- Published on
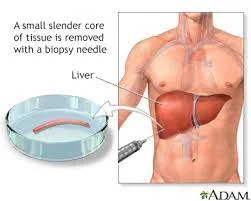
Clinical Procedures - Percutaneous Liver Biopsy
The following describes the technique when using a suction (Menghini) liver biopsy needle.
• Increasingly, 'blind' biopsies are being replaced by ultrasound-guided biopsies performed by the Radiology Department. Check your local guidelines.
Equipment
• Dressing pack (including gauze, bowl, drape)
• Antiseptic solution
• Sterile gloves and gown
• Local anaesthetic (e.g. 1% lidocaine)
• 2 x 10 mL syringes
• 2 × 23G (blue) needles
• Liver biopsy needles/pack
• 10mL sterile saline
• Scalpel/blade
• Tissue/biopsy collection pot.
Procedure
• Introduce yourself, confirm the patient's identity, explain the procedure, and obtain informed consent
• Review the patient's clotting profile and platelet count:
• If platelets <60 × 10°/L or prothrombin time >3 seconds prolonged, consider transjugular approach or clotting factor support
• D Ensure antiplatelets and anticoagulants are stopped at least 3 days prior to procedure to minimize risk of bleeding
• Ensure the patient has IV access
• Position the patient supine with the right arm abducted
• Examine the patient and percuss the borders of the liver before choosing a biopsy site. This is usually at the 7th or 8th intercostal space in the midaxillary line
• Confirm the site with ultrasonography:
• Confirm the direction the needle will take and a safe depth for the biopsy. Ensure that there are no major vessels within the liver at this point and that no bowel lies between the liver and abdominal wall
• Clean the area with antiseptic solution
• Administer local anaesthetic using both a 23G (blue) and
21G (green) needle down to the depth of the liver capsule
• Make a small incision at the point of insertion with the blade
• Half-fill a syringe with saline and attach to the biopsy needle
• Introduce the biopsy needle just above a rib
• As the needle is advanced, flush small amounts of saline until resistance is encountered (the liver surface)
• Pull back the plunger to apply suction and ask the patient to exhale completely and hold the breath in exhalation
• Whilst maintaining suction on the syringe, push the needle into the liver to the depth and direction estimated previously and then quickly remove the needle
• This should be a quick, fluid movement taking 1 second
• The biopsy now lies either within the needle or the syringe
• Deposit the sample in a suitable collection container:
• Judging an 'adequate' biopsy is controversial, but 2.5 cm is the ideal
• If the sample lies within the syringe, don't try to expel it through the needle, this will damage the tissue. Instead, remove the plunger from the syringe completely and pour the contents into the collection pot
• Apply pressure to the biopsy site for a couple of minutes and then cover with a suitable dressing.
Documentation
• Date, time, indication, informed consent obtained
• How was liver position confirmed?
• Type and volume of local anaesthetic used
• How many passes?
• No more than 2 passes should be made (British
Society of Gastroenterology (BS) guidelines 2004)
• Size and nature of the sample obtained
• Any immediate complications
• Instructions for monitoring and discharge if day-case
• Signature, printed name, and contact details.
Indications
• Staging of chronic hepatitis B and C
• Non-alcoholic liver disease (NAFLD)
• Diagnosis of other chronic liver diseases such as Wilson's, haemochromatosis, primary biliary cirrhosis, and sclerosing cholangitis:
• A 4mm portion can be analysed by some clinical chemistry departments for iron or copper index. The sample should be sent on saline-soaked filter paper in a plain universal tube
• Unexplained altered liver function tests
• Suspected malignant lesion
• To exclude rejection in a previous liver transplant patient.
Contraindications
• Uncooperative patient
• Dilated biliary system (risk of biliary peritonitis)
• Thrombocytopenia or coagulopathy
• Ascites
• Vascular or cystic lesions
• Amyloidosis (risk of haemorrhage increased).
Risks
• Haemo- or pneumothorax, intraperitoneal hemorrhage
• Pain, hypotension, sepsis
•Biliary leak due to gallbladder puncture, injury to other organs.
Procedure Tips
• Check the patient's clotting profile and platelet count. Do not perform if INR >1.3 or platelets <50 x 10°/L
• Ensure blood is group and saved prior to the procedure
• The biopsy sample should have clear clinical information on the request form for the Pathologist.
Post-procedure monitoring
Practice varies and you should consult your local guidelines. Most bleeding complications arise within the first 2 hours post-procedure.
A reasonable strategy (based on guidelines from the BS) is:
• Patient to be monitored for total 6 hours
• Monitor vital signs every 15 minutes for first 2 hours
• Monitor vital signs every 30 minutes for next 2 hours
• Monitor vital signs hourly for remaining time.
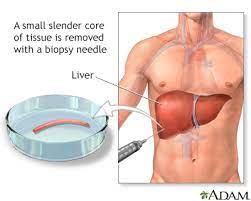
The following describes the technique when using a suction (Menghini) liver biopsy needle.
• Increasingly, 'blind' biopsies are being replaced by ultrasound-guided biopsies performed by the Radiology Department. Check your local guidelines.
Equipment
• Dressing pack (including gauze, bowl, drape)
• Antiseptic solution
• Sterile gloves and gown
• Local anaesthetic (e.g. 1% lidocaine)
• 2 x 10 mL syringes
• 2 × 23G (blue) needles
• Liver biopsy needles/pack
• 10mL sterile saline
• Scalpel/blade
• Tissue/biopsy collection pot.
Procedure
• Introduce yourself, confirm the patient's identity, explain the procedure, and obtain informed consent
• Review the patient's clotting profile and platelet count:
• If platelets <60 × 10°/L or prothrombin time >3 seconds prolonged, consider transjugular approach or clotting factor support
• D Ensure antiplatelets and anticoagulants are stopped at least 3 days prior to procedure to minimize risk of bleeding
• Ensure the patient has IV access
• Position the patient supine with the right arm abducted
• Examine the patient and percuss the borders of the liver before choosing a biopsy site. This is usually at the 7th or 8th intercostal space in the midaxillary line
• Confirm the site with ultrasonography:
• Confirm the direction the needle will take and a safe depth for the biopsy. Ensure that there are no major vessels within the liver at this point and that no bowel lies between the liver and abdominal wall
• Clean the area with antiseptic solution
• Administer local anaesthetic using both a 23G (blue) and
21G (green) needle down to the depth of the liver capsule
• Make a small incision at the point of insertion with the blade
• Half-fill a syringe with saline and attach to the biopsy needle
• Introduce the biopsy needle just above a rib
• As the needle is advanced, flush small amounts of saline until resistance is encountered (the liver surface)
• Pull back the plunger to apply suction and ask the patient to exhale completely and hold the breath in exhalation
• Whilst maintaining suction on the syringe, push the needle into the liver to the depth and direction estimated previously and then quickly remove the needle
• This should be a quick, fluid movement taking 1 second
• The biopsy now lies either within the needle or the syringe
• Deposit the sample in a suitable collection container:
• Judging an 'adequate' biopsy is controversial, but 2.5 cm is the ideal
• If the sample lies within the syringe, don't try to expel it through the needle, this will damage the tissue. Instead, remove the plunger from the syringe completely and pour the contents into the collection pot
• Apply pressure to the biopsy site for a couple of minutes and then cover with a suitable dressing.
Documentation
• Date, time, indication, informed consent obtained
• How was liver position confirmed?
• Type and volume of local anaesthetic used
• How many passes?
• No more than 2 passes should be made (British
Society of Gastroenterology (BS) guidelines 2004)
• Size and nature of the sample obtained
• Any immediate complications
• Instructions for monitoring and discharge if day-case
• Signature, printed name, and contact details.
Indications
• Staging of chronic hepatitis B and C
• Non-alcoholic liver disease (NAFLD)
• Diagnosis of other chronic liver diseases such as Wilson's, haemochromatosis, primary biliary cirrhosis, and sclerosing cholangitis:
• A 4mm portion can be analysed by some clinical chemistry departments for iron or copper index. The sample should be sent on saline-soaked filter paper in a plain universal tube
• Unexplained altered liver function tests
• Suspected malignant lesion
• To exclude rejection in a previous liver transplant patient.
Contraindications
• Uncooperative patient
• Dilated biliary system (risk of biliary peritonitis)
• Thrombocytopenia or coagulopathy
• Ascites
• Vascular or cystic lesions
• Amyloidosis (risk of haemorrhage increased).
Risks
• Haemo- or pneumothorax, intraperitoneal hemorrhage
• Pain, hypotension, sepsis
•Biliary leak due to gallbladder puncture, injury to other organs.
Procedure Tips
• Check the patient's clotting profile and platelet count. Do not perform if INR >1.3 or platelets <50 x 10°/L
• Ensure blood is group and saved prior to the procedure
• The biopsy sample should have clear clinical information on the request form for the Pathologist.
Post-procedure monitoring
Practice varies and you should consult your local guidelines. Most bleeding complications arise within the first 2 hours post-procedure.
A reasonable strategy (based on guidelines from the BS) is:
• Patient to be monitored for total 6 hours
• Monitor vital signs every 15 minutes for first 2 hours
• Monitor vital signs every 30 minutes for next 2 hours
• Monitor vital signs hourly for remaining time.
0 Comments
