmurs of hypertrophic cardiomyopathy or aortic stenosis suggest non-CAD causes of angina. The overall evaluation aims to identify high-risk coronary disease while minimizing resource use. A practical approach considers (1) coronary risk assessment using classic risk factors, (2) functional capacity and stress test results, (3) left and right ventricular function, and (4) coronary anatomy, recognizing not every patient needs every modality. Patients without known coronary artery disease are typically stratified into low, intermediate, or high pretest probability after considering comorbidities and atherosclerotic risk; functional capacity and stress testing (exercise tolerance test, exercise testing with myocardial perfusion imaging, or stress echocardiography) are emphasized for low-to-intermediate probability groups. Exercise testing is preferred when feasible. Stress results help estimate annual mortality risk: <1% low risk, 1%–3% intermediate and>3% high risk.
Laboratory Tests and ECG/Imaging Basics
Screen for hypertension, diabetes, and hyperlipidemia per routine guidelines. Obtain an ECG during pain and when the patient is symptom-free; a normal resting ECG can occur in stable ischemic heart disease, and a small percentage of acute MI patients may have a normal or nondiagnostic ECG. Chest x-ray (PA and lateral) is considered when symptoms suggest heart failure, pericardial disease, or aortic aneurysm/dissection. High-sensitivity CRP (cardio-CRP) is a moderate predictor of coronary disease and adds prognostic value beyond the Framingham risk score.
Exercise Testing and Stress Imaging
Exercise testing is used for diagnosis and prognosis and provides important prognostic information via exercise performance and hemodynamic response. It is most useful in intermediate-likelihood patients because low-likelihood patients can have false positives and high-likelihood patients can have false negatives. The treadmill test is contraindicated when baseline ECG abnormalities make interpretation unreliable, including ST depression >0.5 mm, Wolff-Parkinson-White syndrome, left bundle branch block, or pacemaker rhythm. If baseline ECG abnormalities prevent interpretation, use stress echocardiography or myocardial perfusion imaging. Stress echocardiography tends to have higher specificity and lower cost, whereas radionuclide perfusion imaging has higher sensitivity (notably for single-vessel disease) and higher technical success. If the patient cannot exercise adequately, pharmacologic stress testing (e.g., dobutamine, adenosine, regadenoson) can be paired with these imaging modalities.
Risk Stratification From Noninvasive Testing
High risk (>3% annual risk of death or MI) includes severe resting LV dysfunction (LVEF <35%) not explained by noncoronary causes; resting perfusion abnormalities involving ≥10% of myocardium without prior mi; high-risk stress ecg findings such as ≥2 mm st depression at low workload or persisting into recovery, exercise-induced elevation, ventricular tachycardia />ibrillation; severe stress-induced LV dysfunction (peak exercise LVEF <45% or lvef drop ≥10%); stress-induced perfusion abnormalities involving ≥10% of myocardium multiple vascular territories; lv dilation; inducible wall motion abnormality>2 segments or two coronary beds; wall motion abnormality at low-dose dobutamine (≤10 mg/kg/min) or low heart rate (<120 bpm); and multivessel obstructive cad (≥70%) or left main stenosis (≥50%) on coronary cta.< />pan>
Intermediate risk (1%–3% annual risk) includes mild-to-moderate resting LV dysfunction (LVEF 35%–49%); resting perfusion abnormalities involving 5%–9.9% without prior MI; ≥1 mm ST depression with exertional symptoms; stress perfusion abnormalities involving 5%–9.9% or one vascular territory without LV dilation; small wall motion abnormality involving 1–2 segments and one coronary bed; and single-vessel CAD ≥70% or moderate stenosis (50%–69%) in ≥2 arteries on coronary CTA. Low risk (<1% annual risk) includes a low-risk treadmill score (≥5) or no new st changes exercise-induced chest pain at maximal exercise; normal small perfusion defect involving <5% of myocardium; stress change in limited resting wall motion abnormalities with stress; and coronary stenosis>50% on coronary CTA (noting these “low-risk” findings may not indicate truly low risk if a high-risk treadmill score or severe resting LV dysfunction is present). Coronary artery calcium assessment may also contribute to risk stratification.
A useful predictor in stable angina is the Duke treadmill score, combining exercise time/METS (Bruce protocol), ST-segment depression in millimeters, and an angina index; favorable scores (>5) are associated with >97% five-year survival independent of coronary anatomy and LV function.
Echocardiography, Coronary CTA, Calcium Scoring, Cardiac MRI, and Invasive Angiography
Echocardiography is indicated when murmurs suggest aortic stenosis, hypertrophic cardiomyopathy, mitral regurgitation, or mitral valve prolapse, and in patients with prior MI, pathologic Q waves, complex ventricular arrhythmias, heart failure, hypertension, diabetes, or abnormal ECG. Coronary CT angiography (CCTA) can detect subclinical CAD in asymptomatic patients with intermediate 10-year Framingham risk (10%–20%) and is recommended by 2021 ACC/AHA/ASE chest pain guidelines as a front-line imaging modality for stable angina. Studies comparing CCTA to invasive coronary angiography in stable angina show similar outcomes but fewer procedural complications and fewer invasive angiograms with an initial CCTA strategy. CCTA evaluates coronary calcium, lumen, and vessel wall; it can be first-line for risk assessment when a patient cannot exercise adequately, can clarify indeterminate functional tests, and can assess bypass graft or large stent patency (>3 mm). Cost and radiation limit routine broad use. CCTA has high negative predictive value to rule out severe CAD during ED chest pain evaluation (ROMICAT-II), and the SCOT-HEART trial (2018) showed coronary CTA lowered nonfatal MI risk compared with standard care alone in stable angina. Myocardial perfusion imaging and noninvasive fractional flow reserve can also be derived from cardiac CTA in selected settings.
Coronary artery calcium scoring provides strong predictive value beyond standard risk factors in low-to-intermediate pretest probability patients; a score <100 suggests low risk, while>400 suggests high risk. Cardiac MRI, beyond diagnosing arrhythmogenic right ventricular dysplasia, can assess perfusion, viability, and function in patients unable to exercise, though further cost-effectiveness data are needed in ischemic cardiomyopathy. Invasive coronary angiography remains the gold standard to define clinically significant CAD and is used to map location and extent of disease, especially in patients being considered for revascularization (CABG or angioplasty).
Treatment Overview: Core Strategies
Management involves five overlapping strategies: patient education and shared decision-making; management of comorbid conditions that worsen stable ischemic heart disease; aggressive modification of preventable risk factors (smoking cessation, weight loss in obesity, regular aerobic exercise 30–60 minutes/day for 5 days/week, folate deficiency correction, limiting saturated fat to <7% of calories and trans fats to <1%, low-sodium diet <2 g />ay, and emphasizing medication adherence); evidence-based pharmacologic therapy to improve symptoms and survival; and appropriate revascularization for selected patients to improve survival and long-term outcomes.
Pharmacologic Therapy (Prevention of MI/Death and Symptom Control)
Aspirin reduces cardiovascular mortality and morbidity by about 20%–25% in CAD; the usual dose is 75–162 mg/day if no contraindication. It inhibits cyclooxygenase and thromboxane A2 and reduces adverse cardiovascular events; patients intolerant of aspirin may use clopidogrel or undergo aspirin desensitization. Clopidogrel irreversibly blocks the P2Y12 ADP receptor, reducing platelet activation and aggregation; it can be used alone for aspirin intolerance or combined with aspirin in high-risk stable ischemic heart disease patients with low bleeding risk; dose is 75 mg/day. Ticagrelor (PEGASUS-TIMI 54) reduced death, cardiovascular MI, or stroke in patients after one year post-MI but increases bleeding risk versus placebo. Dipyridamole is not recommended as antiplatelet therapy in stable ischemic heart disease.
Beta-blockers are first-line for stable angina and have proven benefits in preventing MI and death. They reduce myocardial oxygen demand by lowering heart rate, blood pressure, AV nodal conduction, and contractility, raising the ischemic threshold and decreasing angina frequency. Doses are generally adjusted to achieve a resting heart rate of 55–60 bpm. Beta-blockers are recommended for at least 2–3 years after MI and lifelong for patients with LVEF <40% with heart failure or prior mi.< />pan>
Nitrates cause venodilation and vascular smooth muscle relaxation, decreasing preload (and myocardial oxygen consumption) and reducing resistance across obstructed segments, while redistributing coronary flow by augmenting collateral circulation and lowering LV diastolic pressure; they also have antithrombotic and antiplatelet effects. Sublingual nitroglycerin or spray should be prescribed for immediate angina relief in stable ischemic heart disease. Nitrate tolerance can be minimized with a daily nitrate-free interval (e.g., omit bedtime oral isosorbide dinitrate or use a 12-hour on/12-hour off transdermal schedule). Nitrates are relatively contraindicated in hypertrophic obstructive cardiomyopathy and should be avoided in severe aortic stenosis. They must not be used within 24 hours of sildenafil or vardenafil, or within 48 hours of tadalafil because of hypotension risk.
Calcium channel blockers improve oxygen supply by lowering coronary resistance and increasing arterial flow and reduce demand by lowering contractility and systemic vascular resistance; however, they have no proven mortality benefit in stable ischemic heart disease. They are first-line when beta-blockers are contraindicated, are key in coronary spasm, and are effective in microvascular angina. All classes reduce angina episodes, increase exercise duration, and reduce nitroglycerin use in effort-induced angina, but short-acting agents should be avoided. Nondihydropyridine calcium channel blockers should generally be avoided in systolic heart failure due to negative inotropy.
Ranolazine (studied in MARISA, CARISA, RAN080, ERICA; total ~1737 patients) inhibits the late inward sodium current, indirectly reducing sodium-dependent calcium influx during ischemia and improving diastolic tension and oxygen consumption. Its antianginal effects do not depend on heart rate or blood pressure reduction and it is used for chronic angina inadequately controlled by other agents, either as an alternative or in combination. It can prolong the QT interval, and low doses of diltiazem or verapamil should be used if combined.
ACE inhibitors may reduce LV/vascular hypertrophy, slow atherosclerosis progression, reduce plaque rupture/thrombosis risk, and improve hemodynamics and oxygen balance. They reduce cardiovascular death, MI, and stroke in at-risk patients or those with vascular disease, and are indicated in stable ischemic heart disease patients with hypertension, diabetes, LVEF <40%, or chronic kidney disease. arbs are alternatives for ace-intolerant patients who qualify.< />pan>
High-intensity statins are recommended for all patients with CAD. The ACC has recommended an LDL goal <70 mg />L for secondary prevention (no LDL goal for primary prevention). PCSK9 inhibitors (alirocumab, evolocumab) are approved for heterozygous familial hypercholesterolemia and are considered in very-high-risk atherosclerotic cardiovascular disease patients not at LDL goal despite high-intensity statin plus ezetimibe; ezetimibe should generally be tried before PCSK9 inhibitors due to cost. Inclisiran, evinacumab, and bempedoic acid are reasonable nonstatin options for patients unable to tolerate statins or reach LDL targets. Annual influenza vaccination is recommended in stable ischemic heart disease to reduce mortality, morbidity, and hospitalization. In type 2 diabetes, major trials (EMPA-REG OUTCOME, CANVAS, DECLARE-TIMI 58, CREDENCE) show SGLT2 inhibitors reduce cardiovascular events.
Newer and Adjunct Modalities for Chronic Stable Angina
Despite progress with PCI and CABG, some patients need additional therapies for symptom relief and quality of life, especially those with diffuse CAD unsuitable for revascularization, multiple prior PCIs/CABG, lack of bypass conduits, severe LV systolic dysfunction after revascularization, or comorbidities making procedures high risk. Pharmacologic agents explored as adjuncts to standard therapy (nitrates, beta-blockers, calcium channel blockers, ranolazine) include high-dose statins, trimetazidine, perhexiline, nicorandil, allopurinol, ivabradine, fasudil, and testosterone. Experimental nonpharmacologic options include stem cell therapy, therapeutic angiogenesis, and mechanical therapies such as enhanced external counterpulsation, spinal cord stimulation, transmyocardial laser revascularization, and coronary sinus reducing devices.
In TACT, EDTA chelation infusions reduced a composite outcome (including mortality, recurrent MI, stroke, revascularization, or angina hospitalization), leading chelation therapy to be upgraded from Class III (not recommended) to Class IIb in 2014 stable ischemic heart disease guidelines. Allopurinol (xanthine oxidase inhibitor) at 600 mg daily for 6 weeks in a small crossover study of 65 heart failure patients increased median time to ST depression (232 to 393 seconds), but larger studies are needed before recommending it routinely. Testosterone may improve endothelial dysfunction and potentially angina, but safety concerns require more trials. EECP was assessed in MUST-EECP (139 outpatients randomized to 35 hours active EECP), showing it was well tolerated; exercise duration rose in both groups; active EECP increased time to 1-mm ST depression while inactive did not; and more active EECP patients had fewer angina episodes. Professional society updates state EECP may be considered for refractory angina. Treatments not shown to reduce cardiovascular risk or improve outcomes include estrogen therapy; vitamin C, vitamin E, beta-carotene supplementation; folate/B6/B12 therapy solely to lower homocysteine; chelation therapy (outside its limited guideline context); garlic; coenzyme Q10; selenium; and chromium.
Referral and Revascularization
Revascularization strategy is chosen to improve survival and/or symptoms and includes PCI (balloon angioplasty and stenting) or CABG. While PCI is clearly beneficial in acute MI, its role in stable CAD is less clear; PCI use for stable CAD fell substantially from 2007 to 2011, especially in high-volume PCI hospitals.
To improve survival, CABG is recommended for significant left main stenosis (>50%), proximal LAD stenosis >70%, three-vessel disease with >70% stenosis, or two-vessel disease with severe/extensive ischemia, and for patients with mild-to-moderate LV systolic dysfunction (EF 35%–50%) with significant multivessel CAD. A left internal mammary artery graft to the LAD improves survival. CABG is preferred over PCI to improve survival in multivessel CAD with SYNTAX score >22 and in multivessel CAD with diabetes, particularly when LIMA-to-LAD grafting is used. PCI may be a reasonable alternative to CABG in selected stable patients with unprotected left main CAD when SYNTAX is low-to-intermediate and/or surgical risk is high (e.g., STS operative mortality risk >5%), PCI procedural complication risk is low, and likelihood of good long-term outcome is high.
To improve symptoms, CABG or PCI can be beneficial for patients with one or more significant (>70%) stenoses amenable to revascularization who have unacceptable angina despite maximal medical therapy, or when medications cannot be intensified due to contraindications, adverse effects, or patient preference. The ORBITA trial (2017) showed no significant improvement in angina score after PCI in optimally treated stable angina, though most placebo-group patients later underwent PCI. The ISCHEMIA trial (2020) showed no benefit of routine invasive therapy over conservative treatment in moderate-to-severe ischemia, but excluded patients with acute coronary syndrome, severe/frequent symptoms, EF <35%, and left main stenosis. hybrid revascularization (lima-to-lad grafting plus pci to non-lad vessels) may be used when the aorta is unfavorable, cabg targets are poor, conduits unsuitable, or lad anatomy unfavorable for pci. compared with pci, provides more effective angina relief fewer repeat procedures but carries a higher procedural stroke risk; 10-year survival similar.< />pan>
PCI is widely used for symptom relief but is not superior to intensive medical therapy in preventing MI or death in stable patients. Candidates for PCI should also be candidates for CABG. About 80% experience immediate symptom benefit after PCI. Stents are used in the majority of PCI cases and reduce restenosis when used electively in atheromatous lesions. Key limitations of stenting include subacute thrombosis, in-stent restenosis, bleeding risk from antiplatelet therapy, and higher cost. Dual antiplatelet therapy (aspirin plus a P2Y12 inhibitor) prevents stent thrombosis; duration depends on stent type—about 4 weeks for bare metal stents and generally 6–12 months for drug-eluting stents due to delayed endothelialization. Newer drug-eluting stents with thin struts and limus-family drugs from durable polymers reduce stent thrombosis risk compared with early-generation sirolimus- or paclitaxel-eluting stents. Current evidence supports drug-eluting stents in most settings unless dual antiplatelet therapy is contraindicated.
Pearls and Considerations
Although nitrate responsiveness has traditionally been part of the diagnostic approach for stable ischemic heart disease, some evidence suggests that relief after nitroglycerin does not reliably predict active coronary artery disease in general chest pain admissions and should not be used alone to guide acute diagnosis. CABG offers higher long-term survival and fewer repeat revascularizations than PCI in some populations, but many patients prefer stenting because it is less invasive, involves shorter hospitalization, and has lower in-hospital mortality.
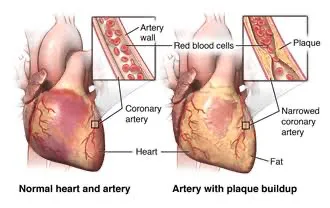
- Published on
KembaraXtra-Medicine- Angioedema
Basic Information
Urticaria and angioedema are mucocutaneous swellings that occur after release of vasoactive mediators. Urticaria affects the superficial dermis and produces wheals, whereas angioedema results from a transient increase in vascular permeability in mucosal/submucosal or dermal/subcutaneous tissues, leading to deeper tissue swelling.
Synonyms
Angioneurotic edema; Hereditary angioedema (HAE).
ICD-10-CM Codes
T78.3 Angioedema; D84.1 Angioedema, hereditary.
Epidemiology and Demographics
Urticaria and angioedema together have an incidence of about 100 to 3000 per 100,000 persons, and approximately 7.4% of the general population will experience angioedema alone. Around 25% of people will have urticaria and/or angioedema at some point in life. Hereditary angioedema occurs in about 1 in 50,000 persons. African Americans have higher rates of ACE inhibitor–induced angioedema. Angioedema occurs more often in women than men and commonly begins after adolescence, often in the third decade of life. Angioedema can occur with urticaria (about 40%) or alone (about 20%); the remaining ~40% have urticaria alone. For HAE due to C1 inhibitor problems, mean onset is 8–12 years and it rarely presents before age 1.
Physical Findings and Clinical Presentation
Angioedema may be acute or chronic. Acute angioedema is defined as symptoms lasting up to 6 weeks, while chronic angioedema lasts longer than 6 weeks. Typical swelling is nonpruritic, nonpitting, burning, and occasionally painful, involving deep skin layers or submucosal membranes. It is poorly demarcated and most often affects eyelids, lips, tongue, and extremities. It can involve the upper airway and cause respiratory distress, and it can involve the gastrointestinal tract, producing cyclic abdominal pain, nausea, vomiting, and diarrhea. Symptoms generally resolve slowly over hours to a few days.
Etiology and Pathophysiology
Angioedema (with or without urticaria) is broadly classified as histaminergic (mast cell–mediated or idiopathic) or bradykinin-mediated (such as hereditary forms). It is primarily triggered by immune activation with mediator release (histamine, serotonin, bradykinin), causing postcapillary venule inflammation, vascular leakage, and edema in deeper dermis/subcutaneous tissues. Mechanisms can be immunologic or nonimmunologic. IgE-mediated angioedema may follow exposure to foods (milk, eggs, peanuts, shellfish) or drugs (beta-lactam antibiotics, aspirin, NSAIDs, phenytoin, sulfonamide antibiotics, recombinant tissue plasminogen activator). Complement/immune-complex–mediated pathways can activate mast cells and may present as serum sickness.
Hereditary angioedema is subdivided into HAE type 1 (C1 inhibitor deficiency), HAE type 2 (C1 inhibitor dysfunction), and HAE with normal C1 inhibitor function (HAE nC1-INH). HAE-1 and HAE-2 are commonly due to autosomal dominant SERPING1 mutations affecting C1 esterase inhibitor (C1-INH). C1-INH inhibits plasma kallikrein; without adequate inhibition, kallikrein promotes bradykinin generation. Bradykinin is a potent vasodilator that increases capillary permeability and activates pain receptors, so excess bradykinin leads to angioedema. HAE-1 and HAE-2 are typically associated with low C4 due to complement activation, because C1 inhibitor is a major regulatory protein in the complement cascade.
Acquired angioedema is often linked to underlying disease—most commonly B-cell lymphoproliferative disorders—or may occur from autoantibodies against C1 inhibitor. Other triggers include infections (herpes simplex, hepatitis B, Coxsackie A/B, Streptococcus, Candida, Ascaris, Strongyloides), insect bites or stings, stress, physical factors (cold, exercise, pressure, vibration), connective tissue diseases (systemic lupus erythematosus, Henoch–Schönlein purpura), and idiopathic causes. ACE inhibitors can increase kinin activity and precipitate angioedema. Other medication triggers include antibiotics (beta-lactams, quinolones), opiates, and muscle relaxants (succinylcholine).
Diagnosis
A careful history and physical examination usually establish the diagnosis. Extensive laboratory testing is often of limited value.
Differential Diagnosis
Consider anaphylaxis, contact dermatitis, cellulitis, lymphedema, arthropod bite, hypothyroidism, atopic dermatitis, mastocytosis, granulomatous cheilitis, bullous pemphigoid, urticaria pigmentosa, erythema multiforme, epiglottitis, peritonsillar abscess, parasitic infection, and superior vena cava syndrome.
Workup
A broad workup to identify a cause is frequently unrevealing (about 40%). Testing is guided by the clinical history and exam. Basic tests such as CBC, ESR, and urinalysis may help in initial evaluation. Serum total tryptase can help confirm mast cell–mediated anaphylaxis. C4 is usually low in acquired and hereditary angioedema that occurs without urticaria; when C4 is low, measure C1-INH level and functional activity. Rarely, HAE may present with normal C4 but reduced C1-INH. If food allergy is suspected, skin prick testing and/or in vitro specific IgE testing (e.g., ImmunoCAP) may be used. Skin biopsy is generally reserved for chronic angioedema that is refractory to corticosteroids. Stool ova and parasite testing may be considered when parasitic infection is a concern.
Treatment: Nonpharmacologic Therapy
Remove or eliminate the offending agent when possible and avoid known triggers such as cold, stress, and culprit medications (especially ACE inhibitors). Cold compresses can be applied to affected areas for symptomatic relief.
Acute General Treatment
Life-threatening angioedema involving the larynx is treated urgently, although it is important to recognize that bradykinin-mediated angioedema responds minimally to these standard allergic-reaction medications. Typical emergency medications include subcutaneous epinephrine 0.3 mg (1:1000), an H1 antihistamine such as diphenhydramine 25–50 mg IV/IM or cetirizine 10 mg (listed as IV in the source), an H2 blocker such as cimetidine 300 mg IV or famotidine 20 mg IV, and methylprednisolone 125 mg IV.
For mast cell–mediated, nonhereditary angioedema, maintenance therapy centers on H1 antihistamines: cetirizine 10 mg daily (sometimes up to 4× FDA-approved dose), fexofenadine 180 mg daily (sometimes up to 4× dose), hydroxyzine 10–25 mg every 6 hours, or diphenhydramine 25–50 mg every 6 hours. H2 antihistamines can be added (cimetidine 400 mg twice daily or famotidine 20 mg twice daily). Doxepin 25–50 mg at bedtime can be used as an adjunct. Corticosteroids may be used for symptomatic relief in refractory acute cases. Antihistamines are ineffective for hereditary angioedema attacks.
Acute HAE attacks due to C1 inhibitor deficiency respond well to targeted therapies. Approved abortive options include plasma-derived C1 inhibitor concentrate (Berinert), icatibant (Firazyr), a bradykinin B2 receptor antagonist, and ecallantide (Kalbitor), a kallikrein inhibitor. Purified plasma-derived C1-INH replacement is considered effective and safe for acute attacks.
Chronic Treatment
Chronic histaminergic angioedema is treated similarly to acute management with H1 antihistamines, addition of H2 antihistamines as needed, and corticosteroids reserved for refractory cases. A regimen cited for refractory cases is prednisone 1 mg/kg/day for 5 days followed by a 7-day taper. Omalizumab (anti-IgE monoclonal antibody) has shown benefit in cases refractory to antihistamines, though it is not FDA-approved specifically for this indication.
For hereditary angioedema long-term prophylaxis, older options include androgens (danazol, stanozolol, oxandrolone, methyltestosterone) and antifibrinolytics, but adverse effects can be significant. Intravenous plasma-derived C1 inhibitors (Cinryze, Berinert) are safe and effective for patients with frequent or severe attacks, though cost may limit access. A twice-weekly subcutaneous C1-INH formulation (Haegarda/CSL830) is FDA-approved for HAE-1 and HAE-2. Lanadelumab and berotralstat (kallikrein inhibitors) have FDA approval for prophylaxis of HAE. In a phase 2 trial, donidalorsen (an antisense oligonucleotide that reduces plasma prekallikrein production) lowered attack rates compared with placebo.
Disposition
More than 85% of patients with nonhereditary acute angioedema achieve symptomatic relief with antihistamines. In chronic nonhereditary angioedema, antihistamines remain the mainstay, and systemic steroids should be reserved for severe or refractory cases. Some patients have recurrence after completing treatment. Chronic angioedema can persist for months to years and may be longer in hereditary angioedema.
Referral
Referral to a dermatologist and/or allergist is recommended for chronic angioedema, hereditary angioedema, and recurrent angioedema. HAE is potentially life-threatening and should be managed by an allergist.
Pearls and Considerations
ACE inhibitor–induced angioedema can occur months or even years after starting the drug. ARB-induced angioedema has been reported, though risk is substantially lower than with ACE inhibitors. About 10% of patients with recurrent angioedema had ACE inhibitor exposure, with a median duration of 1 year before symptoms began. Reported incidence rates per 1000 person-years are approximately 4.38 for ACE inhibitors, 1.66 for ARBs, and notably high for the direct renin inhibitor aliskiren (about 4.67).
Comments
Finding a clear cause is often difficult and can be frustrating. Chronic angioedema is rarely due to an allergic reaction, unlike many acute cases. Hereditary angioedema requires specialized care because of its life-threatening potential.
Basic Information
Urticaria and angioedema are mucocutaneous swellings that occur after release of vasoactive mediators. Urticaria affects the superficial dermis and produces wheals, whereas angioedema results from a transient increase in vascular permeability in mucosal/submucosal or dermal/subcutaneous tissues, leading to deeper tissue swelling.
Synonyms
Angioneurotic edema; Hereditary angioedema (HAE).
ICD-10-CM Codes
T78.3 Angioedema; D84.1 Angioedema, hereditary.
Epidemiology and Demographics
Urticaria and angioedema together have an incidence of about 100 to 3000 per 100,000 persons, and approximately 7.4% of the general population will experience angioedema alone. Around 25% of people will have urticaria and/or angioedema at some point in life. Hereditary angioedema occurs in about 1 in 50,000 persons. African Americans have higher rates of ACE inhibitor–induced angioedema. Angioedema occurs more often in women than men and commonly begins after adolescence, often in the third decade of life. Angioedema can occur with urticaria (about 40%) or alone (about 20%); the remaining ~40% have urticaria alone. For HAE due to C1 inhibitor problems, mean onset is 8–12 years and it rarely presents before age 1.
Physical Findings and Clinical Presentation
Angioedema may be acute or chronic. Acute angioedema is defined as symptoms lasting up to 6 weeks, while chronic angioedema lasts longer than 6 weeks. Typical swelling is nonpruritic, nonpitting, burning, and occasionally painful, involving deep skin layers or submucosal membranes. It is poorly demarcated and most often affects eyelids, lips, tongue, and extremities. It can involve the upper airway and cause respiratory distress, and it can involve the gastrointestinal tract, producing cyclic abdominal pain, nausea, vomiting, and diarrhea. Symptoms generally resolve slowly over hours to a few days.
Etiology and Pathophysiology
Angioedema (with or without urticaria) is broadly classified as histaminergic (mast cell–mediated or idiopathic) or bradykinin-mediated (such as hereditary forms). It is primarily triggered by immune activation with mediator release (histamine, serotonin, bradykinin), causing postcapillary venule inflammation, vascular leakage, and edema in deeper dermis/subcutaneous tissues. Mechanisms can be immunologic or nonimmunologic. IgE-mediated angioedema may follow exposure to foods (milk, eggs, peanuts, shellfish) or drugs (beta-lactam antibiotics, aspirin, NSAIDs, phenytoin, sulfonamide antibiotics, recombinant tissue plasminogen activator). Complement/immune-complex–mediated pathways can activate mast cells and may present as serum sickness.
Hereditary angioedema is subdivided into HAE type 1 (C1 inhibitor deficiency), HAE type 2 (C1 inhibitor dysfunction), and HAE with normal C1 inhibitor function (HAE nC1-INH). HAE-1 and HAE-2 are commonly due to autosomal dominant SERPING1 mutations affecting C1 esterase inhibitor (C1-INH). C1-INH inhibits plasma kallikrein; without adequate inhibition, kallikrein promotes bradykinin generation. Bradykinin is a potent vasodilator that increases capillary permeability and activates pain receptors, so excess bradykinin leads to angioedema. HAE-1 and HAE-2 are typically associated with low C4 due to complement activation, because C1 inhibitor is a major regulatory protein in the complement cascade.
Acquired angioedema is often linked to underlying disease—most commonly B-cell lymphoproliferative disorders—or may occur from autoantibodies against C1 inhibitor. Other triggers include infections (herpes simplex, hepatitis B, Coxsackie A/B, Streptococcus, Candida, Ascaris, Strongyloides), insect bites or stings, stress, physical factors (cold, exercise, pressure, vibration), connective tissue diseases (systemic lupus erythematosus, Henoch–Schönlein purpura), and idiopathic causes. ACE inhibitors can increase kinin activity and precipitate angioedema. Other medication triggers include antibiotics (beta-lactams, quinolones), opiates, and muscle relaxants (succinylcholine).
Diagnosis
A careful history and physical examination usually establish the diagnosis. Extensive laboratory testing is often of limited value.
Differential Diagnosis
Consider anaphylaxis, contact dermatitis, cellulitis, lymphedema, arthropod bite, hypothyroidism, atopic dermatitis, mastocytosis, granulomatous cheilitis, bullous pemphigoid, urticaria pigmentosa, erythema multiforme, epiglottitis, peritonsillar abscess, parasitic infection, and superior vena cava syndrome.
Workup
A broad workup to identify a cause is frequently unrevealing (about 40%). Testing is guided by the clinical history and exam. Basic tests such as CBC, ESR, and urinalysis may help in initial evaluation. Serum total tryptase can help confirm mast cell–mediated anaphylaxis. C4 is usually low in acquired and hereditary angioedema that occurs without urticaria; when C4 is low, measure C1-INH level and functional activity. Rarely, HAE may present with normal C4 but reduced C1-INH. If food allergy is suspected, skin prick testing and/or in vitro specific IgE testing (e.g., ImmunoCAP) may be used. Skin biopsy is generally reserved for chronic angioedema that is refractory to corticosteroids. Stool ova and parasite testing may be considered when parasitic infection is a concern.
Treatment: Nonpharmacologic Therapy
Remove or eliminate the offending agent when possible and avoid known triggers such as cold, stress, and culprit medications (especially ACE inhibitors). Cold compresses can be applied to affected areas for symptomatic relief.
Acute General Treatment
Life-threatening angioedema involving the larynx is treated urgently, although it is important to recognize that bradykinin-mediated angioedema responds minimally to these standard allergic-reaction medications. Typical emergency medications include subcutaneous epinephrine 0.3 mg (1:1000), an H1 antihistamine such as diphenhydramine 25–50 mg IV/IM or cetirizine 10 mg (listed as IV in the source), an H2 blocker such as cimetidine 300 mg IV or famotidine 20 mg IV, and methylprednisolone 125 mg IV.
For mast cell–mediated, nonhereditary angioedema, maintenance therapy centers on H1 antihistamines: cetirizine 10 mg daily (sometimes up to 4× FDA-approved dose), fexofenadine 180 mg daily (sometimes up to 4× dose), hydroxyzine 10–25 mg every 6 hours, or diphenhydramine 25–50 mg every 6 hours. H2 antihistamines can be added (cimetidine 400 mg twice daily or famotidine 20 mg twice daily). Doxepin 25–50 mg at bedtime can be used as an adjunct. Corticosteroids may be used for symptomatic relief in refractory acute cases. Antihistamines are ineffective for hereditary angioedema attacks.
Acute HAE attacks due to C1 inhibitor deficiency respond well to targeted therapies. Approved abortive options include plasma-derived C1 inhibitor concentrate (Berinert), icatibant (Firazyr), a bradykinin B2 receptor antagonist, and ecallantide (Kalbitor), a kallikrein inhibitor. Purified plasma-derived C1-INH replacement is considered effective and safe for acute attacks.
Chronic Treatment
Chronic histaminergic angioedema is treated similarly to acute management with H1 antihistamines, addition of H2 antihistamines as needed, and corticosteroids reserved for refractory cases. A regimen cited for refractory cases is prednisone 1 mg/kg/day for 5 days followed by a 7-day taper. Omalizumab (anti-IgE monoclonal antibody) has shown benefit in cases refractory to antihistamines, though it is not FDA-approved specifically for this indication.
For hereditary angioedema long-term prophylaxis, older options include androgens (danazol, stanozolol, oxandrolone, methyltestosterone) and antifibrinolytics, but adverse effects can be significant. Intravenous plasma-derived C1 inhibitors (Cinryze, Berinert) are safe and effective for patients with frequent or severe attacks, though cost may limit access. A twice-weekly subcutaneous C1-INH formulation (Haegarda/CSL830) is FDA-approved for HAE-1 and HAE-2. Lanadelumab and berotralstat (kallikrein inhibitors) have FDA approval for prophylaxis of HAE. In a phase 2 trial, donidalorsen (an antisense oligonucleotide that reduces plasma prekallikrein production) lowered attack rates compared with placebo.
Disposition
More than 85% of patients with nonhereditary acute angioedema achieve symptomatic relief with antihistamines. In chronic nonhereditary angioedema, antihistamines remain the mainstay, and systemic steroids should be reserved for severe or refractory cases. Some patients have recurrence after completing treatment. Chronic angioedema can persist for months to years and may be longer in hereditary angioedema.
Referral
Referral to a dermatologist and/or allergist is recommended for chronic angioedema, hereditary angioedema, and recurrent angioedema. HAE is potentially life-threatening and should be managed by an allergist.
Pearls and Considerations
ACE inhibitor–induced angioedema can occur months or even years after starting the drug. ARB-induced angioedema has been reported, though risk is substantially lower than with ACE inhibitors. About 10% of patients with recurrent angioedema had ACE inhibitor exposure, with a median duration of 1 year before symptoms began. Reported incidence rates per 1000 person-years are approximately 4.38 for ACE inhibitors, 1.66 for ARBs, and notably high for the direct renin inhibitor aliskiren (about 4.67).
Comments
Finding a clear cause is often difficult and can be frustrating. Chronic angioedema is rarely due to an allergic reaction, unlike many acute cases. Hereditary angioedema requires specialized care because of its life-threatening potential.
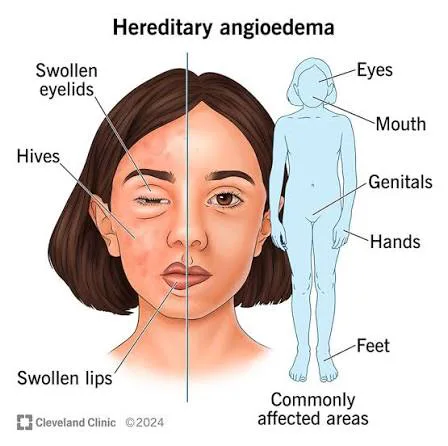
- Published on
KembaraXtra-Medicine – Anaphylaxis
Anaphylaxis is a severe, rapid-onset, life-threatening allergic reaction. It occurs when IgE-mediated and non–IgE-mediated systemic mast cell degranulation leads to release of inflammatory mediators, producing respiratory, cardiovascular, gastrointestinal, and/or mucocutaneous symptoms. A common synonym is anaphylactic reaction. Relevant ICD-10CM codes include T78.2 (anaphylactic shock, unspecified, initial encounter), T78.00XA (anaphylactic reaction due to unspecified food, initial encounter), T80.52XA (anaphylactic reaction due to vaccination, initial encounter), and T63.94XA (toxic effect of contact with unspecified venomous animal, undetermined, initial encounter).
In the United States, the incidence is estimated at 50 to 2000 episodes per 100,000 persons, with a lifetime prevalence of 1.6% to 5.1%. Emergency department visits for anaphylaxis increased by 101% from 2005 to 2014, yet fatalities have remained stable at about 0.7 per million adults per year. In adults, medications and insect stings are leading triggers, while in children and adolescents, foods and insect stings are the leading triggers.
Risk factors depend on the trigger and severity. Atopy increases risk for anaphylaxis triggered by food, exercise, and latex. Risk factors for severe anaphylaxis include cardiovascular disease, asthma, older age, mast cell disorder, beta-blocker use, and ACE inhibitor use.
Clinical presentation commonly includes involvement across multiple systems. Mucocutaneous findings include urticaria, pruritus, flushing, and angioedema. Respiratory symptoms include dyspnea, cough, wheezing, hypoxia, stridor, and rhinitis. Cardiovascular features include hypotension, tachycardia, weakness, dizziness, syncope, malaise, and vascular collapse. Gastrointestinal symptoms include nausea, vomiting, diarrhea, dysphagia, and abdominal pain.
Anaphylaxis results from a sudden systemic release of histamine and other mediators from basophils and mast cells via IgE-dependent and non–IgE-dependent mechanisms, and almost any substance can trigger it. In acute settings, the cause is often not identified, accounting for 30% to 60% of cases. Common triggers include foods and additives (notably peanuts, tree nuts, eggs, shellfish, fish, cow’s milk, fruits, soy). A notable food-related mechanism is alpha-gal syndrome, where a lone star tick bite can cause IgE sensitization to alpha-1,3-galactose, leading to delayed anaphylaxis after eating mammalian (red meat) products. Medication triggers include antibiotics (especially penicillins and sulfa agents), insulin, allergen extracts, opiates, vaccines, NSAIDs, contrast media, streptokinase, immunomodulators, and IV iron. Environmental exposures include bee/wasp stings, snake venom, and fire ant venom. Other triggers include blood products (plasma, immunoglobulin, cryoprecipitate, whole blood), latex, and exercise. Mechanistically, immune (often IgE-mediated) triggers include foods, venoms, many medications, latex, seminal fluid, and sometimes radiocontrast; IgE-independent immune triggers include radiocontrast (in most cases), dextrans, some monoclonal antibodies (e.g., rituximab), and some medications; and nonimmunologic triggers include certain drugs such as opioids and protamine. “Idiopathic” anaphylaxis refers to cases where known causes (including mastocytosis) have been excluded. Non–IgE mechanisms may involve complement activation, kinin production, potentiation, or direct mediator release, and more than one mechanism can occur together (for example, exercise-induced reactions following food). ACE inhibitors are a notable cause of unexplained angioedema, occurring in up to 1 in 200 users and may occur at any time after starting the medication.
The differential diagnosis is broad and includes allergic reactions without anaphylaxis, other causes of shock such as sepsis or pulmonary embolism, endocrine conditions such as carcinoid, adrenal crisis, paradoxical pheochromocytoma, systemic mastocytosis, serum sickness, severe asthma (distinguished by abrupt onset in anaphylaxis versus progressive worsening), scombroid poisoning, localized angioedema, acute urticaria, vasovagal/presyncopal syndromes, airway foreign body, vocal cord dysfunction, and anxiety-related symptoms such as globus hystericus.
Workup is mainly aimed at excluding mimics, but treatment should never be delayed because anaphylaxis can be rapidly fatal. Diagnosis is primarily clinical. Laboratory testing is generally not helpful in the emergency setting, though serum/urine histamine and serum tryptase (drawn 30 minutes to 2 hours after symptom onset and compared with baseline) may support the diagnosis; importantly, normal levels do not exclude anaphylaxis and these tests may not be readily available. Imaging is usually not helpful; chest radiography is considered when evaluating foreign body aspiration or pulmonary pathology in acute respiratory compromise. An ECG should be considered in patients with sudden loss of consciousness, chest pain, dyspnea, and in elderly patients; ECG typically shows sinus tachycardia.
Clinical criteria make anaphylaxis highly likely when any one of the following is met: (1) an acute illness with skin/mucosal involvement plus either respiratory compromise or reduced blood pressure/end-organ dysfunction symptoms; (2) rapid onset of two or more after exposure to a likely allergen--skin/mucosal involvement, respiratory compromise, reduced blood pressure, or persistent GI symptoms such as crampy abdominal pain/vomiting; or (3) reduced blood pressure after exposure to a known allergen--age-specific hypotension or >30% systolic BP decrease in infants/children, or systolic BP <90 mm hg or>30% decrease from baseline in adults.
Immediate nonpharmacologic treatment begins with removing the trigger, rapidly establishing and protecting the airway, providing supplemental oxygen if needed, obtaining IV access, giving IV fluids (normal saline), and placing the patient on cardiac monitoring.
The cornerstone medication is intramuscular epinephrine. Adults and children >30 kg should receive 0.3 to 0.5 mg IM epinephrine (1:1000 concentration) in the anterolateral thigh; anyone >50 kg should receive 0.5 mg IM. Children <30 kg should receive 0.01 mg />g IM epinephrine (1:1000 concentration). IM administration is preferred because it produces a faster and more reliable rise to effective plasma levels, and the dose can be repeated within minutes if symptoms do not improve. Adjunct therapies include H1 and H2 antihistamines such as diphenhydramine and famotidine to improve itching and erythema, but they do not reverse airway obstruction, respiratory compromise, or hypotension, and their onset is delayed 1–2 hours. Corticosteroids do not help acutely because of slow onset and have not been shown to prevent prolonged or biphasic anaphylaxis, but they are commonly used as secondary treatment. Aerosolized beta-agonists help treat bronchospasm. If hypotension or cardiovascular collapse persists despite fluids and IM epinephrine, IV epinephrine (1:10,000 concentration) is used as vasopressor therapy, and small IV boluses may be used in the peri-arrest state. Patients on beta-blockers may respond poorly to initial treatment; in these cases, IV glucagon should be considered.
Disposition depends on severity and risk of recurrence. Patients with mild episodes should be observed for 1 hour after symptom resolution. Patients with severe symptoms—including cyanosis, pulse oximetry <92%, systolic bp <90 mm hg, confusion, loss of consciousness, or incontinence—those needing more than one epinephrine dose, those with a wide pulse pressure, unknown trigger, cutaneous signs />ymptoms, or a medication trigger in children should be observed for at least 6 hours to watch for biphasic anaphylaxis.
For discharge planning and chronic management, patients who are stable and remain asymptomatic should be prescribed two epinephrine autoinjectors, with clear instructions on when and how to use them. Referral to an allergist is helpful when the trigger is unclear in the emergency setting. Patient education is essential: a prior history of anaphylaxis or known triggers is the most reliable way to identify risk. Patients should be instructed to carry an epinephrine device at all times; school-aged children should have an additional autoinjector available at school with appropriate staff. Patients should also be advised to wear or carry MedicAlert identification listing substances that have triggered anaphylaxis. People with prior contrast reactions should avoid radiologic contrast when possible; however, pretreatment regimens with methylprednisolone or diphenhydramine may be used when contrast is unavoidable. For insect-sting anaphylaxis, venom immunotherapy initiated after the event is effective and is recommended for up to 5 years after the incident.