- Published on
Clinical Procedures - Colonoscopy
Indications
• Diagnostic: gastrointestinal bleeding, iron-deficiency anemia, chronic diarrhoea, lower abdominal symptoms (chronic constipation, lower abdominal pain, bloating), evaluation of known inflammatory bowel disease (IBD), surveillance for cancer (in IBD patients/after colonic polypectomy/ after curative intent resection of colorectal cancer), screening for colorectal
cancer
• Therapeutic: polypectomy (including endoscopic mucosal resection techniques: EMR), angiodysplasia treated with argon plasma coagulation
(APC), decompression of volvulus or pseudo-obstruction, dilatation, or stenting of strictures or malignant colonic obstruction.
Contraindications
• Absolute: lack of informed consent, toxic megacolon, fulminant colitis, colonic perforation
•Relative: acute diverticulitis, symptomatic large abdominal aortic aneurysm, immediately post-op, recent MI or PE, severe coagulopathies:
• Colonoscopy can be performed safely in pregnancy but should be
deferred in most instances unless requiring immediate resolution.
Procedure
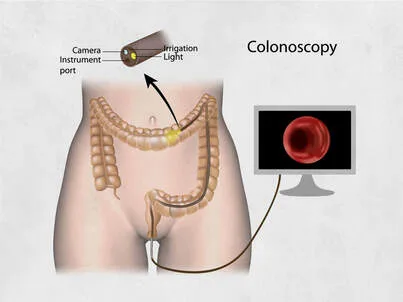
Colonoscopy is an endoscopic examination of the mucosal surface from the anal canal to the terminal ileum.
• Patient lies on the couch in the left lateral position with knees bent
• Endoscopist first performs a digital rectal examination
• Sedation (e.g. midazolam) may be given with monitoring of oxygen saturation. IV analgesia (e.g. pethidine) is also given:
• Increasing use of either no sedation (with improved techniques such as 'Scopeguide®') or inhaled nitric oxide
• Lubricated colonoscope (about 12mm wide and 185cm long) is passed rectally. Air is insufflated. Water-jet may also be used via the scope
• Aim is to pass to the terminal ileum
• Duration varies but averages at about 20 minutes.
Risks
• Perforation (0.2-0.4% diagnostic; higher with therapeutic procedures)
• Bleeding (1 in 1000)
• Abdominal distension, medication effects (allergic reactions, nausea vomiting hypotension, respiratory depression)
• Rarities: infection, postpolypectomy coagulation syndrome: (pain, peritoneal irritation, leucocytosis and fever), splenic rupture, small bowel obstruction.
Patient Preparation
• Iron and constipating agents: discontinue iron tablets 7 days and constipating agents 4 days prior to the procedure
• Anticoagulant and antiplatelet therapy: in the case of a planned polypectomy or other therapeutic procedure, refer to BS guidelines on the management of anticoagulant and antiplatelet therapy (www.bsg.
org.uk)
• Antibiotic prophylaxis: none for colonoscopy. See other topics for comparison
• Bowel preparation: the colon must be empty. Protocols vary but usually include prescribing 1 sachet of sodium picosulfate (Picolax®) for the morning and afternoon of the day before procedure.
Other Information
• The introduction of the bowel cancer screening programme has meant that endoscopists need to pass a 'driving test' to demonstrate high-level competency to perform safe screening colonoscopy
•EMR is used for larger or difficult flat polyps. The lesion is lifted by submucosal injection of gelofusin, adrenaline, and dye followed by snare resection. Polyps can then be retrieved by 'Roth' baskets for histological assessment.
Indications
• Diagnostic: gastrointestinal bleeding, iron-deficiency anemia, chronic diarrhoea, lower abdominal symptoms (chronic constipation, lower abdominal pain, bloating), evaluation of known inflammatory bowel disease (IBD), surveillance for cancer (in IBD patients/after colonic polypectomy/ after curative intent resection of colorectal cancer), screening for colorectal
cancer
• Therapeutic: polypectomy (including endoscopic mucosal resection techniques: EMR), angiodysplasia treated with argon plasma coagulation
(APC), decompression of volvulus or pseudo-obstruction, dilatation, or stenting of strictures or malignant colonic obstruction.
Contraindications
• Absolute: lack of informed consent, toxic megacolon, fulminant colitis, colonic perforation
•Relative: acute diverticulitis, symptomatic large abdominal aortic aneurysm, immediately post-op, recent MI or PE, severe coagulopathies:
• Colonoscopy can be performed safely in pregnancy but should be
deferred in most instances unless requiring immediate resolution.
Procedure
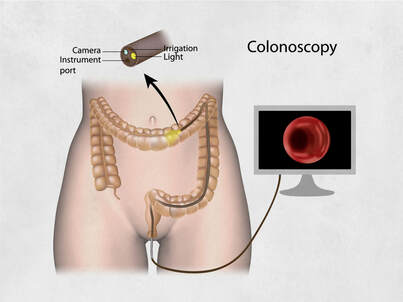
Colonoscopy is an endoscopic examination of the mucosal surface from the anal canal to the terminal ileum.
• Patient lies on the couch in the left lateral position with knees bent
• Endoscopist first performs a digital rectal examination
• Sedation (e.g. midazolam) may be given with monitoring of oxygen saturation. IV analgesia (e.g. pethidine) is also given:
• Increasing use of either no sedation (with improved techniques such as 'Scopeguide®') or inhaled nitric oxide
• Lubricated colonoscope (about 12mm wide and 185cm long) is passed rectally. Air is insufflated. Water-jet may also be used via the scope
• Aim is to pass to the terminal ileum
• Duration varies but averages at about 20 minutes.
Risks
• Perforation (0.2-0.4% diagnostic; higher with therapeutic procedures)
• Bleeding (1 in 1000)
• Abdominal distension, medication effects (allergic reactions, nausea vomiting hypotension, respiratory depression)
• Rarities: infection, postpolypectomy coagulation syndrome: (pain, peritoneal irritation, leucocytosis and fever), splenic rupture, small bowel obstruction.
Patient Preparation
• Iron and constipating agents: discontinue iron tablets 7 days and constipating agents 4 days prior to the procedure
• Anticoagulant and antiplatelet therapy: in the case of a planned polypectomy or other therapeutic procedure, refer to BS guidelines on the management of anticoagulant and antiplatelet therapy (www.bsg.
org.uk)
• Antibiotic prophylaxis: none for colonoscopy. See other topics for comparison
• Bowel preparation: the colon must be empty. Protocols vary but usually include prescribing 1 sachet of sodium picosulfate (Picolax®) for the morning and afternoon of the day before procedure.
Other Information
• The introduction of the bowel cancer screening programme has meant that endoscopists need to pass a 'driving test' to demonstrate high-level competency to perform safe screening colonoscopy
•EMR is used for larger or difficult flat polyps. The lesion is lifted by submucosal injection of gelofusin, adrenaline, and dye followed by snare resection. Polyps can then be retrieved by 'Roth' baskets for histological assessment.
0 Comments
