- Published on
Pathology - Cushing Syndrome
Hypercortisolism can be caused by iatrogenic cortisol injection, increased ACTH production by pituitary adenoma/hyperplasia (Cushing disease), adrenal cortical adenoma/carcinoma, or ectopic ACTH-secreting tumors (typically small cell bronchogenic carcinoma).
The pathophysiology of the adrenal gland is determined by its underlying cause. (1) Iatrogenic: Adrenocortical atrophy caused by medical treatment; (2) ACTH overproduction: Enlargement of lipid-rich cells in the zona fasciculata of both adrenal glands; (3) Adrenal adenoma: Small enclosed growth made up of uniform zona fasciculata cells; (4) Pituitary hyperplasia or adenoma (observed in Cushing disease): Accumulation of basophilic cells.
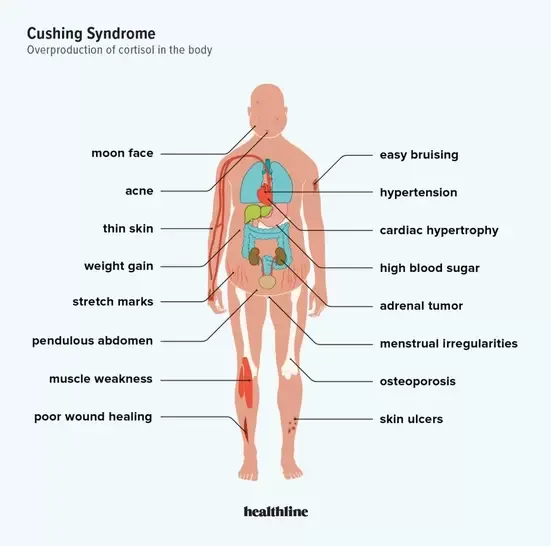
Clinical Symptoms and Signs
Truncal obesity, hypertension, moon facies, buffalo hump, muscular wasting, hyperglycemia from insulin resistance, skin alterations such purple abdomen striae and bruises, osteoporosis, hirsutism, mental state changes, immunological suppression, and central obesity.
Laboratory results: Elevated cortisol levels, atypical ACTH levels (lower in cases of iatrogenic and adrenal adenoma, higher in pituitary adenoma and ectopic ACTH secretion), hyperglycemia.
Clinical manifestations
Surgical removal of pituitary or adrenal adenoma, or ectopic ACTH-secreting tumors.
Therapies
The dexamethasone suppression test is utilized to identify the cause of Cushing's illness.
High doses of dexamethasone decrease cortisol levels in Cushing's disease from pituitary adenomas but do not modify levels in cases caused by ectopic ACTH-secreting tumors.
Hypercortisolism can be caused by iatrogenic cortisol injection, increased ACTH production by pituitary adenoma/hyperplasia (Cushing disease), adrenal cortical adenoma/carcinoma, or ectopic ACTH-secreting tumors (typically small cell bronchogenic carcinoma).
The pathophysiology of the adrenal gland is determined by its underlying cause. (1) Iatrogenic: Adrenocortical atrophy caused by medical treatment; (2) ACTH overproduction: Enlargement of lipid-rich cells in the zona fasciculata of both adrenal glands; (3) Adrenal adenoma: Small enclosed growth made up of uniform zona fasciculata cells; (4) Pituitary hyperplasia or adenoma (observed in Cushing disease): Accumulation of basophilic cells.
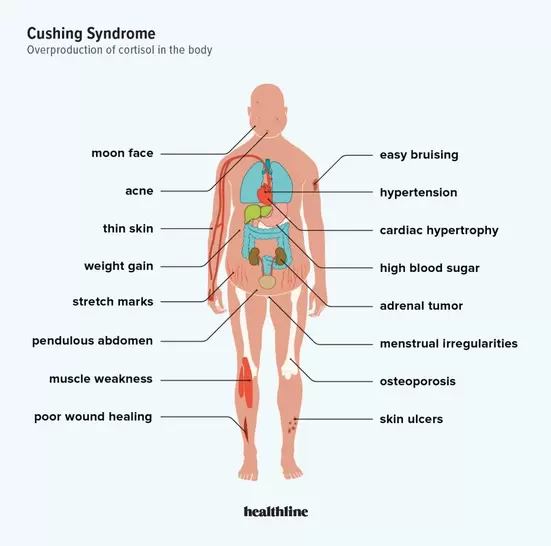
Clinical Symptoms and Signs
Truncal obesity, hypertension, moon facies, buffalo hump, muscular wasting, hyperglycemia from insulin resistance, skin alterations such purple abdomen striae and bruises, osteoporosis, hirsutism, mental state changes, immunological suppression, and central obesity.
Laboratory results: Elevated cortisol levels, atypical ACTH levels (lower in cases of iatrogenic and adrenal adenoma, higher in pituitary adenoma and ectopic ACTH secretion), hyperglycemia.
Clinical manifestations
Surgical removal of pituitary or adrenal adenoma, or ectopic ACTH-secreting tumors.
Therapies
The dexamethasone suppression test is utilized to identify the cause of Cushing's illness.
High doses of dexamethasone decrease cortisol levels in Cushing's disease from pituitary adenomas but do not modify levels in cases caused by ectopic ACTH-secreting tumors.
0 Comments
