- Published on
Dermatology - Systemic Lupus Erythematosus
A dangerous multisystem autoimmune illness that affects blood vessels and connective tissue is systemic lupus erythematosus. It is more common among people of African heritage and is nine times more common in women than in men. Family history and UV exposure are two of the triggering factors, and the onset occurs in the third or fourth decade.
Abdominal discomfort, CNS symptoms, and arthralgia or arthritis are associated with fatigue, fever, weight loss, and malaise.
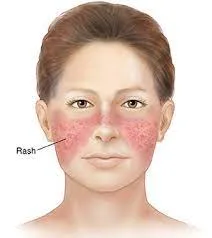
Lesions are itchy or burning and can last for weeks (acute) or months (chronic). A butterfly rash with fine scaling, confluent, strongly defined erosions (acute flares), and crusts develops on the malar areas of the face during the subacute and acute phases of the disease. Similar to psoriasis, there are sharply defined psoriasiform papulosquamous lesions in light-exposed areas during the subacute phase. These lesions have delicate scaling and evolve into bright red confluent plaques that can be oval, arciform, or polycyclic. Annular bright red lesions with little scaling and central regression also occur during this phase. Both may have telangiectasia, but there is minimal induration and no follicular plugging. Lesions heal with hypopigmentation and mild atrophy (no scarring). In the chronic phase, lesions begin as bright red papules that develop into plaques with sharp margins, adhesive scales that are challenging to remove, and undersurface spines that resemble carpet tacks. Round, circular, annular, or polycyclic plaques have uneven borders, grow on the periphery and recede in the middle, leaving scars and atrophy behind. In addition to being pink or white macules and scars, "burned out" lesions can also be hyperpigmented, particularly in those with brown or black skin.
Within the parameters of the updated American Rheumatism Association (ARA) criteria, the diagnosis is made based on clinical symptoms, histology, lupus band test, and serology.
Encourage rest and avoiding the sun. Give immunosuppressants and/or prednisone (60 mg/day in divided doses) if there is severe sickness, hemolytic crisis, thrombocytopenia, or involvement of the CNS or kidneys. Although it helps treat skin lesions in both subacute and chronic SLE, hydroxychloroquine does not lessen the need for prednisone. Take cautious when using hydroxychloroquine. Quinacrines and chloroquine are substitutes.
A dangerous multisystem autoimmune illness that affects blood vessels and connective tissue is systemic lupus erythematosus. It is more common among people of African heritage and is nine times more common in women than in men. Family history and UV exposure are two of the triggering factors, and the onset occurs in the third or fourth decade.
Abdominal discomfort, CNS symptoms, and arthralgia or arthritis are associated with fatigue, fever, weight loss, and malaise.
Lesions are itchy or burning and can last for weeks (acute) or months (chronic). A butterfly rash with fine scaling, confluent, strongly defined erosions (acute flares), and crusts develops on the malar areas of the face during the subacute and acute phases of the disease. Similar to psoriasis, there are sharply defined psoriasiform papulosquamous lesions in light-exposed areas during the subacute phase. These lesions have delicate scaling and evolve into bright red confluent plaques that can be oval, arciform, or polycyclic. Annular bright red lesions with little scaling and central regression also occur during this phase. Both may have telangiectasia, but there is minimal induration and no follicular plugging. Lesions heal with hypopigmentation and mild atrophy (no scarring). In the chronic phase, lesions begin as bright red papules that develop into plaques with sharp margins, adhesive scales that are challenging to remove, and undersurface spines that resemble carpet tacks. Round, circular, annular, or polycyclic plaques have uneven borders, grow on the periphery and recede in the middle, leaving scars and atrophy behind. In addition to being pink or white macules and scars, "burned out" lesions can also be hyperpigmented, particularly in those with brown or black skin.
Within the parameters of the updated American Rheumatism Association (ARA) criteria, the diagnosis is made based on clinical symptoms, histology, lupus band test, and serology.
Encourage rest and avoiding the sun. Give immunosuppressants and/or prednisone (60 mg/day in divided doses) if there is severe sickness, hemolytic crisis, thrombocytopenia, or involvement of the CNS or kidneys. Although it helps treat skin lesions in both subacute and chronic SLE, hydroxychloroquine does not lessen the need for prednisone. Take cautious when using hydroxychloroquine. Quinacrines and chloroquine are substitutes.

0 Comments
