- Published on
Clinical Procedures - Coronary Angiography/Angioplasty
Indications
• Diagnostic: unstable or refractory angina, acute coronary syndrome, positive or inconclusive stress testing
• Emergency therapeutic: where possible, patients presenting with acute ST-elevation myocardial infarction should have primary coronary intervention rather than thrombolysis
• Elective therapeutic: suitable 'target lesion' identified on diagnostic coronary angiogram.
Contraindications
• Absolute: refusal of patient consent
• Relative: acute renal failure, pulmonary edema, known radiographic contrast allergy, uncontrolled hypertension, active gastrointestinal haemorrhage, acute stroke, and untreated coagulopathy.
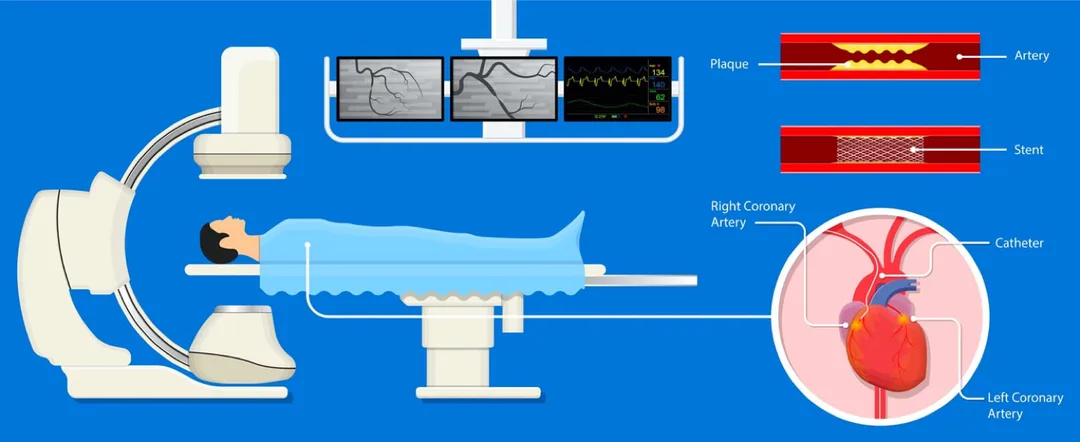
Procedure
• Percutaneous access via a guide needle into a peripheral artery (most commonly the radial artery)
• Guide catheter is introduced, the tip is placed at the coronary ostium, radio-opaque contrast is injected, and real-time x-ray is used to visualize the blood flow through the coronary
• The coronary guidewire is inserted through the catheter into the coronary artery using x-ray guidance
• The guidewire tip is passed across the site of stenosis
• The balloon catheter is passed over the guidewire until the deflated balloon lies across the target lesion
• The balloon is then inflated and compresses the plaque and stretches the artery wall. A stent (wire mesh tube) can be inserted using a similar technique and be left in place maintaining the arterial lumen
• The guidewire, catheter, and sheath are carefully removed
• The patient should remain supine for 4 hours following the procedure unless an arterial closure device has been used.
Risks
• Minor: contrast allergy, vasovagal reaction, hemorrhage and hematoma at puncture site, thrombosis formation, false aneurysm, AV fistulation, pulmonary edema, and renal failure due to contrast nephropathy
• Major: limb ischaemia, coronary artery dissection, aortic dissection, ventricular perforation, air or atheroma embolism, ventricular arrhythmias failure of procedure, and need to proceed to coronary artery bypass graft
• Death (<1 in 1000).
Patient Preparation
• Pre-procedure check list: written consent, group and save, ECG, check full blood count/clotting/U&Es.
Other Information for Junior Doctors
• Coronary angioplasty is associated with increased thrombus formation (balloon inflation disrupts the intima, revealing prothrombotic cores of plaques), therefore antiplatelet therapy is necessary
• Patients will need to have long-term antiplatelet therapy; usually lifelong aspirin 75mg once daily, but they will also need clopidogrel 75mg once daily (see local guidelines: usually 3 months for bare metal stents and 12 months for drug-eluting stents or angioplasty after acute coronary syndrome)
• Patients with renal failure should be carefully considered. lodinated contrast can be nephrotoxic and renal decompensation may occur following coronary angiography/plasty. The risk can be minimized by hydration before and after the procedure. Renal function should be carefully monitored. Check local guidelines.
Indications
• Diagnostic: unstable or refractory angina, acute coronary syndrome, positive or inconclusive stress testing
• Emergency therapeutic: where possible, patients presenting with acute ST-elevation myocardial infarction should have primary coronary intervention rather than thrombolysis
• Elective therapeutic: suitable 'target lesion' identified on diagnostic coronary angiogram.
Contraindications
• Absolute: refusal of patient consent
• Relative: acute renal failure, pulmonary edema, known radiographic contrast allergy, uncontrolled hypertension, active gastrointestinal haemorrhage, acute stroke, and untreated coagulopathy.
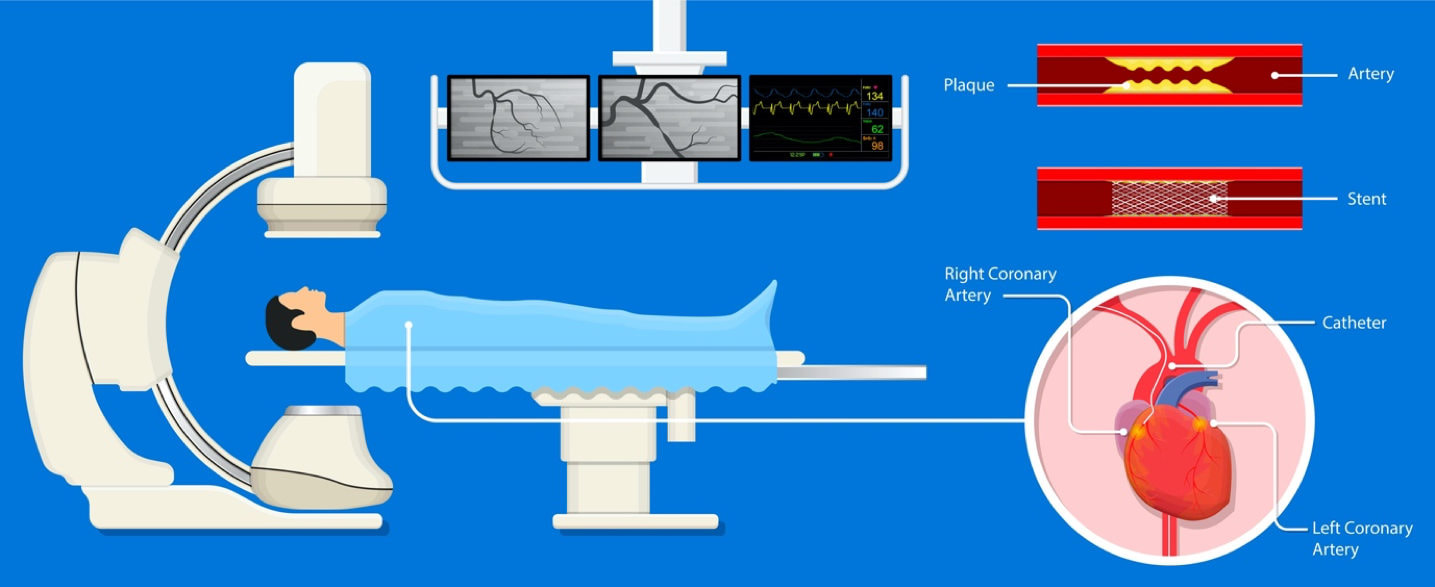
Procedure
• Percutaneous access via a guide needle into a peripheral artery (most commonly the radial artery)
• Guide catheter is introduced, the tip is placed at the coronary ostium, radio-opaque contrast is injected, and real-time x-ray is used to visualize the blood flow through the coronary
• The coronary guidewire is inserted through the catheter into the coronary artery using x-ray guidance
• The guidewire tip is passed across the site of stenosis
• The balloon catheter is passed over the guidewire until the deflated balloon lies across the target lesion
• The balloon is then inflated and compresses the plaque and stretches the artery wall. A stent (wire mesh tube) can be inserted using a similar technique and be left in place maintaining the arterial lumen
• The guidewire, catheter, and sheath are carefully removed
• The patient should remain supine for 4 hours following the procedure unless an arterial closure device has been used.
Risks
• Minor: contrast allergy, vasovagal reaction, hemorrhage and hematoma at puncture site, thrombosis formation, false aneurysm, AV fistulation, pulmonary edema, and renal failure due to contrast nephropathy
• Major: limb ischaemia, coronary artery dissection, aortic dissection, ventricular perforation, air or atheroma embolism, ventricular arrhythmias failure of procedure, and need to proceed to coronary artery bypass graft
• Death (<1 in 1000).
Patient Preparation
• Pre-procedure check list: written consent, group and save, ECG, check full blood count/clotting/U&Es.
Other Information for Junior Doctors
• Coronary angioplasty is associated with increased thrombus formation (balloon inflation disrupts the intima, revealing prothrombotic cores of plaques), therefore antiplatelet therapy is necessary
• Patients will need to have long-term antiplatelet therapy; usually lifelong aspirin 75mg once daily, but they will also need clopidogrel 75mg once daily (see local guidelines: usually 3 months for bare metal stents and 12 months for drug-eluting stents or angioplasty after acute coronary syndrome)
• Patients with renal failure should be carefully considered. lodinated contrast can be nephrotoxic and renal decompensation may occur following coronary angiography/plasty. The risk can be minimized by hydration before and after the procedure. Renal function should be carefully monitored. Check local guidelines.
0 Comments
