- Published on
Kembara Xtra - Medicine - Otitis Media
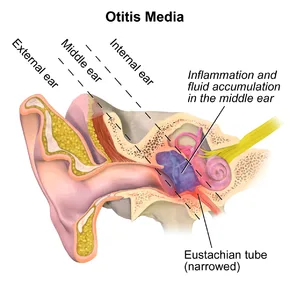
Middle ear inflammation, frequently accompanied with fluid accumulation
Middle ear inflammation is known as acute otitis media (AOM).
Rapid onset; possible infectious causes include viral (AOM-v) or bacterial (AOM-b) infections. This condition is also referred to as suppurative otitis media.
Recurrent AOM: three episodes in six months or four episodes in a year, with one episode occurring in the previous six months.
Otitis medium with effusion (OME) is middle ear fluid without any indication of infection. Serous, secretory, or nonsuppurative otitis media are other names for it.
Recurrent or chronic ear infections, with or without cholesteatoma, are symptoms of chronic otitis media (COM).
Nervous system(s) affected
Epidemiology
AOM prevalence ranges from 6 to 24 months, diminishes beyond 7 years, and is uncommon in adulthood.
By the time they turn three, 50%–85% of kids have experienced at least one episode of AOM; 24% have experienced three or more.
Tympanostomy tube insertion is the second most common surgical operation performed on infants, after circumcision. - OME frequency is higher in the fall and winter. - 90% of children have experienced at least one episode by the age of 4.
Prevalence
More than 5 million cases are identified each year in the United States, making it the most prevalent infection for which antibacterial drugs are prescribed.
Pathophysiology and Etiology
AOM-b (bacterial): Typically, eustachian tube dysfunction brought on by an earlier viral upper respiratory infection (URI) might result in decreased clearance.
- The most common pathogens are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
Less frequently seen mycoplasma species and Streptococcus pyogenes.
AOM-v (viral): Viruses, such as the rhinovirus, respiratory syncytial virus, parainfluenza, influenza, enteroviruses, adenovirus, human metapneumovirus, and bocavirus, are the main cause of 15–44% of AOM infections.
AOM-s: 25–30% (sterile/nonpathogens).
OME: eustachian tube dysfunction and middle ear irritation; allergy reasons are infrequently supported.
Strong hereditary component in twin studies for recurrent and chronic AOM. Immunologic deficiencies and genetic illnesses, such as Down syndrome, might promote alterations in physical architecture, such as more horizontal bones and ear canals, which increase the likelihood of having otitis media.
Age, male gender, race, and ethnicity, bottle-feeding while supine, pacifier use, regular daycare attendance, family history of AOM, environmental smoke exposure, absence of breastfeeding during the first six months of life, low socioeconomic status, atopy, and underlying ENT disease (such as cleft palate, allergic rhinitis) are risk factors for recurrent AOM.
Prevention
The PCV-7 and PCV-13 vaccines have reduced the number of cases of otitis media brought on by streptococcal pneumonia.
Vaccine against influenza
Six months of exclusive breastfeeding is protective.
Steer clear of passive smoking, supine bottle feeding, and pacifiers older than six months.
Secondary prevention: Adenoidectomy and adenotonsillectomy for recurrent AOM are accompanied with their own negative consequences and have little short-term efficacy. AOM can be prevented with xylitol, however because it must be taken five times daily, it is not a feasible prophylactic measure.
Associated Conditions AOM: - Otalgia - URI symptoms that precede or follow
- Reduced hearing Adults with AOM may just experience otalgia, without a fever or unilateral hearing loss.
Alert In the first few months of life, AOM in infants and toddlers may only manifest as irritability.
OME is typically asymptomatic and may only manifest as hearing loss.
clinical assessment
Fever (not necessary for diagnosis): AOM
- Moderate to moderate tympanic membrane bulging; decreased eardrum mobility (with pneumatic otoscopy);
- A tympanic membrane that is red, yellow, or hazy
Otorrhea: - Eardrum is frequently dull but not enlarged
- Lessened motility of the eardrums (pneumatic otoscopy)
Weber test lateralizes to affected ear for an ear with effusion in the presence of air-fluid level.
- Tympanometry in the absence of any evidence from pneumatic otoscopy
Differential diagnosis: Otitis externa, trauma, TMJ in adults, otitis-conjunctivitis syndrome, tympanosclerosis, otitis-conjunctivitis syndrome, and temporal arteritis.
Laboratory Results
Initial examinations (lab, imaging)
Middle ear effusion (MEE) and symptoms of middle ear inflammation on examination are mostly necessary for the clinical diagnosis of AOM. In general, laboratory testing is useless. Although the WBC count in bacterial AOM may be higher than in sterile AOM, this is usually never helpful.
Other/Diagnostic Procedures
Otoscopy—to confirm the presence of fluid in the middle ear
Pneumatic otoscopy, which can be combined with tympanometry and acoustic reflex testing to detect middle ear fluid. Tympanic perforation is a documented contraindication to pneumatic otoscopy.
When hearing loss lasts more than three months or whenever there is a suspicion of a language delay, major hearing loss, or learning difficulties, hearing testing is advised.
Children with hearing impairments should undergo language testing.
If the child appears toxic, is immunocompromised, or has failed prior courses of antibiotic therapy, tympanocentesis for microbiologic diagnosis is indicated; myringotomy may then be performed. Test Interpretation
Tympanic movement will be hampered during pneumatic otoscopy if middle ear fluid is present.
Management: Determine whether there is pain and, if so, suggest a course of action to lessen it.
Reduce all risks to a minimum.
Two-thirds of kids will bounce back without receiving antibiotics.
AOM: For children older than 6 months with moderate acute otitis media, observation with careful waiting is advised. If there is no improvement or a clinical worsening within 24 to 48 hours, prescribe antibiotics.
OME three months of careful observation; if there is no change, consult an ENT for potential surgery.
Steroids, antihistamines, decongestants, and antibiotics are not advised.
First Line of Medicine
There is debate over whether antibiotics are effective in treating this frequently self-resolving illness. When looking at pain alleviation two to three days after starting antibiotics, studies estimate the number needed to treat (NNTB) is 20; the number needed to harm (mainly diarrhea and vomiting) is nine.
The AAP/AAFP advises:
- Care for children under 6 months old: If older than two weeks, treat with amoxicillin.
- >6 months: Antibacterial therapy is advised for people who have bilateral otitis media, otorrhea, or severe otitis media (i.e., moderate to severe otalgia, otalgia >48 hours, or fever 39°C).
● With non-severe otitis media at >6 months to 2 years (otalgia 48 hours, temperature 39°C), observation is an option. Antibiotics are advised since there is a significant probability of treatment failure.
Children >2 who are immune competent can be seen.
Parents and guardians must be aware of the hazards and advantages of observation.
AOM: The AAP/AAFP consensus guideline advises using antibiotics if the following conditions exist: - Between 2 weeks and 6 months OR - >6 months with severe otitis media (e.g., moderate to severe otalgia, otalgia lasting more than 48 hours, or fevers greater than 39°C) - Otorrhea OR - Bilateral otitis media in infants between 6 and 23 months of age without severe signs
In those who are not at risk for developing antibiotic resistance, treat with: - Amoxicillin, 90 mg/kg/day administered in two separate doses (up to 3 g/day) (4).[B]
Treatment lasts 10 days for children under the age of two.
- A 5- to 7-day workshop for toddlers If allergic to penicillin:
- Cefdinir, 1 to 2 doses of 14 mg/kg/day (up to 600 mg/day) for 10 days. Ceftriaxone 50 mg/kg IM/IV per day for 1 to 3 days depending on symptomatic improvement; Cefpodoxime 10 mg/kg/day in 2 divided doses (maximum 400 mg/day); Cefuroxime 30 mg/kg/day in 2 divided doses (maximum 1 g/day);- Azithromycin, 10 mg/kg on day 1 and 5 mg/kg on days 2 through 5 OME: There is no evident advantage to drugs that help 10-15% of patients temporarily resolve their symptoms, but the impact is transient.
Next Line
The following AOM patients are recommended alternative antibiotics:
AOM during a month of amoxicillin medication - Prolonged symptoms after 48 to 72 hours of amoxicillin - Severe earache
- High fever at the age of six months.
- Immunodeficient
Amoxicillin-clavulanate is advised for children who have taken amoxicillin within the last 30 days, as well as those who have concurrent purulent conjunctivitis or a history of AOM that is resistant to amoxicillin. It contains 90 mg/kg/day of amoxicillin and 6.4 mg/kg/day of clavulanate, administered in two separate doses.
Ceftriaxone, 50 mg/kg IM or IV q24h for 2 to 3 straight days can be saved for people who are too ill to take oral drugs or who have tried amoxicillin-clavulanate without result.
When first-line treatments fail, neither erythromycin nor trimethoprim-sulfamethoxazole should be utilized.
Recurrent AOM: Antibiotic prophylaxis is not advised in cases of recurrent AOM (>3 separate, well-documented occurrences in 6 months).
Referral
Follow up with an audiogram if hearing loss persists for more than two weeks after AOM resolution.
If there are more than two occurrences within a six-month period, an ENT referral for a fiberoptic nasopharyngoscopy to rule out malignancy may be appropriate.
Refer to an ENT if COM occurs frequently so that tympanostomy tubes can be considered.
Further Treatments
Acetaminophen, ibuprofen, topical procaine, or lidocaine for children older than 2 years, although these medications shouldn't be taken if there is a tympanic perforation
Surgical Techniques
Recurrent AOM: No clear consensus exists regarding the need for surgery. If there are three or more episodes of well-documented AOM within six months, four episodes within a year with one episode within the previous six months, or if AOM episodes occur while receiving chemotherapy, a referral for surgery may be considered.
Tympanostomy tubes may be helpful for some individuals, especially young children with recurrent AOM under the age of two.
Adenotonsillectomy had a 15% complication risk but only decreased the rate of AOM by 0.7 episodes per kid in the first year following surgery.
COM: Each patient's referral for tympanostomy surgery should be unique. It can be taken into account if there has been bilateral OME for >4 to 6 months, unilateral OME for >6 months, hearing loss of >25 dB, or for high-risk people at any time.
Tympanostomy tubes may only slightly minimize the likelihood of AOM recurrence, but they do not diminish the risk of hearing loss.
Alternative Therapies
Acupuncture, herbal medicine, osteopathy, ear candling, and probiotics all have scant scientific support. Further research is necessary.
Admission
With the exception of febrile infants under 2 months old who require ceftriaxone and who also need to be monitored for 24 hours, outpatient care is appropriate.
Take Action
Patients with otitis media who don't improve in 48–72 hours should get another opinion:
If treatment has already begun, think about switching to a different antibiotic because the benefits of macrolides over amoxicillin against H. influenzae are limited and the majority of oral cephalosporins do not enhance outcomes.
patient observation
AOM: At 1 month, up to 40% of patients may have persistent middle ear effusion, and at 3 months, 10-25%.
OME/COM: If OME persists or if there are warning signs, repeat otoscopic or tympanometric exams at 3 months, as recommended (see earlier discussion).
PROGNOSIS
The majority of mild, nonsevere AOM cases heal without the need for antibiotics.
Complications
AOM: acute mastoiditis, facial nerve paralysis, otitic hydrocephalus, meningitis, labyrinthitis, hearing loss, myringosclerosis, petrositis, brain abscess, epidural or subdural abscess, lateral or cavernous sinus thrombosis, or cholesteatoma.
COM: Speech and language impairments are possible.
OME does not cause hearing loss, but in children at risk for speech, language, or learning issues (such as those with autism spectrum disorders, syndromes, craniofacial disorders, developmental delay, and children already experiencing speech/language delay), a hearing impairment may worsen those issues because these children are less tolerant of it.
Recurrent AOM and COM include cholesteatoma, persistent perforation and otorrhea, atrophy and scarring of the eardrum, chronic mastoiditis, and other intracranial suppurative consequences.
Middle ear inflammation, frequently accompanied with fluid accumulation
Middle ear inflammation is known as acute otitis media (AOM).
Rapid onset; possible infectious causes include viral (AOM-v) or bacterial (AOM-b) infections. This condition is also referred to as suppurative otitis media.
Recurrent AOM: three episodes in six months or four episodes in a year, with one episode occurring in the previous six months.
Otitis medium with effusion (OME) is middle ear fluid without any indication of infection. Serous, secretory, or nonsuppurative otitis media are other names for it.
Recurrent or chronic ear infections, with or without cholesteatoma, are symptoms of chronic otitis media (COM).
Nervous system(s) affected
Epidemiology
AOM prevalence ranges from 6 to 24 months, diminishes beyond 7 years, and is uncommon in adulthood.
By the time they turn three, 50%–85% of kids have experienced at least one episode of AOM; 24% have experienced three or more.
Tympanostomy tube insertion is the second most common surgical operation performed on infants, after circumcision. - OME frequency is higher in the fall and winter. - 90% of children have experienced at least one episode by the age of 4.
Prevalence
More than 5 million cases are identified each year in the United States, making it the most prevalent infection for which antibacterial drugs are prescribed.
Pathophysiology and Etiology
AOM-b (bacterial): Typically, eustachian tube dysfunction brought on by an earlier viral upper respiratory infection (URI) might result in decreased clearance.
- The most common pathogens are Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
Less frequently seen mycoplasma species and Streptococcus pyogenes.
AOM-v (viral): Viruses, such as the rhinovirus, respiratory syncytial virus, parainfluenza, influenza, enteroviruses, adenovirus, human metapneumovirus, and bocavirus, are the main cause of 15–44% of AOM infections.
AOM-s: 25–30% (sterile/nonpathogens).
OME: eustachian tube dysfunction and middle ear irritation; allergy reasons are infrequently supported.
Strong hereditary component in twin studies for recurrent and chronic AOM. Immunologic deficiencies and genetic illnesses, such as Down syndrome, might promote alterations in physical architecture, such as more horizontal bones and ear canals, which increase the likelihood of having otitis media.
Age, male gender, race, and ethnicity, bottle-feeding while supine, pacifier use, regular daycare attendance, family history of AOM, environmental smoke exposure, absence of breastfeeding during the first six months of life, low socioeconomic status, atopy, and underlying ENT disease (such as cleft palate, allergic rhinitis) are risk factors for recurrent AOM.
Prevention
The PCV-7 and PCV-13 vaccines have reduced the number of cases of otitis media brought on by streptococcal pneumonia.
Vaccine against influenza
Six months of exclusive breastfeeding is protective.
Steer clear of passive smoking, supine bottle feeding, and pacifiers older than six months.
Secondary prevention: Adenoidectomy and adenotonsillectomy for recurrent AOM are accompanied with their own negative consequences and have little short-term efficacy. AOM can be prevented with xylitol, however because it must be taken five times daily, it is not a feasible prophylactic measure.
Associated Conditions AOM: - Otalgia - URI symptoms that precede or follow
- Reduced hearing Adults with AOM may just experience otalgia, without a fever or unilateral hearing loss.
Alert In the first few months of life, AOM in infants and toddlers may only manifest as irritability.
OME is typically asymptomatic and may only manifest as hearing loss.
clinical assessment
Fever (not necessary for diagnosis): AOM
- Moderate to moderate tympanic membrane bulging; decreased eardrum mobility (with pneumatic otoscopy);
- A tympanic membrane that is red, yellow, or hazy
Otorrhea: - Eardrum is frequently dull but not enlarged
- Lessened motility of the eardrums (pneumatic otoscopy)
Weber test lateralizes to affected ear for an ear with effusion in the presence of air-fluid level.
- Tympanometry in the absence of any evidence from pneumatic otoscopy
Differential diagnosis: Otitis externa, trauma, TMJ in adults, otitis-conjunctivitis syndrome, tympanosclerosis, otitis-conjunctivitis syndrome, and temporal arteritis.
Laboratory Results
Initial examinations (lab, imaging)
Middle ear effusion (MEE) and symptoms of middle ear inflammation on examination are mostly necessary for the clinical diagnosis of AOM. In general, laboratory testing is useless. Although the WBC count in bacterial AOM may be higher than in sterile AOM, this is usually never helpful.
Other/Diagnostic Procedures
Otoscopy—to confirm the presence of fluid in the middle ear
Pneumatic otoscopy, which can be combined with tympanometry and acoustic reflex testing to detect middle ear fluid. Tympanic perforation is a documented contraindication to pneumatic otoscopy.
When hearing loss lasts more than three months or whenever there is a suspicion of a language delay, major hearing loss, or learning difficulties, hearing testing is advised.
Children with hearing impairments should undergo language testing.
If the child appears toxic, is immunocompromised, or has failed prior courses of antibiotic therapy, tympanocentesis for microbiologic diagnosis is indicated; myringotomy may then be performed. Test Interpretation
Tympanic movement will be hampered during pneumatic otoscopy if middle ear fluid is present.
Management: Determine whether there is pain and, if so, suggest a course of action to lessen it.
Reduce all risks to a minimum.
Two-thirds of kids will bounce back without receiving antibiotics.
AOM: For children older than 6 months with moderate acute otitis media, observation with careful waiting is advised. If there is no improvement or a clinical worsening within 24 to 48 hours, prescribe antibiotics.
OME three months of careful observation; if there is no change, consult an ENT for potential surgery.
Steroids, antihistamines, decongestants, and antibiotics are not advised.
First Line of Medicine
There is debate over whether antibiotics are effective in treating this frequently self-resolving illness. When looking at pain alleviation two to three days after starting antibiotics, studies estimate the number needed to treat (NNTB) is 20; the number needed to harm (mainly diarrhea and vomiting) is nine.
The AAP/AAFP advises:
- Care for children under 6 months old: If older than two weeks, treat with amoxicillin.
- >6 months: Antibacterial therapy is advised for people who have bilateral otitis media, otorrhea, or severe otitis media (i.e., moderate to severe otalgia, otalgia >48 hours, or fever 39°C).
● With non-severe otitis media at >6 months to 2 years (otalgia 48 hours, temperature 39°C), observation is an option. Antibiotics are advised since there is a significant probability of treatment failure.
Children >2 who are immune competent can be seen.
Parents and guardians must be aware of the hazards and advantages of observation.
AOM: The AAP/AAFP consensus guideline advises using antibiotics if the following conditions exist: - Between 2 weeks and 6 months OR - >6 months with severe otitis media (e.g., moderate to severe otalgia, otalgia lasting more than 48 hours, or fevers greater than 39°C) - Otorrhea OR - Bilateral otitis media in infants between 6 and 23 months of age without severe signs
In those who are not at risk for developing antibiotic resistance, treat with: - Amoxicillin, 90 mg/kg/day administered in two separate doses (up to 3 g/day) (4).[B]
Treatment lasts 10 days for children under the age of two.
- A 5- to 7-day workshop for toddlers If allergic to penicillin:
- Cefdinir, 1 to 2 doses of 14 mg/kg/day (up to 600 mg/day) for 10 days. Ceftriaxone 50 mg/kg IM/IV per day for 1 to 3 days depending on symptomatic improvement; Cefpodoxime 10 mg/kg/day in 2 divided doses (maximum 400 mg/day); Cefuroxime 30 mg/kg/day in 2 divided doses (maximum 1 g/day);- Azithromycin, 10 mg/kg on day 1 and 5 mg/kg on days 2 through 5 OME: There is no evident advantage to drugs that help 10-15% of patients temporarily resolve their symptoms, but the impact is transient.
Next Line
The following AOM patients are recommended alternative antibiotics:
AOM during a month of amoxicillin medication - Prolonged symptoms after 48 to 72 hours of amoxicillin - Severe earache
- High fever at the age of six months.
- Immunodeficient
Amoxicillin-clavulanate is advised for children who have taken amoxicillin within the last 30 days, as well as those who have concurrent purulent conjunctivitis or a history of AOM that is resistant to amoxicillin. It contains 90 mg/kg/day of amoxicillin and 6.4 mg/kg/day of clavulanate, administered in two separate doses.
Ceftriaxone, 50 mg/kg IM or IV q24h for 2 to 3 straight days can be saved for people who are too ill to take oral drugs or who have tried amoxicillin-clavulanate without result.
When first-line treatments fail, neither erythromycin nor trimethoprim-sulfamethoxazole should be utilized.
Recurrent AOM: Antibiotic prophylaxis is not advised in cases of recurrent AOM (>3 separate, well-documented occurrences in 6 months).
Referral
Follow up with an audiogram if hearing loss persists for more than two weeks after AOM resolution.
If there are more than two occurrences within a six-month period, an ENT referral for a fiberoptic nasopharyngoscopy to rule out malignancy may be appropriate.
Refer to an ENT if COM occurs frequently so that tympanostomy tubes can be considered.
Further Treatments
Acetaminophen, ibuprofen, topical procaine, or lidocaine for children older than 2 years, although these medications shouldn't be taken if there is a tympanic perforation
Surgical Techniques
Recurrent AOM: No clear consensus exists regarding the need for surgery. If there are three or more episodes of well-documented AOM within six months, four episodes within a year with one episode within the previous six months, or if AOM episodes occur while receiving chemotherapy, a referral for surgery may be considered.
Tympanostomy tubes may be helpful for some individuals, especially young children with recurrent AOM under the age of two.
Adenotonsillectomy had a 15% complication risk but only decreased the rate of AOM by 0.7 episodes per kid in the first year following surgery.
COM: Each patient's referral for tympanostomy surgery should be unique. It can be taken into account if there has been bilateral OME for >4 to 6 months, unilateral OME for >6 months, hearing loss of >25 dB, or for high-risk people at any time.
Tympanostomy tubes may only slightly minimize the likelihood of AOM recurrence, but they do not diminish the risk of hearing loss.
Alternative Therapies
Acupuncture, herbal medicine, osteopathy, ear candling, and probiotics all have scant scientific support. Further research is necessary.
Admission
With the exception of febrile infants under 2 months old who require ceftriaxone and who also need to be monitored for 24 hours, outpatient care is appropriate.
Take Action
Patients with otitis media who don't improve in 48–72 hours should get another opinion:
If treatment has already begun, think about switching to a different antibiotic because the benefits of macrolides over amoxicillin against H. influenzae are limited and the majority of oral cephalosporins do not enhance outcomes.
patient observation
AOM: At 1 month, up to 40% of patients may have persistent middle ear effusion, and at 3 months, 10-25%.
OME/COM: If OME persists or if there are warning signs, repeat otoscopic or tympanometric exams at 3 months, as recommended (see earlier discussion).
PROGNOSIS
The majority of mild, nonsevere AOM cases heal without the need for antibiotics.
Complications
AOM: acute mastoiditis, facial nerve paralysis, otitic hydrocephalus, meningitis, labyrinthitis, hearing loss, myringosclerosis, petrositis, brain abscess, epidural or subdural abscess, lateral or cavernous sinus thrombosis, or cholesteatoma.
COM: Speech and language impairments are possible.
OME does not cause hearing loss, but in children at risk for speech, language, or learning issues (such as those with autism spectrum disorders, syndromes, craniofacial disorders, developmental delay, and children already experiencing speech/language delay), a hearing impairment may worsen those issues because these children are less tolerant of it.
Recurrent AOM and COM include cholesteatoma, persistent perforation and otorrhea, atrophy and scarring of the eardrum, chronic mastoiditis, and other intracranial suppurative consequences.

0 Comments
