- Published on
Clinical Procedures – Defibrillation
Indications
• Elective cardioversion of atrial fibrillation
• Emergency cardioversion in a peri-arrest situation where a tachyarrhythmia is associated with adverse signs
• (See tachyarrhythmia algorithm by Resuscitation Council UK).
Equipment
The 'crash trolley' should contain all the equipment required:
• Gloves, aprons
• Defibrillator, pads, leads, ECG electrodes
• Oxygen, reservoir bag and mask with tubing, airways
• Intubation equipment
• IV fluids, giving sets, selection of syringes, needles, IV cannulas and fixation dressings
• Access to emergency drugs (e.g. atropine, adrenaline, amiodarone, magnesium sulphate).
Before You Start
The procedure is essentially the same whether it is performed electively or as an emergency. However, consider:
Elective procedure
• Obtain informed consent and save a copy of signed form
• Ensure patient fasted >6 hours
• Check serum potassium (>4.0mmol/L is associated with greater success)
• Confirm patient has been successfully anticoagulated for previous 4 weeks (INR >2):
• Warfarin is continued for 3 months post-procedure if successful
• The procedure should be performed in an anaesthetic room, following short-acting induction by an anaesthetist.
Emergency procedure
• Ensure a senior doctor is involved in the decision
• Ensure all other options have been tried or considered
• If possible, discuss with the patient or next of kin.
Procedure
• Ensure skin is dry, free of excess hair, jewellery is removed
• Attach the ECG electrodes; red under right clavicle, yellow under left clavicle, green at the umbilicus
• Switch on defibrillator
• Confirm the ECG rhythm
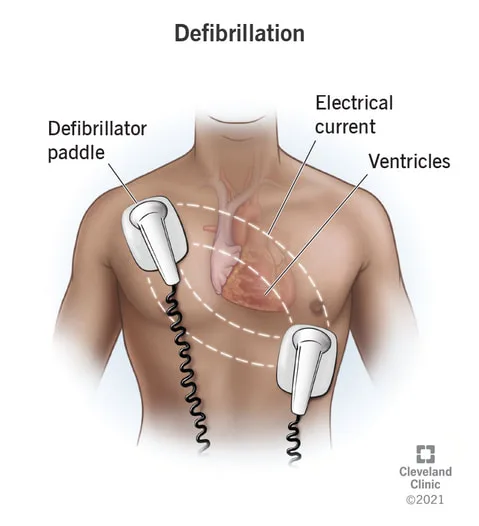
• Place the defibrillator gel pads on the patient's chest; one under the right clavicle and the other inferolateral to the cardiac ape
• Select the 'synchronous mode' on the defibrillator
• D Select the joules (J) required (see below)
• Place the paddles firmly on the chest on the gel pads
• Press the charge button on the paddles to charge the defibrillator and shout 'Stand clear! Charging!'
• Check all persons are standing well clear of the patient and bed (including yourself and that no one is touching the patient or bed (including yourself)
• Ensure the oxygen has been disconnected and removed
• I Check the monitor again to ensure a shockable rhythm
• Shout 'Stand clear! Shocking!'
• Press both discharge buttons on the paddles simultaneously to discharge the shock
• Return the paddles to the defibrillator or keep them on the chest if another shock is required.
Energy Selection
DC Cardioversion usually uses biphasic energies. A reasonable general guide is:
• 50] synchronized shock. If fails..
• 100] synchronized shock. If fails...
• 150] synchronized shock. If fails..
• 150J synchronized anteroposterior shock. If fails...
• Abandon procedure if elective, consult seniors if emergency (may need ICU input).
Contraindications
• Elective: patients unsuitable for general anesthetic, not anticoagulated or who have not signed a consent form
• Emergency: only performed when a tachyarrhythmia is associated with adverse events in the presence of a pulse (pulseless rhythms require management as per the resuscitation guidelines).
Risks
• General anaesthetic risk, if performed electively
• Embolic phenomenon, stroke, myocardial infarction.
Documentation
General
• Date, time and place. Name and grade of persons present
• ECG rhythm
• IV access secured
• Number, volume, dose of any drugs used, and any response noted
• Type of defibrillator machine used
• Method of sedation/anaesthetic
• Asynchronous or synchronous mode. Specify joules of each shock
• Confirm rhythm at end and 12-lead ECG findings
• Sign and bleep/contact details.
Elective
• Indication for DC cardioversion
• Informed consent obtained (retain copy of signed form)
• State time fasted from
• Document anticoagulation type and duration
• Serum potassium level
• Any drug allergies
• Name and grade of anaesthetist
• Type of anaesthetic used.
Emergency
• Events leading up to the peri-arrest situation
• HR, BP, Glasgow coma score on arrival and any deterioration
• Time of decision to shock, name and grade of decision-maker
• Verbal consent obtained?
• Type of sedation used
• Next of kin have been informed or if they are present or on route?
Indications
• Elective cardioversion of atrial fibrillation
• Emergency cardioversion in a peri-arrest situation where a tachyarrhythmia is associated with adverse signs
• (See tachyarrhythmia algorithm by Resuscitation Council UK).
Equipment
The 'crash trolley' should contain all the equipment required:
• Gloves, aprons
• Defibrillator, pads, leads, ECG electrodes
• Oxygen, reservoir bag and mask with tubing, airways
• Intubation equipment
• IV fluids, giving sets, selection of syringes, needles, IV cannulas and fixation dressings
• Access to emergency drugs (e.g. atropine, adrenaline, amiodarone, magnesium sulphate).
Before You Start
The procedure is essentially the same whether it is performed electively or as an emergency. However, consider:
Elective procedure
• Obtain informed consent and save a copy of signed form
• Ensure patient fasted >6 hours
• Check serum potassium (>4.0mmol/L is associated with greater success)
• Confirm patient has been successfully anticoagulated for previous 4 weeks (INR >2):
• Warfarin is continued for 3 months post-procedure if successful
• The procedure should be performed in an anaesthetic room, following short-acting induction by an anaesthetist.
Emergency procedure
• Ensure a senior doctor is involved in the decision
• Ensure all other options have been tried or considered
• If possible, discuss with the patient or next of kin.
Procedure
• Ensure skin is dry, free of excess hair, jewellery is removed
• Attach the ECG electrodes; red under right clavicle, yellow under left clavicle, green at the umbilicus
• Switch on defibrillator
• Confirm the ECG rhythm
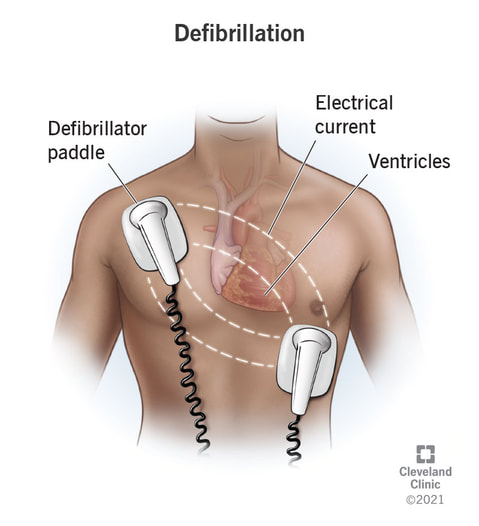
• Place the defibrillator gel pads on the patient's chest; one under the right clavicle and the other inferolateral to the cardiac ape
• Select the 'synchronous mode' on the defibrillator
• D Select the joules (J) required (see below)
• Place the paddles firmly on the chest on the gel pads
• Press the charge button on the paddles to charge the defibrillator and shout 'Stand clear! Charging!'
• Check all persons are standing well clear of the patient and bed (including yourself and that no one is touching the patient or bed (including yourself)
• Ensure the oxygen has been disconnected and removed
• I Check the monitor again to ensure a shockable rhythm
• Shout 'Stand clear! Shocking!'
• Press both discharge buttons on the paddles simultaneously to discharge the shock
• Return the paddles to the defibrillator or keep them on the chest if another shock is required.
Energy Selection
DC Cardioversion usually uses biphasic energies. A reasonable general guide is:
• 50] synchronized shock. If fails..
• 100] synchronized shock. If fails...
• 150] synchronized shock. If fails..
• 150J synchronized anteroposterior shock. If fails...
• Abandon procedure if elective, consult seniors if emergency (may need ICU input).
Contraindications
• Elective: patients unsuitable for general anesthetic, not anticoagulated or who have not signed a consent form
• Emergency: only performed when a tachyarrhythmia is associated with adverse events in the presence of a pulse (pulseless rhythms require management as per the resuscitation guidelines).
Risks
• General anaesthetic risk, if performed electively
• Embolic phenomenon, stroke, myocardial infarction.
Documentation
General
• Date, time and place. Name and grade of persons present
• ECG rhythm
• IV access secured
• Number, volume, dose of any drugs used, and any response noted
• Type of defibrillator machine used
• Method of sedation/anaesthetic
• Asynchronous or synchronous mode. Specify joules of each shock
• Confirm rhythm at end and 12-lead ECG findings
• Sign and bleep/contact details.
Elective
• Indication for DC cardioversion
• Informed consent obtained (retain copy of signed form)
• State time fasted from
• Document anticoagulation type and duration
• Serum potassium level
• Any drug allergies
• Name and grade of anaesthetist
• Type of anaesthetic used.
Emergency
• Events leading up to the peri-arrest situation
• HR, BP, Glasgow coma score on arrival and any deterioration
• Time of decision to shock, name and grade of decision-maker
• Verbal consent obtained?
• Type of sedation used
• Next of kin have been informed or if they are present or on route?
0 Comments
