- Published on
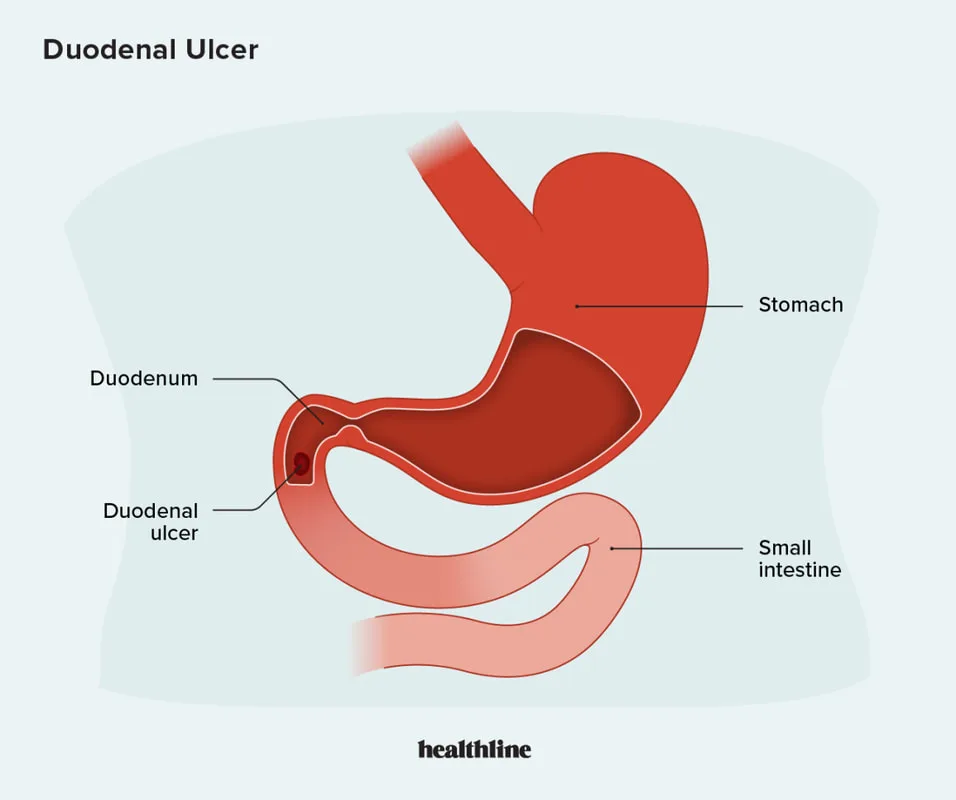
Pathology - Duodenal Ulcer
Pathophysiology
An imbalance between protective and aggressive elements might lead to mucosal abnormalities in the small intestine or stomach. The surface mucous barrier, surface cell bicarbonate secretion, and increased mucosal blood flow are significant protective benefits that are bolstered by local prostaglandin synthesis. The most frequent aggressive variables are NSAID use and H. pylori infection.
Another risk factor is smoking. Life-threatening GI bleeding, such as bleeding from a posterior ulceration into the gastroduodenal artery or peritonitis from a GI wall perforation, are examples of complications. This patient most likely has a duodenal ulcer, which, unlike gastric ulcers, is more common in younger people and is frequently eased by eating. Due to its ability to cause chronic mucosal inflammation, H. pylori infection is a major pathogenic factor in up to 90% of duodenal ulcers. Microcytic erythrocytes and blood in the stool are signs of chronic gastrointestinal bleeding in this patient, who also has iron-deficiency anemia. The goal of treatment is to get rid of aggravating factors (such H. pylori and stop taking NSAIDs) and utilize PPIs or H2 blockers to lessen acidity. The best way to diagnose and assess the severity of an ulcer, as well as to treat severe ulcers and perforations with sclerotherapy, is by endoscopy. Unlike stomach ulcers, which have a 5% to 10% chance of being malignant, duodenal ulcers never need to be biopsyed.
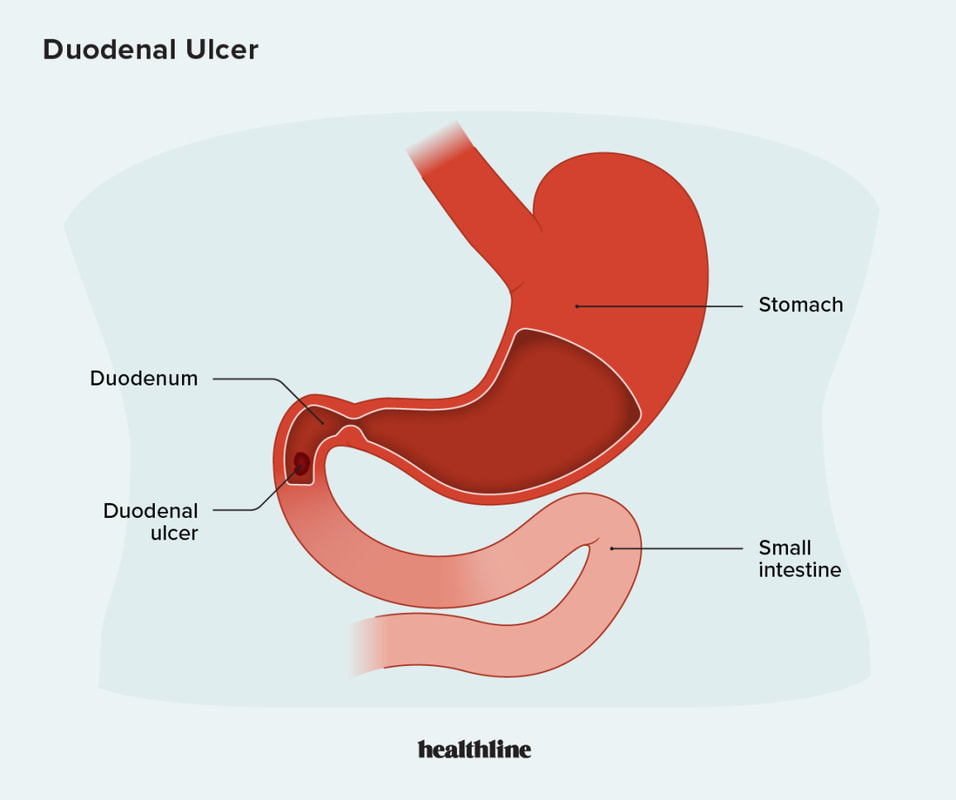
Pathophysiology
An imbalance between protective and aggressive elements might lead to mucosal abnormalities in the small intestine or stomach. The surface mucous barrier, surface cell bicarbonate secretion, and increased mucosal blood flow are significant protective benefits that are bolstered by local prostaglandin synthesis. The most frequent aggressive variables are NSAID use and H. pylori infection.
Another risk factor is smoking. Life-threatening GI bleeding, such as bleeding from a posterior ulceration into the gastroduodenal artery or peritonitis from a GI wall perforation, are examples of complications. This patient most likely has a duodenal ulcer, which, unlike gastric ulcers, is more common in younger people and is frequently eased by eating. Due to its ability to cause chronic mucosal inflammation, H. pylori infection is a major pathogenic factor in up to 90% of duodenal ulcers. Microcytic erythrocytes and blood in the stool are signs of chronic gastrointestinal bleeding in this patient, who also has iron-deficiency anemia. The goal of treatment is to get rid of aggravating factors (such H. pylori and stop taking NSAIDs) and utilize PPIs or H2 blockers to lessen acidity. The best way to diagnose and assess the severity of an ulcer, as well as to treat severe ulcers and perforations with sclerotherapy, is by endoscopy. Unlike stomach ulcers, which have a 5% to 10% chance of being malignant, duodenal ulcers never need to be biopsyed.
0 Comments
