- Published on
Dermatology - Adverse Cutaneous Drug Reaction
Drug-induced rash, also known as adverse cutaneous drug reaction (ACDR), is a condition characterized by a skin rash caused by the use of medication.
Exanthematous drug reactions are the predominant kind of adverse cutaneous drug reactions (ACDR). Specific medications, such as penicillin and related antibiotics, carbamazepine, allopurinol, and gold salts, are highly likely to cause a response. Other substances with a moderate likelihood include sulfonamides (which have bacteriostatic, antidiabetic, and diuretic properties), nonsteroidal anti-inflammatory medications (NSAIDs), hydantoin derivatives, isoniazid, chloramphenicol, erythromycin, and streptomycin. The low likelihood include barbiturates, benzodiazepines, phenothiazines, and tetracyclines.
Sensitization takes place within the period of drug administration, starting from the first day and continuing for three weeks, with the highest occurrence observed on the ninth day. Allergic reactions to penicillin can manifest up to a fortnight after the cessation of the medication. Patients who have previously experienced exanthematous drug eruptions are highly likely to have a similar reaction if they are administered the same drug, and the eruption often occurs 2-3 days following therapy. The rash typically causes intense itching, and the presence of discomfort indicates a more severe reaction. Pyrexia and rigors frequently accompany the condition.
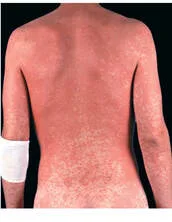
A symmetrical rash manifests on the torso and limbs and may also affect the palms, soles, and oral cavity. The rash exhibits a comparable visual manifestation to viral exanthems, such as measles. Macules and/or papules are small skin lesions ranging from a few millimeters to 1 cm in diameter. They exhibit colors ranging from bright red to tan and purple.
The lesions merge together to create extensive flat areas of skin discoloration, characterized by irregular or circular patterns of redness. Additionally, there may be a network-like pattern of red eruptions, a widespread redness like a sheet, severe redness of the skin, and purple discoloration in the lower thighs. Thrombocytopenic individuals may experience exanthematous eruptions that resemble vasculitis. Scaling and/or desquamation may manifest during the process of healing.
The diagnosis is made based on clinical examination, and the differential diagnosis encompasses all types of skin rashes, including those caused by viral infections, secondary syphilis, atypical pityriasis rosea, and early broad allergic contact dermatitis.
The crucial measure is to identify and cease the administration of the drug causing the problem. Administer oral antihistamines to alleviate itching. Topical glucocorticoids with high potency can accelerate the resolution of the eruption. If it is not possible to replace or exclude the problematic medicine, systemic glucocorticoids can be used to treat the ACDR. Patients should have knowledge of their individual drug hypersensitivity and be aware that other drugs in the same category may elicit a similar allergic reaction. It is recommended to wear a medical alert bracelet.
Drug-induced rash, also known as adverse cutaneous drug reaction (ACDR), is a condition characterized by a skin rash caused by the use of medication.
Exanthematous drug reactions are the predominant kind of adverse cutaneous drug reactions (ACDR). Specific medications, such as penicillin and related antibiotics, carbamazepine, allopurinol, and gold salts, are highly likely to cause a response. Other substances with a moderate likelihood include sulfonamides (which have bacteriostatic, antidiabetic, and diuretic properties), nonsteroidal anti-inflammatory medications (NSAIDs), hydantoin derivatives, isoniazid, chloramphenicol, erythromycin, and streptomycin. The low likelihood include barbiturates, benzodiazepines, phenothiazines, and tetracyclines.
Sensitization takes place within the period of drug administration, starting from the first day and continuing for three weeks, with the highest occurrence observed on the ninth day. Allergic reactions to penicillin can manifest up to a fortnight after the cessation of the medication. Patients who have previously experienced exanthematous drug eruptions are highly likely to have a similar reaction if they are administered the same drug, and the eruption often occurs 2-3 days following therapy. The rash typically causes intense itching, and the presence of discomfort indicates a more severe reaction. Pyrexia and rigors frequently accompany the condition.
A symmetrical rash manifests on the torso and limbs and may also affect the palms, soles, and oral cavity. The rash exhibits a comparable visual manifestation to viral exanthems, such as measles. Macules and/or papules are small skin lesions ranging from a few millimeters to 1 cm in diameter. They exhibit colors ranging from bright red to tan and purple.
The lesions merge together to create extensive flat areas of skin discoloration, characterized by irregular or circular patterns of redness. Additionally, there may be a network-like pattern of red eruptions, a widespread redness like a sheet, severe redness of the skin, and purple discoloration in the lower thighs. Thrombocytopenic individuals may experience exanthematous eruptions that resemble vasculitis. Scaling and/or desquamation may manifest during the process of healing.
The diagnosis is made based on clinical examination, and the differential diagnosis encompasses all types of skin rashes, including those caused by viral infections, secondary syphilis, atypical pityriasis rosea, and early broad allergic contact dermatitis.
The crucial measure is to identify and cease the administration of the drug causing the problem. Administer oral antihistamines to alleviate itching. Topical glucocorticoids with high potency can accelerate the resolution of the eruption. If it is not possible to replace or exclude the problematic medicine, systemic glucocorticoids can be used to treat the ACDR. Patients should have knowledge of their individual drug hypersensitivity and be aware that other drugs in the same category may elicit a similar allergic reaction. It is recommended to wear a medical alert bracelet.

0 Comments
