- Published on
Clinical Procedures – Knee Joint Aspiration
Indications
• Differential diagnosis of acute hot swollen joint
• Recurrent aspiration for joint sepsis.
Contraindications
• Superficial infection or broken skin
• Coagulopathy: patients with thrombocytopenia or a high IN should be discussed with rheumatologist or orthopedic surgeon before a joint injection is attempted
• Prosthetic joint. This is a relative contraindication. A prosthetic joint should be aspirated by an orthopedic surgeon in a theatre using full surgical sterile precautions.
Risks
• Discomfort: usually short lived and minor
• Septic arthritis: risk is very small (1 in 78,000 in a recent retrospective study from France).
Procedure Tips
• If you are unable to aspirate synovial fluid:
•Simply withdraw the needle and insert at a different angle (aiming inferomedially)
• Change the position of the patient. Ask them to sit on the edge of a bed with their feet on a stool or chair and repeat the procedure in this position
• Other joints may be aspirated using a similar technique. Use 23-25G (blue, orange) for small joints such as wrist, MCP.
Aspiration of a prosthetic joint should be performed by an Orthopaedic Surgeon in a theatre with full surgical sterility.
Equipment
• Sterile gloves
• Isopropyl alcohol swabs
• 21G (green) needles
• 10mL syringe
• White-capped universal containers
• Elastoplast or cotton wool and sticky tape.
Procedure (Medial Approach)
• Introduce yourself, confirm the patient's identity, explain the procedure, and obtain informed consent
• Position the patient resting on a couch with the leg slightly flexed and supported on a pillow (relaxes quadriceps)
• Identify and mark the point of entry just below the midpoint of the patella by indenting the skin with the tip of a syringe
• Wash hands and put on the gloves
• ( A no-touch technique is essential after cleaning so any mark to identify the point of entry should be made earlier
• Wipe the site with alcohol swabs
• Attach a 10mL syringe to a green needle
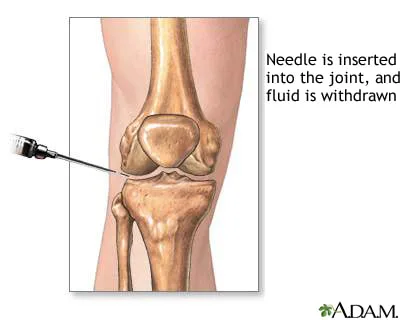
• Insert the needle just below the midpoint of patella, aiming behind the patella. Your free hand can apply pressure to move any synovial fluid to the medial side
• Intra-articular placement of the needle is confirmed by effortless aspiration of synovial fluid
• If the syringe fills up, it can be detached from the needle, the synovial fluid discarded in a specimen pot, and the syringe re-attached to the needle to aspirate more synovial fluid
• Withdraw the needle and dress the site with a suitable plaster
• Send the samples for crystal study, Gram stain, and culture.
Procedure (Superolateral Approach)
Used for large effusions that distend the suprapatellar pouch.
• The needle is introduced above and lateral to the patella at the maximum convexity of the distended pouch
• The needle should be inserted at a 45° angle and aimed inferiorly and medially under the patella
• Continue to advance the needle with negative pressure on the plunger until fluid is aspirated.
Documentation
• Date, time, indication, informed consent obtained
• Site and approach taken
• Aseptic technique used?
• How many passes?
• Volume and nature of fluid aspirated and tests requested:
• The pathology request form should provide the pathologist with information on the date, time, and site of joint aspirate
• The sample should be sent to the laboratories and analysed fresh for crystals, Gram stain, and culture.
The laboratory should be alerted if septic arthritis is suspected
• Any immediate complications
• Signature, printed name, and contact details.
Indications
• Differential diagnosis of acute hot swollen joint
• Recurrent aspiration for joint sepsis.
Contraindications
• Superficial infection or broken skin
• Coagulopathy: patients with thrombocytopenia or a high IN should be discussed with rheumatologist or orthopedic surgeon before a joint injection is attempted
• Prosthetic joint. This is a relative contraindication. A prosthetic joint should be aspirated by an orthopedic surgeon in a theatre using full surgical sterile precautions.
Risks
• Discomfort: usually short lived and minor
• Septic arthritis: risk is very small (1 in 78,000 in a recent retrospective study from France).
Procedure Tips
• If you are unable to aspirate synovial fluid:
•Simply withdraw the needle and insert at a different angle (aiming inferomedially)
• Change the position of the patient. Ask them to sit on the edge of a bed with their feet on a stool or chair and repeat the procedure in this position
• Other joints may be aspirated using a similar technique. Use 23-25G (blue, orange) for small joints such as wrist, MCP.
Aspiration of a prosthetic joint should be performed by an Orthopaedic Surgeon in a theatre with full surgical sterility.
Equipment
• Sterile gloves
• Isopropyl alcohol swabs
• 21G (green) needles
• 10mL syringe
• White-capped universal containers
• Elastoplast or cotton wool and sticky tape.
Procedure (Medial Approach)
• Introduce yourself, confirm the patient's identity, explain the procedure, and obtain informed consent
• Position the patient resting on a couch with the leg slightly flexed and supported on a pillow (relaxes quadriceps)
• Identify and mark the point of entry just below the midpoint of the patella by indenting the skin with the tip of a syringe
• Wash hands and put on the gloves
• ( A no-touch technique is essential after cleaning so any mark to identify the point of entry should be made earlier
• Wipe the site with alcohol swabs
• Attach a 10mL syringe to a green needle
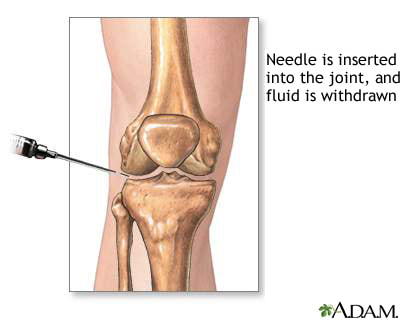
• Insert the needle just below the midpoint of patella, aiming behind the patella. Your free hand can apply pressure to move any synovial fluid to the medial side
• Intra-articular placement of the needle is confirmed by effortless aspiration of synovial fluid
• If the syringe fills up, it can be detached from the needle, the synovial fluid discarded in a specimen pot, and the syringe re-attached to the needle to aspirate more synovial fluid
• Withdraw the needle and dress the site with a suitable plaster
• Send the samples for crystal study, Gram stain, and culture.
Procedure (Superolateral Approach)
Used for large effusions that distend the suprapatellar pouch.
• The needle is introduced above and lateral to the patella at the maximum convexity of the distended pouch
• The needle should be inserted at a 45° angle and aimed inferiorly and medially under the patella
• Continue to advance the needle with negative pressure on the plunger until fluid is aspirated.
Documentation
• Date, time, indication, informed consent obtained
• Site and approach taken
• Aseptic technique used?
• How many passes?
• Volume and nature of fluid aspirated and tests requested:
• The pathology request form should provide the pathologist with information on the date, time, and site of joint aspirate
• The sample should be sent to the laboratories and analysed fresh for crystals, Gram stain, and culture.
The laboratory should be alerted if septic arthritis is suspected
• Any immediate complications
• Signature, printed name, and contact details.
0 Comments
