- Published on
Clinical Procedures - Sengstaken-Blakemore Tube Insertion
Indications
• Life-threatening variceal bleeding where facilities for endoscopy are not available or pending endoscopic therapy
• Life-threatening variceal bleeding where other modalities to control bleeding have failed.
Contraindications
• Variceal bleeding has ceased or significantly slowed
• Recent surgery to the GO]
• Known esophageal stricture (s).
Risks
• Mucosal necrosis due to inadvertent traction
• Oesophageal perforation. This may be due to a gastric balloon being inflated within the esophagus or can occur secondary to over- or prolonged inflation of the esophageal balloon
• Aspiration of fluid into the respiratory tract. The greatest risk occurs during insertion
• Asphyxiation due to superior migration of the tube and balloons. See last 'procedure tip' below.
Procedure Tips
• The tube can be used as a measure to control bleeding for about
12-18 hours. Generally, it should not be left in place for >24 hours
• Frequent aspirations from the gastric port are needed to assess the status of bleeding
• The tube has to remain in traction at the gastric balloon which will decompress the varices. However, direct pressure from the tube can cause mucosal ulceration. Examine frequently to ensure that excessive force is not being exerted
• If the balloons migrate superiorly, airway obstruction may occur. In this instance, as an emergency measure, the tube can be quickly cut with a pair of scissors and removed. Keep a pair of scissors handy.
This should be performed only by senior medical staff in close liaison with an anaesthetist and, ideally, with endotracheal intubation especially in agitated patients and those with hepatic encephalopathy.
• The threshold to perform endotracheal intubation should be low, as the risk of regurgitation and aspiration is extremely high. To minimize this risk, perform nasogastric lavage and maximal stomach evacuation prior to procedure.
Equipment
• Gloves, gown, and goggles
• Saline flush
• 2 x 50mL syringe.
• Local anaesthetic spray
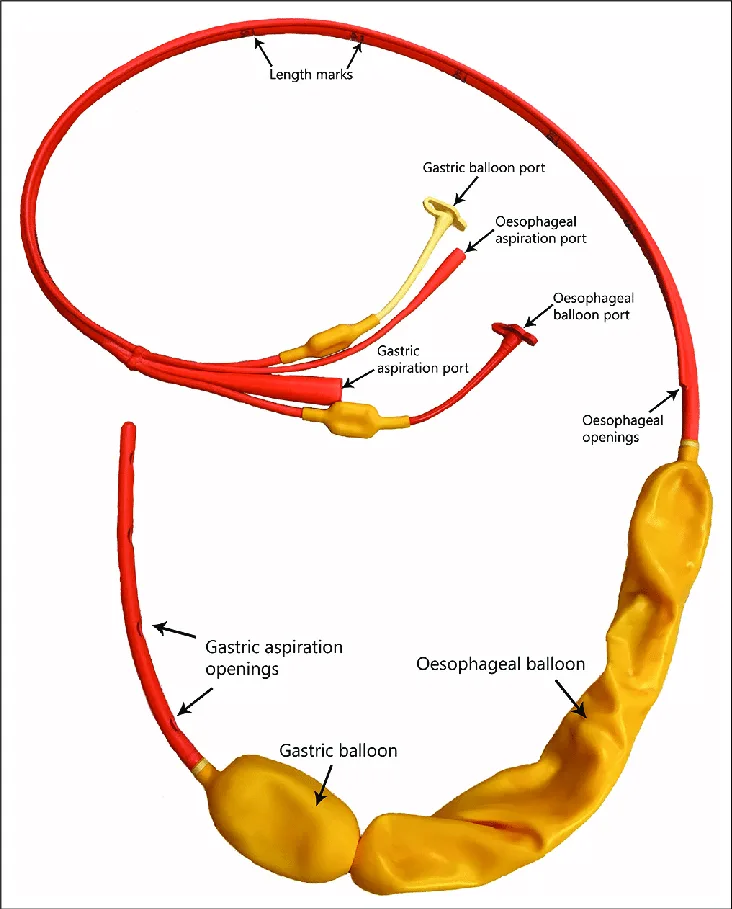
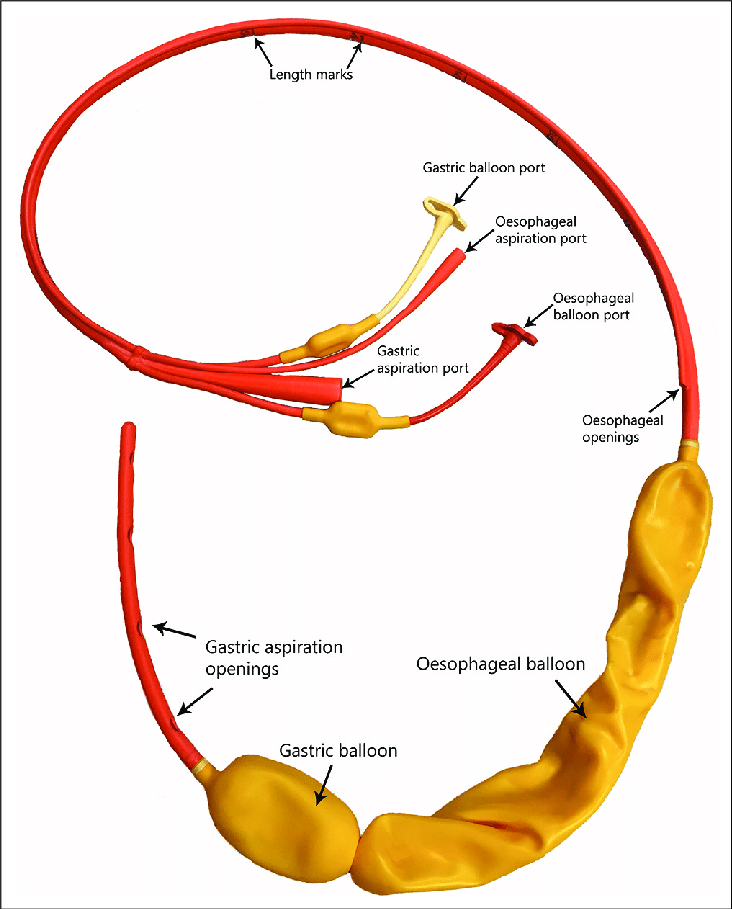
• Sengstaken-Blakemore tube (usually kept in refrigerator to increase its stiffness)
• Lubricant jelly (e.g. Aquagel®
• Basin with sterile water
• Suction equipment
• Sphygmomanometer for pressure monitoring.
Procedure
• Introduce yourself, confirm the patient's identity, explain the procedure to the patient, and obtain informed consent
• Position the patient at 45°
• Administer anaesthetic throat spray to the oropharynx
• Check the balloons in the tube for air leak by inflating them with an air-filled syringe and immersing in a basin of water.
Air leak is indicated by air bubbles appearing
• Deflate the balloons
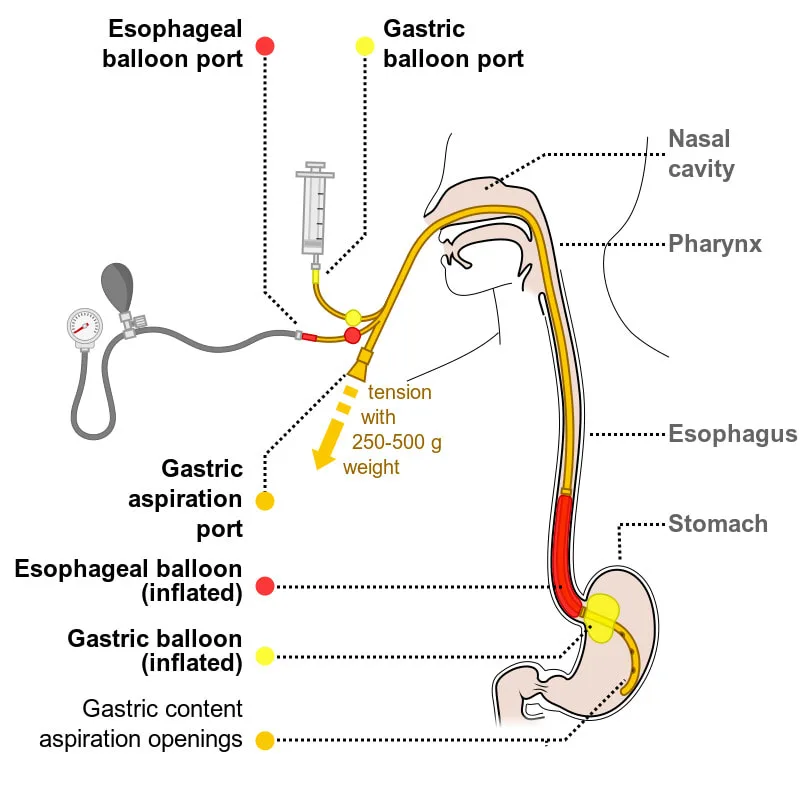
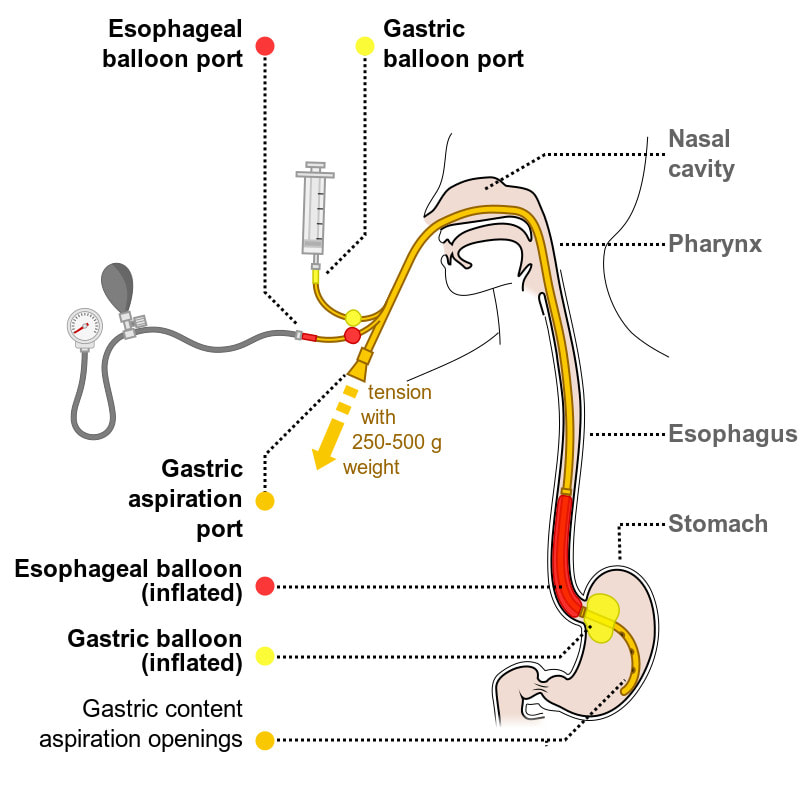
• Apply lubricant over the tip of the tube and advance it through the oral cavity slowly until it crosses the gastro-oesophageal junction (GOJ):
• The GOJ is generally 38-42cm from the nostril so advancement of the tube 55-60cm usually positions the tip within the stomach
• Withdraw if the patient becomes breathless
• Inflate the gastric (not esophageal) balloon with 50mL air
• At this stage an abdominal radiograph may be performed to confirm the position of the tube in the stomach
• Once position is confirmed, inflate the gastric balloon to a total volume of 250mL air
• Pull gently on the tube until resistance is felt
• Secure with tape near the mouth with gauze pads, maintaining traction and tie the tube to a 500mL bag of saline. A pulley (e.g. a drip stand) is helpful in maintaining traction
• Mark the tube near the mouth which will serve as an indicator to whether the tube has migrated later
• Flush the gastric port with normal saline and aspirate at frequent intervals until it is clear, which indicates that bleeding has ceased
• • If bleeding continues, inflate the esophageal balloon with 40mL air and monitor the pressures using the sphygmomanometer at frequent intervals
• D After 12 hours of traction, relax the tension and push the tube into the stomach. If there is evidence of further bleeding, the gastric balloon can be re-inflated and traction re-applied with a view to repeat therapeutic endoscopy
• D During extubation (usually after 10-12 hours depending on clinical condition), deflate the gastric balloon first then the esophageal balloon and withdraw the tube slowly.
Documentation
• Date, time, indication, informed consent obtained
• Those present, including anaesthetic support
• How many passes?
• Volume balloon inflated to and level of tube insertion
• Any immediate complications
• Signature, printed name, and contact details.
Indications
• Life-threatening variceal bleeding where facilities for endoscopy are not available or pending endoscopic therapy
• Life-threatening variceal bleeding where other modalities to control bleeding have failed.
Contraindications
• Variceal bleeding has ceased or significantly slowed
• Recent surgery to the GO]
• Known esophageal stricture (s).
Risks
• Mucosal necrosis due to inadvertent traction
• Oesophageal perforation. This may be due to a gastric balloon being inflated within the esophagus or can occur secondary to over- or prolonged inflation of the esophageal balloon
• Aspiration of fluid into the respiratory tract. The greatest risk occurs during insertion
• Asphyxiation due to superior migration of the tube and balloons. See last 'procedure tip' below.
Procedure Tips
• The tube can be used as a measure to control bleeding for about
12-18 hours. Generally, it should not be left in place for >24 hours
• Frequent aspirations from the gastric port are needed to assess the status of bleeding
• The tube has to remain in traction at the gastric balloon which will decompress the varices. However, direct pressure from the tube can cause mucosal ulceration. Examine frequently to ensure that excessive force is not being exerted
• If the balloons migrate superiorly, airway obstruction may occur. In this instance, as an emergency measure, the tube can be quickly cut with a pair of scissors and removed. Keep a pair of scissors handy.
This should be performed only by senior medical staff in close liaison with an anaesthetist and, ideally, with endotracheal intubation especially in agitated patients and those with hepatic encephalopathy.
• The threshold to perform endotracheal intubation should be low, as the risk of regurgitation and aspiration is extremely high. To minimize this risk, perform nasogastric lavage and maximal stomach evacuation prior to procedure.
Equipment
• Gloves, gown, and goggles
• Saline flush
• 2 x 50mL syringe.
• Local anaesthetic spray
• Sengstaken-Blakemore tube (usually kept in refrigerator to increase its stiffness)
• Lubricant jelly (e.g. Aquagel®
• Basin with sterile water
• Suction equipment
• Sphygmomanometer for pressure monitoring.
Procedure
• Introduce yourself, confirm the patient's identity, explain the procedure to the patient, and obtain informed consent
• Position the patient at 45°
• Administer anaesthetic throat spray to the oropharynx
• Check the balloons in the tube for air leak by inflating them with an air-filled syringe and immersing in a basin of water.
Air leak is indicated by air bubbles appearing
• Deflate the balloons
• Apply lubricant over the tip of the tube and advance it through the oral cavity slowly until it crosses the gastro-oesophageal junction (GOJ):
• The GOJ is generally 38-42cm from the nostril so advancement of the tube 55-60cm usually positions the tip within the stomach
• Withdraw if the patient becomes breathless
• Inflate the gastric (not esophageal) balloon with 50mL air
• At this stage an abdominal radiograph may be performed to confirm the position of the tube in the stomach
• Once position is confirmed, inflate the gastric balloon to a total volume of 250mL air
• Pull gently on the tube until resistance is felt
• Secure with tape near the mouth with gauze pads, maintaining traction and tie the tube to a 500mL bag of saline. A pulley (e.g. a drip stand) is helpful in maintaining traction
• Mark the tube near the mouth which will serve as an indicator to whether the tube has migrated later
• Flush the gastric port with normal saline and aspirate at frequent intervals until it is clear, which indicates that bleeding has ceased
• • If bleeding continues, inflate the esophageal balloon with 40mL air and monitor the pressures using the sphygmomanometer at frequent intervals
• D After 12 hours of traction, relax the tension and push the tube into the stomach. If there is evidence of further bleeding, the gastric balloon can be re-inflated and traction re-applied with a view to repeat therapeutic endoscopy
• D During extubation (usually after 10-12 hours depending on clinical condition), deflate the gastric balloon first then the esophageal balloon and withdraw the tube slowly.
Documentation
• Date, time, indication, informed consent obtained
• Those present, including anaesthetic support
• How many passes?
• Volume balloon inflated to and level of tube insertion
• Any immediate complications
• Signature, printed name, and contact details.
0 Comments
