- Published on
Clinical Procedures – Temporary External Pacing
This describes temporary transcutaneous pacing as an emergency.
Before You Start
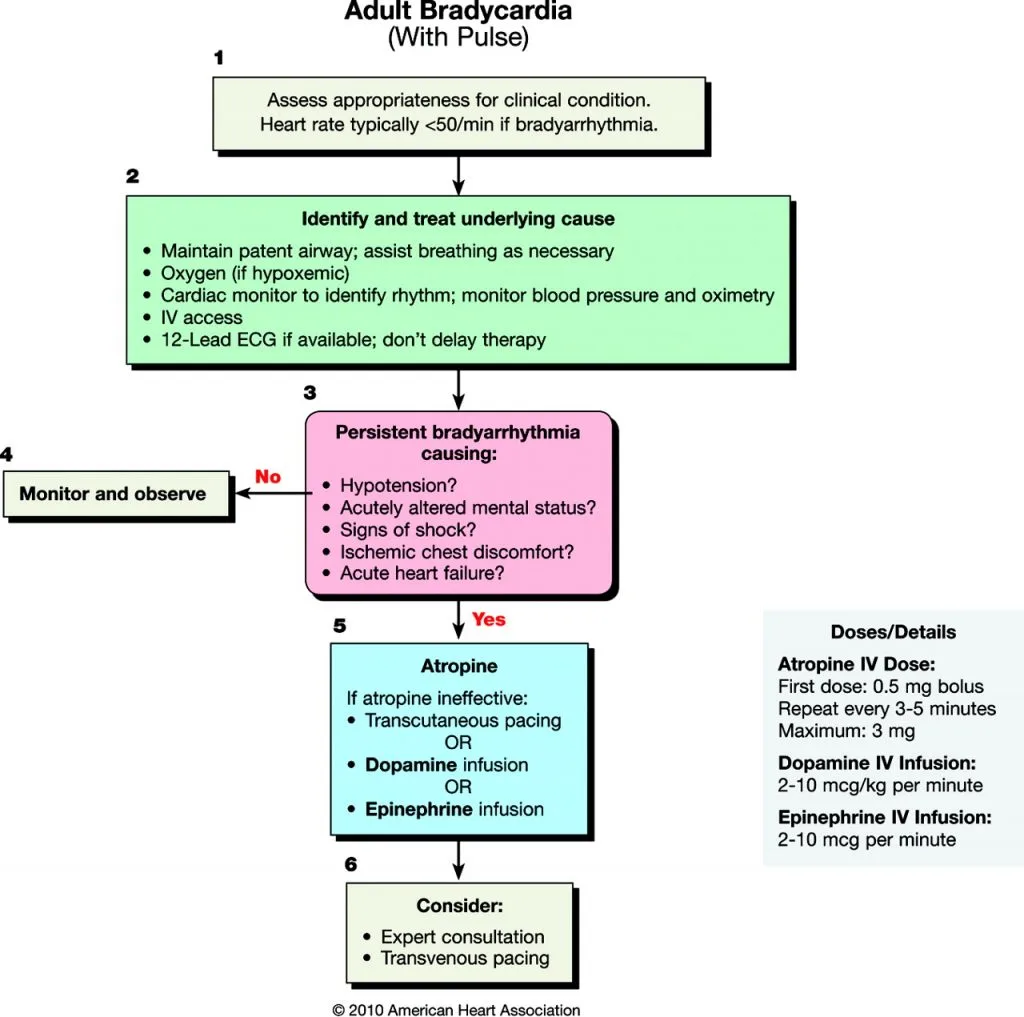
• External pacing is usually performed in an emergency resuscitation situation following failure of response to initial management, as per the bradycardia algorithm from the Resuscitation Council (UK) at the end of this topic
• A senior doctor should be present and make the decision to proceed with external transcutaneous pacing
• There should be a plan in place for an experienced clinician to insert a temporary pacing wire within the next few hours. External pacing should only be a short-term management of decompensated bradycardia
• There should also be a bed available for the patient on a high-dependency unit or coronary care unit so that they can be closely monitored by experienced nursing staff whilst waiting for a temporary pacing wire. The patient should not be left on a general hospital ward.
Indications
• Symptomatic bradycardia unresponsive to treatment (see bradycardia algorithm)
• Mobitz type II block
• Complete heart block
• Heart block secondary to myocardial infarction
• Profound bradycardia secondary to drug overdose, e.g. beta blockers, digoxin
• systole or ventricular standstill
• External pacing can be used as overdrive pacing to terminate certain tachyarrhythmias that are unresponsive to initial treatment, e.g. polymorphic ventricular tachycardia (torsades de pointes) or refractory ventricular tachycardia.
Equipment
• Full resuscitation equipment: defibrillator with pacing setting
• Defibrillator pads
• Oxygen
• ECG monitoring
• Emergency drugs (including atropine and adrenaline)
• IV fluids
• Sedative drugs (e.g. midazolam or diazepam)
• Analgesia (e.g. morphine)
• Intubation equipment (in case indicated)
• Senior support.
Procedure
• The patient should already have:
• Large-bore IV access
• IV fluids running (unless in heart failure)
• Oxygen via a non-rebreathe mask at 15L/min
• ECG monitor connected and running
• Interval BP monitoring
• Place the pacing pads from the defibrillation kit on the patient's chest: one anteriorly in the V3 position and one posteriorly below the left scapula
• Sedation and analgesia may be required
• Attach the leads from the defibrillator to the pads
• Switch the defibrillator to its pacing mode.
Risks
• Failure and progression to temporary pacing wire insertion.
Documentation
Temporary external pacing is usually an emergency procedure so documentation may be delayed until the patient is stable. It should outline the resuscitation and external pacing simultaneously:
• Date and time
• Name and grade of persons present
•Events leading up to the need for external pacing
• Any drugs used, e.g. atropine or adrenaline, volume/ dose, and response
• Indication for external pacing
• If patient was conscious, document consent (usually verbal consent only)
• Any sedation used
• When external pacing commenced
• Details of plans for temporary pacing wire insertion
• Sign and bleep/contact details.
This describes temporary transcutaneous pacing as an emergency.
Before You Start
• External pacing is usually performed in an emergency resuscitation situation following failure of response to initial management, as per the bradycardia algorithm from the Resuscitation Council (UK) at the end of this topic
• A senior doctor should be present and make the decision to proceed with external transcutaneous pacing
• There should be a plan in place for an experienced clinician to insert a temporary pacing wire within the next few hours. External pacing should only be a short-term management of decompensated bradycardia
• There should also be a bed available for the patient on a high-dependency unit or coronary care unit so that they can be closely monitored by experienced nursing staff whilst waiting for a temporary pacing wire. The patient should not be left on a general hospital ward.
Indications
• Symptomatic bradycardia unresponsive to treatment (see bradycardia algorithm)
• Mobitz type II block
• Complete heart block
• Heart block secondary to myocardial infarction
• Profound bradycardia secondary to drug overdose, e.g. beta blockers, digoxin
• systole or ventricular standstill
• External pacing can be used as overdrive pacing to terminate certain tachyarrhythmias that are unresponsive to initial treatment, e.g. polymorphic ventricular tachycardia (torsades de pointes) or refractory ventricular tachycardia.
Equipment
• Full resuscitation equipment: defibrillator with pacing setting
• Defibrillator pads
• Oxygen
• ECG monitoring
• Emergency drugs (including atropine and adrenaline)
• IV fluids
• Sedative drugs (e.g. midazolam or diazepam)
• Analgesia (e.g. morphine)
• Intubation equipment (in case indicated)
• Senior support.
Procedure
• The patient should already have:
• Large-bore IV access
• IV fluids running (unless in heart failure)
• Oxygen via a non-rebreathe mask at 15L/min
• ECG monitor connected and running
• Interval BP monitoring
• Place the pacing pads from the defibrillation kit on the patient's chest: one anteriorly in the V3 position and one posteriorly below the left scapula
• Sedation and analgesia may be required
• Attach the leads from the defibrillator to the pads
• Switch the defibrillator to its pacing mode.
Risks
• Failure and progression to temporary pacing wire insertion.
Documentation
Temporary external pacing is usually an emergency procedure so documentation may be delayed until the patient is stable. It should outline the resuscitation and external pacing simultaneously:
• Date and time
• Name and grade of persons present
•Events leading up to the need for external pacing
• Any drugs used, e.g. atropine or adrenaline, volume/ dose, and response
• Indication for external pacing
• If patient was conscious, document consent (usually verbal consent only)
• Any sedation used
• When external pacing commenced
• Details of plans for temporary pacing wire insertion
• Sign and bleep/contact details.
0 Comments
