- Published on
Pathology - Dysplasia, Carcinoma in Situ, and Squamous Cell Carcinoma of the Cervix
Linked to HPV types 16, 18, 31, and 33, early sexual debut, multiple sexual partners, HIV infection, and smoking.
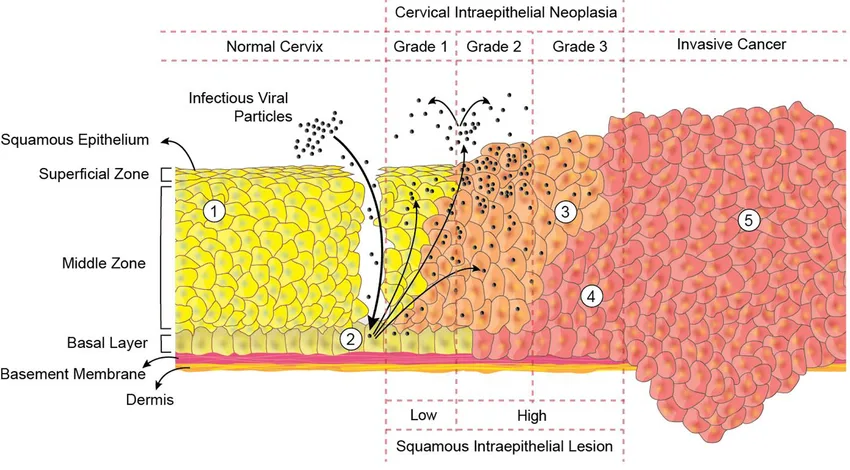
Cervical dysplasia (CD): Concerns the squamocolumnar junction; identified by cells with hyperchromatic nuclei, irregular nuclear shapes, and minimal cytoplasm; epithelial proliferation starts at the basal layer and spreads outward; categorized as cervical intraepithelial neoplasia (CIN) grades I-III; CIN I displays abnormal undifferentiated cells solely in the lower third of the epithelium, while CIN III exhibits atypical cells throughout more than two-thirds of the epithelium.
Cervical carcinoma in situ (CIS) is characterized by dysplastic cells that spread over the whole epithelium but do not invade the basement membrane.
Symptoms and signs
Cervical cancer that has invaded surrounding tissues/ invasive cervical carcinoma (ICC). Gross: may present as exophytic, ulcerating, or infiltrating mass.
The microscopic findings typically show squamous cell carcinoma (SCC) with big cells and keratinization. It can also present as adenocarcinoma or undifferentiated carcinoma. The cancer originates from preexisting cervical intraepithelial neoplasia (CIN) at the squamocolumnar junction. Non-neoplastic epithelial cells generally exhibit koilocytosis, which is linked to HPV infection.
Therapies
Clinical ICC symptoms include irregular vaginal bleeding, postcoital spotting, pelvic pain, cervical ulceration and discharge, dysuria, and potential ureter obstruction causing renal failure.
Treatment: For CIN I, consider either expectant management or excision as 75% regress spontaneously. Treat CIN II-III by excision.
ICC: Hysterectomy, chemotherapy, and radiation for treatment; HPV vaccine for prevention.
Linked to HPV types 16, 18, 31, and 33, early sexual debut, multiple sexual partners, HIV infection, and smoking.
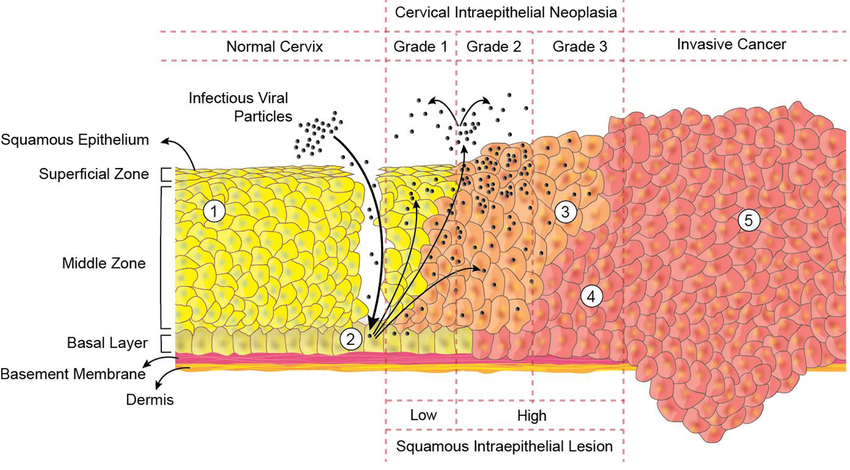
Cervical dysplasia (CD): Concerns the squamocolumnar junction; identified by cells with hyperchromatic nuclei, irregular nuclear shapes, and minimal cytoplasm; epithelial proliferation starts at the basal layer and spreads outward; categorized as cervical intraepithelial neoplasia (CIN) grades I-III; CIN I displays abnormal undifferentiated cells solely in the lower third of the epithelium, while CIN III exhibits atypical cells throughout more than two-thirds of the epithelium.
Cervical carcinoma in situ (CIS) is characterized by dysplastic cells that spread over the whole epithelium but do not invade the basement membrane.
Symptoms and signs
Cervical cancer that has invaded surrounding tissues/ invasive cervical carcinoma (ICC). Gross: may present as exophytic, ulcerating, or infiltrating mass.
The microscopic findings typically show squamous cell carcinoma (SCC) with big cells and keratinization. It can also present as adenocarcinoma or undifferentiated carcinoma. The cancer originates from preexisting cervical intraepithelial neoplasia (CIN) at the squamocolumnar junction. Non-neoplastic epithelial cells generally exhibit koilocytosis, which is linked to HPV infection.
Therapies
Clinical ICC symptoms include irregular vaginal bleeding, postcoital spotting, pelvic pain, cervical ulceration and discharge, dysuria, and potential ureter obstruction causing renal failure.
Treatment: For CIN I, consider either expectant management or excision as 75% regress spontaneously. Treat CIN II-III by excision.
ICC: Hysterectomy, chemotherapy, and radiation for treatment; HPV vaccine for prevention.
0 Comments
