- Published on
Pathology - Acute and Chronic Pyelonephritis
Acute renal parenchymal infection is more common in women.
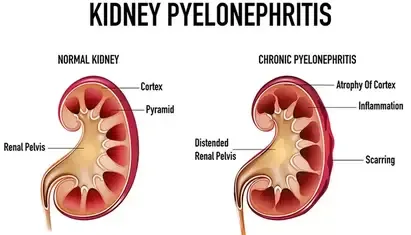
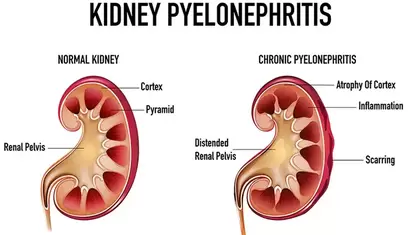
Chronic: Arises from persistent urinary tract blockage and repeated UTIs.
Study of diseases
Acute renal cortex involvement with neutrophilic infiltration and abscess formation in the interstitium, with potential rupture of abscesses leading to the presence of white blood cells in the tubular lumen, whereas glomeruli are unaffected.
Chronic kidney damage characterized by uneven scarring between the cortex and medulla, with tubules filled with protein-rich casts that give the kidneys a thyroid-like look. This condition progresses to tubular shrinkage and fibrosis in advanced stages.
Clinical presentation of acute pyelonephritis includes fever, flank pain with costovertebral angle tenderness, increased urination and painful urination, as well as symptoms of nausea, vomiting, and diarrhea.
Chronic episodes of acute pyelonephritis can cause renal hypertension and end-stage renal disease (ESRD).
Laboratory results indicate the presence of white blood cells and/or white blood cell casts in the urine.
Treatment for acute conditions includes antibiotics and intravenous fluids.
Chronic renal transplant is indicated for patients who have end-stage renal disease (ESRD).
Renal papillary necrosis is a consequence of acute pyelonephritis that occurs in individuals with diabetes or those who use phenacetin chronically. It is identified by ischemic necrosis at the tips of the renal papillae.
Diffuse cortical necrosis is a sudden widespread death of renal cortices, typically caused by a combination of disseminated intravascular coagulation (DIC) and end-organ vasospasm in connection with obstetric emergencies or septic shock. The medulla is normally unaffected.
Acute renal parenchymal infection is more common in women.
Chronic: Arises from persistent urinary tract blockage and repeated UTIs.
Study of diseases
Acute renal cortex involvement with neutrophilic infiltration and abscess formation in the interstitium, with potential rupture of abscesses leading to the presence of white blood cells in the tubular lumen, whereas glomeruli are unaffected.
Chronic kidney damage characterized by uneven scarring between the cortex and medulla, with tubules filled with protein-rich casts that give the kidneys a thyroid-like look. This condition progresses to tubular shrinkage and fibrosis in advanced stages.
Clinical presentation of acute pyelonephritis includes fever, flank pain with costovertebral angle tenderness, increased urination and painful urination, as well as symptoms of nausea, vomiting, and diarrhea.
Chronic episodes of acute pyelonephritis can cause renal hypertension and end-stage renal disease (ESRD).
Laboratory results indicate the presence of white blood cells and/or white blood cell casts in the urine.
Treatment for acute conditions includes antibiotics and intravenous fluids.
Chronic renal transplant is indicated for patients who have end-stage renal disease (ESRD).
Renal papillary necrosis is a consequence of acute pyelonephritis that occurs in individuals with diabetes or those who use phenacetin chronically. It is identified by ischemic necrosis at the tips of the renal papillae.
Diffuse cortical necrosis is a sudden widespread death of renal cortices, typically caused by a combination of disseminated intravascular coagulation (DIC) and end-organ vasospasm in connection with obstetric emergencies or septic shock. The medulla is normally unaffected.
0 Comments
