- Published on
Infectious Disease -Adenovirus Infections
OVERVIEW
• Adenovirus infections are induced by double-stranded DNA viruses ranging from 70 to 80 nm in diameter. • Human adenoviruses are classified within the genus Mastadenovirus, with more than 50 serotypes.
EPIDEMIOLOGY Incidence • 80% of acute respiratory sickness cases are attributable to viral infections, predominantly rhinovirus, with adenovirus occurring less frequently. • Infections are most prevalent from autumn to spring.
RISK FACTORS • Adenovirus infection may be transmitted through inhalation of aerosolized virus, injection into conjunctival sacs, and likely via the fecal-oral pathway.
Adenoviruses are responsible for up to 5% of acute respiratory infections in children, but they account for less than 2% of respiratory disorders in adults.
• Specific adenovirus serotypes are linked to outbreaks of acute respiratory illness among military recruits during the winter and spring seasons.
• Antibodies are produced following infection and confer protection against reinfection with the same serotype. • Adenoviruses have been linked to disseminated disease and pneumonia in immunocompromised individuals, including those with AIDS, recipients of solid organ or bone marrow transplants, and children with congenital immunodeficiency syndromes.
The etiology of adenoviruses is defined by their distinctive morphology, which features an icosahedral shell made up of 20 equilateral triangular faces and 12 vertices.
Human adenoviruses are classified into six subgenera (A to F) based on DNA genome homology and other characteristics.
The adenovirus genome is a linear double-stranded DNA that encodes structural and nonstructural polypeptides. The replicative cycle of adenovirus can lead to either lytic infection of cells or the creation of a latent infection. • Certain viral strains can provoke oncogenic transformation. Tumor development has been shown in animals.
DIAGNOSTIC HISTORY
Adenoviruses induce various clinical disorders in children. The most prevalent condition is an acute upper respiratory tract infection characterized by significant rhinitis.
• Occasionally, lower respiratory tract diseases such as bronchiolitis and pneumonia manifest.
Adenoviruses can induce pharyngoconjunctival fever, a distinct acute febrile condition in children that typically manifests during outbreaks, predominantly at summer camps. A low-grade fever typically occurs during the initial 3–5 days, succeeded by rhinitis, pharyngitis, and cervical lymphadenopathy. The ailment often endures for 1 to 2 weeks and fades autonomously.
Pharyngitis has been linked to viral infection.
• In adults, acute respiratory disease has been the most commonly reported ailment. This ailment is characterized by a significant painful throat and a slow emergence of fever, frequently attaining 39°C. Cough is typically prevalent, and coryza along with regional lymphadenopathy is often observed.
Adenoviruses may also induce non-respiratory tract infections. Diseases: – Acute diarrheal sickness in young infants – Hemorrhagic cystitis – Epidemic keratoconjunctivitis
Immunocompromised patients with adenovirus pneumonia may exhibit a sudden onset of fever, chills, malaise, nonproductive cough, nausea, vomiting, diarrhea, abdominal discomfort, headache, and joint pain.
PHYSICAL EXAMINATION
• The physical examination may reveal pharyngeal edema, erythema, and tonsillar hypertrophy with minimal or absent exudate.
• In immunocompromised individuals, regional physical examination findings may be absent.
– Individuals with eye disorders may exhibit conjunctival irritation accompanied by discharge.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
Preliminary laboratory examinations
A conclusive diagnosis of adenovirus infection is determined by cultural methods or the identification of the virus from locations such as the conjunctiva and oropharynx, or from sputum, urine, or feces.
• Viruses can be recognized in tissue culture through cytopathic alterations and particularly characterized using immunofluorescence or other immunological methods.
• Adenovirus strains linked to diarrheal illness in children necessitate specific tissue-culture cells for isolation or are detected using direct ELISA of stool samples. • Increases in serum antibodies can be evidenced through complement-fixation or neutralization assays, ELISA, or radioimmunoassay.
Imaging
Adenovirus pneumonia typically presents on chest radiographs as bilateral, diffuse interstitial infiltrates, with infrequent pleural effusions.
DIFFERENTIAL DIAGNOSIS
In many instances, diseases resulting from adenovirus infection cannot be distinguished from those caused by many other viral respiratory pathogens like Mycoplasma pneumoniae.
THERAPEUTIC PHARMACEUTICAL
Only symptomatic treatment and supportive therapy are available for adenovirus infections.
Live vaccinations have been created for adenovirus types 4 and 7 (given as live, unattenuated virus in enteric-coated capsules) and are utilized to manage outbreaks among military recruits. The management of adenovirus infections in immunocompromised individuals is typically supportive.
• • •
Severe adenovirus infections in immunocompromised individuals may be treated with cidofovir and a single administration of intravenous immunoglobulin. Intravenous gamma globulin has been utilized in the management of adenovirus infections in transplant recipients and immunocompromised individuals, with type-specific antibodies potentially contributing to the therapy of this illness.
Ribavirin or ganciclovir has been effectively utilized for treating adenovirus infections in both immunocompromised and immunocompetent individuals; nevertheless, the evidence supporting its efficiency is restricted to case studies.
CONTINUING CARE COMPLICATIONS
Adenovirus pneumonia in transplant recipients and immunocompromised individuals is linked to considerable morbidity and mortality, perhaps surpassing 60%.
ICD-9 CODES • 008.62 Enteritis attributable to adenovirus • 079.0 Adenovirus infection in conditions categorized elsewhere and of undetermined location • 480.0 Pneumonia resulting from adenovirus
OVERVIEW
• Adenovirus infections are induced by double-stranded DNA viruses ranging from 70 to 80 nm in diameter. • Human adenoviruses are classified within the genus Mastadenovirus, with more than 50 serotypes.
EPIDEMIOLOGY Incidence • 80% of acute respiratory sickness cases are attributable to viral infections, predominantly rhinovirus, with adenovirus occurring less frequently. • Infections are most prevalent from autumn to spring.
RISK FACTORS • Adenovirus infection may be transmitted through inhalation of aerosolized virus, injection into conjunctival sacs, and likely via the fecal-oral pathway.
Adenoviruses are responsible for up to 5% of acute respiratory infections in children, but they account for less than 2% of respiratory disorders in adults.
• Specific adenovirus serotypes are linked to outbreaks of acute respiratory illness among military recruits during the winter and spring seasons.
• Antibodies are produced following infection and confer protection against reinfection with the same serotype. • Adenoviruses have been linked to disseminated disease and pneumonia in immunocompromised individuals, including those with AIDS, recipients of solid organ or bone marrow transplants, and children with congenital immunodeficiency syndromes.
The etiology of adenoviruses is defined by their distinctive morphology, which features an icosahedral shell made up of 20 equilateral triangular faces and 12 vertices.
Human adenoviruses are classified into six subgenera (A to F) based on DNA genome homology and other characteristics.
The adenovirus genome is a linear double-stranded DNA that encodes structural and nonstructural polypeptides. The replicative cycle of adenovirus can lead to either lytic infection of cells or the creation of a latent infection. • Certain viral strains can provoke oncogenic transformation. Tumor development has been shown in animals.
DIAGNOSTIC HISTORY
Adenoviruses induce various clinical disorders in children. The most prevalent condition is an acute upper respiratory tract infection characterized by significant rhinitis.
• Occasionally, lower respiratory tract diseases such as bronchiolitis and pneumonia manifest.
Adenoviruses can induce pharyngoconjunctival fever, a distinct acute febrile condition in children that typically manifests during outbreaks, predominantly at summer camps. A low-grade fever typically occurs during the initial 3–5 days, succeeded by rhinitis, pharyngitis, and cervical lymphadenopathy. The ailment often endures for 1 to 2 weeks and fades autonomously.
Pharyngitis has been linked to viral infection.
• In adults, acute respiratory disease has been the most commonly reported ailment. This ailment is characterized by a significant painful throat and a slow emergence of fever, frequently attaining 39°C. Cough is typically prevalent, and coryza along with regional lymphadenopathy is often observed.
Adenoviruses may also induce non-respiratory tract infections. Diseases: – Acute diarrheal sickness in young infants – Hemorrhagic cystitis – Epidemic keratoconjunctivitis
Immunocompromised patients with adenovirus pneumonia may exhibit a sudden onset of fever, chills, malaise, nonproductive cough, nausea, vomiting, diarrhea, abdominal discomfort, headache, and joint pain.
PHYSICAL EXAMINATION
• The physical examination may reveal pharyngeal edema, erythema, and tonsillar hypertrophy with minimal or absent exudate.
• In immunocompromised individuals, regional physical examination findings may be absent.
– Individuals with eye disorders may exhibit conjunctival irritation accompanied by discharge.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
Preliminary laboratory examinations
A conclusive diagnosis of adenovirus infection is determined by cultural methods or the identification of the virus from locations such as the conjunctiva and oropharynx, or from sputum, urine, or feces.
• Viruses can be recognized in tissue culture through cytopathic alterations and particularly characterized using immunofluorescence or other immunological methods.
• Adenovirus strains linked to diarrheal illness in children necessitate specific tissue-culture cells for isolation or are detected using direct ELISA of stool samples. • Increases in serum antibodies can be evidenced through complement-fixation or neutralization assays, ELISA, or radioimmunoassay.
Imaging
Adenovirus pneumonia typically presents on chest radiographs as bilateral, diffuse interstitial infiltrates, with infrequent pleural effusions.
DIFFERENTIAL DIAGNOSIS
In many instances, diseases resulting from adenovirus infection cannot be distinguished from those caused by many other viral respiratory pathogens like Mycoplasma pneumoniae.
THERAPEUTIC PHARMACEUTICAL
Only symptomatic treatment and supportive therapy are available for adenovirus infections.
Live vaccinations have been created for adenovirus types 4 and 7 (given as live, unattenuated virus in enteric-coated capsules) and are utilized to manage outbreaks among military recruits. The management of adenovirus infections in immunocompromised individuals is typically supportive.
• • •
Severe adenovirus infections in immunocompromised individuals may be treated with cidofovir and a single administration of intravenous immunoglobulin. Intravenous gamma globulin has been utilized in the management of adenovirus infections in transplant recipients and immunocompromised individuals, with type-specific antibodies potentially contributing to the therapy of this illness.
Ribavirin or ganciclovir has been effectively utilized for treating adenovirus infections in both immunocompromised and immunocompetent individuals; nevertheless, the evidence supporting its efficiency is restricted to case studies.
CONTINUING CARE COMPLICATIONS
Adenovirus pneumonia in transplant recipients and immunocompromised individuals is linked to considerable morbidity and mortality, perhaps surpassing 60%.
ICD-9 CODES • 008.62 Enteritis attributable to adenovirus • 079.0 Adenovirus infection in conditions categorized elsewhere and of undetermined location • 480.0 Pneumonia resulting from adenovirus

- Published on
Infectious Disease – Anaerobic Infections
• Anaerobic infections are induced by bacteria that necessitate diminished oxygen levels for proliferation.
Anaerobes linked to human diseases are aerotolerant; they can endure, but not proliferate, for up to 72 hours in an oxygen-rich environment.
Anaerobic bacteria inhabit mucosal membranes and are predominant in illnesses originating from mucosal and surrounding areas.
EPIDEMIOLOGY Incidence
Anaerobes comprise up to 10% of blood culture isolates in patients with clinically severe bacteremia. No incidence data exists for anaerobic infections at other sites.
FACTORS OF RISK
• Disruption of the mucosal barrier due to neoplasm, chemotherapy, radiation, neutropenia, graft-versus-host disease, surgical intervention, trauma, inflammatory bowel disease, diverticulitis, and appendicitis • Inadequate dental hygiene • Altered mental state, diminished gag reflex, and impaired swallowing
GENERAL PREVENTION
• Bowel preparation and preoperative antibacterial prophylaxis • Excellent oral hygiene • Aspiration precautions
Pathophysiology
• Translocation of indigenous flora into sterile sites resulting from mucosal membrane disruption • Translocation of oral flora into the lungs due to aspiration • Proliferation of obligate anaerobes during polymicrobial infections caused by reduced oxidation–reduction potential from aerobic organisms • Virulence factors allow anaerobic bacteria to induce abscess formation (e.g., Bacteroides fragilis: capsular polysaccharide), evade host defenses (e.g., Prevotella: IgA proteases), and adhere to cell surfaces
For instance, Porphyromonas gingivalis produces proteases, while Fusobacterium necrophorum generates leukotoxin and endotoxin.
ETIOLOGY
• B. fragilis is the predominant isolated anaerobic Gram-negative bacillus. Other Gram-negative bacteria include Fusobacterium, Prevotella, and Porphyromonas species. Peptostreptococcus species are the predominant Gram-positive cocci, while Clostridia represent the primary Gram-positive rods responsible for disease.
FREQUENTLY CO-OCCURRING CONDITIONS
• Dental infections – Pulpitis – Periapical and dental abscess – Perimandibular space infection • Gingivitis – Periodontitis – Periodontal abscess • Extension of periodontal infection resulting in maxillary sinus osteomyelitis or submandibular space infection • Vincent’s stomatitis (trench mouth) • Ludwig’s angina: Bilateral infection of the sublingual region and submandibular regions
Lemierre Syndrome: Infection of the posterior compartment of the lateral pharyngeal space by F. necrophorum, resulting in suppurative thrombophlebitis of the jugular vein and subsequent metastases, predominantly to the lungs.
• Chronic sinusitis and otitis media • Pleuropulmonary infections – Aspiration pneumonia – Necrotizing pneumonia – Lung abscess – Empyema
• Intra-abdominal infections – Peritonitis – Abscesses – Neutropenic colitis (Typhlitis) • Female genital tract infections – Pelvic inflammatory illness – Pelvic abscess – Septic abortion – Endometritis – Tubo-ovarian abscess – Postoperative infection
– Bacterial vaginosis – Pelvic cellulitis – Amnionitis – Septic thrombosis of pelvic veins • Central nervous system infections
Cerebral abscess, epidural abscess, subdural empyema
Anaerobic meningitis: Uncommon, indicative of shunt infection or parameningeal collection.
• Dermatological and subcutaneous conditions – Necrotizing fasciitis – Gas gangrene – Crepitant cellulitis – Bite injuries – Surgical incisions
– Diabetic foot infections – Pressure ulcers
• Bone and joint – Osteomyelitis and septic arthritis in proximity to affected soft tissue locations • Bacteremia – Resulting from an intra-abdominal, vaginal tract, respiratory tract, or soft tissue infection – B. fragilis is the most prevalent isolate
HISTORY OF DIAGNOSIS
• Abrupt emergence of sensitive, hemorrhaging gums, halitosis, unpleasant taste, fever, and cervical lymphadenopathy - Vincent’s stomatitis (trench mouth) • Pain in the submandibular and/or sublingual regions, trismus, and lateral or posterior displacement of the tongue leading to dysphagia and/or airway obstruction – Ludwig’s angina
• Nasopharyngitis or tonsillar abscess, succeeded 1–2 weeks later by pyrexia, submandibular angle lymphadenopathy, discomfort along the lateral portion of the sternocleidomastoid muscle, and pulmonary metastases.
Lemierre's syndrome
• Weight reduction, thoracic discomfort, or pleuritic pain - Empyema
• Persistent malaise, weight reduction, pyrexia, chills, malodorous sputum, and anemia – Anaerobic pulmonary abscess • Impaired cognitive function, dysphagia, chronic respiratory manifestations, weight reduction, pyrexia, and anemia
Aspiration pneumonia
• Neutropenia, right lower quadrant stomach discomfort, fever, diarrhea – Typhlitis • Lack of progress in the infectious process on an antibiotic regimen devoid of anaerobic activity – Indicative of anaerobes
PHYSICAL EXAMINATION
• Deteriorated dental condition – Prevalence of anaerobic oral microbiota with potential for translocation
• Gas in tissue, crepitus – Infection with gas-producing bacteria • Malodorous discharge • Infection near mucosal surfaces • Tissue necrosis, abscess development – Suggestive of anaerobic organisms DIAGNOSTIC TESTS & INTERPRETATION Laboratory
Anaerobes present significant challenges in cultivation and identification. In numerous instances, the anaerobic origin of an infection remains unverified.
• Cultural methodology
Specimens must be obtained while preventing contamination of the indigenous flora of mucosal surfaces.
- Liquids or tissues are preferred over swab specimens.
Air must be removed from the syringe utilized for aspiration, and the needle must be sealed.
– Utilization of anaerobic transport media. – Expedited processing of samples.
All specimens must undergo Gram staining; the absence of growth in culture alongside the presence of Gram-positive and Gram-negative organisms in Gram staining indicates the potential existence of anaerobic organisms.
Imaging • Radiographs – Presence of air–fluid levels, cavity formation, and gas in tissue • CT and/or MRI scans – Frequently essential for delineating anatomical location and disease extent
Diagnostic Procedures/Other: CT- or ultrasound-guided aspiration or biopsy
DIFFERENTIAL DIAGNOSIS
Anaerobic lung abscesses must be distinguished from mycobacterial infections.
TREATMENT
• The treatment comprises a combination of surgical interventions (resection, debridement, drainage) and antimicrobial therapy. • Antibiotics administered must encompass both aerobic and anaerobic bacteria due to the polymicrobial characteristics of numerous illnesses.
Empirical selection of antibiotic regimen based on infection type, Gram stain results, tissue penetration, and toxicity. Susceptibility testing is challenging because to anaerobic culture methodologies, prolonged turnaround times, and inadequate quality control.
• Susceptibility testing is advised for patients requiring extended antibiotic treatment: cerebral abscess, osteomyelitis, and infections associated with prosthetic devices. • Anaerobic infections originating from below the diaphragm should be managed with targeted therapy against B. fragilis. Members of the B. fragilis group exhibit resistance to penicillin.
Antimicrobial drugs effective against anaerobes include carbapenems, β-lactam/β-lactamase inhibitor combinations, and metronidazole (note that metronidazole is ineffective against Actinomyces spp., Propionibacterium spp., peptostreptococci, and microaerophilic streptococci).
• Rising incidence of antibiotic resistance in B. fragilis.
Resistance to cephamycins is 8–14%, clindamycin 26% and moxifloxacin 38%
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patient Surveillance
Ensure sufficient drainage of abscesses with further imaging.
Surgical resection is warranted if drainage proves ineffective.
• Conduct repeat sampling if the infection does not respond to antimicrobial therapy to assess for drug-resistant organisms.
• Surveillance for antimicrobial drug toxicities.
COMPLICATIONS
Uninterrupted dissemination of untreated illnesses
• Anaerobic infections are induced by bacteria that necessitate diminished oxygen levels for proliferation.
Anaerobes linked to human diseases are aerotolerant; they can endure, but not proliferate, for up to 72 hours in an oxygen-rich environment.
Anaerobic bacteria inhabit mucosal membranes and are predominant in illnesses originating from mucosal and surrounding areas.
EPIDEMIOLOGY Incidence
Anaerobes comprise up to 10% of blood culture isolates in patients with clinically severe bacteremia. No incidence data exists for anaerobic infections at other sites.
FACTORS OF RISK
• Disruption of the mucosal barrier due to neoplasm, chemotherapy, radiation, neutropenia, graft-versus-host disease, surgical intervention, trauma, inflammatory bowel disease, diverticulitis, and appendicitis • Inadequate dental hygiene • Altered mental state, diminished gag reflex, and impaired swallowing
GENERAL PREVENTION
• Bowel preparation and preoperative antibacterial prophylaxis • Excellent oral hygiene • Aspiration precautions
Pathophysiology
• Translocation of indigenous flora into sterile sites resulting from mucosal membrane disruption • Translocation of oral flora into the lungs due to aspiration • Proliferation of obligate anaerobes during polymicrobial infections caused by reduced oxidation–reduction potential from aerobic organisms • Virulence factors allow anaerobic bacteria to induce abscess formation (e.g., Bacteroides fragilis: capsular polysaccharide), evade host defenses (e.g., Prevotella: IgA proteases), and adhere to cell surfaces
For instance, Porphyromonas gingivalis produces proteases, while Fusobacterium necrophorum generates leukotoxin and endotoxin.
ETIOLOGY
• B. fragilis is the predominant isolated anaerobic Gram-negative bacillus. Other Gram-negative bacteria include Fusobacterium, Prevotella, and Porphyromonas species. Peptostreptococcus species are the predominant Gram-positive cocci, while Clostridia represent the primary Gram-positive rods responsible for disease.
FREQUENTLY CO-OCCURRING CONDITIONS
• Dental infections – Pulpitis – Periapical and dental abscess – Perimandibular space infection • Gingivitis – Periodontitis – Periodontal abscess • Extension of periodontal infection resulting in maxillary sinus osteomyelitis or submandibular space infection • Vincent’s stomatitis (trench mouth) • Ludwig’s angina: Bilateral infection of the sublingual region and submandibular regions
Lemierre Syndrome: Infection of the posterior compartment of the lateral pharyngeal space by F. necrophorum, resulting in suppurative thrombophlebitis of the jugular vein and subsequent metastases, predominantly to the lungs.
• Chronic sinusitis and otitis media • Pleuropulmonary infections – Aspiration pneumonia – Necrotizing pneumonia – Lung abscess – Empyema
• Intra-abdominal infections – Peritonitis – Abscesses – Neutropenic colitis (Typhlitis) • Female genital tract infections – Pelvic inflammatory illness – Pelvic abscess – Septic abortion – Endometritis – Tubo-ovarian abscess – Postoperative infection
– Bacterial vaginosis – Pelvic cellulitis – Amnionitis – Septic thrombosis of pelvic veins • Central nervous system infections
Cerebral abscess, epidural abscess, subdural empyema
Anaerobic meningitis: Uncommon, indicative of shunt infection or parameningeal collection.
• Dermatological and subcutaneous conditions – Necrotizing fasciitis – Gas gangrene – Crepitant cellulitis – Bite injuries – Surgical incisions
– Diabetic foot infections – Pressure ulcers
• Bone and joint – Osteomyelitis and septic arthritis in proximity to affected soft tissue locations • Bacteremia – Resulting from an intra-abdominal, vaginal tract, respiratory tract, or soft tissue infection – B. fragilis is the most prevalent isolate
HISTORY OF DIAGNOSIS
• Abrupt emergence of sensitive, hemorrhaging gums, halitosis, unpleasant taste, fever, and cervical lymphadenopathy - Vincent’s stomatitis (trench mouth) • Pain in the submandibular and/or sublingual regions, trismus, and lateral or posterior displacement of the tongue leading to dysphagia and/or airway obstruction – Ludwig’s angina
• Nasopharyngitis or tonsillar abscess, succeeded 1–2 weeks later by pyrexia, submandibular angle lymphadenopathy, discomfort along the lateral portion of the sternocleidomastoid muscle, and pulmonary metastases.
Lemierre's syndrome
• Weight reduction, thoracic discomfort, or pleuritic pain - Empyema
• Persistent malaise, weight reduction, pyrexia, chills, malodorous sputum, and anemia – Anaerobic pulmonary abscess • Impaired cognitive function, dysphagia, chronic respiratory manifestations, weight reduction, pyrexia, and anemia
Aspiration pneumonia
• Neutropenia, right lower quadrant stomach discomfort, fever, diarrhea – Typhlitis • Lack of progress in the infectious process on an antibiotic regimen devoid of anaerobic activity – Indicative of anaerobes
PHYSICAL EXAMINATION
• Deteriorated dental condition – Prevalence of anaerobic oral microbiota with potential for translocation
• Gas in tissue, crepitus – Infection with gas-producing bacteria • Malodorous discharge • Infection near mucosal surfaces • Tissue necrosis, abscess development – Suggestive of anaerobic organisms DIAGNOSTIC TESTS & INTERPRETATION Laboratory
Anaerobes present significant challenges in cultivation and identification. In numerous instances, the anaerobic origin of an infection remains unverified.
• Cultural methodology
Specimens must be obtained while preventing contamination of the indigenous flora of mucosal surfaces.
- Liquids or tissues are preferred over swab specimens.
Air must be removed from the syringe utilized for aspiration, and the needle must be sealed.
– Utilization of anaerobic transport media. – Expedited processing of samples.
All specimens must undergo Gram staining; the absence of growth in culture alongside the presence of Gram-positive and Gram-negative organisms in Gram staining indicates the potential existence of anaerobic organisms.
Imaging • Radiographs – Presence of air–fluid levels, cavity formation, and gas in tissue • CT and/or MRI scans – Frequently essential for delineating anatomical location and disease extent
Diagnostic Procedures/Other: CT- or ultrasound-guided aspiration or biopsy
DIFFERENTIAL DIAGNOSIS
Anaerobic lung abscesses must be distinguished from mycobacterial infections.
TREATMENT
• The treatment comprises a combination of surgical interventions (resection, debridement, drainage) and antimicrobial therapy. • Antibiotics administered must encompass both aerobic and anaerobic bacteria due to the polymicrobial characteristics of numerous illnesses.
Empirical selection of antibiotic regimen based on infection type, Gram stain results, tissue penetration, and toxicity. Susceptibility testing is challenging because to anaerobic culture methodologies, prolonged turnaround times, and inadequate quality control.
• Susceptibility testing is advised for patients requiring extended antibiotic treatment: cerebral abscess, osteomyelitis, and infections associated with prosthetic devices. • Anaerobic infections originating from below the diaphragm should be managed with targeted therapy against B. fragilis. Members of the B. fragilis group exhibit resistance to penicillin.
Antimicrobial drugs effective against anaerobes include carbapenems, β-lactam/β-lactamase inhibitor combinations, and metronidazole (note that metronidazole is ineffective against Actinomyces spp., Propionibacterium spp., peptostreptococci, and microaerophilic streptococci).
• Rising incidence of antibiotic resistance in B. fragilis.
Resistance to cephamycins is 8–14%, clindamycin 26% and moxifloxacin 38%
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patient Surveillance
Ensure sufficient drainage of abscesses with further imaging.
Surgical resection is warranted if drainage proves ineffective.
• Conduct repeat sampling if the infection does not respond to antimicrobial therapy to assess for drug-resistant organisms.
• Surveillance for antimicrobial drug toxicities.
COMPLICATIONS
Uninterrupted dissemination of untreated illnesses

- Published on
Infectious Disease - Amebiasis
Protozoan infection induced by Entamoeba histolytica. Infection by these organisms results in diarrhea, colitis, and occasionally, extra-intestinal symptoms such as liver abscesses.
• Symptomatic illness manifests in fewer than 10% of affected persons. A minimal proportion of individuals with intestinal infections will progress to invasive illness.
Epidemiology
Frequency
Approximately ten percent of the global population is thought to be infected with E. histolytica.
• Prevalence varies from less than 5% in developed nations to 20–30% in tropical regions.
The estimated prevalence in the US is approximately 4%.
The disease manifests across all age groups and affects both genders equally.
RISK FACTORS • Risk factors in endemic regions encompass: – Low socioeconomic status – Inadequate sanitation
– Overcrowding • In nations with low prevalence:
- Immigrants or travelers from endemic areas – Institutionalized individuals – Males engaging in sexual relations with other males
• Risk factors linked to serious disease: - Newborns – Gestation
Corticosteroid treatment; malnutrition.
COMPREHENSIVE PREVENTION
• Humans constitute the sole reservoir of the infection.
Contaminated water or vegetables frequently serve as sources of infection in humans.
Cysts are not eliminated by chlorine; boiling water is essential for decontamination.
• Refrain from consuming polluted water and food. • Ensure that vegetables are thoroughly cleansed with potable water or treated with detergent and immersed in acetic acid or vinegar.
PATHOPHYSIOLOGY
• Infection transmits through the fecal–oral pathway • The organism manifests in two forms:
Trophozoite possessing a singular nucleus, with or without swallowed erythrocytes.
Cyst with four nuclei
The ingestion of the cyst leads to excystation in the small intestine. Trophozoites are generated, infecting the colon and causing symptoms.
• Under adverse conditions, the trophozoite encysts, and the cyst form is excreted in feces.
Cysts persist in a damp environment for several months.
• The majority of individuals infected with the bacterium exhibit minimal invasion of the intestinal mucosa and remain asymptomatic (cyst passers).
Patients exhibiting colonic invasion present with flask-shaped colonic ulcers.
ETIOLOGY • E. histolytica is one of the several Entamoeba species that infect people.
Nonpathogenic species encompass Entamoeba dispar, Entamoeba moshkovskii (both morphologically indistinguishable), Entamoeba hartmanni, and Entamoeba coli.
HISTORY OF DIAGNOSIS
• Patients exhibit symptoms of invasive illness within four weeks following the intake of cysts.
Amebic liver abscess typically requires approximately three months for development.
• Certain patients harbor the germs for extended durations prior to exhibiting notable clinical symptoms. • Intestinal disorder – Asymptomatic infection
— Symptomatic non-invasive infection
- Symptoms are minor; diarrhea is the sole manifestation. - Amebic colitis (dysentery) - Crampy abdominal discomfort - Hemorrhagic, mucoid diarrhea - Rectal hemorrhage may accompany diarrhea, particularly in pediatric patients - Fever is present in one-third of affected individuals – Weight reduction – Anorexia nervosa
• Extra-intestinal disease – Extra-intestinal amebiasis can impact the liver (abscess), spleen, lungs, or brain.
Amebic liver abscess manifests with fever and right upper quadrant pain.
ache in the upper quadrant. Fifty percent of patients with amebic liver abscess exhibit no prior history of colitis.
– Occasionally, the rupture of the abscess may result in peritonitis.
– Rupture of the liver abscess into the pleural cavity results in empyema. Patients exhibit fever, dyspnea, and pleuritic thoracic pain.
Cerebral amebiasis: Nausea, vomiting, cephalalgia, alterations in mental condition
PHYSICAL EXAMINATION
• Colitis – Widespread abdominal pain – Distension, rebound tenderness in severe colitis/perforation • Liver abscess – pain upon palpation of the liver Hepatomegaly - Jaundice is infrequent
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
• Stool microscopy and O&P examination may reveal the presence of stool leukocytes.
- Intracytoplasmic erythrocytes within trophozoites (observed)
In E. histolytica and E. dispar, a wet mount for motile trophozoites and formal-ether concentration, followed by an iodine-stained deposit, enhances the probability of finding cysts.
– To enhance the efficacy of microscopic diagnosis, many samples must be analyzed. • Antigen detection – Fecal antigen identified with ELISA. More sensitive than O&P, however less effective than PCR. Requires either fresh or frozen specimens.
Applicable in hepatic abscess fluid.
– The TechLab E. histolytica II ELISA differentiates between pathogenic and nonpathogenic amebae• Serology – Beneficial in diagnosing liver abscess and invasive colonic illness – ELISA (most frequently utilized), indirect immunofluorescent assay, indirect hemagglutination assay – False positives in the early stages of the disease – Titers persist at elevated levels for years – In endemic regions, high seropositivity precludes differentiation between active and prior infection.
• Culture is conducted exclusively in research laboratories. • PCR – Real-time PCR is technically intricate yet exhibits more sensitivity than the stool antigen.
- Applicable in hepatic abscess fluid. • Additional laboratory examinations
Leukocytosis absent of eosinophilia is frequently observed in individuals with invasive amebic illness. Elevated alkaline phosphatase levels and moderately increased transaminases are noted in liver abscess cases.
Imaging
Imaging modalities, including ultrasound, CT, and MRI scans, are beneficial in evaluating patients with suspected amebic liver abscess. The amebic abscess is typically situated in the right lobe, specifically in the right upper posterior section of the liver.
Diagnostic Procedures and Additional Methods
• Colonoscopy and biopsy for colonic pathology – Results may appear normal in the first stages of the condition
– Fragile, ulcerated mucosa exhibiting punctate hemorrhages – Lateral infiltration into the submucosal tissues results in the distinctive flask-shaped ulcer associated with amebic colitis – Amebomas manifest as annular lesions
The aspiration of a liver abscess produces dark, odorless, sterile pus, typically referred to as "anchovy paste," which may contain trophozoites. Aspiration of liver abscesses frequently does not yield the organism, as it resides within the abscess walls.
Pathological Observations
Intestinal biopsy specimens obtained from the margins of ulcers must be assessed for motile trophozoites.
• The biopsy reveals mucosal thickening with many distinct ulcers interspersed among areas of normal-appearing mucosa.
DIFFERENTIAL DIAGNOSIS
• Ulcerative colitis • Colorectal carcinoma • Crohn's disease • Diverticulitis • Abdominal abscess • Irritable bowel syndrome • Pyogenic abscess • Hepatoma • Echinococcal liver cyst
MEDICATION FOR TREATMENT
• Asymptomatic disease – Intra-luminal carriage necessitates treatment due to the potential risk of invasive disease.
Paromomycin 500 mg orally three times day for seven days should be used as the first-line treatment.
Diloxanide furoate 500 mg three times daily for 10 days Iodoquinol 650 mg orally three times daily for 20 days
• Colitis – Metronidazole 750 mg orally three times daily for 10 days or tinidazole 1 g orally twice daily for 3 days, followed by one of the subsequent treatments:
Iodoquinol 650 mg orally three times daily for 20 days
Paromomycin 500 mg orally three times daily for seven days • Liver abscess – Administer Metronidazole 750 mg orally or intravenously three times daily for 10 days, followed by Iodoquinol 650 mg orally three times daily for 20 days
CLINICAL INTERVENTIONS/ADDITIONAL PROCEDURES
For a substantial abscess (>3 cm), aspiration and needle intervention
Drainage is warranted. Minor abscesses dissolve with medical intervention.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patients undergoing treatment for liver abscesses should receive follow-up ultrasounds to confirm cyst clearance, which may require many months.
OUTLOOK
Amebiasis presents significant morbidity and mortality, particularly in underdeveloped nations.
COMPLICATIONS
Fulminant colitis accompanied with toxic megacolon, perforation, and peritonitis is uncommon however thoroughly documented.
Amebomas are mass lesions located in the colon, frequently found in the cecum or ascending colon, resulting from inflammation associated with amebic colitis. Amebomas can lead to blockage and may mimic colon cancer.
• Ruptured liver abscess with diaphragm perforation resulting in pleural or pericardial illness.
Protozoan infection induced by Entamoeba histolytica. Infection by these organisms results in diarrhea, colitis, and occasionally, extra-intestinal symptoms such as liver abscesses.
• Symptomatic illness manifests in fewer than 10% of affected persons. A minimal proportion of individuals with intestinal infections will progress to invasive illness.
Epidemiology
Frequency
Approximately ten percent of the global population is thought to be infected with E. histolytica.
• Prevalence varies from less than 5% in developed nations to 20–30% in tropical regions.
The estimated prevalence in the US is approximately 4%.
The disease manifests across all age groups and affects both genders equally.
RISK FACTORS • Risk factors in endemic regions encompass: – Low socioeconomic status – Inadequate sanitation
– Overcrowding • In nations with low prevalence:
- Immigrants or travelers from endemic areas – Institutionalized individuals – Males engaging in sexual relations with other males
• Risk factors linked to serious disease: - Newborns – Gestation
Corticosteroid treatment; malnutrition.
COMPREHENSIVE PREVENTION
• Humans constitute the sole reservoir of the infection.
Contaminated water or vegetables frequently serve as sources of infection in humans.
Cysts are not eliminated by chlorine; boiling water is essential for decontamination.
• Refrain from consuming polluted water and food. • Ensure that vegetables are thoroughly cleansed with potable water or treated with detergent and immersed in acetic acid or vinegar.
PATHOPHYSIOLOGY
• Infection transmits through the fecal–oral pathway • The organism manifests in two forms:
Trophozoite possessing a singular nucleus, with or without swallowed erythrocytes.
Cyst with four nuclei
The ingestion of the cyst leads to excystation in the small intestine. Trophozoites are generated, infecting the colon and causing symptoms.
• Under adverse conditions, the trophozoite encysts, and the cyst form is excreted in feces.
Cysts persist in a damp environment for several months.
• The majority of individuals infected with the bacterium exhibit minimal invasion of the intestinal mucosa and remain asymptomatic (cyst passers).
Patients exhibiting colonic invasion present with flask-shaped colonic ulcers.
ETIOLOGY • E. histolytica is one of the several Entamoeba species that infect people.
Nonpathogenic species encompass Entamoeba dispar, Entamoeba moshkovskii (both morphologically indistinguishable), Entamoeba hartmanni, and Entamoeba coli.
HISTORY OF DIAGNOSIS
• Patients exhibit symptoms of invasive illness within four weeks following the intake of cysts.
Amebic liver abscess typically requires approximately three months for development.
• Certain patients harbor the germs for extended durations prior to exhibiting notable clinical symptoms. • Intestinal disorder – Asymptomatic infection
— Symptomatic non-invasive infection
- Symptoms are minor; diarrhea is the sole manifestation. - Amebic colitis (dysentery) - Crampy abdominal discomfort - Hemorrhagic, mucoid diarrhea - Rectal hemorrhage may accompany diarrhea, particularly in pediatric patients - Fever is present in one-third of affected individuals – Weight reduction – Anorexia nervosa
• Extra-intestinal disease – Extra-intestinal amebiasis can impact the liver (abscess), spleen, lungs, or brain.
Amebic liver abscess manifests with fever and right upper quadrant pain.
ache in the upper quadrant. Fifty percent of patients with amebic liver abscess exhibit no prior history of colitis.
– Occasionally, the rupture of the abscess may result in peritonitis.
– Rupture of the liver abscess into the pleural cavity results in empyema. Patients exhibit fever, dyspnea, and pleuritic thoracic pain.
Cerebral amebiasis: Nausea, vomiting, cephalalgia, alterations in mental condition
PHYSICAL EXAMINATION
• Colitis – Widespread abdominal pain – Distension, rebound tenderness in severe colitis/perforation • Liver abscess – pain upon palpation of the liver Hepatomegaly - Jaundice is infrequent
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
• Stool microscopy and O&P examination may reveal the presence of stool leukocytes.
- Intracytoplasmic erythrocytes within trophozoites (observed)
In E. histolytica and E. dispar, a wet mount for motile trophozoites and formal-ether concentration, followed by an iodine-stained deposit, enhances the probability of finding cysts.
– To enhance the efficacy of microscopic diagnosis, many samples must be analyzed. • Antigen detection – Fecal antigen identified with ELISA. More sensitive than O&P, however less effective than PCR. Requires either fresh or frozen specimens.
Applicable in hepatic abscess fluid.
– The TechLab E. histolytica II ELISA differentiates between pathogenic and nonpathogenic amebae• Serology – Beneficial in diagnosing liver abscess and invasive colonic illness – ELISA (most frequently utilized), indirect immunofluorescent assay, indirect hemagglutination assay – False positives in the early stages of the disease – Titers persist at elevated levels for years – In endemic regions, high seropositivity precludes differentiation between active and prior infection.
• Culture is conducted exclusively in research laboratories. • PCR – Real-time PCR is technically intricate yet exhibits more sensitivity than the stool antigen.
- Applicable in hepatic abscess fluid. • Additional laboratory examinations
Leukocytosis absent of eosinophilia is frequently observed in individuals with invasive amebic illness. Elevated alkaline phosphatase levels and moderately increased transaminases are noted in liver abscess cases.
Imaging
Imaging modalities, including ultrasound, CT, and MRI scans, are beneficial in evaluating patients with suspected amebic liver abscess. The amebic abscess is typically situated in the right lobe, specifically in the right upper posterior section of the liver.
Diagnostic Procedures and Additional Methods
• Colonoscopy and biopsy for colonic pathology – Results may appear normal in the first stages of the condition
– Fragile, ulcerated mucosa exhibiting punctate hemorrhages – Lateral infiltration into the submucosal tissues results in the distinctive flask-shaped ulcer associated with amebic colitis – Amebomas manifest as annular lesions
The aspiration of a liver abscess produces dark, odorless, sterile pus, typically referred to as "anchovy paste," which may contain trophozoites. Aspiration of liver abscesses frequently does not yield the organism, as it resides within the abscess walls.
Pathological Observations
Intestinal biopsy specimens obtained from the margins of ulcers must be assessed for motile trophozoites.
• The biopsy reveals mucosal thickening with many distinct ulcers interspersed among areas of normal-appearing mucosa.
DIFFERENTIAL DIAGNOSIS
• Ulcerative colitis • Colorectal carcinoma • Crohn's disease • Diverticulitis • Abdominal abscess • Irritable bowel syndrome • Pyogenic abscess • Hepatoma • Echinococcal liver cyst
MEDICATION FOR TREATMENT
• Asymptomatic disease – Intra-luminal carriage necessitates treatment due to the potential risk of invasive disease.
Paromomycin 500 mg orally three times day for seven days should be used as the first-line treatment.
Diloxanide furoate 500 mg three times daily for 10 days Iodoquinol 650 mg orally three times daily for 20 days
• Colitis – Metronidazole 750 mg orally three times daily for 10 days or tinidazole 1 g orally twice daily for 3 days, followed by one of the subsequent treatments:
Iodoquinol 650 mg orally three times daily for 20 days
Paromomycin 500 mg orally three times daily for seven days • Liver abscess – Administer Metronidazole 750 mg orally or intravenously three times daily for 10 days, followed by Iodoquinol 650 mg orally three times daily for 20 days
CLINICAL INTERVENTIONS/ADDITIONAL PROCEDURES
For a substantial abscess (>3 cm), aspiration and needle intervention
Drainage is warranted. Minor abscesses dissolve with medical intervention.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patients undergoing treatment for liver abscesses should receive follow-up ultrasounds to confirm cyst clearance, which may require many months.
OUTLOOK
Amebiasis presents significant morbidity and mortality, particularly in underdeveloped nations.
COMPLICATIONS
Fulminant colitis accompanied with toxic megacolon, perforation, and peritonitis is uncommon however thoroughly documented.
Amebomas are mass lesions located in the colon, frequently found in the cecum or ascending colon, resulting from inflammation associated with amebic colitis. Amebomas can lead to blockage and may mimic colon cancer.
• Ruptured liver abscess with diaphragm perforation resulting in pleural or pericardial illness.

- Published on
Infectious Disease – Anorectql Infection
Anorectal infections pertain to infections of the anus and rectum, which constitute the terminal section of the large intestine.
Fournier’s gangrene encompasses any necrotizing infection of the external genitalia and perineum.
EPIDEMIOLOGY
Incidence
The prevalence of external anogenital lesions among organ transplant recipients is 1.5–2.3%, with a higher incidence in women. The majority of lesions are attributable to anogenital warts, succeeded by bowenoid papulosis, gigantic condyloma, and in situ cancer.
FACTORS OF RISK
Fournier’s gangrene frequently presents with a history of urinary infections, urologic instrumentation, or chronic colorectal illness. Moreover, the majority of patients
are impacted by comorbidities such as diabetes, alcoholism, or intravenous drug use, which impede host defense mechanisms.
COMPREHENSIVE PREVENTION
In immunocompromised patients exhibiting abscesses, perianal sepsis should be regarded as a potential source. Perianal fistulas in these patients should be incised or managed with fistulectomy, while perianal abscesses necessitate proper drainage to prevent necrotizing gangrene and metastatic abscesses.
Pathophysiology
Primary anal or rectal infection occurs in women and men who have sex with men following receptive anorectal intercourse. In women, rectal infection with lymphogranuloma venereum (or non-LGV) strains of Chlamydia trachomatis may occur through the contiguous dissemination of infected secretions along the perineum, similar to rectal gonococcal infections, or potentially via the pelvic lymphatics to the rectum.
Both herpes simplex viruses types 1 and 2 may induce symptomatic or asymptomatic infections in the rectal and perianal regions. Herpes infection proctitis is typically pertaining to anal intercourse. Nonetheless, asymptomatic perianal shedding of herpes simplex virus (HSV) is observed in both heterosexual men and women who do not engage in rectal intercourse.
Perianal warts are prevalent in men who engage in sexual relations with other men, yet they also occur in heterosexual men.
Perirectal abscesses frequently signify the migration of purulent material from the rectosigmoid region into the anal vicinity. Diverticulitis, Crohn's disease, ulcerative colitis, or prior surgical intervention may be the etiological factors.
Aerobic bacteria are present in most instances of Fournier’s gangrene, although mixed aerobic and anaerobic infections also occur.
ETIOLOGY • The predominant anorectal infections comprise bacterial and parasite infections (e.g., abscesses or soft-tissue infections) as well as sexually transmitted diseases. Many of these infections are also addressed in other chapters of the book.
• In men who engage in sexual activity with other men, the predominant causes of anorectal infection are as follows:
Anorectal gonococcal infection and herpes simplex virus (HSV)
- Infections caused by intestinal microorganisms, typically Giardia
Lamblia, Entamoeba histolytica, Campylobacter spp., and C. trachomatis - Syphilis Rectal lesions frequently occur in HIV-infected individuals, especially perirectal ulcers and erosions resulting from the reactivation of HSV infection. Additional rectal lesions frequently observed in HIV-infected individuals encompass condyloma acuminatum, Kaposi's sarcoma, and intraepithelial neoplasia.
FREQUENTLY CO-OCCURRING CONDITIONS
• Type I Diabetes Mellitus • Type II Diabetes Mellitus
HISTORY OF DIAGNOSIS
Symptoms of herpes simplex proctitis encompass anorectal pain, anorectal discharge, tenesmus, and constipation. Disproportionate pain relative to cutaneous manifestations may occur in Fournier’s gangrene.
PHYSICAL EXAM
• The primary presentations of anogenital warts are cauliflower-like condyloma acuminata typically affecting moist surfaces; keratotic and smooth papular warts, generally located on dry surfaces; and subclinical "flat" warts, which may appear on any mucosal or cutaneous surface.
Fournier’s gangrene is marked by localized gangrene and significant enlargement of the scrotum and penis, extending into the perineum, abdominal wall, and legs.
• Blisters • Bullae • Erythema
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Initial laboratory assessments
Anorectal swab specimens can assist in the diagnosis of C. trachomatis infections with the application of PCR.
In cases of anorectal infection caused by HSV, sigmoidoscopy demonstrates ulcerative lesions in the distal 10 cm of the rectal mucosa. Rectal biopsies reveal mucosal ulceration, necrosis, polymorphonuclear and lymphocytic infiltration of the lamina propria, and, in rare instances, multinucleated intranuclear inclusion-bearing cells.
• Complete Blood Count (CBC) • Creatine Phosphokinase (CPK) • Erythrocyte Sedimentation Rate (ESR) • C-Reactive Protein (CRP) • Comprehensive Metabolic Panel (Chem 7) • Glucose • Arterial Blood Gas Analysis for critically unwell patients
Imaging modalities: • Computed Tomography (CT) scan • Magnetic Resonance Imaging (MRI)
DIFFERENTIAL DIAGNOSIS • Perianal donovanosis may mimic condylomata lata associated with secondary syphilis. Other venereal illnesses, especially syphilis, often coexist with donovanosis. In regions where donovanosis is endemic, the continued presence of suspected condylomata lata following adequate penicillin treatment for syphilis strongly indicates donovanosis. The differential diagnosis for anogenital warts encompasses condylomata lata associated with secondary syphilis, molluscum contagiosum, hirsutoid papillomatosis (pearly penile papules), fibroepitheliomas, and neoplasms.
THERAPEUTIC MEDICATION
• Cryotherapy may effectively eliminate warts that have not responded to podophyllin treatment. Perianal warts, however, exhibit poor responsiveness. Interferons have been utilized as adjuncts to various therapies.
Conservative treatment of local or systemic antibiotics is suitable for perianal abscess. Spontaneous clearance of granulomatous lesions is improbable, hence surgical intervention should be the preferred treatment.
Early and assertive surgical intervention is crucial for patients with Fournier’s gangrene, focusing on the excision of necrotic tissue, alleviation of compartment pressure, and acquisition of specimens for Gram staining as well as aerobic and anaerobic cultures. Empirical antibiotic therapy for mixed aerobic–anaerobic infections may include clindamycin (900 mg intravenously three times daily), ampicillin or ampicillin/sulbactam (2–3 g intravenously every six hours), in addition to gentamicin (1.0–1.5 mg/kg three times daily). Hyperbaric oxygen therapy may also be beneficial in cases of gas gangrene caused by clostridial species. The duration of therapy is variable; nonetheless, antibiotics must be administered until all indications of infection are resolved.
Systemic toxicity has been resolved, and all necrotic tissue has been excised.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
An early surgical consultation is essential for patients suspected of or diagnosed with Fournier’s gangrene.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
Patients diagnosed with Fournier’s gangrene may necessitate hospitalization to the Intensive Care Unit (ICU).
CONTINUOUS MANAGEMENT POST-TREATMENT GUIDELINES
Anal warts and HIV infection are independent risk factors for cytologic abnormalities. Individuals at elevated risk for anal abnormalities comprise men with anal human papillomavirus infection and a history of intravenous drug use. Certain authorities recommend that these individuals, together with organ transplant recipients infected with oncogenic human papillomavirus, should be prioritized for anal cytology screening to detect and manage potentially precancerous anal conditions.
COMPLICATIONS
• Epidermodysplasia verruciformis is an uncommon autosomal recessive disorder marked by the inability to regulate human papillomavirus infection. Patients regularly get atypical human papillomavirus strains and commonly develop cutaneous squamous cell carcinomas, especially in sun-exposed regions. The lesions resemble flat warts or macules akin to those.
Pityriasis versicolor consequences include irritation and, at times, bleeding associated with warts. Warts may, in uncommon instances, become secondarily infected by bacteria or fungi. Extensive clusters of warts may induce mechanical complications, such as blockage of the delivery canal.
Perianal sepsis should consistently be considered as a potential source of infection in HIV-infected individuals, particularly in those with diminished CD4 cell levels. Fournier’s gangrene may lead to septicemia and has fatality rates ranging from 22% to 66%.
Anorectal infections pertain to infections of the anus and rectum, which constitute the terminal section of the large intestine.
Fournier’s gangrene encompasses any necrotizing infection of the external genitalia and perineum.
EPIDEMIOLOGY
Incidence
The prevalence of external anogenital lesions among organ transplant recipients is 1.5–2.3%, with a higher incidence in women. The majority of lesions are attributable to anogenital warts, succeeded by bowenoid papulosis, gigantic condyloma, and in situ cancer.
FACTORS OF RISK
Fournier’s gangrene frequently presents with a history of urinary infections, urologic instrumentation, or chronic colorectal illness. Moreover, the majority of patients
are impacted by comorbidities such as diabetes, alcoholism, or intravenous drug use, which impede host defense mechanisms.
COMPREHENSIVE PREVENTION
In immunocompromised patients exhibiting abscesses, perianal sepsis should be regarded as a potential source. Perianal fistulas in these patients should be incised or managed with fistulectomy, while perianal abscesses necessitate proper drainage to prevent necrotizing gangrene and metastatic abscesses.
Pathophysiology
Primary anal or rectal infection occurs in women and men who have sex with men following receptive anorectal intercourse. In women, rectal infection with lymphogranuloma venereum (or non-LGV) strains of Chlamydia trachomatis may occur through the contiguous dissemination of infected secretions along the perineum, similar to rectal gonococcal infections, or potentially via the pelvic lymphatics to the rectum.
Both herpes simplex viruses types 1 and 2 may induce symptomatic or asymptomatic infections in the rectal and perianal regions. Herpes infection proctitis is typically pertaining to anal intercourse. Nonetheless, asymptomatic perianal shedding of herpes simplex virus (HSV) is observed in both heterosexual men and women who do not engage in rectal intercourse.
Perianal warts are prevalent in men who engage in sexual relations with other men, yet they also occur in heterosexual men.
Perirectal abscesses frequently signify the migration of purulent material from the rectosigmoid region into the anal vicinity. Diverticulitis, Crohn's disease, ulcerative colitis, or prior surgical intervention may be the etiological factors.
Aerobic bacteria are present in most instances of Fournier’s gangrene, although mixed aerobic and anaerobic infections also occur.
ETIOLOGY • The predominant anorectal infections comprise bacterial and parasite infections (e.g., abscesses or soft-tissue infections) as well as sexually transmitted diseases. Many of these infections are also addressed in other chapters of the book.
• In men who engage in sexual activity with other men, the predominant causes of anorectal infection are as follows:
Anorectal gonococcal infection and herpes simplex virus (HSV)
- Infections caused by intestinal microorganisms, typically Giardia
Lamblia, Entamoeba histolytica, Campylobacter spp., and C. trachomatis - Syphilis Rectal lesions frequently occur in HIV-infected individuals, especially perirectal ulcers and erosions resulting from the reactivation of HSV infection. Additional rectal lesions frequently observed in HIV-infected individuals encompass condyloma acuminatum, Kaposi's sarcoma, and intraepithelial neoplasia.
FREQUENTLY CO-OCCURRING CONDITIONS
• Type I Diabetes Mellitus • Type II Diabetes Mellitus
HISTORY OF DIAGNOSIS
Symptoms of herpes simplex proctitis encompass anorectal pain, anorectal discharge, tenesmus, and constipation. Disproportionate pain relative to cutaneous manifestations may occur in Fournier’s gangrene.
PHYSICAL EXAM
• The primary presentations of anogenital warts are cauliflower-like condyloma acuminata typically affecting moist surfaces; keratotic and smooth papular warts, generally located on dry surfaces; and subclinical "flat" warts, which may appear on any mucosal or cutaneous surface.
Fournier’s gangrene is marked by localized gangrene and significant enlargement of the scrotum and penis, extending into the perineum, abdominal wall, and legs.
• Blisters • Bullae • Erythema
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Initial laboratory assessments
Anorectal swab specimens can assist in the diagnosis of C. trachomatis infections with the application of PCR.
In cases of anorectal infection caused by HSV, sigmoidoscopy demonstrates ulcerative lesions in the distal 10 cm of the rectal mucosa. Rectal biopsies reveal mucosal ulceration, necrosis, polymorphonuclear and lymphocytic infiltration of the lamina propria, and, in rare instances, multinucleated intranuclear inclusion-bearing cells.
• Complete Blood Count (CBC) • Creatine Phosphokinase (CPK) • Erythrocyte Sedimentation Rate (ESR) • C-Reactive Protein (CRP) • Comprehensive Metabolic Panel (Chem 7) • Glucose • Arterial Blood Gas Analysis for critically unwell patients
Imaging modalities: • Computed Tomography (CT) scan • Magnetic Resonance Imaging (MRI)
DIFFERENTIAL DIAGNOSIS • Perianal donovanosis may mimic condylomata lata associated with secondary syphilis. Other venereal illnesses, especially syphilis, often coexist with donovanosis. In regions where donovanosis is endemic, the continued presence of suspected condylomata lata following adequate penicillin treatment for syphilis strongly indicates donovanosis. The differential diagnosis for anogenital warts encompasses condylomata lata associated with secondary syphilis, molluscum contagiosum, hirsutoid papillomatosis (pearly penile papules), fibroepitheliomas, and neoplasms.
THERAPEUTIC MEDICATION
• Cryotherapy may effectively eliminate warts that have not responded to podophyllin treatment. Perianal warts, however, exhibit poor responsiveness. Interferons have been utilized as adjuncts to various therapies.
Conservative treatment of local or systemic antibiotics is suitable for perianal abscess. Spontaneous clearance of granulomatous lesions is improbable, hence surgical intervention should be the preferred treatment.
Early and assertive surgical intervention is crucial for patients with Fournier’s gangrene, focusing on the excision of necrotic tissue, alleviation of compartment pressure, and acquisition of specimens for Gram staining as well as aerobic and anaerobic cultures. Empirical antibiotic therapy for mixed aerobic–anaerobic infections may include clindamycin (900 mg intravenously three times daily), ampicillin or ampicillin/sulbactam (2–3 g intravenously every six hours), in addition to gentamicin (1.0–1.5 mg/kg three times daily). Hyperbaric oxygen therapy may also be beneficial in cases of gas gangrene caused by clostridial species. The duration of therapy is variable; nonetheless, antibiotics must be administered until all indications of infection are resolved.
Systemic toxicity has been resolved, and all necrotic tissue has been excised.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
An early surgical consultation is essential for patients suspected of or diagnosed with Fournier’s gangrene.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
Patients diagnosed with Fournier’s gangrene may necessitate hospitalization to the Intensive Care Unit (ICU).
CONTINUOUS MANAGEMENT POST-TREATMENT GUIDELINES
Anal warts and HIV infection are independent risk factors for cytologic abnormalities. Individuals at elevated risk for anal abnormalities comprise men with anal human papillomavirus infection and a history of intravenous drug use. Certain authorities recommend that these individuals, together with organ transplant recipients infected with oncogenic human papillomavirus, should be prioritized for anal cytology screening to detect and manage potentially precancerous anal conditions.
COMPLICATIONS
• Epidermodysplasia verruciformis is an uncommon autosomal recessive disorder marked by the inability to regulate human papillomavirus infection. Patients regularly get atypical human papillomavirus strains and commonly develop cutaneous squamous cell carcinomas, especially in sun-exposed regions. The lesions resemble flat warts or macules akin to those.
Pityriasis versicolor consequences include irritation and, at times, bleeding associated with warts. Warts may, in uncommon instances, become secondarily infected by bacteria or fungi. Extensive clusters of warts may induce mechanical complications, such as blockage of the delivery canal.
Perianal sepsis should consistently be considered as a potential source of infection in HIV-infected individuals, particularly in those with diminished CD4 cell levels. Fournier’s gangrene may lead to septicemia and has fatality rates ranging from 22% to 66%.

- Published on
Infectious Disease – Anthrax
BASICS DESCRIPTION
• Anthrax is a zoonotic illness primarily affecting herbivores and infrequently infects humans. The phrase originates from the Greek word for coal and refers to the black eschar associated with the cutaneous variant of the disease. • In humans, the disease manifests predominantly in three forms: cutaneous, respiratory, and gastrointestinal. • Duration of incubation: - Dermatological condition: 3–10 days - Pulmonary disease: 3 to 5 days
Epidemiology • Anthrax is an infrequent disease in the United States. • Epidemics have been documented in relation to the importation of wool, skins, and other animal derivatives. Epidemics in humans in underdeveloped nations are associated with diseases in animals. Foodborne outbreaks have been recorded and associated with the consumption of contaminated meat. In 2001, there were 22 confirmed or suspected cases of anthrax (11 cutaneous and 11 inhalational) associated with bioterrorism in the United States. Five of these patients succumbed. Since December 2009, Scotland has reported a total of 31 instances, including 11 fatalities, of a novel variant of the disease previously characterized as "injectional."
ETIOLOGY
Bacillus anthracis is an aerobic, gram-positive, spore-forming bacterium. Endospores exhibit resistance to desiccation, radiation, and disinfectants, and can remain dormant in soil for extended periods, often for years.
risk FACTORS • In developing nations, the primary danger arises from exposure to contaminated soil or diseased animals. In urban areas, the primary risk arises from exposure to tainted skins and animal fur.
COMPREHENSIVE PREVENTION
• Vaccination of livestock is recommended in endemic regions. • Decontamination of imported skins and animal hair would mitigate danger. The anthrax vaccination is accessible to those at risk of exposure to the pathogen. These encompass military personnel, veterinarians, and individuals exposed to imported hides or animal fur.
Pathophysiology
The synthesis of two binary toxins (lethal toxin and edema toxin) is crucial for the pathogenic process.
DIAGNOSIS
Disease can present as cutaneous, respiratory, or gastrointestinal, with cutaneous being the predominant type. Meningitis may arise as a complication from bacteremic dissemination originating from any of the three principal types.
PHYSICAL EXAM
• Cutaneous disease: The characteristic lesion is a circular eschar (1–3 cm) that may initially present as an ulcerating papule. If neglected, the infection may advance to bacteremia and sepsis. Respiratory sickness typically manifests in two stages. A viral upper respiratory disease persists for 2–4 days, subsequently leading to severe fulminant pneumonitis. Nonetheless, the clinical manifestation may be uncommon, with certain patients exhibiting an absence of cough, chest pain, or irregular lung examination findings. Gastrointestinal disease typically manifests with abdominal discomfort, nausea, vomiting, and fever, and may be accompanied by hematemesis and hematochezia. • Anthrax meningoencephalitis can aggravate bacteremia and may present with a hyperacute onset, rapidly progressing to coma and death. Anthrax in injectable drug users is a serious condition characterized by soft tissue infection, tight edema, cerebral or subarachnoid bleeding, and gastrointestinal symptoms. A typical cutaneous lesion should raise suspicion of anthrax. Assessing the history of exposure to sick or deceased animals, hides, or fur can be beneficial. The diagnosis of pneumonia or gastroenteritis is challenging to ascertain due to the vague clinical manifestations. • A significant observation is that in advanced pulmonary disease, the mediastinum expands on chest X-ray. The conjunction of mediastinal enlargement, altered mental status, and raised hematocrit is 100% sensitive in differentiating inhalational anthrax from community-acquired pneumonia. • Hemorrhagic cerebrospinal fluid and gram-positive bacilli on Gram staining indicate potential meningeal involvement.
DIAGNOSTIC TESTS AND INTERPRETATION LAB • Cultures and Gram stains of vesicular lesions should identify the organism—a large, encapsulated, gram-positive rod arranged in short chains. • Blood cultures are typically positive in febrile, acutely ill patients with pulmonary or gastrointestinal conditions. • Stool cultures detect the organism in gastrointestinal disease. Chest X-ray films frequently demonstrate diffuse infiltrates and effusions. The mediastinum may exhibit widening in the later stages of the disease.
DIFFERENTIAL DIAGNOSIS • Cutaneous – Tularemia – Staphylococcus aureus – Spider bite – Burn lesion • Pulmonary – Diverse bacterial and viral infections • Gastrointestinal – Shigella – Yersinia – Campylobacter • Meningitis – Tuberculosis – Amebic meningoencephalitis – Specific viral infections: Hantavirus, dengue, Ebola
Treatment / Medication
• Naturally acquired cutaneous anthrax in individuals over 2 years of age: - Administer oral ciprofloxacin (500 mg twice day for adults and 15 mg/kg twice daily, not to exceed 500 mg for children) for a duration of 7 to 10 days. - Oral doxycycline (100 mg twice daily in adults and 2.2 mg/kg—capped at 100 mg—twice daily in children) for a duration of 7 to 10 days If susceptibility testing is accessible, administer penicillin G 6–8 million units per day intravenously, penicillin VK 500 mg four times daily, and 50 mg/kg/day in children under 12 years, or amoxicillin orally 500 mg three times daily and 45 mg/kg/day in children to finish the treatment course. – Notwithstanding the possibility of resistance and inducible resistance, an administration of penicillin for approximately 7–10 days may be adequate for the treatment of naturally acquired simple cutaneous anthrax. Levofloxacin may be suggested as an alternative choice.
• For severe cases of spontaneously occurring cutaneous anthrax: – Administer IV ciprofloxacin 400 mg twice daily and 10 mg/kg twice daily in pediatric patients – Administer IV doxycycline 100 mg twice daily in adults and 2.2 mg/kg twice daily in pediatric patients • Cutaneous anthrax associated with bioterrorism: administer oral ciprofloxacin, oral doxycycline, or oral amoxicillin at the recommended dosages for 60 days to fulfill the complete course of postexposure prophylaxis. • For inhalational anthrax, gastrointestinal anthrax, and fulminant bacteremia: – Intravenous ciprofloxacin is preferred over intravenous doxycycline. The combination regimens may consist of IV ciprofloxacin or IV doxycycline in conjunction with one or two of the following agents: imipenem, meropenem, rifampin, vancomycin, penicillin, ampicillin, chloramphenicol, or clindamycin. • Employ a minimum of one drug with enough CNS penetration to address the potential for subclinical meningitis. Some experts recommend the inclusion of clindamycin to suppress endotoxin formation. A human IgG1λ monoclonal antibody targeting a component of the anthrax toxin (raxibacumab) enhanced survival in rabbits and monkeys afflicted with symptomatic inhalational anthrax (IA).
CONTINUED MANAGEMENT SUBSEQUENT SUGGESTIONS
Patients should be monitored for signs of disease recurrence following treatment.
COMPLICATIONS • Pulmonary and gastrointestinal disorders are typically lethal. • Cutaneous disease frequently results in scarring at the site of the eschar.
BASICS DESCRIPTION
• Anthrax is a zoonotic illness primarily affecting herbivores and infrequently infects humans. The phrase originates from the Greek word for coal and refers to the black eschar associated with the cutaneous variant of the disease. • In humans, the disease manifests predominantly in three forms: cutaneous, respiratory, and gastrointestinal. • Duration of incubation: - Dermatological condition: 3–10 days - Pulmonary disease: 3 to 5 days
Epidemiology • Anthrax is an infrequent disease in the United States. • Epidemics have been documented in relation to the importation of wool, skins, and other animal derivatives. Epidemics in humans in underdeveloped nations are associated with diseases in animals. Foodborne outbreaks have been recorded and associated with the consumption of contaminated meat. In 2001, there were 22 confirmed or suspected cases of anthrax (11 cutaneous and 11 inhalational) associated with bioterrorism in the United States. Five of these patients succumbed. Since December 2009, Scotland has reported a total of 31 instances, including 11 fatalities, of a novel variant of the disease previously characterized as "injectional."
ETIOLOGY
Bacillus anthracis is an aerobic, gram-positive, spore-forming bacterium. Endospores exhibit resistance to desiccation, radiation, and disinfectants, and can remain dormant in soil for extended periods, often for years.
risk FACTORS • In developing nations, the primary danger arises from exposure to contaminated soil or diseased animals. In urban areas, the primary risk arises from exposure to tainted skins and animal fur.
COMPREHENSIVE PREVENTION
• Vaccination of livestock is recommended in endemic regions. • Decontamination of imported skins and animal hair would mitigate danger. The anthrax vaccination is accessible to those at risk of exposure to the pathogen. These encompass military personnel, veterinarians, and individuals exposed to imported hides or animal fur.
Pathophysiology
The synthesis of two binary toxins (lethal toxin and edema toxin) is crucial for the pathogenic process.
DIAGNOSIS
Disease can present as cutaneous, respiratory, or gastrointestinal, with cutaneous being the predominant type. Meningitis may arise as a complication from bacteremic dissemination originating from any of the three principal types.
PHYSICAL EXAM
• Cutaneous disease: The characteristic lesion is a circular eschar (1–3 cm) that may initially present as an ulcerating papule. If neglected, the infection may advance to bacteremia and sepsis. Respiratory sickness typically manifests in two stages. A viral upper respiratory disease persists for 2–4 days, subsequently leading to severe fulminant pneumonitis. Nonetheless, the clinical manifestation may be uncommon, with certain patients exhibiting an absence of cough, chest pain, or irregular lung examination findings. Gastrointestinal disease typically manifests with abdominal discomfort, nausea, vomiting, and fever, and may be accompanied by hematemesis and hematochezia. • Anthrax meningoencephalitis can aggravate bacteremia and may present with a hyperacute onset, rapidly progressing to coma and death. Anthrax in injectable drug users is a serious condition characterized by soft tissue infection, tight edema, cerebral or subarachnoid bleeding, and gastrointestinal symptoms. A typical cutaneous lesion should raise suspicion of anthrax. Assessing the history of exposure to sick or deceased animals, hides, or fur can be beneficial. The diagnosis of pneumonia or gastroenteritis is challenging to ascertain due to the vague clinical manifestations. • A significant observation is that in advanced pulmonary disease, the mediastinum expands on chest X-ray. The conjunction of mediastinal enlargement, altered mental status, and raised hematocrit is 100% sensitive in differentiating inhalational anthrax from community-acquired pneumonia. • Hemorrhagic cerebrospinal fluid and gram-positive bacilli on Gram staining indicate potential meningeal involvement.
DIAGNOSTIC TESTS AND INTERPRETATION LAB • Cultures and Gram stains of vesicular lesions should identify the organism—a large, encapsulated, gram-positive rod arranged in short chains. • Blood cultures are typically positive in febrile, acutely ill patients with pulmonary or gastrointestinal conditions. • Stool cultures detect the organism in gastrointestinal disease. Chest X-ray films frequently demonstrate diffuse infiltrates and effusions. The mediastinum may exhibit widening in the later stages of the disease.
DIFFERENTIAL DIAGNOSIS • Cutaneous – Tularemia – Staphylococcus aureus – Spider bite – Burn lesion • Pulmonary – Diverse bacterial and viral infections • Gastrointestinal – Shigella – Yersinia – Campylobacter • Meningitis – Tuberculosis – Amebic meningoencephalitis – Specific viral infections: Hantavirus, dengue, Ebola
Treatment / Medication
• Naturally acquired cutaneous anthrax in individuals over 2 years of age: - Administer oral ciprofloxacin (500 mg twice day for adults and 15 mg/kg twice daily, not to exceed 500 mg for children) for a duration of 7 to 10 days. - Oral doxycycline (100 mg twice daily in adults and 2.2 mg/kg—capped at 100 mg—twice daily in children) for a duration of 7 to 10 days If susceptibility testing is accessible, administer penicillin G 6–8 million units per day intravenously, penicillin VK 500 mg four times daily, and 50 mg/kg/day in children under 12 years, or amoxicillin orally 500 mg three times daily and 45 mg/kg/day in children to finish the treatment course. – Notwithstanding the possibility of resistance and inducible resistance, an administration of penicillin for approximately 7–10 days may be adequate for the treatment of naturally acquired simple cutaneous anthrax. Levofloxacin may be suggested as an alternative choice.
• For severe cases of spontaneously occurring cutaneous anthrax: – Administer IV ciprofloxacin 400 mg twice daily and 10 mg/kg twice daily in pediatric patients – Administer IV doxycycline 100 mg twice daily in adults and 2.2 mg/kg twice daily in pediatric patients • Cutaneous anthrax associated with bioterrorism: administer oral ciprofloxacin, oral doxycycline, or oral amoxicillin at the recommended dosages for 60 days to fulfill the complete course of postexposure prophylaxis. • For inhalational anthrax, gastrointestinal anthrax, and fulminant bacteremia: – Intravenous ciprofloxacin is preferred over intravenous doxycycline. The combination regimens may consist of IV ciprofloxacin or IV doxycycline in conjunction with one or two of the following agents: imipenem, meropenem, rifampin, vancomycin, penicillin, ampicillin, chloramphenicol, or clindamycin. • Employ a minimum of one drug with enough CNS penetration to address the potential for subclinical meningitis. Some experts recommend the inclusion of clindamycin to suppress endotoxin formation. A human IgG1λ monoclonal antibody targeting a component of the anthrax toxin (raxibacumab) enhanced survival in rabbits and monkeys afflicted with symptomatic inhalational anthrax (IA).
CONTINUED MANAGEMENT SUBSEQUENT SUGGESTIONS
Patients should be monitored for signs of disease recurrence following treatment.
COMPLICATIONS • Pulmonary and gastrointestinal disorders are typically lethal. • Cutaneous disease frequently results in scarring at the site of the eschar.

- Published on
Infectious Disease – Diarrhea and Fever
FUNDAMENTALS AND DESCRIPTION
Diarrhea is clinically defined as an elevation in daily stool weight above 200 grams and more broadly characterized as the occurrence of three or more loose stools daily. Diarrhea is classified as acute when it persists for less than 14 days and as chronic when it endures for more than 4 weeks. An inflammatory diarrheal syndrome is defined by frequent, small-volume feces that may be mucoid, bloody, or both. It may be associated with tenesmus, fever, or intense stomach pain. The defining characteristic of inflammatory diarrheas is the presence of leukocytes in the feces. A noninflammatory diarrheal condition is defined by the presence of voluminous watery stools (>1 L/d) that lack blood, pus, significant abdominal pain, or fever.
Epidemiology: Incidence Approximately 200 to 375 million instances of severe diarrhea transpire annually in the United States. Approximately 38 million of these events are ascribed to a recognized pathogen (bacteria, parasite, or virus). Foodborne transmission is responsible for approximately 36% of diarrheal diseases caused by identified pathogens. In 2007, of the 9 bacterial enteropathogens monitored by FoodNet, the predominant causes were non-typhoid salmonella (14.86 cases per 100,000 population), campylobacter (12.78), shigella (6.24), cryptosporidium (2.67), and Shiga toxin-producing E. coli (STEC) O157 (1.19). • The prevalence of bacterial diarrhea attributed to salmonella, campylobacter, and yersinia is greatest in infants under one year of age. The prevalence of post-diarrheal hemolytic uremic syndrome (HUS) in the United States is 0.65 instances per 100,000 individuals, with the highest frequency observed in children under five years of age. • Traveler's diarrhea impacts 20–60% of global travelers.
RISK FACTORS • Ingesting uncooked eggs, pork, shellfish, poultry, or unpasteurized dairy products. • Consuming unpurified water from streams or rivers. Conditions linked to heightened illness severity or increased susceptibility to specific pathogens encompass HIV infection, immunosuppressive therapies (such as glucocorticoids, TNF inhibitors, and chemotherapy), recent antibiotic administration, hepatic disease, neutropenia, malnutrition, zinc deficiency, and IgA deficiency. • Oral-anal sexual intercourse • Antibiotic exposure is a risk factor for C. difficile-associated diarrhea.
GENERAL PREVENTION
• Cleanse hands with soap prior to consuming or preparing food. • Refrain from ingesting raw or undercooked eggs, poultry, meat, fish, and seafood. • Avoid unpasteurized dairy products. • Do not consume untreated stream or river water. • When traveling, eschew tap water and ice in regions with potentially contaminated water. • Vaccines are accessible to prevent Salmonella typhi related to international travel. Refer to the CDC website for recommended immunizations according to your destination (http://www.cdc.gov/). The Advisory Committee on Immunization Practices recommends the rotavirus vaccine for infants in the United States. CAUSES Bacteria include Campylobacter, Salmonella species, E. coli (a. Enterotoxigenic [ETEC], b. Enteropathogenic [EPEC], c. Enteroinvasive [EIEC], d. Shiga toxin-producing [STEC] including E. coli O157:H7, and e. Enteroaggregative [EAEC]), Shigella species, Yersinia enterocolitica, Clostridium difficile, Vibrio cholera, Vibrio parahaemolyticus, Aeromonas species, and Plesiomonas shigelloides. • Viruses (Rotavirus, human caliciviruses including noroviruses, Adenovirus, and Cytomegalovirus) • Parasites (Giardia intestinalis, Cryptosporidium parvum, Entamoeba histolytica, Cyclospora cayetanensis, Isospora belli, and Strongyloides stercoralis) • Toxin-mediated diarrhea (Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens)
DIAGNOSIS HISTORY
A comprehensive medical history and physical examination are crucial for identifying the potential cause, severity, and existence of problems. • Inquire about recent travel, dietary habits, antibiotic consumption, sexual activity, attendance at day-care facilities, other illnesses, outbreaks, and seasonal factors. • Ascertain the frequency, duration, and nature of diarrhea (e.g., watery, bloody, etc.). • Infectious diarrhea may be accompanied by fever, chills, vomiting, nausea, stomach discomfort, and tenesmus. A history of dizziness, syncope, or presyncope suggests volume depletion. Bloody stools (dysentery) indicate the presence of an invasive infection, including Shigella, Salmonella, Campylobacter, Shiga toxin-producing E. coli (notably in the absence of fever), or Yersinia. Shiga toxin-producing E. coli, particularly O157:H7, induces watery diarrhea that progresses to bloody diarrhea and is linked to the consumption of contaminated beef or produce in around fifty percent of cases. Fever is frequently absent. Yersinia and Salmonella can infect the terminal ileum and cecum, presenting with right lower quadrant pain and tenderness indicative of acute appendicitis. • Watery diarrhea is clinically ambiguous. Gastroenteritis resulting from an enterotoxin (food poisoning) may be attributed to S. aureus, B. cereus, or C. perfringens. These instances may manifest with isolated vomiting (S. aureus or C. perfringens) or watery diarrhea (B. cereus or C. perfringens). Fever is typically absent. The incubation period is brief (2–7 hours for S. aureus; 8–14 hours for C. perfringens; C. perfringens may exhibit either duration) and the overall duration is limited. Extraintestinal signs, like arthritis, dermatological diseases, or eye problems, indicate the presence of inflammatory bowel disease. • The cause of recent overseas travel is contingent upon the place, environment, and season. The predominant pathogens comprise enterotoxigenic E. coli, enteroaggregative E. coli, Campylobacter, Salmonella, and norovirus. The CDC Travelers' Health website or other travel medicine resources can assist in diagnostic evaluation.
PHYSICAL EXAMINATION • Evaluate blood pressure, heart rate, respiration rate, temperature, and mental status to determine the severity. • Assess for indicators of dehydration such as xerostomia, impaired skin turgor, enophthalmos, reduced capillary refill time, low jugular venous pressure, or orthostatic hypotension. • Examine for abdominal discomfort, manifestations of peritonitis (guarding, rebound tenderness), hepatomegaly, and splenomegaly.
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Initial Assessments
• The indications for diagnostic testing encompass the following: Fever, systemic sickness, hematochezia, dehydration, a confirmed or suspected outbreak of foodborne illness, recent international travel, immunosuppression, or recent antibiotic administration. Submit stool specimen for culture analysis. In the majority of microbiology laboratories, stool samples submitted for the culture of enteric pathogens will be analyzed for Shigella, Salmonella, and Campylobacter. Consequently, if there is a strong clinical suspicion for E. coli (STEC, ETEC, EPEC, EIEC), Yersinia, Vibrio, etc., inform the microbiology laboratory. The diagnostic yield of stool cultures varies between 1.5% and 5.6%. • In cases with bloody diarrhea, do stool cultures for Salmonella, Shigella, Campylobacter, and Shiga toxin-producing E. coli, and conduct an immunoassay for Shiga toxin. Upon isolation of E. coli, dispatch to a reference laboratory for serotyping. • In cases of recent antibiotic use, hospitalization, daycare exposure, or chemotherapy, stool specimens should be analyzed for C. difficile toxins A and B. For diarrhea lasting over 7 days, collect numerous stool specimens for ova and parasite analysis, specifically targeting Giardia, Cryptosporidium, Isospora belli, and Cyclospora. Evaluate noninfectious etiology. In individuals with AIDS or immunosuppression, further test for microsporidia, Mycobacterium avium.
complex, and CMV. • A positive fecal test for polymorphonuclear cells indicates inflammatory diarrhea. Subsequent Actions & Unique Considerations In cases of dehydration or severe sickness, assess serum electrolytes, renal function, hepatic function, total blood count, and blood cultures. Imaging If the diagnosis is ambiguous, accompanied by critical illness, significant abdominal pain, or signs of peritonitis, consider performing a CT scan with both oral and intravenous contrast. Diagnostic Procedures and Additional Methods For additional assessment, contemplate upper gastrointestinal endoscopy or colonoscopy accompanied by diagnostic biopsies.
DIFFERENTIAL DIAGNOSIS • Acute inflammatory diarrheal syndrome may also arise from noninfectious causes, including ulcerative colitis, Crohn’s disease, radiation or ischemic colitis, partial bowel obstruction, diverticulitis, laxative abuse, rectosigmoid abscess, Whipple’s disease, pernicious anemia, diabetes, malabsorption, scleroderma, or celiac sprue. Diarrhea and fever may also arise from infections beyond the gastrointestinal tract, such as malaria or sepsis.
THERAPY PHARMACEUTICALS
The major elements of treatment consist of fluids and antibiotics. Oral rehydration constitutes the most suitable and cost-effective management strategy for both developing and wealthy nations. Intravenous volume repletion is warranted in cases of severe dehydration or significant electrolyte imbalance. The rice-based oral solution is more effective in adults and children suffering from cholera. Antimicrobial therapy is warranted in cases of severe infection and is advised for persistent gastroenteritis, individuals over 65 years of age, immunocompromised patients, those with prosthetic devices, and in instances of invasive infections, excluding those caused by Shiga toxin-producing E. coli. Empiric therapy: For febrile community-acquired invasive diarrhea or moderate to severe traveler's diarrhea, administer ciprofloxacin 500 mg twice day or levofloxacin 500 mg daily while awaiting stool investigations, unless Shiga toxin-producing E. coli is suspected. In the event of recent travel to Southeast Asia, investigate fluoroquinolone-resistant Campylobacter. If there has been recent antibiotic usage or nosocomial diarrhea, administer metronidazole or vancomycin while awaiting assay results for C. difficile toxin.
Chosen pathogens and their treatment: • Salmonella (non-typhi species) — Bacteremia manifests in 2–8% of cases. Administer treatment for severe disease in individuals under 12 months, over 50 years, with valvular disease, severe atherosclerosis, prosthetic devices, cancer, HIV, uremia, sickle cell disease, and other immunocompromised conditions. Ciprofloxacin 500 mg orally twice daily or levofloxacin 500 mg orally once daily for 5 to 7 days. If susceptible, provide TMP-SMX DS twice daily for 5–7 days, or ceftriaxone 2 g IV/IM daily for 5–7 days. Administer treatment for 14 days if the individual is immunocompromised. Antibiotics may augment shedding. • Shigellosis – provide ciprofloxacin 500 mg orally twice daily, or levofloxacin 500 mg once daily for 3 days, or if susceptible, TMP-SMX DS twice daily for 3 days. Administer treatment for 7 to 10 days in cases of severe disease or in immunocompromised individuals. • Campylobacter – provide erythromycin 500 mg bi-daily for a duration of 5 days. Significant fluoroquinolone resistance, particularly in Southeast Asia. • Escherichia coli, Shiga toxin-producing (STEC) – Avoid antibiotics as they may elevate the risk of hemolytic uremic syndrome (HUS).
Auxiliary care. • E. coli (ETEC, EPEC, EIEC) – provide ciprofloxacin 500 mg orally twice daily or levofloxacin 500 mg daily for a duration of 3 days. Administer TMP-SMX DS bi-daily for three days if susceptible. • Yersinia – antibiotics are generally unnecessary. For severe infections or immunocompromised patients, administer doxycycline in conjunction with an aminoglycoside, fluoroquinolone, or TMP-SMX. • C. difficile – discontinue superfluous antibiotics and use metronidazole 500 mg three times daily for moderate cases or vancomycin 125 mg four times daily for 10–14 days. Kindly refer to the pertinent subject. • Cholera: Fluid replenishment is essential. Examine local susceptibilities. Treatment options include doxycycline, tetracycline, TMP-SMX, or fluoroquinolone. Amebiasis: Administer metronidazole 750 mg three times daily for five days (ten days in severe cases), followed by paromomycin 500 mg three times daily for seven days, or iodoquinol 650 mg three times daily for twenty days. • Giardiasis: Metronidazole 250–750 mg administered thrice day for 7–10 days or tinidazole 2 g as a single dose • Cyclospora & Isospora – Administer TMP-SMX 1 DS bi-daily for a duration of 7–10 days. If immunocompromised, prolong treatment and contemplate suppression.
SUPPLEMENTARY THERAPY
Comprehensive Strategies • The majority of mild instances are self-resolving. Symptomatic treatment encompasses water and anti-motility medicines, including loperamide. Loperamide is the preferred antidiarrheal medication for people experiencing mild to moderate diarrhea without hematochezia. It is contraindicated in instances of severe inflammatory or bloody diarrhea, C. difficile infection, and in children under 2 years of age. Bismuth salicylate functions as an antisecretory agent and can diminish stool output in both children and adults. Concerns for Referral • In instances of severe or persistent diarrhea of indeterminate origin, consider consulting gastroenterology and/or infectious diseases specialists. • Document instances of Salmonella species, Shigella, Campylobacter, E. coli, cholera, cryptosporidiosis, cyclosporiasis, Vibrio species, and any suspected or confirmed outbreaks.
INPATIENT CONSIDERATIONS
Preliminary Stabilization Immediate rehydration and empirical antibiotics are necessary in cases of severe acute diarrhea accompanied by systemic toxicity. Criteria for Admission Admit individuals exhibiting severe dehydration or an inability to sustain fluid intake. Intravenous Fluids Intravenous volume repletion is warranted in cases of severe dehydration or when the patient exhibits changed mental status. Criteria for Discharge Patients may be discharged after fevers diminish for over 24 hours, vital signs stabilize, and the patient can sustain sufficient fluid and food intake.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Evaluate and administer treatment to families exhibiting like symptoms.
DIET • Nutritional intake may commence four hours following the initiation of oral or intravenous hydration. • Provide regular, little portions of easily digestible food. Avoid hyperosmolar fruit juices, as they may worsen diarrhea.
INFORMATION FOR PATIENTS
Instruct patients on general food safety practices and methods to prevent foodborne infections, particularly during travel. OUTLOOK Gastrointestinal diseases account for about 900,000 hospitalizations and 6,000 fatalities in the United States each year.
COMPLICATIONS
Complications encompass dehydration, electrolyte imbalances, bacteremia and sepsis, malnutrition and vitamin deficiency, hemolytic uremic syndrome (HUS), and systemic amebiasis.
FUNDAMENTALS AND DESCRIPTION
Diarrhea is clinically defined as an elevation in daily stool weight above 200 grams and more broadly characterized as the occurrence of three or more loose stools daily. Diarrhea is classified as acute when it persists for less than 14 days and as chronic when it endures for more than 4 weeks. An inflammatory diarrheal syndrome is defined by frequent, small-volume feces that may be mucoid, bloody, or both. It may be associated with tenesmus, fever, or intense stomach pain. The defining characteristic of inflammatory diarrheas is the presence of leukocytes in the feces. A noninflammatory diarrheal condition is defined by the presence of voluminous watery stools (>1 L/d) that lack blood, pus, significant abdominal pain, or fever.
Epidemiology: Incidence Approximately 200 to 375 million instances of severe diarrhea transpire annually in the United States. Approximately 38 million of these events are ascribed to a recognized pathogen (bacteria, parasite, or virus). Foodborne transmission is responsible for approximately 36% of diarrheal diseases caused by identified pathogens. In 2007, of the 9 bacterial enteropathogens monitored by FoodNet, the predominant causes were non-typhoid salmonella (14.86 cases per 100,000 population), campylobacter (12.78), shigella (6.24), cryptosporidium (2.67), and Shiga toxin-producing E. coli (STEC) O157 (1.19). • The prevalence of bacterial diarrhea attributed to salmonella, campylobacter, and yersinia is greatest in infants under one year of age. The prevalence of post-diarrheal hemolytic uremic syndrome (HUS) in the United States is 0.65 instances per 100,000 individuals, with the highest frequency observed in children under five years of age. • Traveler's diarrhea impacts 20–60% of global travelers.
RISK FACTORS • Ingesting uncooked eggs, pork, shellfish, poultry, or unpasteurized dairy products. • Consuming unpurified water from streams or rivers. Conditions linked to heightened illness severity or increased susceptibility to specific pathogens encompass HIV infection, immunosuppressive therapies (such as glucocorticoids, TNF inhibitors, and chemotherapy), recent antibiotic administration, hepatic disease, neutropenia, malnutrition, zinc deficiency, and IgA deficiency. • Oral-anal sexual intercourse • Antibiotic exposure is a risk factor for C. difficile-associated diarrhea.
GENERAL PREVENTION
• Cleanse hands with soap prior to consuming or preparing food. • Refrain from ingesting raw or undercooked eggs, poultry, meat, fish, and seafood. • Avoid unpasteurized dairy products. • Do not consume untreated stream or river water. • When traveling, eschew tap water and ice in regions with potentially contaminated water. • Vaccines are accessible to prevent Salmonella typhi related to international travel. Refer to the CDC website for recommended immunizations according to your destination (http://www.cdc.gov/). The Advisory Committee on Immunization Practices recommends the rotavirus vaccine for infants in the United States. CAUSES Bacteria include Campylobacter, Salmonella species, E. coli (a. Enterotoxigenic [ETEC], b. Enteropathogenic [EPEC], c. Enteroinvasive [EIEC], d. Shiga toxin-producing [STEC] including E. coli O157:H7, and e. Enteroaggregative [EAEC]), Shigella species, Yersinia enterocolitica, Clostridium difficile, Vibrio cholera, Vibrio parahaemolyticus, Aeromonas species, and Plesiomonas shigelloides. • Viruses (Rotavirus, human caliciviruses including noroviruses, Adenovirus, and Cytomegalovirus) • Parasites (Giardia intestinalis, Cryptosporidium parvum, Entamoeba histolytica, Cyclospora cayetanensis, Isospora belli, and Strongyloides stercoralis) • Toxin-mediated diarrhea (Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens)
DIAGNOSIS HISTORY
A comprehensive medical history and physical examination are crucial for identifying the potential cause, severity, and existence of problems. • Inquire about recent travel, dietary habits, antibiotic consumption, sexual activity, attendance at day-care facilities, other illnesses, outbreaks, and seasonal factors. • Ascertain the frequency, duration, and nature of diarrhea (e.g., watery, bloody, etc.). • Infectious diarrhea may be accompanied by fever, chills, vomiting, nausea, stomach discomfort, and tenesmus. A history of dizziness, syncope, or presyncope suggests volume depletion. Bloody stools (dysentery) indicate the presence of an invasive infection, including Shigella, Salmonella, Campylobacter, Shiga toxin-producing E. coli (notably in the absence of fever), or Yersinia. Shiga toxin-producing E. coli, particularly O157:H7, induces watery diarrhea that progresses to bloody diarrhea and is linked to the consumption of contaminated beef or produce in around fifty percent of cases. Fever is frequently absent. Yersinia and Salmonella can infect the terminal ileum and cecum, presenting with right lower quadrant pain and tenderness indicative of acute appendicitis. • Watery diarrhea is clinically ambiguous. Gastroenteritis resulting from an enterotoxin (food poisoning) may be attributed to S. aureus, B. cereus, or C. perfringens. These instances may manifest with isolated vomiting (S. aureus or C. perfringens) or watery diarrhea (B. cereus or C. perfringens). Fever is typically absent. The incubation period is brief (2–7 hours for S. aureus; 8–14 hours for C. perfringens; C. perfringens may exhibit either duration) and the overall duration is limited. Extraintestinal signs, like arthritis, dermatological diseases, or eye problems, indicate the presence of inflammatory bowel disease. • The cause of recent overseas travel is contingent upon the place, environment, and season. The predominant pathogens comprise enterotoxigenic E. coli, enteroaggregative E. coli, Campylobacter, Salmonella, and norovirus. The CDC Travelers' Health website or other travel medicine resources can assist in diagnostic evaluation.
PHYSICAL EXAMINATION • Evaluate blood pressure, heart rate, respiration rate, temperature, and mental status to determine the severity. • Assess for indicators of dehydration such as xerostomia, impaired skin turgor, enophthalmos, reduced capillary refill time, low jugular venous pressure, or orthostatic hypotension. • Examine for abdominal discomfort, manifestations of peritonitis (guarding, rebound tenderness), hepatomegaly, and splenomegaly.
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Initial Assessments
• The indications for diagnostic testing encompass the following: Fever, systemic sickness, hematochezia, dehydration, a confirmed or suspected outbreak of foodborne illness, recent international travel, immunosuppression, or recent antibiotic administration. Submit stool specimen for culture analysis. In the majority of microbiology laboratories, stool samples submitted for the culture of enteric pathogens will be analyzed for Shigella, Salmonella, and Campylobacter. Consequently, if there is a strong clinical suspicion for E. coli (STEC, ETEC, EPEC, EIEC), Yersinia, Vibrio, etc., inform the microbiology laboratory. The diagnostic yield of stool cultures varies between 1.5% and 5.6%. • In cases with bloody diarrhea, do stool cultures for Salmonella, Shigella, Campylobacter, and Shiga toxin-producing E. coli, and conduct an immunoassay for Shiga toxin. Upon isolation of E. coli, dispatch to a reference laboratory for serotyping. • In cases of recent antibiotic use, hospitalization, daycare exposure, or chemotherapy, stool specimens should be analyzed for C. difficile toxins A and B. For diarrhea lasting over 7 days, collect numerous stool specimens for ova and parasite analysis, specifically targeting Giardia, Cryptosporidium, Isospora belli, and Cyclospora. Evaluate noninfectious etiology. In individuals with AIDS or immunosuppression, further test for microsporidia, Mycobacterium avium.
complex, and CMV. • A positive fecal test for polymorphonuclear cells indicates inflammatory diarrhea. Subsequent Actions & Unique Considerations In cases of dehydration or severe sickness, assess serum electrolytes, renal function, hepatic function, total blood count, and blood cultures. Imaging If the diagnosis is ambiguous, accompanied by critical illness, significant abdominal pain, or signs of peritonitis, consider performing a CT scan with both oral and intravenous contrast. Diagnostic Procedures and Additional Methods For additional assessment, contemplate upper gastrointestinal endoscopy or colonoscopy accompanied by diagnostic biopsies.
DIFFERENTIAL DIAGNOSIS • Acute inflammatory diarrheal syndrome may also arise from noninfectious causes, including ulcerative colitis, Crohn’s disease, radiation or ischemic colitis, partial bowel obstruction, diverticulitis, laxative abuse, rectosigmoid abscess, Whipple’s disease, pernicious anemia, diabetes, malabsorption, scleroderma, or celiac sprue. Diarrhea and fever may also arise from infections beyond the gastrointestinal tract, such as malaria or sepsis.
THERAPY PHARMACEUTICALS
The major elements of treatment consist of fluids and antibiotics. Oral rehydration constitutes the most suitable and cost-effective management strategy for both developing and wealthy nations. Intravenous volume repletion is warranted in cases of severe dehydration or significant electrolyte imbalance. The rice-based oral solution is more effective in adults and children suffering from cholera. Antimicrobial therapy is warranted in cases of severe infection and is advised for persistent gastroenteritis, individuals over 65 years of age, immunocompromised patients, those with prosthetic devices, and in instances of invasive infections, excluding those caused by Shiga toxin-producing E. coli. Empiric therapy: For febrile community-acquired invasive diarrhea or moderate to severe traveler's diarrhea, administer ciprofloxacin 500 mg twice day or levofloxacin 500 mg daily while awaiting stool investigations, unless Shiga toxin-producing E. coli is suspected. In the event of recent travel to Southeast Asia, investigate fluoroquinolone-resistant Campylobacter. If there has been recent antibiotic usage or nosocomial diarrhea, administer metronidazole or vancomycin while awaiting assay results for C. difficile toxin.
Chosen pathogens and their treatment: • Salmonella (non-typhi species) — Bacteremia manifests in 2–8% of cases. Administer treatment for severe disease in individuals under 12 months, over 50 years, with valvular disease, severe atherosclerosis, prosthetic devices, cancer, HIV, uremia, sickle cell disease, and other immunocompromised conditions. Ciprofloxacin 500 mg orally twice daily or levofloxacin 500 mg orally once daily for 5 to 7 days. If susceptible, provide TMP-SMX DS twice daily for 5–7 days, or ceftriaxone 2 g IV/IM daily for 5–7 days. Administer treatment for 14 days if the individual is immunocompromised. Antibiotics may augment shedding. • Shigellosis – provide ciprofloxacin 500 mg orally twice daily, or levofloxacin 500 mg once daily for 3 days, or if susceptible, TMP-SMX DS twice daily for 3 days. Administer treatment for 7 to 10 days in cases of severe disease or in immunocompromised individuals. • Campylobacter – provide erythromycin 500 mg bi-daily for a duration of 5 days. Significant fluoroquinolone resistance, particularly in Southeast Asia. • Escherichia coli, Shiga toxin-producing (STEC) – Avoid antibiotics as they may elevate the risk of hemolytic uremic syndrome (HUS).
Auxiliary care. • E. coli (ETEC, EPEC, EIEC) – provide ciprofloxacin 500 mg orally twice daily or levofloxacin 500 mg daily for a duration of 3 days. Administer TMP-SMX DS bi-daily for three days if susceptible. • Yersinia – antibiotics are generally unnecessary. For severe infections or immunocompromised patients, administer doxycycline in conjunction with an aminoglycoside, fluoroquinolone, or TMP-SMX. • C. difficile – discontinue superfluous antibiotics and use metronidazole 500 mg three times daily for moderate cases or vancomycin 125 mg four times daily for 10–14 days. Kindly refer to the pertinent subject. • Cholera: Fluid replenishment is essential. Examine local susceptibilities. Treatment options include doxycycline, tetracycline, TMP-SMX, or fluoroquinolone. Amebiasis: Administer metronidazole 750 mg three times daily for five days (ten days in severe cases), followed by paromomycin 500 mg three times daily for seven days, or iodoquinol 650 mg three times daily for twenty days. • Giardiasis: Metronidazole 250–750 mg administered thrice day for 7–10 days or tinidazole 2 g as a single dose • Cyclospora & Isospora – Administer TMP-SMX 1 DS bi-daily for a duration of 7–10 days. If immunocompromised, prolong treatment and contemplate suppression.
SUPPLEMENTARY THERAPY
Comprehensive Strategies • The majority of mild instances are self-resolving. Symptomatic treatment encompasses water and anti-motility medicines, including loperamide. Loperamide is the preferred antidiarrheal medication for people experiencing mild to moderate diarrhea without hematochezia. It is contraindicated in instances of severe inflammatory or bloody diarrhea, C. difficile infection, and in children under 2 years of age. Bismuth salicylate functions as an antisecretory agent and can diminish stool output in both children and adults. Concerns for Referral • In instances of severe or persistent diarrhea of indeterminate origin, consider consulting gastroenterology and/or infectious diseases specialists. • Document instances of Salmonella species, Shigella, Campylobacter, E. coli, cholera, cryptosporidiosis, cyclosporiasis, Vibrio species, and any suspected or confirmed outbreaks.
INPATIENT CONSIDERATIONS
Preliminary Stabilization Immediate rehydration and empirical antibiotics are necessary in cases of severe acute diarrhea accompanied by systemic toxicity. Criteria for Admission Admit individuals exhibiting severe dehydration or an inability to sustain fluid intake. Intravenous Fluids Intravenous volume repletion is warranted in cases of severe dehydration or when the patient exhibits changed mental status. Criteria for Discharge Patients may be discharged after fevers diminish for over 24 hours, vital signs stabilize, and the patient can sustain sufficient fluid and food intake.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Evaluate and administer treatment to families exhibiting like symptoms.
DIET • Nutritional intake may commence four hours following the initiation of oral or intravenous hydration. • Provide regular, little portions of easily digestible food. Avoid hyperosmolar fruit juices, as they may worsen diarrhea.
INFORMATION FOR PATIENTS
Instruct patients on general food safety practices and methods to prevent foodborne infections, particularly during travel. OUTLOOK Gastrointestinal diseases account for about 900,000 hospitalizations and 6,000 fatalities in the United States each year.
COMPLICATIONS
Complications encompass dehydration, electrolyte imbalances, bacteremia and sepsis, malnutrition and vitamin deficiency, hemolytic uremic syndrome (HUS), and systemic amebiasis.
- Published on
Infectious Disease - Babesiosis
FUNDAMENTALS AND DESCRIPTION
Babesia is a protozoan that exhibits a preference for human erythrocytes. It is a prevalent etiology of hemolytic illness in endemic regions. The primary mode of transmission for Babesia microti is by bites from deer ticks (Ixodid species). Alternative, less prevalent transmission methods encompass blood transfusions and maternal transmission of babesiosis. The majority of B. microti is predominantly located in the Northeastern and Midwestern regions of the United States. Additional Babesia species are present in the western United States and Europe.
EPIDEMIOLOGY
• Babesia is classified as an emerging infectious illness due to the rising incidence of reported cases over the past decade. • The escalation of deer populations, tick density, and heightened human activity in endemic regions are believed to contribute to the increase in Babesia infections. • Numerous cases of Babesia remain subclinical in younger persons, suggesting that the incidence of this infection is likely underestimated. Data from blood donors indicate that 0.5–15% of individuals have been exposed in highly endemic regions.
FACTORS OF RISK
• Residing in or visiting endemic areas. • Patients without a spleen. • Immunosuppression (e.g., HIV, chemotherapy).
COMPREHENSIVE PREVENTION
• Individuals who are asplenic or immunocompromised, and so at heightened risk of severe illness, should avoid endemic locations during periods of elevated transmission, namely from May to October (3). Insect repellent is effective in preventing tick bites, particularly ones containing N-diethyl-meta-toluamide (DEET). Early removal of ticks is crucial; the tick must be attached for a minimum of 24 hours before transmission commences. Daily self-assessment is advised for individuals participating in outdoor activities in endemic regions. It is advisable to inspect pets for ticks in endemic regions. Clothing can be treated with permethrin to avert infection.
PATHOPHYSIOLOGY
The life cycle include the transmission of Babesia between vertebrate hosts and Ixodes ticks. Humans serve as "dead end" and "accidental" hosts, with the predominant transmission vectors for B. microti being white-footed mice and ticks. Humans may become unwell upon infection; yet, they do not contribute to the transmission of the pathogen. Ixodes ticks deliver sporozoites to the host's bloodstream. The sporozoites infiltrate the erythrocytes and transform into trophozoites. The trophozoites reproduce asexually through budding, resulting in 2–4 merozoites. The merozoites compromise red blood cells (RBCs) and infiltrate other RBCs, resulting in hemolysis and anemia. ETIOLOGY • The predominant cause of Babesia in the United States is B. microti, which is prevalent in New England, coastal New York, and the Midwest. Other prevalent Babesia species that induce sickness in humans are Babesia divergens in Europe and Babesia duncani in the Western United States.
FREQUENTLY CO-OCCURRING CONDITIONS
Co-infection with Lyme disease and human granulocytic anaplasmosis frequently occurs, as both are transmitted by Ixodes ticks in endemic areas. In endemic regions, up to 10% of those diagnosed with Lyme disease are concurrently infected with Babesia.
DIAGNOSIS HISTORY
Patients may be asymptomatic or exhibit the following symptoms: • Pyrexia • Rigors • Asthenia • Cephalalgia • Nausea/emesis • Abdominal discomfort • Diarrhea • Arthralgia • Dyspnea/thoracic pain • Darkened urine Inquire about recent Lyme disease illness, residence or travel in endemic regions, outdoor exposures, pet ownership, and recent tick bites.
PHYSICAL EXAMINATION
• Pyrexia • Splenomegaly • Hepatomegaly • Pallor • Icterus • Absence of lymphadenopathy • Assess for a rash indicative of erythema chronicum migrans in instances of Lyme co-infection
DIAGNOSTIC EXAMINATIONS & ANALYSIS
Laboratory Initial Assessments • Prepare thin blood smears to evaluate for intra-erythrocytic parasites and indications of hemolysis. In instances of low parasitemia and early infection, multiple blood smears may be required over several days. • Complete blood count: Anemia and thrombocytopenia detected. • Indicators of hemolysis: Increased reticulocyte count, LDH, and indirect bilirubin levels. Additionally, haptoglobin levels are low. • Hepatic function assays. Subsequent Actions & Unique Considerations • If the bacterium is undetected via blood smear, PCR amplification of 18S rRNA is advised. In patients with a significant likelihood of infection, indirect immunofluorescent antibody testing is advised when both blood smear and PCR results are negative. Imaging Imaging is typically unnecessary in moderate situations. Abdominal ultrasonography will verify hepatomegaly or splenomegaly. Pathological Observations Similar to malaria, Babesia manifests as an intra-erythrocytic parasite. Babesia parasites may be observed outside of red blood cells during severe infections, a phenomenon not present in malarial infections. At times, Babesia parasites (in the internal merozoite phase) manifest in tetrads, referred to as the "Maltese cross."
Differential Diagnosis: • Sepsis • Lyme Disease • Human Granulocytic Anaplasmosis • Hepatitis • Malaria • Lymphoma
TREATMENT MEDICATION
For B. microti infection: administer oral atovaquone 750 mg twice daily for 7–10 days, in conjunction with oral azithromycin 500–1,000 mg on day 1, followed by 250 mg daily thereafter. Second Line For B. microti infection: Administer oral quinine 650 mg three or four times daily in conjunction with oral clindamycin 600 mg three times daily for a duration of 7 to 10 days. Intravenous formulations are applicable. Quinine and clindamycin are utilized in critical instances.
SUPPLEMENTARY THERAPY
Comprehensive Strategies Asymptomatic immunocompetent people with detectable parasites on blood smear for less than three months do not necessitate treatment (5). Extended treatment durations may be required for immunocompromised individuals or in instances of significant parasite load. Treatment must persist for a minimum of 6 weeks, encompassing 2 weeks of therapy following the undetectability of parasites in blood smears. Concerns for Referral An infectious disease specialist should be consulted if there are indications of serious infection or infection in an immunocompromised individual. Supplementary Treatments Red blood cell exchange transfusions may be required in severe instances of excessive parasitemia (>10%) or the presence of shock/ARDS symptoms.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patient Surveillance Hospitalized patients should undergo daily CBC and blood smear assessments to monitor for hemolysis, anemia, and parasite load.
INFORMATION FOR PATIENTS
Educate patients of the risk factors associated with Babesia transmission and implement measures to prevent re-infection.
COMPLICATIONS
• Disseminated Intravascular Coagulation (DIC) • Anemia • Congestive Heart Failure (CHF) • Acute Respiratory Distress Syndrome (ARDS) • Renal Dysfunction • Hypotension
FUNDAMENTALS AND DESCRIPTION
Babesia is a protozoan that exhibits a preference for human erythrocytes. It is a prevalent etiology of hemolytic illness in endemic regions. The primary mode of transmission for Babesia microti is by bites from deer ticks (Ixodid species). Alternative, less prevalent transmission methods encompass blood transfusions and maternal transmission of babesiosis. The majority of B. microti is predominantly located in the Northeastern and Midwestern regions of the United States. Additional Babesia species are present in the western United States and Europe.
EPIDEMIOLOGY
• Babesia is classified as an emerging infectious illness due to the rising incidence of reported cases over the past decade. • The escalation of deer populations, tick density, and heightened human activity in endemic regions are believed to contribute to the increase in Babesia infections. • Numerous cases of Babesia remain subclinical in younger persons, suggesting that the incidence of this infection is likely underestimated. Data from blood donors indicate that 0.5–15% of individuals have been exposed in highly endemic regions.
FACTORS OF RISK
• Residing in or visiting endemic areas. • Patients without a spleen. • Immunosuppression (e.g., HIV, chemotherapy).
COMPREHENSIVE PREVENTION
• Individuals who are asplenic or immunocompromised, and so at heightened risk of severe illness, should avoid endemic locations during periods of elevated transmission, namely from May to October (3). Insect repellent is effective in preventing tick bites, particularly ones containing N-diethyl-meta-toluamide (DEET). Early removal of ticks is crucial; the tick must be attached for a minimum of 24 hours before transmission commences. Daily self-assessment is advised for individuals participating in outdoor activities in endemic regions. It is advisable to inspect pets for ticks in endemic regions. Clothing can be treated with permethrin to avert infection.
PATHOPHYSIOLOGY
The life cycle include the transmission of Babesia between vertebrate hosts and Ixodes ticks. Humans serve as "dead end" and "accidental" hosts, with the predominant transmission vectors for B. microti being white-footed mice and ticks. Humans may become unwell upon infection; yet, they do not contribute to the transmission of the pathogen. Ixodes ticks deliver sporozoites to the host's bloodstream. The sporozoites infiltrate the erythrocytes and transform into trophozoites. The trophozoites reproduce asexually through budding, resulting in 2–4 merozoites. The merozoites compromise red blood cells (RBCs) and infiltrate other RBCs, resulting in hemolysis and anemia. ETIOLOGY • The predominant cause of Babesia in the United States is B. microti, which is prevalent in New England, coastal New York, and the Midwest. Other prevalent Babesia species that induce sickness in humans are Babesia divergens in Europe and Babesia duncani in the Western United States.
FREQUENTLY CO-OCCURRING CONDITIONS
Co-infection with Lyme disease and human granulocytic anaplasmosis frequently occurs, as both are transmitted by Ixodes ticks in endemic areas. In endemic regions, up to 10% of those diagnosed with Lyme disease are concurrently infected with Babesia.
DIAGNOSIS HISTORY
Patients may be asymptomatic or exhibit the following symptoms: • Pyrexia • Rigors • Asthenia • Cephalalgia • Nausea/emesis • Abdominal discomfort • Diarrhea • Arthralgia • Dyspnea/thoracic pain • Darkened urine Inquire about recent Lyme disease illness, residence or travel in endemic regions, outdoor exposures, pet ownership, and recent tick bites.
PHYSICAL EXAMINATION
• Pyrexia • Splenomegaly • Hepatomegaly • Pallor • Icterus • Absence of lymphadenopathy • Assess for a rash indicative of erythema chronicum migrans in instances of Lyme co-infection
DIAGNOSTIC EXAMINATIONS & ANALYSIS
Laboratory Initial Assessments • Prepare thin blood smears to evaluate for intra-erythrocytic parasites and indications of hemolysis. In instances of low parasitemia and early infection, multiple blood smears may be required over several days. • Complete blood count: Anemia and thrombocytopenia detected. • Indicators of hemolysis: Increased reticulocyte count, LDH, and indirect bilirubin levels. Additionally, haptoglobin levels are low. • Hepatic function assays. Subsequent Actions & Unique Considerations • If the bacterium is undetected via blood smear, PCR amplification of 18S rRNA is advised. In patients with a significant likelihood of infection, indirect immunofluorescent antibody testing is advised when both blood smear and PCR results are negative. Imaging Imaging is typically unnecessary in moderate situations. Abdominal ultrasonography will verify hepatomegaly or splenomegaly. Pathological Observations Similar to malaria, Babesia manifests as an intra-erythrocytic parasite. Babesia parasites may be observed outside of red blood cells during severe infections, a phenomenon not present in malarial infections. At times, Babesia parasites (in the internal merozoite phase) manifest in tetrads, referred to as the "Maltese cross."
Differential Diagnosis: • Sepsis • Lyme Disease • Human Granulocytic Anaplasmosis • Hepatitis • Malaria • Lymphoma
TREATMENT MEDICATION
For B. microti infection: administer oral atovaquone 750 mg twice daily for 7–10 days, in conjunction with oral azithromycin 500–1,000 mg on day 1, followed by 250 mg daily thereafter. Second Line For B. microti infection: Administer oral quinine 650 mg three or four times daily in conjunction with oral clindamycin 600 mg three times daily for a duration of 7 to 10 days. Intravenous formulations are applicable. Quinine and clindamycin are utilized in critical instances.
SUPPLEMENTARY THERAPY
Comprehensive Strategies Asymptomatic immunocompetent people with detectable parasites on blood smear for less than three months do not necessitate treatment (5). Extended treatment durations may be required for immunocompromised individuals or in instances of significant parasite load. Treatment must persist for a minimum of 6 weeks, encompassing 2 weeks of therapy following the undetectability of parasites in blood smears. Concerns for Referral An infectious disease specialist should be consulted if there are indications of serious infection or infection in an immunocompromised individual. Supplementary Treatments Red blood cell exchange transfusions may be required in severe instances of excessive parasitemia (>10%) or the presence of shock/ARDS symptoms.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patient Surveillance Hospitalized patients should undergo daily CBC and blood smear assessments to monitor for hemolysis, anemia, and parasite load.
INFORMATION FOR PATIENTS
Educate patients of the risk factors associated with Babesia transmission and implement measures to prevent re-infection.
COMPLICATIONS
• Disseminated Intravascular Coagulation (DIC) • Anemia • Congestive Heart Failure (CHF) • Acute Respiratory Distress Syndrome (ARDS) • Renal Dysfunction • Hypotension
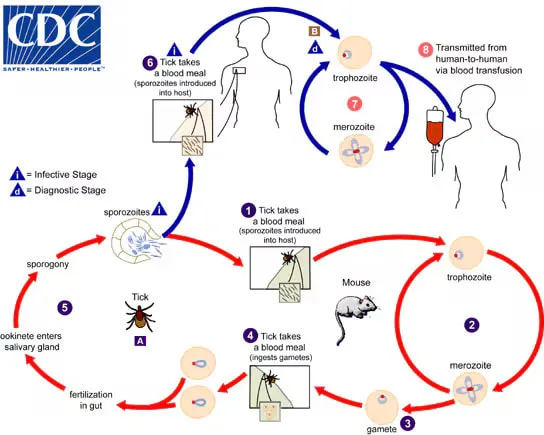
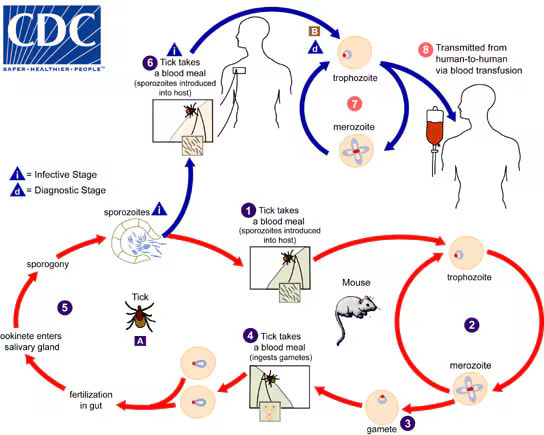
- Published on
Infectious Disease - Appendicitis
FUNDAMENTALS OVERVIEW
• Appendicitis refers to the inflammation of the appendix. • When the blood supply to the appendix is impaired, it is termed “gangrenous appendicitis.” When appendicitis is complicated by perforation, it is referred to as "perforating appendicitis." When appendicitis is caused by a blockage of the lumen, it is referred to as "obstructive appendicitis."
EPIDEMIOLOGY
Incidence Appendectomy is the most common indication for abdominal surgery. Annually in the United States, there are a minimum of 250,000 instances of appendicitis, necessitating over 1 million inpatient hospital days. • The appendix appears normal in around one-third of patients who need emergency appendectomy. • Missed appendicitis ranks among the most commonly successful malpractice claims against emergency room clinicians.
RISK FACTORS
Males exhibit a little greater rate than females, with a male-to-female ratio of 3:2. The lifetime risk of appendicitis is 8.5% for males and 6.7% for females. • Acute appendicitis may manifest at any age, with peak incidence observed during the second and third decades of life. • Perforation is more prevalent among infants and the elderly.
PATHOPHYSIOLOGY
• Luminal blockage is the principal etiology of appendicitis. • The obstruction is most frequently attributed to a fecalith, but may also result from foreign bodies, increased lymphoid hyperplasia linked to viral infections (e.g., measles), helminths, or neoplasms (e.g., carcinoid or carcinoma). • Mucus accumulates behind the obstruction, leading to bacterial proliferation and invasion of the appendiceal wall, which causes venous engorgement and subsequent arterial impairment and ischemia due to elevated intraluminal pressures. • Ultimately, gangrene and perforation ensue. Rupture of primary appendiceal abscesses may result in fistulas. • Acute appendicitis may, at times, serve as the initial symptom of Crohn’s disease. • Infrequently, recurrent acute appendicitis may manifest with complete remission of inflammation and symptoms between episodes.
ETIOLOGY • Proliferation of several gastrointestinal bacteria (E. coli, Peptostreptococcus, B. fragilis, Enterobacteriaceae, viridans streptococcus) transpires within the obstructed appendix. • Chronic appendiceal infection may arise from tuberculosis, amebiasis, and actinomycosis.
DIAGNOSIS HISTORY
The onset of pain transpires across several hours. The earliest visceral abdominal pain of appendicitis is colicky and typically poorly localized in the periumbilical or epigastric area. As inflammation spreads to the parietal peritoneal surfaces, the pain becomes somatic, steady, and more intense. The pain intensifies with movement or coughing and is localized in the right lower quadrant (McBurney's point). • An associated need to defecate or expel flatus frequently occurs, neither of which alleviates the discomfort. Anorexia is prevalent enough that the manifestation of hunger should raise concern for a diagnosis of acute appendicitis. Nausea and vomiting manifest in 50–60% of instances; however, vomiting is seldom severe and prolonged. The occurrence of nausea and vomiting prior to the onset of pain is exceedingly uncommon. • Urinary frequency and dysuria manifest when the appendix is positioned near to the bladder.
PHYSICAL EXAM • Physical results fluctuate over time following the commencement of the illness and are contingent upon the appendix's position. • Tenderness may initially be absent in the early visceral stage of the disease, but it eventually manifests in the area corresponding to the appendix's location. Pregnant women frequently exhibit pain in the right upper quadrant. Guarding is a result of parietal peritoneal involvement. Tenderness upon percussion, rebound tenderness, and referred rebound tenderness are frequently observed. Rebound soreness in the right lower quadrant during probing of the left lower quadrant is referred to as "Rovsing's sign." Pain induced by passive flexion of the right hip is referred to as "the psoas sign"; pain induced by internal rotation of the right hip is referred to as "the obturator sign." • The temperature is often normal or marginally elevated; however, a temperature beyond 38.3°C (101°F) indicates potential perforation. • A discernible mass in the right lower quadrant implies the possibility of an abscess or cecal cancer.
DIAGNOSTIC TESTS AND INTERPRETATION Lab
Leukocytosis ranging from 10,000 to 18,000 cells per milliliter with a left shift is prevalent; however, the lack of leukocytosis does not preclude the diagnosis of acute appendicitis. A pregnancy test must be conducted for all women of childbearing age to exclude the possibility of uterine or ectopic pregnancy. Imaging: Preliminary Strategy Among noninvasive diagnostic tools, appendiceal CT has demonstrated superior precision, achieving an accuracy of 90%. The greatest accuracy has been documented with helical CT following the administration of a 3% diatrizoate meglumine (Gastrografin)–saline solution into the colon. Appendiceal CT is safe, can be conducted in roughly 15 minutes, and necessitates only one-third of the radiation exposure compared to normal CT of the belly and pelvis. Routine appendiceal CT conducted in patients with probable appendicitis enhances patient care and diminishes the utilization of hospital resources. Ultrasound is particularly beneficial for women of childbearing age to rule out ovarian cysts, ectopic pregnancy, or tubo-ovarian abscess. It is also utilized in pediatrics. Normal ultrasonographic findings should not dissuade the surgeon from conducting an appendectomy if the clinical history suggests appendicitis and there is definitive discomfort in the right lower quadrant. Subsequent Actions & Unique Considerations The management strategies for clinicians assessing patients with suspected appendicitis including observation, diagnostic imaging, laparoscopy, and appendectomy. • Patients with a history strongly indicative of appendicitis are frequently sent to the operating room for laparoscopy, irrespective of imaging outcomes. • Patients with a less compelling history are typically subjected to imaging or monitoring. Histopathological Observations Pathology specimens from acute appendicitis exhibit indicators of inflammation, including polymorphonuclear leukocytes, edema, and vascular congestion in the appendiceal walls.
DIFFERENTIAL DIAGNOSIS • The lack of right lower quadrant pain, the absence of typical pain migration, and a history of analogous pain render appendicitis less probable. The absence of right lower quadrant discomfort, rigidity, or guarding during the physical examination diminishes the likelihood of appendicitis. • The differential diagnosis of acute appendicitis encompasses the following: – Acute cholecystitis – Acute diverticulitis – Acute gastroenteritis – Acute pancreatitis – Acute pelvic inflammatory illness – Endometriosis – Mesenteric lymphadenitis – Perforated ulcer – Pyelonephritis – Ruptured Graafian follicle or corpus luteum cyst – Ruptured ectopic pregnancy – Strangulating intestinal blockage – Torted ovarian cyst – Ureteral calculus The differential diagnosis of acute appendicitis is elaborated upon in Section I, chapter "Abdominal Pain and Fever."
THERAPY
The principal intervention for appendicitis is immediate surgical intervention. Antibiotics are the normal preoperative treatment and must be effective against gram-negative aerobes and anaerobes.
MEDICATION • Antibiotic care parallels that of other intra-abdominal infections, as elaborated in Section II chapters, “Peritonitis” and “Intra-abdominal Abscess.” • Options comprise: – Beta-lactam and beta-lactamase inhibitor (ampicillin–sulbactam, piperacillin–tazobactam, ticarcillin–clavulanate) – Ceftriaxone and metronidazole – Fluoroquinolone and metronidazole - Carbapenems (imipenem, meropenem)
SUPPLEMENTARY THERAPY
Referral Considerations Surgical intervention should be integrated into the management of a patient with suspected appendicitis from the moment of initial presentation.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Prompt surgical assessment of a patient with a compelling history and/or imaging indicative of appendicitis is essential. • Both laparoscopic and open techniques are permissible. Patients undergoing laparoscopic surgery experience fewer wound infections, reduced discomfort, and shorter hospital stays compared to those undergoing open surgery. Nonetheless, laparoscopic appendectomies are correlated with an increased incidence of intra-abdominal abscesses, extended operative durations, and elevated surgical expenses. • If a palpable mass is detected 3–5 days post-symptom onset, the procedure should be postponed, since a phlegmon rather than a definite abscess is likely to be present. Patients should get broad-spectrum antibiotics, parenteral fluids, and rest. An appendectomy should be performed safely three months later. If the tumor increases in size or the patient exhibits heightened toxicity, abscess drainage is required.
INPATIENT CONSIDERATIONS
Preliminary Stabilization If unstable, the patient with appendicitis is likely experiencing sepsis or has a perforated appendix with subsequent peritonitis. The patient requires resuscitation with intravenous fluids, and vasopressors should be administered if deemed required. Admission Criteria All patients with suspected appendicitis must be admitted. Intravenous Fluids Patients should be thoroughly hydrated preoperatively, and electrolyte imbalances must be corrected. Criteria for Discharge Discharge criteria encompass the normalization of white blood cell count, the resolution of fever, and the restoration of bowel function.
CONTINUING MANAGEMENT POST-TREATMENT SUGGESTIONS
Close monitoring of patients with stomach pain who do not undergo additional diagnostic testing is warranted.
NUTRITION
Individuals suspected of having appendicitis should refrain from eating.
PROGNOSIS • The mortality rate in Europe and the US has consistently declined to less than 1 per 100,000. The general mortality rate for perforated appendicitis is 3%, escalating to 15% in the elderly population.
COMPLICATIONS
The postponement of appendicitis diagnosis elevates the likelihood of appendiceal perforation, which is linked to postoperative complications in as many as 40% of patients, in contrast to 5–10% for uncomplicated appendicitis. Perforation is uncommon within the first 24 hours of symptom onset, but the incidence increases to 80% after 48 hours. The formation of intra-abdominal abscesses or phlegmon typically occurs subsequent to perforation accompanied by generalized peritonitis and can be prevented with early disease detection. • Wounds must be monitored for indications of infection. • Portal vein thrombophlebitis and pyogenic liver abscess are rare occurrences.
FUNDAMENTALS OVERVIEW
• Appendicitis refers to the inflammation of the appendix. • When the blood supply to the appendix is impaired, it is termed “gangrenous appendicitis.” When appendicitis is complicated by perforation, it is referred to as "perforating appendicitis." When appendicitis is caused by a blockage of the lumen, it is referred to as "obstructive appendicitis."
EPIDEMIOLOGY
Incidence Appendectomy is the most common indication for abdominal surgery. Annually in the United States, there are a minimum of 250,000 instances of appendicitis, necessitating over 1 million inpatient hospital days. • The appendix appears normal in around one-third of patients who need emergency appendectomy. • Missed appendicitis ranks among the most commonly successful malpractice claims against emergency room clinicians.
RISK FACTORS
Males exhibit a little greater rate than females, with a male-to-female ratio of 3:2. The lifetime risk of appendicitis is 8.5% for males and 6.7% for females. • Acute appendicitis may manifest at any age, with peak incidence observed during the second and third decades of life. • Perforation is more prevalent among infants and the elderly.
PATHOPHYSIOLOGY
• Luminal blockage is the principal etiology of appendicitis. • The obstruction is most frequently attributed to a fecalith, but may also result from foreign bodies, increased lymphoid hyperplasia linked to viral infections (e.g., measles), helminths, or neoplasms (e.g., carcinoid or carcinoma). • Mucus accumulates behind the obstruction, leading to bacterial proliferation and invasion of the appendiceal wall, which causes venous engorgement and subsequent arterial impairment and ischemia due to elevated intraluminal pressures. • Ultimately, gangrene and perforation ensue. Rupture of primary appendiceal abscesses may result in fistulas. • Acute appendicitis may, at times, serve as the initial symptom of Crohn’s disease. • Infrequently, recurrent acute appendicitis may manifest with complete remission of inflammation and symptoms between episodes.
ETIOLOGY • Proliferation of several gastrointestinal bacteria (E. coli, Peptostreptococcus, B. fragilis, Enterobacteriaceae, viridans streptococcus) transpires within the obstructed appendix. • Chronic appendiceal infection may arise from tuberculosis, amebiasis, and actinomycosis.
DIAGNOSIS HISTORY
The onset of pain transpires across several hours. The earliest visceral abdominal pain of appendicitis is colicky and typically poorly localized in the periumbilical or epigastric area. As inflammation spreads to the parietal peritoneal surfaces, the pain becomes somatic, steady, and more intense. The pain intensifies with movement or coughing and is localized in the right lower quadrant (McBurney's point). • An associated need to defecate or expel flatus frequently occurs, neither of which alleviates the discomfort. Anorexia is prevalent enough that the manifestation of hunger should raise concern for a diagnosis of acute appendicitis. Nausea and vomiting manifest in 50–60% of instances; however, vomiting is seldom severe and prolonged. The occurrence of nausea and vomiting prior to the onset of pain is exceedingly uncommon. • Urinary frequency and dysuria manifest when the appendix is positioned near to the bladder.
PHYSICAL EXAM • Physical results fluctuate over time following the commencement of the illness and are contingent upon the appendix's position. • Tenderness may initially be absent in the early visceral stage of the disease, but it eventually manifests in the area corresponding to the appendix's location. Pregnant women frequently exhibit pain in the right upper quadrant. Guarding is a result of parietal peritoneal involvement. Tenderness upon percussion, rebound tenderness, and referred rebound tenderness are frequently observed. Rebound soreness in the right lower quadrant during probing of the left lower quadrant is referred to as "Rovsing's sign." Pain induced by passive flexion of the right hip is referred to as "the psoas sign"; pain induced by internal rotation of the right hip is referred to as "the obturator sign." • The temperature is often normal or marginally elevated; however, a temperature beyond 38.3°C (101°F) indicates potential perforation. • A discernible mass in the right lower quadrant implies the possibility of an abscess or cecal cancer.
DIAGNOSTIC TESTS AND INTERPRETATION Lab
Leukocytosis ranging from 10,000 to 18,000 cells per milliliter with a left shift is prevalent; however, the lack of leukocytosis does not preclude the diagnosis of acute appendicitis. A pregnancy test must be conducted for all women of childbearing age to exclude the possibility of uterine or ectopic pregnancy. Imaging: Preliminary Strategy Among noninvasive diagnostic tools, appendiceal CT has demonstrated superior precision, achieving an accuracy of 90%. The greatest accuracy has been documented with helical CT following the administration of a 3% diatrizoate meglumine (Gastrografin)–saline solution into the colon. Appendiceal CT is safe, can be conducted in roughly 15 minutes, and necessitates only one-third of the radiation exposure compared to normal CT of the belly and pelvis. Routine appendiceal CT conducted in patients with probable appendicitis enhances patient care and diminishes the utilization of hospital resources. Ultrasound is particularly beneficial for women of childbearing age to rule out ovarian cysts, ectopic pregnancy, or tubo-ovarian abscess. It is also utilized in pediatrics. Normal ultrasonographic findings should not dissuade the surgeon from conducting an appendectomy if the clinical history suggests appendicitis and there is definitive discomfort in the right lower quadrant. Subsequent Actions & Unique Considerations The management strategies for clinicians assessing patients with suspected appendicitis including observation, diagnostic imaging, laparoscopy, and appendectomy. • Patients with a history strongly indicative of appendicitis are frequently sent to the operating room for laparoscopy, irrespective of imaging outcomes. • Patients with a less compelling history are typically subjected to imaging or monitoring. Histopathological Observations Pathology specimens from acute appendicitis exhibit indicators of inflammation, including polymorphonuclear leukocytes, edema, and vascular congestion in the appendiceal walls.
DIFFERENTIAL DIAGNOSIS • The lack of right lower quadrant pain, the absence of typical pain migration, and a history of analogous pain render appendicitis less probable. The absence of right lower quadrant discomfort, rigidity, or guarding during the physical examination diminishes the likelihood of appendicitis. • The differential diagnosis of acute appendicitis encompasses the following: – Acute cholecystitis – Acute diverticulitis – Acute gastroenteritis – Acute pancreatitis – Acute pelvic inflammatory illness – Endometriosis – Mesenteric lymphadenitis – Perforated ulcer – Pyelonephritis – Ruptured Graafian follicle or corpus luteum cyst – Ruptured ectopic pregnancy – Strangulating intestinal blockage – Torted ovarian cyst – Ureteral calculus The differential diagnosis of acute appendicitis is elaborated upon in Section I, chapter "Abdominal Pain and Fever."
THERAPY
The principal intervention for appendicitis is immediate surgical intervention. Antibiotics are the normal preoperative treatment and must be effective against gram-negative aerobes and anaerobes.
MEDICATION • Antibiotic care parallels that of other intra-abdominal infections, as elaborated in Section II chapters, “Peritonitis” and “Intra-abdominal Abscess.” • Options comprise: – Beta-lactam and beta-lactamase inhibitor (ampicillin–sulbactam, piperacillin–tazobactam, ticarcillin–clavulanate) – Ceftriaxone and metronidazole – Fluoroquinolone and metronidazole - Carbapenems (imipenem, meropenem)
SUPPLEMENTARY THERAPY
Referral Considerations Surgical intervention should be integrated into the management of a patient with suspected appendicitis from the moment of initial presentation.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Prompt surgical assessment of a patient with a compelling history and/or imaging indicative of appendicitis is essential. • Both laparoscopic and open techniques are permissible. Patients undergoing laparoscopic surgery experience fewer wound infections, reduced discomfort, and shorter hospital stays compared to those undergoing open surgery. Nonetheless, laparoscopic appendectomies are correlated with an increased incidence of intra-abdominal abscesses, extended operative durations, and elevated surgical expenses. • If a palpable mass is detected 3–5 days post-symptom onset, the procedure should be postponed, since a phlegmon rather than a definite abscess is likely to be present. Patients should get broad-spectrum antibiotics, parenteral fluids, and rest. An appendectomy should be performed safely three months later. If the tumor increases in size or the patient exhibits heightened toxicity, abscess drainage is required.
INPATIENT CONSIDERATIONS
Preliminary Stabilization If unstable, the patient with appendicitis is likely experiencing sepsis or has a perforated appendix with subsequent peritonitis. The patient requires resuscitation with intravenous fluids, and vasopressors should be administered if deemed required. Admission Criteria All patients with suspected appendicitis must be admitted. Intravenous Fluids Patients should be thoroughly hydrated preoperatively, and electrolyte imbalances must be corrected. Criteria for Discharge Discharge criteria encompass the normalization of white blood cell count, the resolution of fever, and the restoration of bowel function.
CONTINUING MANAGEMENT POST-TREATMENT SUGGESTIONS
Close monitoring of patients with stomach pain who do not undergo additional diagnostic testing is warranted.
NUTRITION
Individuals suspected of having appendicitis should refrain from eating.
PROGNOSIS • The mortality rate in Europe and the US has consistently declined to less than 1 per 100,000. The general mortality rate for perforated appendicitis is 3%, escalating to 15% in the elderly population.
COMPLICATIONS
The postponement of appendicitis diagnosis elevates the likelihood of appendiceal perforation, which is linked to postoperative complications in as many as 40% of patients, in contrast to 5–10% for uncomplicated appendicitis. Perforation is uncommon within the first 24 hours of symptom onset, but the incidence increases to 80% after 48 hours. The formation of intra-abdominal abscesses or phlegmon typically occurs subsequent to perforation accompanied by generalized peritonitis and can be prevented with early disease detection. • Wounds must be monitored for indications of infection. • Portal vein thrombophlebitis and pyogenic liver abscess are rare occurrences.
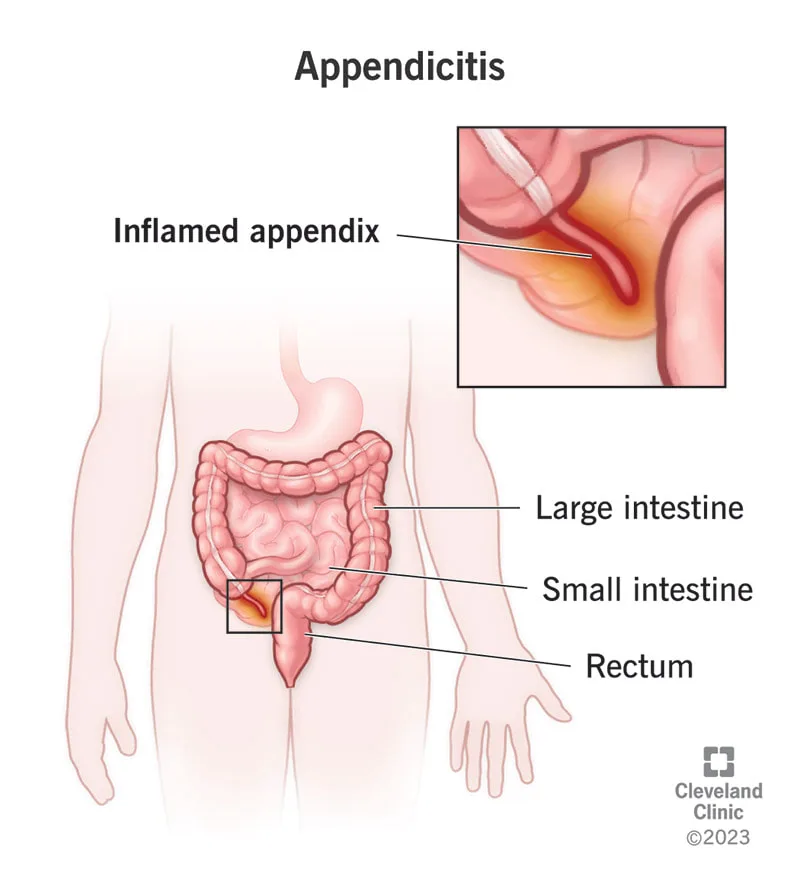
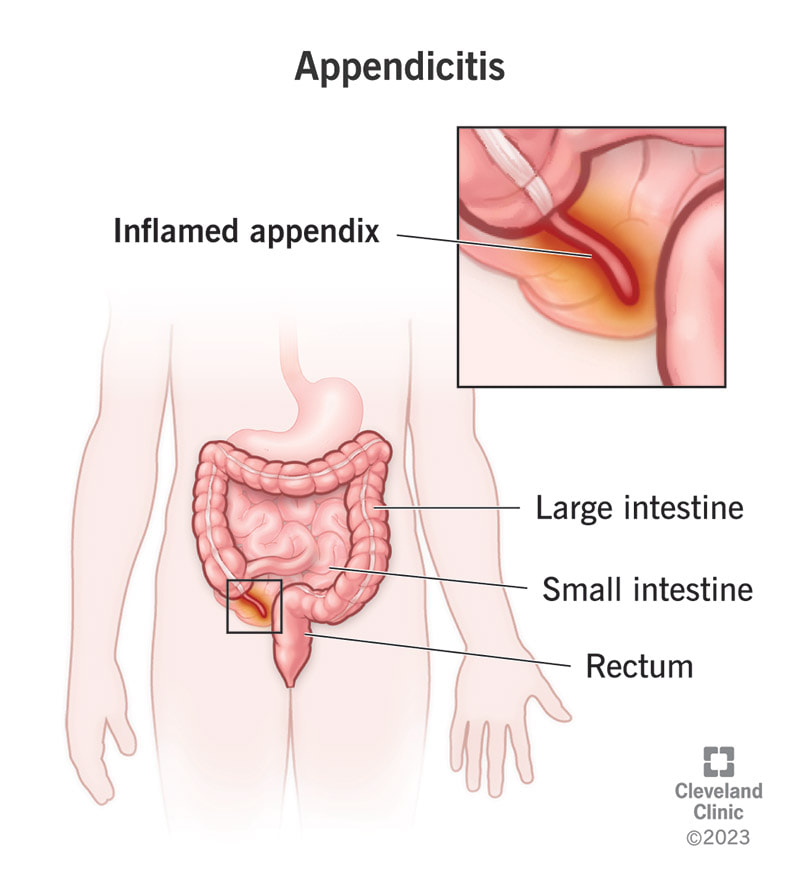
- Published on
Infectious Disease - Aspergillosis
BASICS DESCRIPTION • The term “aspergillosis” encompasses a broad spectrum of conditions, ranging from mere colonization or allergic reactions to localized or widespread invasive diseases. The illness typically targets the lungs, while it can also affect any organ, with the paranasal sinuses and central nervous system (CNS) being less frequently implicated.
EPIDEMIOLOGY
Incidence • The variety of Aspergillus species responsible for invasive illness seems to be increasing. A. fumigatus is the predominant species; however, A. flavus, A. terreus, A. niger, and A. versicolor have also been implicated in aspergillosis. Invasive aspergillosis ranks second in prevalence to candidiasis among invasive mycoses in the majority of immunosuppressed patient populations.
RISK FACTORS
• Granulocytopenia (the most significant predisposing factor) • Hematopoietic cell transplant recipients • Solid-organ transplant recipients • Individuals with acute leukemia • Chronic obstructive pulmonary disease (COPD) patients undergoing steroid therapy • Extended corticosteroid or cytotoxic treatment • Prolonged antibiotic administration • Hepatic failure • Diabetes mellitus • Chronic granulomatous illness in childhood • Acquired immunodeficiency syndrome (AIDS) (CD4 count of 50 cells/mm³ or fewer) Genetics • Polymorphisms in Toll-like receptor 4 may elevate the risk of invasive aspergillosis. • Polymorphisms in Toll-like receptor 9 may influence the risk of allergic bronchopulmonary aspergillosis (ABPA).
GENERAL PREVENTION
• Implementation of environmental control measures, particularly during building operations, to prevent conidia from reaching at-risk patients. • Airflow units equipped with high-efficiency particle air filters. Prophylactic use of voriconazole or amphotericin B may be contemplated for individuals with a history of invasive illness who are at risk of becoming neutropenic.
PATHOPHYSIOLOGY
• ABPA – Aspergillus colonization in atopic individuals activates TH2 CD4+ T cells, resulting in increased IgE expression and eosinophilia. This inflammatory milieu aggravates asthma, resulting in worse symptoms. Airway injury and central bronchiectasis may develop. • Chronic pulmonary aspergillosis, including aspergilloma, typically manifests in patients with the following diseases. – History of tuberculosis – Allergic bronchopulmonary aspergillosis – Lung cancer with surgical excision – Bulla formation • COPD – Lesions exhibit persistent inflammatory alterations, fibrosis, and necrosis. – Invasion is not observed unless the patient enters an immunocompromised state. • Invasive aspergillosis – Conidia are omnipresent and sufficiently diminutive to reach the alveolus upon inhalation. Alveolar macrophages generally phagocytize these infections. – In an immunocompromised state, macrophages are unable to retain the conidia, allowing them to germinate into hyphae. The existence of hyphal forms induces the influx of macrophages and the release of inflammatory cytokines. Vascular invasion and subsequent tissue necrosis may occur. – Circulation via the bloodstream is feasible.
DIAGNOSIS HISTORY
• ABPA – Present in individuals with diagnosed asthma or cystic fibrosis – Possible bronchial obstruction – General malaise – Rare occurrence of hemoptysis • Chronic aspergillosis – Weight loss – Persistent cough – Hemoptysis – Shortness of breath – Dyspnea upon exertion • Invasive aspergillosis – Pleuritic chest pain – Cough – Hemoptysis – Dyspnea
PHYSICAL EXAMINATION
• ABPA – Wheezing may be seen, but is not mandatory. – Fever • Chronic aspergillosis – Abnormal pulmonary auscultation – Fever • Invasive aspergillosis – Fever – Abnormal pulmonary auscultation
DIAGNOSTIC TESTS AND INTERPRETATION
Diagnostic Procedures and Additional Methods • ABPA – Chest X-ray may reveal parenchymal infiltrates, typically affecting the higher lobes. CT scan reveals bronchial wall thickening, bronchiectasis, and ground-glass opacities. – Peripheral eosinophilia – Immediate reaction to skin tests for Aspergillus – Increased total serum IgE – Serum IgG to A. fumigatus • Chronic aspergillosis – Chest X-ray and/or Chest CT reveal one or more cavities – Aspergilloma masses may be observed within the cavity, typically encircled by air- Crescent shadow - Serum IgG to A. fumigatus - Elevated CRP or ESR • Invasive aspergillosis - Positive culture from tissue biopsy is the gold standard - Evidence of fungal invasion in tissue - Positive galactomannan level in serum - Positive β-glucan level in serum
THERAPY PHARMACEUTICALS
First Line • ABPA – A regimen of glucocorticoids and itraconazole is employed. – Steroids may be gradually reduced over a period of 3 to 6 months. – In certain instances, steroids cannot be reduced, necessitating ongoing steroid maintenance. • Chronic aspergillosis – Aspergilloma generally necessitates surgical resection in patients capable of enduring the procedure. Certain individuals derive advantages from antifungal treatment, predominantly voriconazole. Chronic pulmonary aspergillosis necessitates prolonged antifungal treatment. Embolization is employed in patients to mitigate the risk of hemoptysis. • Invasive aspergillosis – Voriconazole is regarded as the primary treatment. Surgical debridement is necessary whenever feasible. Second Line • For invasive aspergillosis, other medicines comprise amphotericin B, itraconazole, and echinocandins. – The efficacy of combination therapy involving the aforementioned antimicrobials remains unverified.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Aggressive debridement should be contemplated for patients with persistent or invasive diseases.
INPATIENT CONSIDERATIONS
Preliminary Stabilization • Antifungal therapy, either intravenous or oral, should be commenced promptly. • Hemodynamic parameters must be stabilized. Admission Criteria: • Patients exhibiting hemodynamic instability • Patients presenting with hemoptysis • Certain patients with fever and immunocompromised conditions
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patients with hypersensitivity lung disorders must be followed for relapses and the onset of pulmonary fibrosis or bronchiectasis. Patients with aspergillomas who do not get surgical intervention require clinical and radiological surveillance for lesion progression and the onset of hemoptysis. Patients who receive surgical intervention for aspergillomas require monitoring for potential return of the infection, despite initial surgical success. Patients with invasive illness require monitoring for relapses, particularly during episodes of neutropenia. Patient Surveillance Monitoring of voriconazole trough levels is essential for individuals undergoing prolonged treatment with the drug.
PROGNOSIS
The prognosis for patients with invasive aspergillosis is contingent upon the fungal load and the extent of immunosuppression.
COMPLICATIONS
The most dreaded consequence of chronic pulmonary aspergillosis is hemoptysis. • Dissemination and mortality are critical consequences in patients with invasive aspergillosis. Bronchiectasis may complicate allergic bronchopulmonary aspergillosis (ABPA). Pulmonary fibrosis may complicate both allergic bronchopulmonary aspergillosis (ABPA) and extrinsic allergic alveolitis. Hemoptysis, which can be substantial, particularly for lesions situated near the hilum, may aggravate both invasive and noninvasive pulmonary aspergillosis. Pneumothorax may arise in immunocompromised individuals and is typically linked to the enhancement of the immune system. The introduction of Aspergilli into the pleural space, resulting from pneumothorax or the formation of a bronchopleural fistula, may result in empyema. In instances of pulmonary and extrapulmonary invasive aspergillosis, persistent dissemination to other organs and lesion enlargement may occur, particularly in immunocompromised persons. Patients with central nervous system involvement may have occlusion of cerebral vessels due to Aspergillus.
BASICS DESCRIPTION • The term “aspergillosis” encompasses a broad spectrum of conditions, ranging from mere colonization or allergic reactions to localized or widespread invasive diseases. The illness typically targets the lungs, while it can also affect any organ, with the paranasal sinuses and central nervous system (CNS) being less frequently implicated.
EPIDEMIOLOGY
Incidence • The variety of Aspergillus species responsible for invasive illness seems to be increasing. A. fumigatus is the predominant species; however, A. flavus, A. terreus, A. niger, and A. versicolor have also been implicated in aspergillosis. Invasive aspergillosis ranks second in prevalence to candidiasis among invasive mycoses in the majority of immunosuppressed patient populations.
RISK FACTORS
• Granulocytopenia (the most significant predisposing factor) • Hematopoietic cell transplant recipients • Solid-organ transplant recipients • Individuals with acute leukemia • Chronic obstructive pulmonary disease (COPD) patients undergoing steroid therapy • Extended corticosteroid or cytotoxic treatment • Prolonged antibiotic administration • Hepatic failure • Diabetes mellitus • Chronic granulomatous illness in childhood • Acquired immunodeficiency syndrome (AIDS) (CD4 count of 50 cells/mm³ or fewer) Genetics • Polymorphisms in Toll-like receptor 4 may elevate the risk of invasive aspergillosis. • Polymorphisms in Toll-like receptor 9 may influence the risk of allergic bronchopulmonary aspergillosis (ABPA).
GENERAL PREVENTION
• Implementation of environmental control measures, particularly during building operations, to prevent conidia from reaching at-risk patients. • Airflow units equipped with high-efficiency particle air filters. Prophylactic use of voriconazole or amphotericin B may be contemplated for individuals with a history of invasive illness who are at risk of becoming neutropenic.
PATHOPHYSIOLOGY
• ABPA – Aspergillus colonization in atopic individuals activates TH2 CD4+ T cells, resulting in increased IgE expression and eosinophilia. This inflammatory milieu aggravates asthma, resulting in worse symptoms. Airway injury and central bronchiectasis may develop. • Chronic pulmonary aspergillosis, including aspergilloma, typically manifests in patients with the following diseases. – History of tuberculosis – Allergic bronchopulmonary aspergillosis – Lung cancer with surgical excision – Bulla formation • COPD – Lesions exhibit persistent inflammatory alterations, fibrosis, and necrosis. – Invasion is not observed unless the patient enters an immunocompromised state. • Invasive aspergillosis – Conidia are omnipresent and sufficiently diminutive to reach the alveolus upon inhalation. Alveolar macrophages generally phagocytize these infections. – In an immunocompromised state, macrophages are unable to retain the conidia, allowing them to germinate into hyphae. The existence of hyphal forms induces the influx of macrophages and the release of inflammatory cytokines. Vascular invasion and subsequent tissue necrosis may occur. – Circulation via the bloodstream is feasible.
DIAGNOSIS HISTORY
• ABPA – Present in individuals with diagnosed asthma or cystic fibrosis – Possible bronchial obstruction – General malaise – Rare occurrence of hemoptysis • Chronic aspergillosis – Weight loss – Persistent cough – Hemoptysis – Shortness of breath – Dyspnea upon exertion • Invasive aspergillosis – Pleuritic chest pain – Cough – Hemoptysis – Dyspnea
PHYSICAL EXAMINATION
• ABPA – Wheezing may be seen, but is not mandatory. – Fever • Chronic aspergillosis – Abnormal pulmonary auscultation – Fever • Invasive aspergillosis – Fever – Abnormal pulmonary auscultation
DIAGNOSTIC TESTS AND INTERPRETATION
Diagnostic Procedures and Additional Methods • ABPA – Chest X-ray may reveal parenchymal infiltrates, typically affecting the higher lobes. CT scan reveals bronchial wall thickening, bronchiectasis, and ground-glass opacities. – Peripheral eosinophilia – Immediate reaction to skin tests for Aspergillus – Increased total serum IgE – Serum IgG to A. fumigatus • Chronic aspergillosis – Chest X-ray and/or Chest CT reveal one or more cavities – Aspergilloma masses may be observed within the cavity, typically encircled by air- Crescent shadow - Serum IgG to A. fumigatus - Elevated CRP or ESR • Invasive aspergillosis - Positive culture from tissue biopsy is the gold standard - Evidence of fungal invasion in tissue - Positive galactomannan level in serum - Positive β-glucan level in serum
THERAPY PHARMACEUTICALS
First Line • ABPA – A regimen of glucocorticoids and itraconazole is employed. – Steroids may be gradually reduced over a period of 3 to 6 months. – In certain instances, steroids cannot be reduced, necessitating ongoing steroid maintenance. • Chronic aspergillosis – Aspergilloma generally necessitates surgical resection in patients capable of enduring the procedure. Certain individuals derive advantages from antifungal treatment, predominantly voriconazole. Chronic pulmonary aspergillosis necessitates prolonged antifungal treatment. Embolization is employed in patients to mitigate the risk of hemoptysis. • Invasive aspergillosis – Voriconazole is regarded as the primary treatment. Surgical debridement is necessary whenever feasible. Second Line • For invasive aspergillosis, other medicines comprise amphotericin B, itraconazole, and echinocandins. – The efficacy of combination therapy involving the aforementioned antimicrobials remains unverified.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Aggressive debridement should be contemplated for patients with persistent or invasive diseases.
INPATIENT CONSIDERATIONS
Preliminary Stabilization • Antifungal therapy, either intravenous or oral, should be commenced promptly. • Hemodynamic parameters must be stabilized. Admission Criteria: • Patients exhibiting hemodynamic instability • Patients presenting with hemoptysis • Certain patients with fever and immunocompromised conditions
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patients with hypersensitivity lung disorders must be followed for relapses and the onset of pulmonary fibrosis or bronchiectasis. Patients with aspergillomas who do not get surgical intervention require clinical and radiological surveillance for lesion progression and the onset of hemoptysis. Patients who receive surgical intervention for aspergillomas require monitoring for potential return of the infection, despite initial surgical success. Patients with invasive illness require monitoring for relapses, particularly during episodes of neutropenia. Patient Surveillance Monitoring of voriconazole trough levels is essential for individuals undergoing prolonged treatment with the drug.
PROGNOSIS
The prognosis for patients with invasive aspergillosis is contingent upon the fungal load and the extent of immunosuppression.
COMPLICATIONS
The most dreaded consequence of chronic pulmonary aspergillosis is hemoptysis. • Dissemination and mortality are critical consequences in patients with invasive aspergillosis. Bronchiectasis may complicate allergic bronchopulmonary aspergillosis (ABPA). Pulmonary fibrosis may complicate both allergic bronchopulmonary aspergillosis (ABPA) and extrinsic allergic alveolitis. Hemoptysis, which can be substantial, particularly for lesions situated near the hilum, may aggravate both invasive and noninvasive pulmonary aspergillosis. Pneumothorax may arise in immunocompromised individuals and is typically linked to the enhancement of the immune system. The introduction of Aspergilli into the pleural space, resulting from pneumothorax or the formation of a bronchopleural fistula, may result in empyema. In instances of pulmonary and extrapulmonary invasive aspergillosis, persistent dissemination to other organs and lesion enlargement may occur, particularly in immunocompromised persons. Patients with central nervous system involvement may have occlusion of cerebral vessels due to Aspergillus.
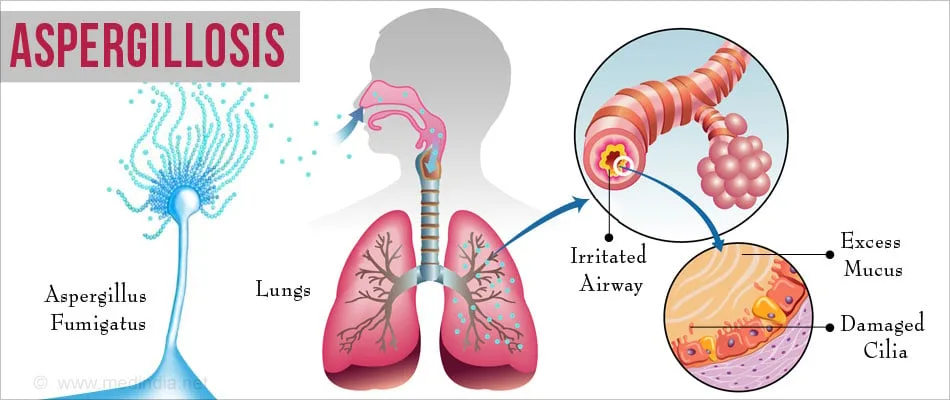
- Published on
Symptoms and Signs – Differential Diagnosis of McMurray’s Sign
Among older patients, McBurney's sign, along with other peritoneal signs, may be reduced or nonexistent.
Typically a symptom of damage to the medial meniscus, McMurray's sign is a detectable, audible click or pop produced by moving the tibia on the femur. This occurs when delicate manipulation of the leg traps causes the cartilage to tear and then break loose. Because evoking this symptom compels the tibial plateau surface to come into contact with the femoral condyles, manipulating these structures is not recommended for individuals who are suspected to have fractures of the tibial plateau or femoral condyles.
A positive McMurray's sign enhances additional symptoms often described with meniscal damage, such as intense discomfort, locking, or clicking of the joint line.
The joint has reduced range of motion (ROM).
Background and Physical Assessment
Upon obtaining McMurray's sign, determine whether the patient is now suffering from acute knee discomfort. Next, request his account of a recent knee injury. For instance, did his injury result in a twisting external or internal force on the knee, or did he get blunt knee injuries related to a fall? In addition, inquire about any prior knee injuries, surgical procedures, prosthetic replacements, or other joint conditions, such arthritis, that may have compromised the knee. Seek clarification on any factors that worsen or alleviate the discomfort and whether he need aid in ambulation.
Prompt the patient to indicate the precise location of the pain. Evaluate the range of motion (ROM) of the leg, both passively and with resistance. Subsequently, assess the stability of the cruciate ligament by seeing any vertical displacement of the tibia on the femur (drawer sign). Ultimately, assess the quadriceps muscles in both legs to determine their symmetry.
Guidelines for Examination
Invoking McMurray's Sign The elicitation of McMurray's sign necessitates specialized training and delicate manipulation of the patient's leg to prevent the extension of a meniscal tear or the locking of the knee. Having received training to elicit McMurray's sign, arrange the patient in a supine posture and flex the knee in question until the heel comes close to making contact with the buttock. Position both your thumb and index finger on opposite sides of the knee joint space, and firmly hold onto his heel with your other hand. Proceed to laterally rotate the foot and lower leg in order to assess the posterior portion of the medial meniscus.
The anterior aspect of the medial meniscus can be tested by extending the knee to a 90-degree angle while keeping the patient's foot in a lateral posture. An audible or perceptible click, known as a positive McMurray's sign, suggests damage to the meniscal structures.
Medical Causes
McMurray's sign is often elicited in cases of meniscal tear damage. The associated signs and symptoms consist of sudden knee discomfort at either the medial or lateral joint line (depending on the location of the injury) and reduced range of motion or locking of the knee joint. Muscle weakness and atrophy of the quadriceps may also manifest.
Key Factors to Consider
The patient should be prepared for knee X-rays, arthroscopy, and arthrography, and any prior X-rays should be obtained for direct comparison. Should the knee discomfort and McMurray's sign be triggered by trauma, it is possible that an effusion or hemarthrosis may develop. Arrange the patient for joint aspiration. Stabilize and administer cold compresses to the knee, and then put a cast or
A knee immobilizing device.
Therapeutic Counseling for Patients
Justify the need of raising the afflicted leg, the correct utilization of any necessary assistive equipment, and the correct administration of analgesics and anti-inflammatory medications. Provide instruction on knee exercises and address any necessary lifestyle modifications for the patient.
Guidelines for Pediatric Populations
The manifestation of McMurray's sign in adolescents is often observed in cases of meniscal tear resulting from a sports-related injury. The phenomenon may also be evoked in children diagnosed with congenital discoid meniscus.
Among older patients, McBurney's sign, along with other peritoneal signs, may be reduced or nonexistent.
Typically a symptom of damage to the medial meniscus, McMurray's sign is a detectable, audible click or pop produced by moving the tibia on the femur. This occurs when delicate manipulation of the leg traps causes the cartilage to tear and then break loose. Because evoking this symptom compels the tibial plateau surface to come into contact with the femoral condyles, manipulating these structures is not recommended for individuals who are suspected to have fractures of the tibial plateau or femoral condyles.
A positive McMurray's sign enhances additional symptoms often described with meniscal damage, such as intense discomfort, locking, or clicking of the joint line.
The joint has reduced range of motion (ROM).
Background and Physical Assessment
Upon obtaining McMurray's sign, determine whether the patient is now suffering from acute knee discomfort. Next, request his account of a recent knee injury. For instance, did his injury result in a twisting external or internal force on the knee, or did he get blunt knee injuries related to a fall? In addition, inquire about any prior knee injuries, surgical procedures, prosthetic replacements, or other joint conditions, such arthritis, that may have compromised the knee. Seek clarification on any factors that worsen or alleviate the discomfort and whether he need aid in ambulation.
Prompt the patient to indicate the precise location of the pain. Evaluate the range of motion (ROM) of the leg, both passively and with resistance. Subsequently, assess the stability of the cruciate ligament by seeing any vertical displacement of the tibia on the femur (drawer sign). Ultimately, assess the quadriceps muscles in both legs to determine their symmetry.
Guidelines for Examination
Invoking McMurray's Sign The elicitation of McMurray's sign necessitates specialized training and delicate manipulation of the patient's leg to prevent the extension of a meniscal tear or the locking of the knee. Having received training to elicit McMurray's sign, arrange the patient in a supine posture and flex the knee in question until the heel comes close to making contact with the buttock. Position both your thumb and index finger on opposite sides of the knee joint space, and firmly hold onto his heel with your other hand. Proceed to laterally rotate the foot and lower leg in order to assess the posterior portion of the medial meniscus.
The anterior aspect of the medial meniscus can be tested by extending the knee to a 90-degree angle while keeping the patient's foot in a lateral posture. An audible or perceptible click, known as a positive McMurray's sign, suggests damage to the meniscal structures.
Medical Causes
McMurray's sign is often elicited in cases of meniscal tear damage. The associated signs and symptoms consist of sudden knee discomfort at either the medial or lateral joint line (depending on the location of the injury) and reduced range of motion or locking of the knee joint. Muscle weakness and atrophy of the quadriceps may also manifest.
Key Factors to Consider
The patient should be prepared for knee X-rays, arthroscopy, and arthrography, and any prior X-rays should be obtained for direct comparison. Should the knee discomfort and McMurray's sign be triggered by trauma, it is possible that an effusion or hemarthrosis may develop. Arrange the patient for joint aspiration. Stabilize and administer cold compresses to the knee, and then put a cast or
A knee immobilizing device.
Therapeutic Counseling for Patients
Justify the need of raising the afflicted leg, the correct utilization of any necessary assistive equipment, and the correct administration of analgesics and anti-inflammatory medications. Provide instruction on knee exercises and address any necessary lifestyle modifications for the patient.
Guidelines for Pediatric Populations
The manifestation of McMurray's sign in adolescents is often observed in cases of meniscal tear resulting from a sports-related injury. The phenomenon may also be evoked in children diagnosed with congenital discoid meniscus.
