- Published on
Branchial Cyst, Sinus and Fistula
Introduction
swelling or discharge in the neck resulting from pharyngeal pouches and clefts not fully obliterated during embryonic development.
Etiology
Ninety-five percent originate from congenital remnants of the branchial cleft or second pharyngeal pouch, while it's unclear exactly where they originated embryologically (perhaps ectopic tissue or incomplete involution).
Epidemiology
Not common. The most prevalent are branchial cysts, which typically manifest in the third decade and can vary greatly. In children, fistulae and sinuses are typically present.
History
The patient reports having a lateral neck swelling that fluctuates in size over time. Until inflammation and infection occur, the swelling is normally painless but eventually turns red and unpleasant. Mucus or mucopurulent fluid may leak from a neck dimple that is indicative of a sinus or fistula.
Examination
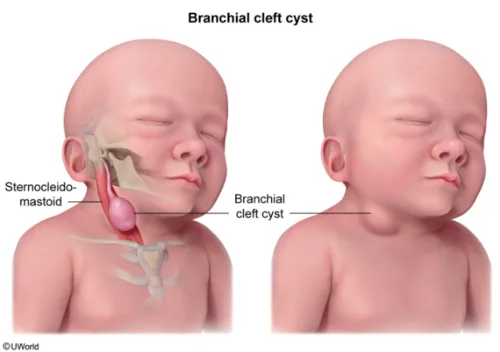
A lump is located at the intersection of the sternocleidomastoid's top and lower two-thirds, if this is indeed a cyst.
Upon palpation, the swelling is often oval-shaped, hard, and smooth. It can also fluctuate and transilluminate, as well as be somewhat soft in the early stages. There are 2% bilateral cases.
The intersection of the middle and lower thirds of the anterior margin of the sternocleidomastoid represents the external opening of a branchial sinus or fistula.
Pathogenesis
During the fifth week of fetal development, branchial clefts—neck grooves with branchial arches between—appear. The external auditory meatus, the first cleft, remains, while the other clefts usually vanish. Should the second cleft's remnants persist, a cyst, sinus, or fistula might form. Squamous or respiratory epithelium lines the cysts, which are filled with turbid fluid made up of cholesterol crystals and epithelial detritus, with lymphoid tissue present in some cases.
Between the internal and external carotid arteries, a branchial fistula terminates in the posterior portion of the tonsillar fossa in the oropharynx, superior to the hypoglossal nerve and inferior to the glossopharyngeal nerve.
Investigations
Imaging: To see the cyst, employ CT, MRI, or ultrasound scanning.
FNA: Used to differentiate cervical lymph node metastases in elderly patients from other types of cancer (such as thyroid cancer and mucoepidermoid carcinomas of the salivary glands, which may contain a significant cystic component).
Management
Surgery: The cyst and any related sinuses or tracts are surgically removed as part of the treatment. Usually, a transverse neck incision is used for this. To gain access to the cyst, the sternomastoid is retracted posteriorly and the platysma is separated. Subsequently, it is extracted with meticulous dissection, identification, and caution to prevent harm to any nerves, particularly the vagus, hypoglossal, and spinal accessory nerves. Before the cyst is removed, a branchial cyst abscess needs to be drained and antibiotics administered to prevent infection.
Complications
Incomplete excision of a sinus or fistula tract, infection, branchial cyst abscess, nerve injury during surgery.
Prognosis
Good, with full excision leading to a cure. Rates of recurrence are higher in cases of prior infection.
Introduction
swelling or discharge in the neck resulting from pharyngeal pouches and clefts not fully obliterated during embryonic development.
Etiology
Ninety-five percent originate from congenital remnants of the branchial cleft or second pharyngeal pouch, while it's unclear exactly where they originated embryologically (perhaps ectopic tissue or incomplete involution).
Epidemiology
Not common. The most prevalent are branchial cysts, which typically manifest in the third decade and can vary greatly. In children, fistulae and sinuses are typically present.
History
The patient reports having a lateral neck swelling that fluctuates in size over time. Until inflammation and infection occur, the swelling is normally painless but eventually turns red and unpleasant. Mucus or mucopurulent fluid may leak from a neck dimple that is indicative of a sinus or fistula.
Examination
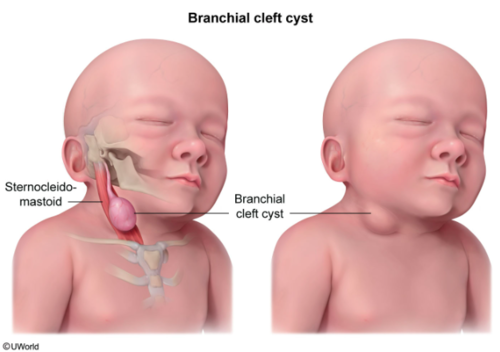
A lump is located at the intersection of the sternocleidomastoid's top and lower two-thirds, if this is indeed a cyst.
Upon palpation, the swelling is often oval-shaped, hard, and smooth. It can also fluctuate and transilluminate, as well as be somewhat soft in the early stages. There are 2% bilateral cases.
The intersection of the middle and lower thirds of the anterior margin of the sternocleidomastoid represents the external opening of a branchial sinus or fistula.
Pathogenesis
During the fifth week of fetal development, branchial clefts—neck grooves with branchial arches between—appear. The external auditory meatus, the first cleft, remains, while the other clefts usually vanish. Should the second cleft's remnants persist, a cyst, sinus, or fistula might form. Squamous or respiratory epithelium lines the cysts, which are filled with turbid fluid made up of cholesterol crystals and epithelial detritus, with lymphoid tissue present in some cases.
Between the internal and external carotid arteries, a branchial fistula terminates in the posterior portion of the tonsillar fossa in the oropharynx, superior to the hypoglossal nerve and inferior to the glossopharyngeal nerve.
Investigations
Imaging: To see the cyst, employ CT, MRI, or ultrasound scanning.
FNA: Used to differentiate cervical lymph node metastases in elderly patients from other types of cancer (such as thyroid cancer and mucoepidermoid carcinomas of the salivary glands, which may contain a significant cystic component).
Management
Surgery: The cyst and any related sinuses or tracts are surgically removed as part of the treatment. Usually, a transverse neck incision is used for this. To gain access to the cyst, the sternomastoid is retracted posteriorly and the platysma is separated. Subsequently, it is extracted with meticulous dissection, identification, and caution to prevent harm to any nerves, particularly the vagus, hypoglossal, and spinal accessory nerves. Before the cyst is removed, a branchial cyst abscess needs to be drained and antibiotics administered to prevent infection.
Complications
Incomplete excision of a sinus or fistula tract, infection, branchial cyst abscess, nerve injury during surgery.
Prognosis
Good, with full excision leading to a cure. Rates of recurrence are higher in cases of prior infection.
0 Comments
