- Published on
Clinical Procedures – Endoscopic Retrograde Cholangiopancreatography ( ERCP)
Indications
• Diagnostic: largely superseded by safer modalities such as endoscopic ultrasound and MRI/MRCP. Diagnostic indications include sphincter of Oddi dysfunction and primary sclerosing cholangitis
• Therapeutic: endoscopic sphincterotomy (biliary and pancreatic), removal of stones, dilation of strictures (e.g. primary sclerosing cholangitis), stent placement.
Contraindications
• Lack of informed consent, uncooperative patient, recent attack of pancreatitis, recent Ml, history of contrast anaphylaxis, severe cardiopulmonary disease, futility (anticipated short-term survival with no features of sepsis).
Procedure
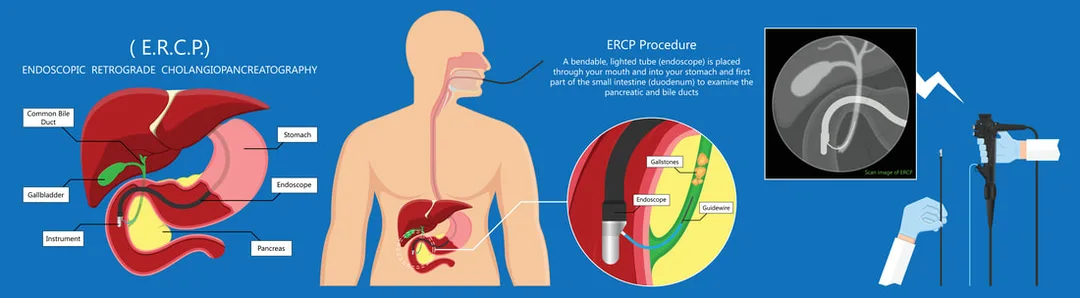
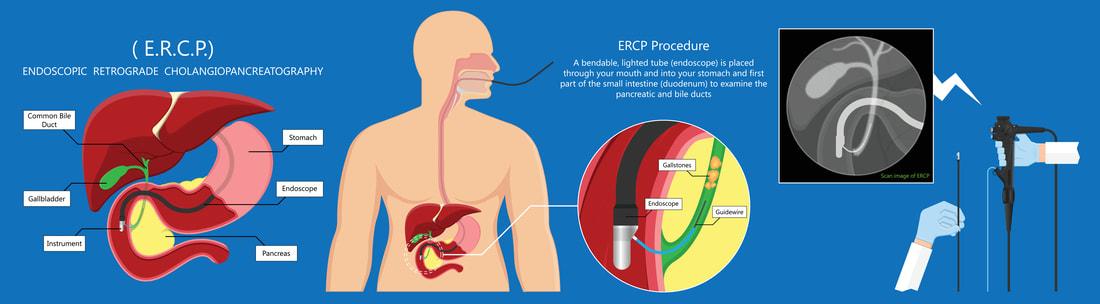
An ERCP involves the passage of an endoscope into the duodenum. The endoscopist injects contrast medium through the ampulla of Vater via a catheter. Real-time fluoroscopy is used to visualize the pancreas and biliary tree. Selected images are taken.
• Dentures (if present) are removed
• Patient is given anaesthetic throat spray (lidocaine) and sometimes IV sedation/analgesia (e.g. midazolam, pethidine)
• Patient lies on the couch in a modified left lateral ('swimmer's") position with the left arm adducted and the right abducted. The endoscope is inserted as for OGD
• Under x-ray guidance, a polyethylene catheter is inserted into the biliary tree and contrast instilled to outline the pancreatic duct as well as the common bile duct and its tributaries
• Procedure time varies from 30-90 minutes.
Risks
• Pancreatitis (2-9% of procedures of which 10% of cases are mild-moderate). Serum amylase is temporarily raised in 70%
• Infection (ascending cholangitis, acute cholecystitis, infected pancreatic pseudocyst, liver abscess, endocarditis
• Bleeding, perforation of the oesophagus, duodenum, bile ducts
• Failure of gallstone retrieval
• Prolonged pancreatic stenting associated with stent occlusion, pancreatic duct obstruction, pseudocyst formation
• Basket impaction around a large gallstone (may require surgery).
Patient Preparation
• Blood tests: liver enzymes, platelets and clotting are checked prior to the procedure.
• Nil by mouth: 4 hours except in the case of an emergency.
• Antibiotic prophylaxis: recommended for:
• Patients in whom biliary decompression is unlikely to be achieved at a single procedure (e.g. dilatation of dominant stricture in multifocal sclerosing cholangitis or hilar cholangiocarcinoma)
• Consider also in patients with severe neutropenia (<0.5 × 109/L) and/ or profound immunocompromise.
Other Information
• © I sedation and analgesia is usually administered and the back of the throat is sprayed with local anaesthetic
• Hilar biliary obstruction demonstrated on MR or CT imaging may be more successfully stented using percutaneous transhepatic cholangiography (PTC) than ERCP
• Equipment allowing direct cholangioscopy (with the potential for sampling lesions) is becoming more widely available.
Indications
• Diagnostic: largely superseded by safer modalities such as endoscopic ultrasound and MRI/MRCP. Diagnostic indications include sphincter of Oddi dysfunction and primary sclerosing cholangitis
• Therapeutic: endoscopic sphincterotomy (biliary and pancreatic), removal of stones, dilation of strictures (e.g. primary sclerosing cholangitis), stent placement.
Contraindications
• Lack of informed consent, uncooperative patient, recent attack of pancreatitis, recent Ml, history of contrast anaphylaxis, severe cardiopulmonary disease, futility (anticipated short-term survival with no features of sepsis).
Procedure
An ERCP involves the passage of an endoscope into the duodenum. The endoscopist injects contrast medium through the ampulla of Vater via a catheter. Real-time fluoroscopy is used to visualize the pancreas and biliary tree. Selected images are taken.
• Dentures (if present) are removed
• Patient is given anaesthetic throat spray (lidocaine) and sometimes IV sedation/analgesia (e.g. midazolam, pethidine)
• Patient lies on the couch in a modified left lateral ('swimmer's") position with the left arm adducted and the right abducted. The endoscope is inserted as for OGD
• Under x-ray guidance, a polyethylene catheter is inserted into the biliary tree and contrast instilled to outline the pancreatic duct as well as the common bile duct and its tributaries
• Procedure time varies from 30-90 minutes.
Risks
• Pancreatitis (2-9% of procedures of which 10% of cases are mild-moderate). Serum amylase is temporarily raised in 70%
• Infection (ascending cholangitis, acute cholecystitis, infected pancreatic pseudocyst, liver abscess, endocarditis
• Bleeding, perforation of the oesophagus, duodenum, bile ducts
• Failure of gallstone retrieval
• Prolonged pancreatic stenting associated with stent occlusion, pancreatic duct obstruction, pseudocyst formation
• Basket impaction around a large gallstone (may require surgery).
Patient Preparation
• Blood tests: liver enzymes, platelets and clotting are checked prior to the procedure.
• Nil by mouth: 4 hours except in the case of an emergency.
• Antibiotic prophylaxis: recommended for:
• Patients in whom biliary decompression is unlikely to be achieved at a single procedure (e.g. dilatation of dominant stricture in multifocal sclerosing cholangitis or hilar cholangiocarcinoma)
• Consider also in patients with severe neutropenia (<0.5 × 109/L) and/ or profound immunocompromise.
Other Information
• © I sedation and analgesia is usually administered and the back of the throat is sprayed with local anaesthetic
• Hilar biliary obstruction demonstrated on MR or CT imaging may be more successfully stented using percutaneous transhepatic cholangiography (PTC) than ERCP
• Equipment allowing direct cholangioscopy (with the potential for sampling lesions) is becoming more widely available.
0 Comments
