- Published on
Clinical Procedures - Pneumothorax Aspiration
Indications
Simple pneumothorax
• Aspiration is indicated if the rim of pleural air visible on chest radiograph is >2cm or the patient is breathless
• If initial aspiration is unsuccessful, repeat aspiration may be successful in
>30% of cases and may avoid intercostal drain insertion
• The total volume aspirated should not exceed 2.5L.
Secondary pneumothorax
• That is, a pneumothorax in the presence of underlying lung disease
• Aspiration is only indicated in minimally symptomatic patients with small pneumothoraces (<2cm) aged <50 years.
Contraindications
• Previous failed attempts at aspiration
• Significant secondary pneumothorax
• Traumatic pneumothorax.
Risks
• Pain
• Cough
• Failure to resolve/recurrence
• Re-expansion pulmonary edema may theoretically occur if large volumes (>2.5L) are aspirated.
• Tension Pneumothorax
In the case of tension pneumothorax, a wide-bore cannula should be inserted into the 2nd intercostal space, midclavicular line without delay and left open to convert the tension pneumothorax to a simple pneumothorax.
Equipment
• Sterile pack
• Sterile gloves
• Cleaning solution (e.g. chlorhexidine)
• Large-bore (green) cannula
• 3-way tap
• 50mL syringe
• 5mL 1% lidocaine
• 23G (blue) needle
• 2 x 10mL syringe
• Dressing/gauze.
Procedure
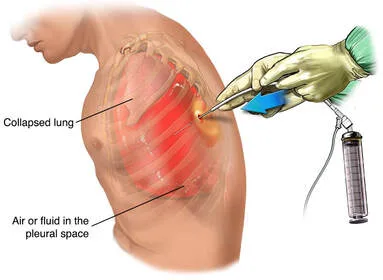
• Pneumothorax is usually aspirated from either the 2nd intercostal space at the midclavicular line or the 4th_ 6th intercostal spaces at the midaxillary line.
• Introduce yourself, confirm the patient's identity, explain the procedure, and obtain informed consent
• Position the patient leaning back comfortably at about 45°
• Identify the site for needle insertion and double-check the radiograph to be certain you have the correct side. Confirm with clinical examination
• Clean the area with the chlorhexidine
• Infiltrate local anaesthetic down to the pleura using the blue needle and a 10mL syringe
• Attach the other 10mL syringe to the cannula and insert the cannula perpendicular to the chest wall, aspirating as you advance until resistance reduces:
• D Insert the cannula just above a rib to avoid the neurovascular bundle
• Remove the needle and quickly attach the 3-way tap and 50mL syringe
• Aspirate with the syringe; close the 3-way tap when the syringe is full, remove the syringe, and eject the air; reattach and open the 3-way tap to continue aspiration:
• © The pleural space should never be in continuity with the environment (i.e. tap open with syringe detached) or pneumothorax will re-accumulate
• Aspirate until resistance is felt, or up to a maximum of 2.5L
• Remove the cannula and apply the dressing
• Request chest radiograph to re-assess.
Documentation
• Date, time, indication, informed consent obtained
• Aseptic technique used?
• Local anaesthetic used
• Site needle inserted
• Volume of air aspirated
• Any immediate complications
• Investigations requested
• Signature, printed name, and contact details.
Indications
Simple pneumothorax
• Aspiration is indicated if the rim of pleural air visible on chest radiograph is >2cm or the patient is breathless
• If initial aspiration is unsuccessful, repeat aspiration may be successful in
>30% of cases and may avoid intercostal drain insertion
• The total volume aspirated should not exceed 2.5L.
Secondary pneumothorax
• That is, a pneumothorax in the presence of underlying lung disease
• Aspiration is only indicated in minimally symptomatic patients with small pneumothoraces (<2cm) aged <50 years.
Contraindications
• Previous failed attempts at aspiration
• Significant secondary pneumothorax
• Traumatic pneumothorax.
Risks
• Pain
• Cough
• Failure to resolve/recurrence
• Re-expansion pulmonary edema may theoretically occur if large volumes (>2.5L) are aspirated.
• Tension Pneumothorax
In the case of tension pneumothorax, a wide-bore cannula should be inserted into the 2nd intercostal space, midclavicular line without delay and left open to convert the tension pneumothorax to a simple pneumothorax.
Equipment
• Sterile pack
• Sterile gloves
• Cleaning solution (e.g. chlorhexidine)
• Large-bore (green) cannula
• 3-way tap
• 50mL syringe
• 5mL 1% lidocaine
• 23G (blue) needle
• 2 x 10mL syringe
• Dressing/gauze.
Procedure
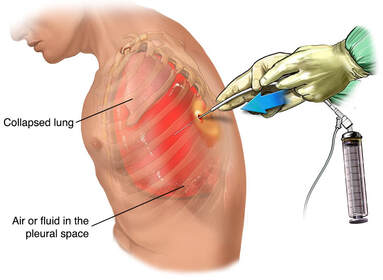
• Pneumothorax is usually aspirated from either the 2nd intercostal space at the midclavicular line or the 4th_ 6th intercostal spaces at the midaxillary line.
• Introduce yourself, confirm the patient's identity, explain the procedure, and obtain informed consent
• Position the patient leaning back comfortably at about 45°
• Identify the site for needle insertion and double-check the radiograph to be certain you have the correct side. Confirm with clinical examination
• Clean the area with the chlorhexidine
• Infiltrate local anaesthetic down to the pleura using the blue needle and a 10mL syringe
• Attach the other 10mL syringe to the cannula and insert the cannula perpendicular to the chest wall, aspirating as you advance until resistance reduces:
• D Insert the cannula just above a rib to avoid the neurovascular bundle
• Remove the needle and quickly attach the 3-way tap and 50mL syringe
• Aspirate with the syringe; close the 3-way tap when the syringe is full, remove the syringe, and eject the air; reattach and open the 3-way tap to continue aspiration:
• © The pleural space should never be in continuity with the environment (i.e. tap open with syringe detached) or pneumothorax will re-accumulate
• Aspirate until resistance is felt, or up to a maximum of 2.5L
• Remove the cannula and apply the dressing
• Request chest radiograph to re-assess.
Documentation
• Date, time, indication, informed consent obtained
• Aseptic technique used?
• Local anaesthetic used
• Site needle inserted
• Volume of air aspirated
• Any immediate complications
• Investigations requested
• Signature, printed name, and contact details.
0 Comments
