- Published on
Dermatology - Seborrheic Keratosis
Benign epithelial tumors most commonly occur from seborrheic keratosis. The onset of lesions is delayed until age thirty and is inherited. Over the course of a lifetime, they continue to develop, ranging in size from a few dispersed lesions to literally hundreds in certain extremely old patients.
Lesions can vary in size from tiny, hardly noticeable papules to plaques that have a warty surface and seem to be "stuck on." The lesions are rarely itchy. If they have secondary infections, they become painful.
Damage
Little, scarcely elevated papules, measuring 1 to 3 mm, develop into bigger plaques, either with or without pigment.
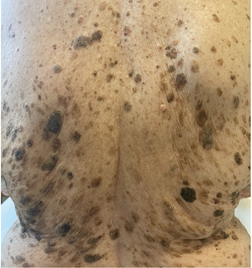
The surface feels oily, the edge is strongly marginated, and fine stippling, resembling a thimble's surface, is frequently visible with a hand lens. By using liquid nitrogen to gently freeze the lesion, elevation can be seen. Late plaques appear "greasy" or "stuck on" and have a warty surface. Horn cysts are frequently visible using a hand lens; however, they are always visible and diagnostic through dermoscopy. These are flat, round, oval, brown, gray, black, or skin-colored nodules that range in size from 1 to 6 cm. Lesions can form on the face, trunk, upper limbs, and in women, usually in the submammary skin folds. They can be localized or widespread. Dermatosis papulosa nigra is the term for a group of tiny, black lesions on the face that appear in people with darker complexion. In sun-exposed areas where dermatoheliosis is present, seborrheic keratoses are most prevalent. They have the potential to congregate when numerous and dense.
In a clinical setting, diagnosis is made with ease. Make sure squamous cell carcinoma is not the cause. Malignant melanoma, pigmented basal cell carcinoma (BCC), squamous cell carcinoma, solar lentigo or spreading pigmented actinic keratosis, and verruca vulgaris (differentiated by the presence of thrombosed capillaries in verrucae) are among the conditions included in the differential.
Treatment is not necessary for benign lesions, unless they are for aesthetic purposes. It is possible to simply rub off the entire lesion with light electrocautery. To stop recurrence, the base can then be gently cauterized. However, this makes histopathologic verification of the diagnosis impossible and should only be carried out by a qualified diagnostician. Liquid nitrogen spray cryosurgery is only effective on flat lesions, and recurrences may be more common.
The optimum method is curettage with cryospray after a brief freezing period, which enables histopathologic analysis.
Benign epithelial tumors most commonly occur from seborrheic keratosis. The onset of lesions is delayed until age thirty and is inherited. Over the course of a lifetime, they continue to develop, ranging in size from a few dispersed lesions to literally hundreds in certain extremely old patients.
Lesions can vary in size from tiny, hardly noticeable papules to plaques that have a warty surface and seem to be "stuck on." The lesions are rarely itchy. If they have secondary infections, they become painful.
Damage
Little, scarcely elevated papules, measuring 1 to 3 mm, develop into bigger plaques, either with or without pigment.
The surface feels oily, the edge is strongly marginated, and fine stippling, resembling a thimble's surface, is frequently visible with a hand lens. By using liquid nitrogen to gently freeze the lesion, elevation can be seen. Late plaques appear "greasy" or "stuck on" and have a warty surface. Horn cysts are frequently visible using a hand lens; however, they are always visible and diagnostic through dermoscopy. These are flat, round, oval, brown, gray, black, or skin-colored nodules that range in size from 1 to 6 cm. Lesions can form on the face, trunk, upper limbs, and in women, usually in the submammary skin folds. They can be localized or widespread. Dermatosis papulosa nigra is the term for a group of tiny, black lesions on the face that appear in people with darker complexion. In sun-exposed areas where dermatoheliosis is present, seborrheic keratoses are most prevalent. They have the potential to congregate when numerous and dense.
In a clinical setting, diagnosis is made with ease. Make sure squamous cell carcinoma is not the cause. Malignant melanoma, pigmented basal cell carcinoma (BCC), squamous cell carcinoma, solar lentigo or spreading pigmented actinic keratosis, and verruca vulgaris (differentiated by the presence of thrombosed capillaries in verrucae) are among the conditions included in the differential.
Treatment is not necessary for benign lesions, unless they are for aesthetic purposes. It is possible to simply rub off the entire lesion with light electrocautery. To stop recurrence, the base can then be gently cauterized. However, this makes histopathologic verification of the diagnosis impossible and should only be carried out by a qualified diagnostician. Liquid nitrogen spray cryosurgery is only effective on flat lesions, and recurrences may be more common.
The optimum method is curettage with cryospray after a brief freezing period, which enables histopathologic analysis.

0 Comments
