- Published on
Dermatology - Exfoliative Erythroderma Syndrome
Exfoliative erythroderma is a severe and potentially life-threatening response pattern marked by a consistent redness, infiltration, and scaling. Typically found in individuals aged 50 and over, while in youngsters, it commonly arises from atopic dermatitis, pityriasis rubra pilaris, or atopic dermatitis. Males are more frequently impacted than females.
Exfoliative erythroderma is characterized by the presence of fever, malaise, shivering, and widespread lymphadenopathy.
There are two distinct stages, namely acute and chronic, that seamlessly transition into one another. The acute phase can manifest swiftly, typically in response to a medication reaction, cancer, eczema, or psoriasis.
During the initial acute phase, it is still feasible to detect the prior skin condition. The individual is experiencing symptoms such as fever, pruritus, weariness, weakness, anorexia, weight loss, malaise, feeling cold, and chills.
Abnormalities
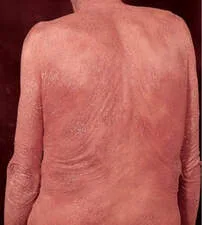
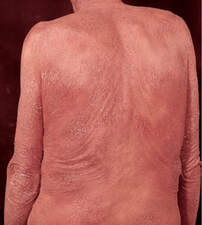
The skin appears red, thickened, and covered with scales. The dermatitis is evenly distributed across the entire body, with the exception of pityriasis rubra pilaris, when distinct regions of unaffected skin are present.
Thickening of the skin results in the formation of prominent skin folds. This can be accompanied by either subtle or more pronounced scaling, ranging from small to big flakes measuring up to 0.5 cm, appearing in layers. In conditions such as pityriasis rubra pilaris, Sézary syndrome, and psoriasis, the palms and soles are typically affected, exhibiting significant thickening of the skin and the presence of deep cracks. Scalp and body hair may be lost, and the nails may grow thicker and detached from the nail bed (a condition known as onycholysis). Hyperpigmentation or hypopigmentation may occur, particularly in people with darker skin.Diagnosing the condition is challenging, and the previous history of the skin disorder may be the sole indication.
Despite undergoing treatment, patients may die from infections or, if they have cardiac issues, from cardiac failure (specifically "high-output" failure), or from the consequences of extended glucocorticoid therapy.
The patient should be admitted to a private room in the hospital, maintaining a warm environment, and receiving topical water baths infused with bath oils. This should be followed by the use of mild moisturizers. Systemic oral glucocorticoids can bring about a state of remission, but they should not be employed for long-term maintenance. Administer appropriate supportive care and administer systemic and topical medication as needed for the underlying problem.
0 Comments
