- Published on
Pathology- Antimicrobial agents
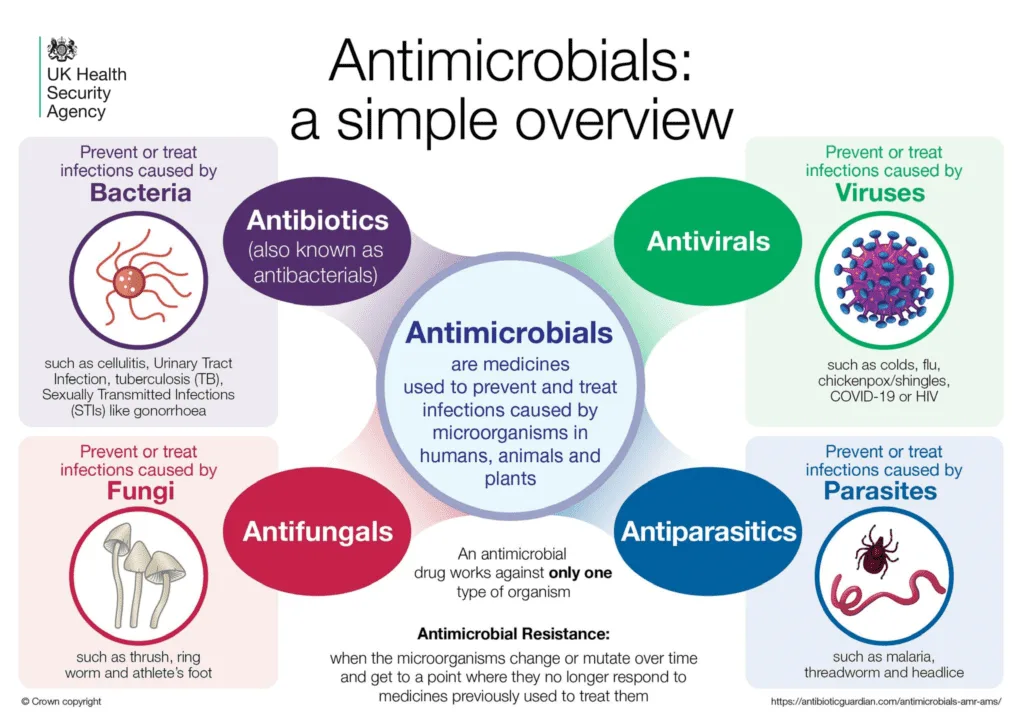
Antibacterial agents
Inhibitors of cellular wall biosynthesis • Disrupt peptidoglycan production. • Beta-lactams, such as penicillins and cephalosporins. • Glycopeptides, such as vancomycin and teicoplanin.
Protein synthesis inhibitors
• Bind to bacterial ribosomes and inhibit the elongation of protein chains. Aminoglycosides, such as gentamicin. • Tetracyclines, such as doxycycline. • Macrolides, such as erythromycin and clarithromycin.
Nucleic acid synthesis inhibitors
• Disrupt the production of DNA precursors or the process of DNA replication. • Sulfonamides, such as sulfamethoxazole. • Trimethoprim. • Quinolones, such as ciprofloxacin. • Rifamycins, such as rifampicin. • Nitroimidazoles, such as metronidazole.
Antiviral medications
Aciclovir is a guanosine analogue that undergoes phosphorylation by viral thymidine kinase. Aciclovir triphosphate is integrated into viral DNA, resulting in the cessation of chain replication. Ganciclovir is analogous to acyclovir, although exhibits more efficacy against cytomegalovirus (CMV). Contemporary HIV treatment employs a mix of reverse transcriptase inhibitors and protease inhibitors.
Antifungal medications
Azoles inhibit the formation of ergosterol, such as fluconazole. Polyenes disrupt the functionality of fungal cell membranes, such as amphotericin and nystatin.
Antibacterial agents
Inhibitors of cellular wall biosynthesis • Disrupt peptidoglycan production. • Beta-lactams, such as penicillins and cephalosporins. • Glycopeptides, such as vancomycin and teicoplanin.
Protein synthesis inhibitors
• Bind to bacterial ribosomes and inhibit the elongation of protein chains. Aminoglycosides, such as gentamicin. • Tetracyclines, such as doxycycline. • Macrolides, such as erythromycin and clarithromycin.
Nucleic acid synthesis inhibitors
• Disrupt the production of DNA precursors or the process of DNA replication. • Sulfonamides, such as sulfamethoxazole. • Trimethoprim. • Quinolones, such as ciprofloxacin. • Rifamycins, such as rifampicin. • Nitroimidazoles, such as metronidazole.
Antiviral medications
Aciclovir is a guanosine analogue that undergoes phosphorylation by viral thymidine kinase. Aciclovir triphosphate is integrated into viral DNA, resulting in the cessation of chain replication. Ganciclovir is analogous to acyclovir, although exhibits more efficacy against cytomegalovirus (CMV). Contemporary HIV treatment employs a mix of reverse transcriptase inhibitors and protease inhibitors.
Antifungal medications
Azoles inhibit the formation of ergosterol, such as fluconazole. Polyenes disrupt the functionality of fungal cell membranes, such as amphotericin and nystatin.
- Published on
Pathology- Adaptive immunity
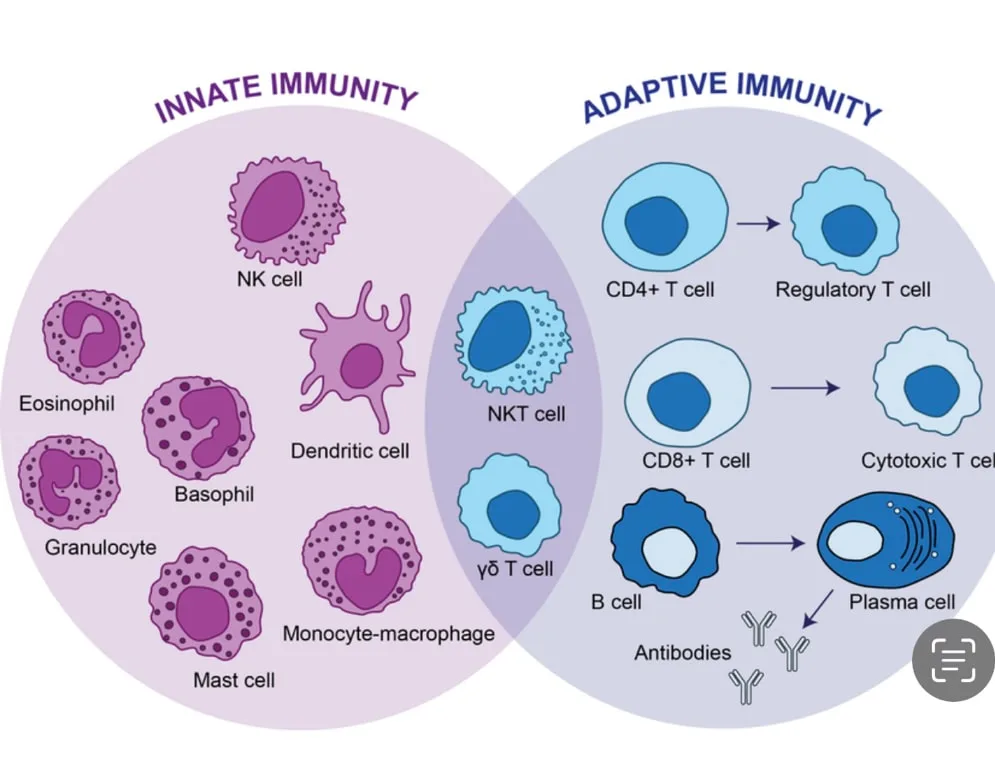
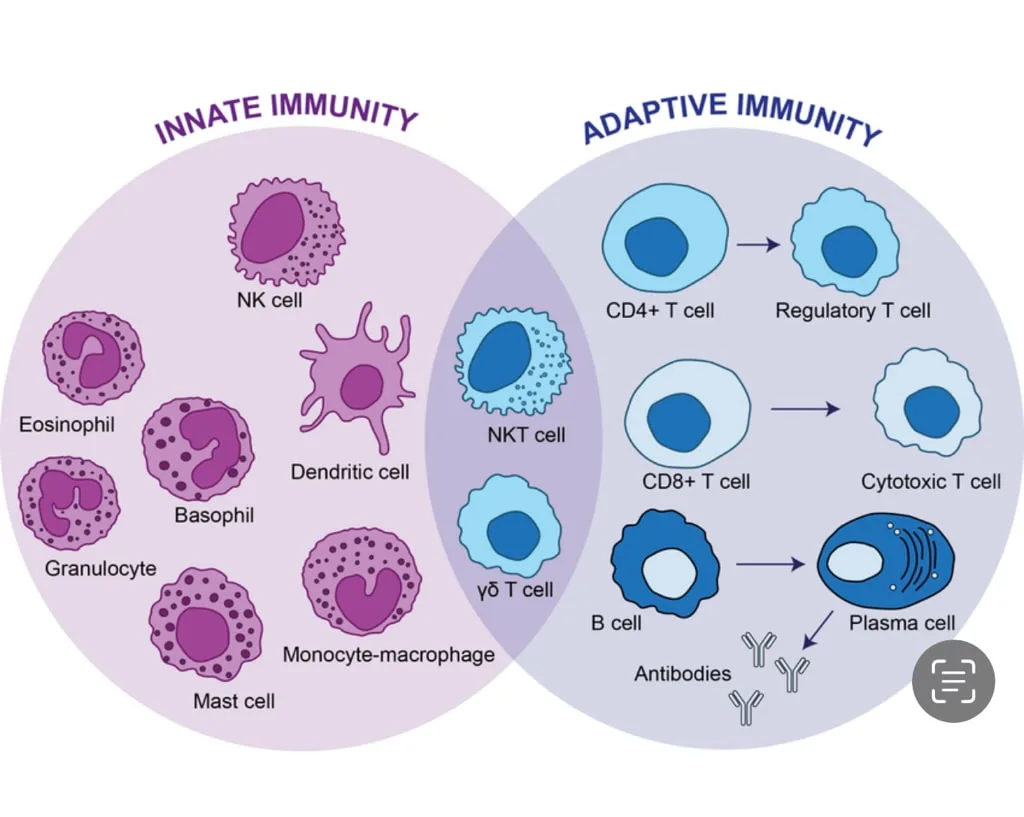
Immunity mediated by antibodies
• Facilitated by proteins known as antibodies or immunoglobulins. The binding of an antigen to the Fab antigen-binding region reveals the binding sites on the Fc section, which facilitates the functions of the antibody. • Antibodies function through four primary mechanisms: • Inhibit the biological function of an essential microbial molecule, such as a binding protein or toxin. • Identify microorganisms for phagocytosis. • Initiate complement. • Stimulate cytotoxic immune cells. Antibody formation commences upon the binding of an antigen to its specific B-cell receptor on the surface of naïve B-lymphocytes, facilitated by an extra signal from CD4+ helper T-lymphocytes.
Cellular immunity • Primarily facilitated by T-lymphocytes (Fig. 1.3). CD4+ helper T-cells are activated by foreign peptides displayed by class II MHC molecules on specialized antigen-presenting cells, including dendritic cells and macrophages. Activated CD4+ helper T-cells undergo proliferation and produce cytokines that facilitate various immunological responses. Numerous subtypes of helper T-cells are identified based on the cytokines they secrete upon activation, including Th1, Th2, Th3, and Th17. CD8+ cytotoxic T-cells are activated by foreign peptides presented by class I MHC, which is expressed by all nucleated cells. Activated CD8+ cytotoxic T-cells eliminate the presenting host cell by either inducing apoptosis via the Fas ligand or by introducing a membrane pore known as perforin, through which the T-cell delivers proteolytic enzymes.
Immunity mediated by antibodies
• Facilitated by proteins known as antibodies or immunoglobulins. The binding of an antigen to the Fab antigen-binding region reveals the binding sites on the Fc section, which facilitates the functions of the antibody. • Antibodies function through four primary mechanisms: • Inhibit the biological function of an essential microbial molecule, such as a binding protein or toxin. • Identify microorganisms for phagocytosis. • Initiate complement. • Stimulate cytotoxic immune cells. Antibody formation commences upon the binding of an antigen to its specific B-cell receptor on the surface of naïve B-lymphocytes, facilitated by an extra signal from CD4+ helper T-lymphocytes.
Cellular immunity • Primarily facilitated by T-lymphocytes (Fig. 1.3). CD4+ helper T-cells are activated by foreign peptides displayed by class II MHC molecules on specialized antigen-presenting cells, including dendritic cells and macrophages. Activated CD4+ helper T-cells undergo proliferation and produce cytokines that facilitate various immunological responses. Numerous subtypes of helper T-cells are identified based on the cytokines they secrete upon activation, including Th1, Th2, Th3, and Th17. CD8+ cytotoxic T-cells are activated by foreign peptides presented by class I MHC, which is expressed by all nucleated cells. Activated CD8+ cytotoxic T-cells eliminate the presenting host cell by either inducing apoptosis via the Fas ligand or by introducing a membrane pore known as perforin, through which the T-cell delivers proteolytic enzymes.
- Published on
Pathology - Hypersensitivity reactions
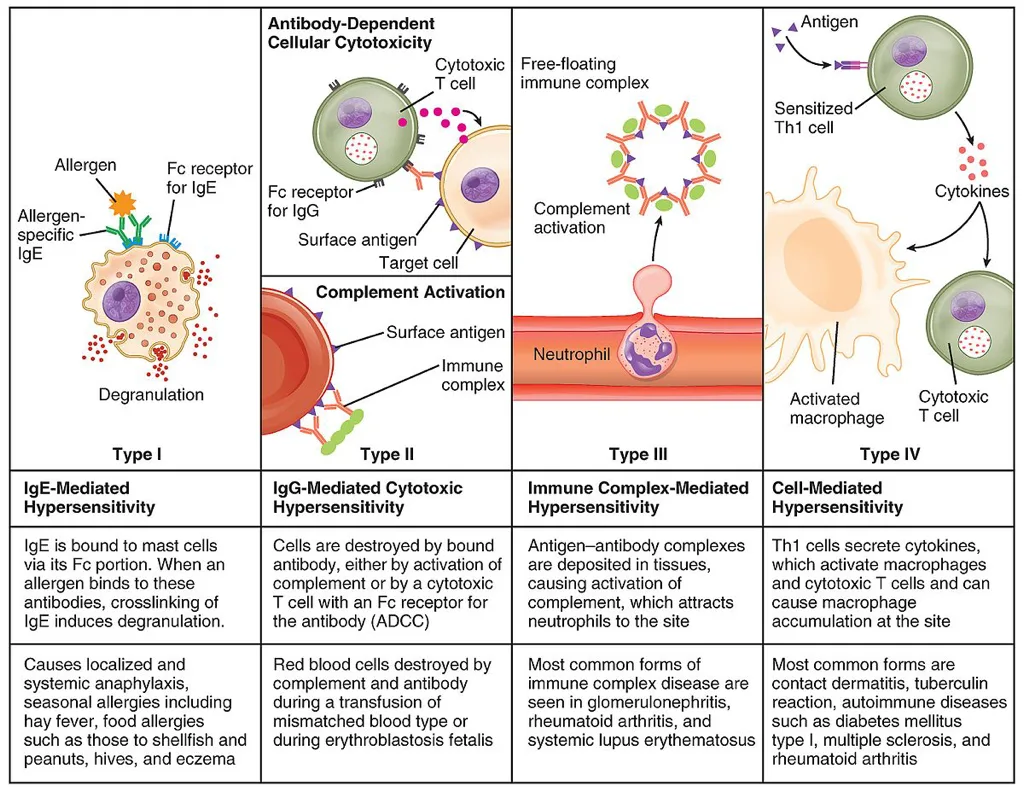
Definition • A collection of disorders resulting from an aberrant immune-mediated response. • This response may target an exogenous antigen from the environment or a self-antigen, in which case it constitutes a kind of autoimmunity.
Type 1 hypersensitivity
• Defined by the synthesis of IgE antibodies in reaction to an antigen. • The cross-linking of surface IgE receptors on mast cells triggers the release of mediators, including histamine, which incite acute inflammation. • Characteristic of individuals with atopy, a hereditary predisposition to generate elevated levels of IgE in reaction to environmental antigens such as pollen and house dust mites. Anaphylaxis is a systemic type of acute hypersensitivity resulting from the extensive release of histamine. In its most extreme manifestation, it may result in anaphylactic shock. • Immediate hypersensitivity disorders impact over 20% of the population, and their prevalence is increasing.
Antibody-mediated (type 2) hypersensitivity is induced by IgG or IgM antibodies attaching to a fixed antigen within a tissue. The binding of antibodies can activate the complement system, resulting in cellular damage, as seen in bullous pemphigoid or induce alterations in cellular function, exemplified by TSH-receptor stimulating antibodies in Graves' disease.
Immune complex-mediated (type 3) hypersensitivity • Arises from circulating IgG or IgM antibodies that form immune complexes with antigens in the bloodstream, subsequently depositing in tissues and activating complement. • Preferred sites for immune complex deposition include small blood vessels, kidneys, and joints. • Reactions characterized by immune complex-mediated hypersensitivity often manifest as multisystem disorders, prominently featuring vasculitis, arthritis, and glomerulonephritis, as observed in systemic lupus erythematosus.
T-cell-mediated (type 4) hypersensitivity is induced by activated T-lymphocytes that damage cells through direct cytotoxicity or by secreting cytokines that stimulate macrophage activation. • T-cell responses are characterized by a latency of 1–2 days, hence the designation delayed-type hypersensitivity. • Illustrative cases encompass contact dermatitisHashimoto’s thyroiditis primary biliary cirrhosisand tuberculosis.
Definition • A collection of disorders resulting from an aberrant immune-mediated response. • This response may target an exogenous antigen from the environment or a self-antigen, in which case it constitutes a kind of autoimmunity.
Type 1 hypersensitivity
• Defined by the synthesis of IgE antibodies in reaction to an antigen. • The cross-linking of surface IgE receptors on mast cells triggers the release of mediators, including histamine, which incite acute inflammation. • Characteristic of individuals with atopy, a hereditary predisposition to generate elevated levels of IgE in reaction to environmental antigens such as pollen and house dust mites. Anaphylaxis is a systemic type of acute hypersensitivity resulting from the extensive release of histamine. In its most extreme manifestation, it may result in anaphylactic shock. • Immediate hypersensitivity disorders impact over 20% of the population, and their prevalence is increasing.
Antibody-mediated (type 2) hypersensitivity is induced by IgG or IgM antibodies attaching to a fixed antigen within a tissue. The binding of antibodies can activate the complement system, resulting in cellular damage, as seen in bullous pemphigoid or induce alterations in cellular function, exemplified by TSH-receptor stimulating antibodies in Graves' disease.
Immune complex-mediated (type 3) hypersensitivity • Arises from circulating IgG or IgM antibodies that form immune complexes with antigens in the bloodstream, subsequently depositing in tissues and activating complement. • Preferred sites for immune complex deposition include small blood vessels, kidneys, and joints. • Reactions characterized by immune complex-mediated hypersensitivity often manifest as multisystem disorders, prominently featuring vasculitis, arthritis, and glomerulonephritis, as observed in systemic lupus erythematosus.
T-cell-mediated (type 4) hypersensitivity is induced by activated T-lymphocytes that damage cells through direct cytotoxicity or by secreting cytokines that stimulate macrophage activation. • T-cell responses are characterized by a latency of 1–2 days, hence the designation delayed-type hypersensitivity. • Illustrative cases encompass contact dermatitisHashimoto’s thyroiditis primary biliary cirrhosisand tuberculosis.
- Published on
Pathology – Innate Immunity
innate immunity
Epithelial interfaces
Epithelial surfaces serve as the primary entry points for infections into the body. A continuous epithelial layer establishes a physical barrier to infection. The acidic pH of the skin and the presence of fatty acids in sebum suppress microbial proliferation.
The gastrointestinal system contains gastric acid, pancreatic enzymes, mucosal IgA, and normal colonic flora that function to inhibit the onset of infection. The respiratory tract produces mucus to capture organisms, while cilia facilitate their passage to the throat for swallowing. Continuous urination along the urinary system inhibits microbial adherence to the urothelium.
Phagocytes
Organisms penetrating epithelial surfaces meet tissue macrophages that identify infections and recruit neutrophils to the location
Macrophages and neutrophils are phagocytic cells that engulf bacteria through phagocytosis, forming a phagosome
The phagosome then merges with cytoplasmic lysosomes, which harbor enzymes and reactive oxygen species that eliminate the bacterium. Phagocytes identify species by pattern recognition receptors, such as mannose receptors, Toll-like receptors, and Nod-like receptors.
Acute-phase proteins
Cytokines generated by phagocytes prompt the liver to swiftly manufacture and discharge acute phase proteins. Mannose-binding lectin identifies microbial surface sugars and undergoes a conformational alteration, enabling it to attach to the protein MASP, thereby forming a complex that activates the complement system.
C-reactive protein attaches to the phosphorylcholine components of microbial lipopolysaccharides, facilitating their phagocytosis by macrophages.
Complement
• A assemblage of circulating proteins that aid the immune system in eliminating pathogens.
• Can be initiated by antibodies attached to a microbe (traditional pathway), automatically activated by bacteria devoid of a regulatory protein found on host cells (alternative pathway), or by mannose-binding protein (lectin pathway). A sequential cascade results in the formation of C3 convertase, an enzyme that cleaves many C3 molecules into C3b.
• Microbes coated with C3b are eliminated through phagocytosis or the membrane assault complex, a polymer of terminal complement components that creates pores in the microbial cell membrane.
• The complement system is stringently regulated to avert unregulated activation. Decay-accelerating factor impedes the binding of C3b to cellular surfaces, while membrane cofactor protein degrades C3b.
innate immunity
Epithelial interfaces
Epithelial surfaces serve as the primary entry points for infections into the body. A continuous epithelial layer establishes a physical barrier to infection. The acidic pH of the skin and the presence of fatty acids in sebum suppress microbial proliferation.
The gastrointestinal system contains gastric acid, pancreatic enzymes, mucosal IgA, and normal colonic flora that function to inhibit the onset of infection. The respiratory tract produces mucus to capture organisms, while cilia facilitate their passage to the throat for swallowing. Continuous urination along the urinary system inhibits microbial adherence to the urothelium.
Phagocytes
Organisms penetrating epithelial surfaces meet tissue macrophages that identify infections and recruit neutrophils to the location
Macrophages and neutrophils are phagocytic cells that engulf bacteria through phagocytosis, forming a phagosome
The phagosome then merges with cytoplasmic lysosomes, which harbor enzymes and reactive oxygen species that eliminate the bacterium. Phagocytes identify species by pattern recognition receptors, such as mannose receptors, Toll-like receptors, and Nod-like receptors.
Acute-phase proteins
Cytokines generated by phagocytes prompt the liver to swiftly manufacture and discharge acute phase proteins. Mannose-binding lectin identifies microbial surface sugars and undergoes a conformational alteration, enabling it to attach to the protein MASP, thereby forming a complex that activates the complement system.
C-reactive protein attaches to the phosphorylcholine components of microbial lipopolysaccharides, facilitating their phagocytosis by macrophages.
Complement
• A assemblage of circulating proteins that aid the immune system in eliminating pathogens.
• Can be initiated by antibodies attached to a microbe (traditional pathway), automatically activated by bacteria devoid of a regulatory protein found on host cells (alternative pathway), or by mannose-binding protein (lectin pathway). A sequential cascade results in the formation of C3 convertase, an enzyme that cleaves many C3 molecules into C3b.
• Microbes coated with C3b are eliminated through phagocytosis or the membrane assault complex, a polymer of terminal complement components that creates pores in the microbial cell membrane.
• The complement system is stringently regulated to avert unregulated activation. Decay-accelerating factor impedes the binding of C3b to cellular surfaces, while membrane cofactor protein degrades C3b.
- Published on
Pathology - Inflammation and Healing
Acute inflammation
• A swift, non-specific reaction to cellular damage
. • Coordinated by cytokines generated from damaged cells, such as histamine, serotonin, prostaglandins, leukotrienes, and platelet-activating factor. Cytokines stimulate endothelial cells, resulting in the development of an acute inflammatory exudate including fluid, fibrin, and neutrophils. Severe acute inflammation may result in a localized accumulation of pus within a necrotic cavity (abscess). Acute inflammation may resolve, heal with fibrosis, or advance to chronic inflammation.
Chronic inflammation is a sustained type of inflammation characterized by concurrent tissue damage and attempts at healing.
• May originate from acute inflammation or manifest from the onset.
• Defined by the presence of chronic inflammatory cells, specifically macrophages, lymphocytes, and plasma cells.
• More prone to healing with permanent scarring rather than resolution.
Granulomatous inflammation is a distinct form of chronic inflammation marked by the presence of activated macrophages referred to as epithelioid histiocytes. Collections of epithelioid macrophages are referred to as granulomas. Granulomatous inflammation is linked to foreign substances, chronic infections (such as mycobacteria), and conditions of indeterminate etiology (for instance, sarcoidosis).
Restoration
• The procedure of substituting necrotic and impaired tissue with viable tissue
. • May transpire via regeneration or repair. Regeneration (resolution) substitutes injured cells with identical cell types and represents the optimal outcome. This can only happen if the connective tissue framework is intact and if the tissue possesses regenerative capabilities. Repair initiates with the development of granulation tissue, subsequently transformed into a collagen-dense scar. While the structural integrity is preserved, the functionality of the damaged tissue is compromised.
Acute inflammation
• A swift, non-specific reaction to cellular damage
. • Coordinated by cytokines generated from damaged cells, such as histamine, serotonin, prostaglandins, leukotrienes, and platelet-activating factor. Cytokines stimulate endothelial cells, resulting in the development of an acute inflammatory exudate including fluid, fibrin, and neutrophils. Severe acute inflammation may result in a localized accumulation of pus within a necrotic cavity (abscess). Acute inflammation may resolve, heal with fibrosis, or advance to chronic inflammation.
Chronic inflammation is a sustained type of inflammation characterized by concurrent tissue damage and attempts at healing.
• May originate from acute inflammation or manifest from the onset.
• Defined by the presence of chronic inflammatory cells, specifically macrophages, lymphocytes, and plasma cells.
• More prone to healing with permanent scarring rather than resolution.
Granulomatous inflammation is a distinct form of chronic inflammation marked by the presence of activated macrophages referred to as epithelioid histiocytes. Collections of epithelioid macrophages are referred to as granulomas. Granulomatous inflammation is linked to foreign substances, chronic infections (such as mycobacteria), and conditions of indeterminate etiology (for instance, sarcoidosis).
Restoration
• The procedure of substituting necrotic and impaired tissue with viable tissue
. • May transpire via regeneration or repair. Regeneration (resolution) substitutes injured cells with identical cell types and represents the optimal outcome. This can only happen if the connective tissue framework is intact and if the tissue possesses regenerative capabilities. Repair initiates with the development of granulation tissue, subsequently transformed into a collagen-dense scar. While the structural integrity is preserved, the functionality of the damaged tissue is compromised.
- Published on
Pathology - Cellular death
Necrosis is an inadequately regulated kind of cell death characterized by the loss of membrane integrity, resulting in the spilling of cellular contents and an inflammatory reaction.
• Coagulative necrosis is the predominant type, marked by the absence of cell nuclei while maintaining the overall structural integrity. The necrotic tissue appears macroscopically pale and firm.
Liquefactive necrosis results in the total destruction of cellular architecture, transforming it into a mushy, semi-solid mass. This is commonly observed in the brain subsequent to cerebral infarction.
Caseous necrosis is a form of necrosis characterized by dead tissue that macroscopically resembles cream cheese. It can manifest in several diseases, but is predominantly linked to tuberculosis.
• Gangrene denotes necrotic tissues altered by air exposure, leading to desiccation (dry gangrene) or infection (wet gangrene). In cases of critical limb ischaemia, toes that experience blood deprivation typically exhibit dry gangrene.
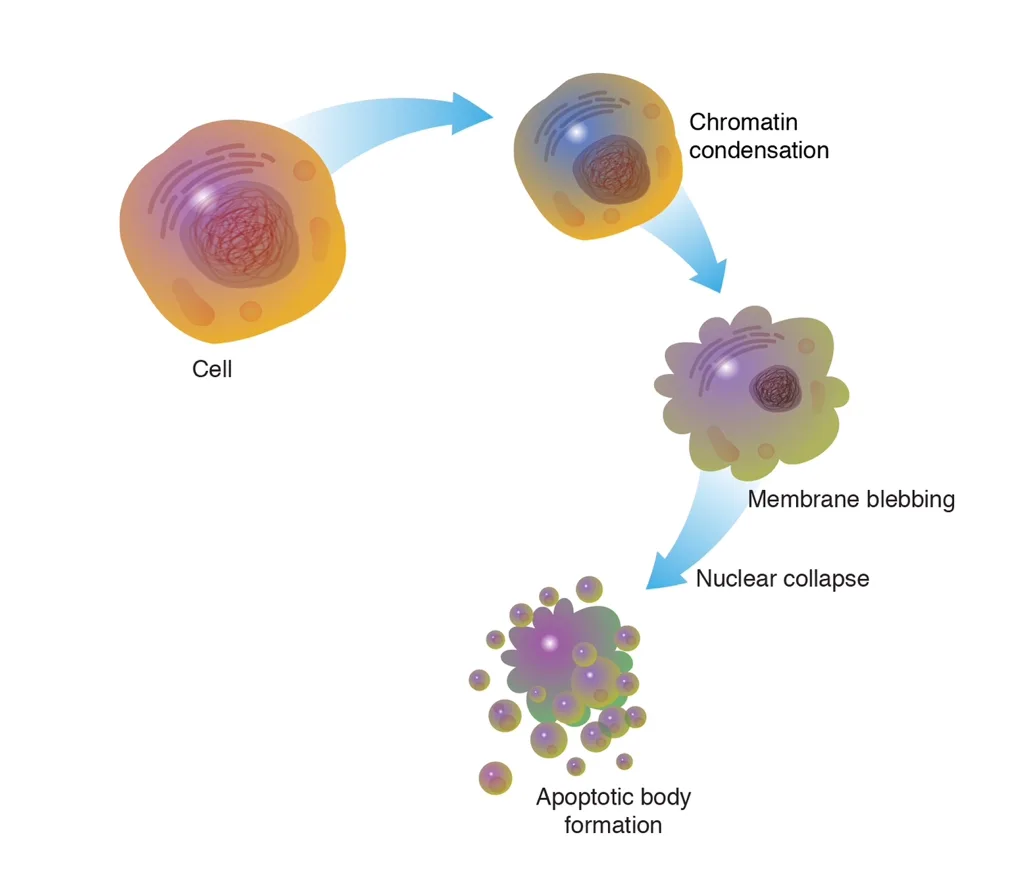
Apoptosis is a regulated process of cellular demise when no intracellular components are expelled from the dying cell, hence preventing any inflammatory response. Apoptosis can occur naturally, such as in the elimination of cells during embryogenesis and those with DNA damage, or pathologically. Apoptosis can be initiated via two primary mechanisms: the activation of surface death receptors, such as Fas or TNF-α (extrinsic pathway), or through cellular damage (intrinsic pathway). The final outcome is the activation of protease enzymes known as caspases, which deconstruct the cell's cytoplasm and nucleus.
Apoptotic cells undergo shrinkage and fragmentation into apoptotic bodies, each maintaining an unbroken cell membrane. • Apoptotic entities are promptly eliminated by neighboring cells. • Dysregulated apoptosis is believed to play a crucial role in various significant disease mechanisms, especially carcinogenesis.
Necrosis is an inadequately regulated kind of cell death characterized by the loss of membrane integrity, resulting in the spilling of cellular contents and an inflammatory reaction.
• Coagulative necrosis is the predominant type, marked by the absence of cell nuclei while maintaining the overall structural integrity. The necrotic tissue appears macroscopically pale and firm.
Liquefactive necrosis results in the total destruction of cellular architecture, transforming it into a mushy, semi-solid mass. This is commonly observed in the brain subsequent to cerebral infarction.
Caseous necrosis is a form of necrosis characterized by dead tissue that macroscopically resembles cream cheese. It can manifest in several diseases, but is predominantly linked to tuberculosis.
• Gangrene denotes necrotic tissues altered by air exposure, leading to desiccation (dry gangrene) or infection (wet gangrene). In cases of critical limb ischaemia, toes that experience blood deprivation typically exhibit dry gangrene.
Apoptosis is a regulated process of cellular demise when no intracellular components are expelled from the dying cell, hence preventing any inflammatory response. Apoptosis can occur naturally, such as in the elimination of cells during embryogenesis and those with DNA damage, or pathologically. Apoptosis can be initiated via two primary mechanisms: the activation of surface death receptors, such as Fas or TNF-α (extrinsic pathway), or through cellular damage (intrinsic pathway). The final outcome is the activation of protease enzymes known as caspases, which deconstruct the cell's cytoplasm and nucleus.
Apoptotic cells undergo shrinkage and fragmentation into apoptotic bodies, each maintaining an unbroken cell membrane. • Apoptotic entities are promptly eliminated by neighboring cells. • Dysregulated apoptosis is believed to play a crucial role in various significant disease mechanisms, especially carcinogenesis.
- Published on
Terminology of pathology
Nomenclature of diseases
Aetiology denotes the fundamental cause of an illness. Diseases with an unclear aetiology are termed idiopathic, cryptogenic, or essential.
Pathogenesis denotes the mechanism via which the etiological agent induces the signs of a disease.
Incidence denotes the quantity of newly diagnosed instances of an illness within a specified timeframe.
Prevalence denotes the aggregate number of disease cases within a community at a specific point in time.
Prognosis refers to the anticipated progression of an illness.
Morbidity refers to the degree to which a patient's overall health is impacted by a condition. •
Mortality indicates the probability of mortality due to a specific disease
.Acute and chronic denote the temporal progression of a disease occurrence. Acute diseases manifest abruptly.
Chronic illnesses typically exhibit a gradual onset and are more prone to a protracted duration.
A syndrome denotes a collection of symptoms and clinical indications that, when present concurrently, indicate a certain underlying cause(s).
Classification of diseases
Genetic disorders are hereditary conditions resulting from a faulty gene, such as cystic fibrosis.
Infectious disorders arise from the invasion of the body by pathogenic microorganisms, such as malaria.
Inflammatory disorders result from excessive activity of inflammatory cells in an organ, such as rheumatoid arthritis.
Neoplastic illness arises from the unregulated proliferation of cells, such as breast cancer.
• Vascular diseases occur as a result of blood vessel disorders, such as ischemic heart disease.
• Metabolic disorders stem from abnormalities in metabolic processes, such as diabetes mellitus.
Degenerative diseases arise from the destruction and/or loss of specialized cells, such as the loss of neurons from the cerebral cortex in Alzheimer's disease. Iatrogenic disease arises from the consequences of medical treatment, such as osteoporosis resulting from prolonged glucocorticoid therapy
. • Congenital disorders are present at birth, while those that arise postnatally are termed acquired diseases.
Nomenclature of diseases
Aetiology denotes the fundamental cause of an illness. Diseases with an unclear aetiology are termed idiopathic, cryptogenic, or essential.
Pathogenesis denotes the mechanism via which the etiological agent induces the signs of a disease.
Incidence denotes the quantity of newly diagnosed instances of an illness within a specified timeframe.
Prevalence denotes the aggregate number of disease cases within a community at a specific point in time.
Prognosis refers to the anticipated progression of an illness.
Morbidity refers to the degree to which a patient's overall health is impacted by a condition. •
Mortality indicates the probability of mortality due to a specific disease
.Acute and chronic denote the temporal progression of a disease occurrence. Acute diseases manifest abruptly.
Chronic illnesses typically exhibit a gradual onset and are more prone to a protracted duration.
A syndrome denotes a collection of symptoms and clinical indications that, when present concurrently, indicate a certain underlying cause(s).
Classification of diseases
Genetic disorders are hereditary conditions resulting from a faulty gene, such as cystic fibrosis.
Infectious disorders arise from the invasion of the body by pathogenic microorganisms, such as malaria.
Inflammatory disorders result from excessive activity of inflammatory cells in an organ, such as rheumatoid arthritis.
Neoplastic illness arises from the unregulated proliferation of cells, such as breast cancer.
• Vascular diseases occur as a result of blood vessel disorders, such as ischemic heart disease.
• Metabolic disorders stem from abnormalities in metabolic processes, such as diabetes mellitus.
Degenerative diseases arise from the destruction and/or loss of specialized cells, such as the loss of neurons from the cerebral cortex in Alzheimer's disease. Iatrogenic disease arises from the consequences of medical treatment, such as osteoporosis resulting from prolonged glucocorticoid therapy
. • Congenital disorders are present at birth, while those that arise postnatally are termed acquired diseases.
- Published on
Pathology - Cellular modifications
Atrophy
• A decrease in the dimensions of a tissue or organ.
• Can result from a decrease in cell quantity by death or a loss in cell volume through shrinkage.
• Atrophy can manifest as a natural physiological phenomenon, such as thymic atrophy throughout puberty and ovarian atrophy during menopause. Pathological atrophy examples encompass muscle atrophy resulting from denervation and cerebral atrophy caused by cerebrovascular illness.
Hypertrophy
An augmentation in the dimensions of individual cells.
• As a result of an augmentation of cellular proteins and organelles.
• Observed in organs with terminally differentiated cells that are incapable of proliferation, such as cardiac and skeletal muscle. Examples of physiological hypertrophy encompass the myometrium of the uterus during pregnancy and the musculature of a bodybuilder. Pathological hypertrophy examples encompass left ventricular hypertrophy resulting from hypertension or aortic stenosis.
Hyperplasia
• An augmentation in cellular quantity. Examples of physiological hyperplasia encompass the endometrium and breast lobules in reaction to cyclical estrogen stimulation. Pathological hyperplasia examples include benign prostatic hyperplasia and parathyroid hyperplasia.
Metaplasia
A transformation in which one cellular type is replaced by another. • Considered to arise from progenitor cells differentiating into a novel cell type rather than through direct morphogenesis from one cell type to another. • Predominantly observed in epithelial cells, frequently as a reaction to chronic injury. • Metaplasia is designated based on the newly formed cell type; for instance, a transition from non-squamous to squamous epithelium is referred to as squamous metaplasia. Common locations of squamous metaplasia encompass the endocervix, forming the transformation zone associated with cervical neoplasia, and the bronchi of smokers. Common locations of glandular metaplasia encompass the lower esophagus in certain individuals with reflux illness, resulting in a discernible Barrett's esophagus.
Metaplasia serves as an indicator of chronic epithelial injury that may, in certain instances, progress to epithelial dysplasia and ultimately cancer.
Atrophy
• A decrease in the dimensions of a tissue or organ.
• Can result from a decrease in cell quantity by death or a loss in cell volume through shrinkage.
• Atrophy can manifest as a natural physiological phenomenon, such as thymic atrophy throughout puberty and ovarian atrophy during menopause. Pathological atrophy examples encompass muscle atrophy resulting from denervation and cerebral atrophy caused by cerebrovascular illness.
Hypertrophy
An augmentation in the dimensions of individual cells.
• As a result of an augmentation of cellular proteins and organelles.
• Observed in organs with terminally differentiated cells that are incapable of proliferation, such as cardiac and skeletal muscle. Examples of physiological hypertrophy encompass the myometrium of the uterus during pregnancy and the musculature of a bodybuilder. Pathological hypertrophy examples encompass left ventricular hypertrophy resulting from hypertension or aortic stenosis.
Hyperplasia
• An augmentation in cellular quantity. Examples of physiological hyperplasia encompass the endometrium and breast lobules in reaction to cyclical estrogen stimulation. Pathological hyperplasia examples include benign prostatic hyperplasia and parathyroid hyperplasia.
Metaplasia
A transformation in which one cellular type is replaced by another. • Considered to arise from progenitor cells differentiating into a novel cell type rather than through direct morphogenesis from one cell type to another. • Predominantly observed in epithelial cells, frequently as a reaction to chronic injury. • Metaplasia is designated based on the newly formed cell type; for instance, a transition from non-squamous to squamous epithelium is referred to as squamous metaplasia. Common locations of squamous metaplasia encompass the endocervix, forming the transformation zone associated with cervical neoplasia, and the bronchi of smokers. Common locations of glandular metaplasia encompass the lower esophagus in certain individuals with reflux illness, resulting in a discernible Barrett's esophagus.
Metaplasia serves as an indicator of chronic epithelial injury that may, in certain instances, progress to epithelial dysplasia and ultimately cancer.
- Published on
Medical Physiology - Fundamental Mechanism of Muscle Contraction
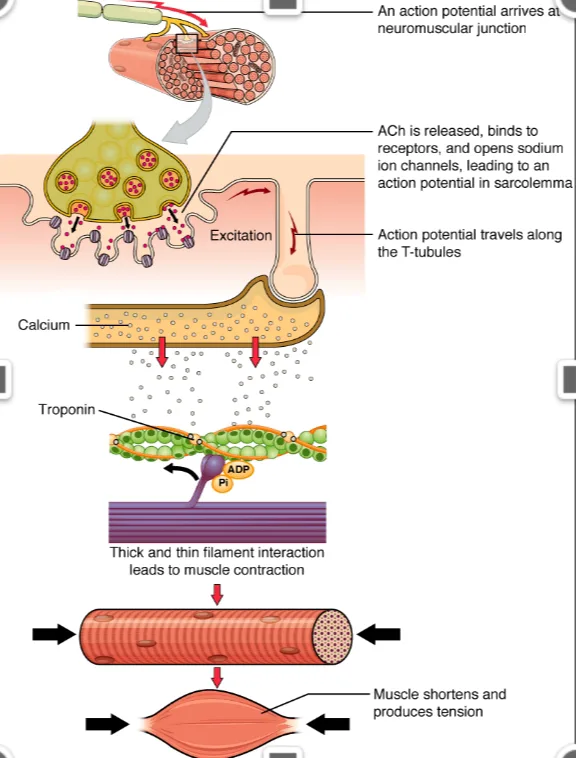
The commencement and implementation of muscular contraction transpire in the subsequent sequential steps: 1. An action potential propagates along a motor neuron to its terminals on muscle fibers, where each terminal releases a minute quantity of the neurotransmitter acetylcholine. 2. Acetylcholine interacts with a specific region of the muscular membrane to activate acetylcholine-gated cation channels, permitting primarily sodium ions, along with calcium ions, to enter the muscle fiber, resulting in localized depolarization. The local depolarization subsequently causes the opening of voltage-gated sodium channels, culminating in an action potential. The action potential propagates over the muscle fiber membrane, prompting the sarcoplasmic reticulum to release calcium ions into the myofibrils that were previously stored in the sarcoplasmic reticulum. 4. Calcium ions instigate attractive interactions between the actin and myosin filaments, resulting in their sliding together; this constitutes the contractile process. 5. Calcium ions are continuously transported back into the sarcoplasmic reticulum, where they are stored until a muscular action potential occurs; this expulsion of calcium ions from the myofibrils results in the cessation of muscle
contraction.
The commencement and implementation of muscular contraction transpire in the subsequent sequential steps: 1. An action potential propagates along a motor neuron to its terminals on muscle fibers, where each terminal releases a minute quantity of the neurotransmitter acetylcholine. 2. Acetylcholine interacts with a specific region of the muscular membrane to activate acetylcholine-gated cation channels, permitting primarily sodium ions, along with calcium ions, to enter the muscle fiber, resulting in localized depolarization. The local depolarization subsequently causes the opening of voltage-gated sodium channels, culminating in an action potential. The action potential propagates over the muscle fiber membrane, prompting the sarcoplasmic reticulum to release calcium ions into the myofibrils that were previously stored in the sarcoplasmic reticulum. 4. Calcium ions instigate attractive interactions between the actin and myosin filaments, resulting in their sliding together; this constitutes the contractile process. 5. Calcium ions are continuously transported back into the sarcoplasmic reticulum, where they are stored until a muscular action potential occurs; this expulsion of calcium ions from the myofibrils results in the cessation of muscle
contraction.
- Published on
Medical Physiology - Physiological Anatomy of Skeletal Muscle
ZApproximately 40% of body mass comprises skeletal muscle, with an additional 10% consisting of smooth and cardiac muscle. Numerous concepts of contraction are applicable to all three muscle types. Skeletal Muscle Fiber In the majority of muscles, the fibers span the full length of the muscle. Each fiber is innervated by a single nerve terminal. Myofibrils consist of actin and myosin filaments. Each muscle fiber comprises hundreds to thousands of myofibrils, with each myofibril consisting of approximately 1500 myosin filaments and 3000 actin filaments arranged laterally. These filaments are substantial polymerized protein molecules that facilitate muscle contraction. The thick filaments consist of myosin, whereas the thin filaments comprise actin; observe the subsequent characteristics:
• light and dark bands.
The myosin and actin filaments partially interdigitate, resulting in the myofibrils exhibiting alternating bright and dark bands. The light bands consist solely of actin filaments and are referred to as I bands. The dark regions known as A bands comprise myosin filaments along with the terminal portions of actin filaments. The A band length corresponds to the length of the myosin filament
. • Cross-bridges. The diminutive extensions from the myosin filament sides are termed cross-bridges. They extend from the surfaces of the myosin filament over its whole length, with the exception of the core. Myosin cross-bridges engage with actin filaments, resulting in contraction.
• Z the disc. The termini of the actin filaments are affixed to Z discs.The Z disc traverses the myofibril, connecting and aligning the myofibrils throughout the muscle fiber.
The complete muscle fiber exhibits alternating light and dark bands, resulting in a striated appearance in skeletal and cardiac muscle.
• Sarcomere. The segment of a myofibril situated between two consecutive Z discs is referred to as a sarcomere. At rest, actin filaments exhibit ideal interdigitation with myosin filaments in skeletal muscle, while in cardiac muscle, the interdigitation is somewhat less than optimal.
ZApproximately 40% of body mass comprises skeletal muscle, with an additional 10% consisting of smooth and cardiac muscle. Numerous concepts of contraction are applicable to all three muscle types. Skeletal Muscle Fiber In the majority of muscles, the fibers span the full length of the muscle. Each fiber is innervated by a single nerve terminal. Myofibrils consist of actin and myosin filaments. Each muscle fiber comprises hundreds to thousands of myofibrils, with each myofibril consisting of approximately 1500 myosin filaments and 3000 actin filaments arranged laterally. These filaments are substantial polymerized protein molecules that facilitate muscle contraction. The thick filaments consist of myosin, whereas the thin filaments comprise actin; observe the subsequent characteristics:
• light and dark bands.
The myosin and actin filaments partially interdigitate, resulting in the myofibrils exhibiting alternating bright and dark bands. The light bands consist solely of actin filaments and are referred to as I bands. The dark regions known as A bands comprise myosin filaments along with the terminal portions of actin filaments. The A band length corresponds to the length of the myosin filament
. • Cross-bridges. The diminutive extensions from the myosin filament sides are termed cross-bridges. They extend from the surfaces of the myosin filament over its whole length, with the exception of the core. Myosin cross-bridges engage with actin filaments, resulting in contraction.
• Z the disc. The termini of the actin filaments are affixed to Z discs.The Z disc traverses the myofibril, connecting and aligning the myofibrils throughout the muscle fiber.
The complete muscle fiber exhibits alternating light and dark bands, resulting in a striated appearance in skeletal and cardiac muscle.
• Sarcomere. The segment of a myofibril situated between two consecutive Z discs is referred to as a sarcomere. At rest, actin filaments exhibit ideal interdigitation with myosin filaments in skeletal muscle, while in cardiac muscle, the interdigitation is somewhat less than optimal.

