- Published on
Pathology - Folate-Deficiency Anemia
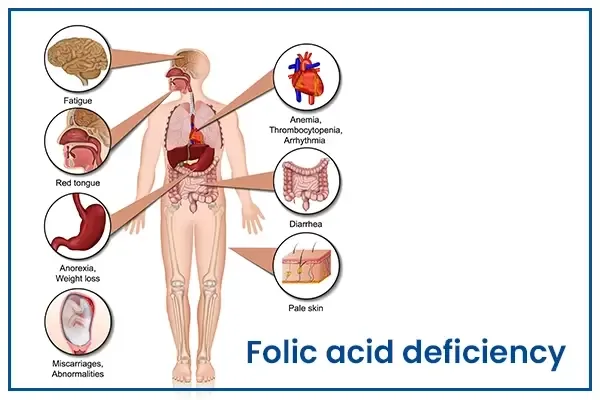
Folate-deficiency anemia is the most usually caused by a decreased dietary intake of folate, but can also come from malabsorptive disorders, increased folate usage, and some medicines (5-fluorouracil, methotrexate, trimethoprim-sulfa, phenytoin). Both folate and B12 are involved in the production of deoxythymidine monophosphate. Without production of the nucleic acid thymine, DNA synthesis is impaired, resulting in persistent cell proliferation without division, producing macrocytosis. Thus, RBCs are larger than normal (high MCV) and neutrophils have an increased number of nuclear lobes (hypersegmented neutrophils). Populations at risk for folate-deficiency anemia include those with diets lacking in green vegetables and animal protein, including indigent, elderly (tea and toast diet), and alcoholic patients in particular.
Alcohol also hinders the release of folate from the liver, further contributing to the shortfall. Symptoms include those of anemia including fatigue, weakness, headaches, and irritability as well as aphthous ulcers, poor growth, and a swollen tongue. This patient likely has not eaten adequately since the death of his wife. Folate stores normally only last 2 to 3 months. Other indications of self-neglect include absence of appropriate medical care for hypertension and indicators of dehydration (dry mucous membranes and delayed capillary refill).
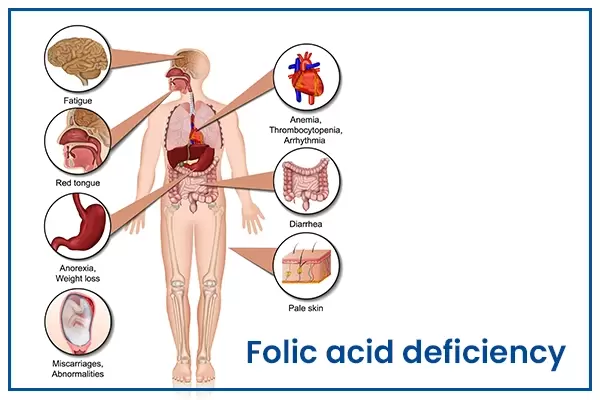
Folate-deficiency anemia is the most usually caused by a decreased dietary intake of folate, but can also come from malabsorptive disorders, increased folate usage, and some medicines (5-fluorouracil, methotrexate, trimethoprim-sulfa, phenytoin). Both folate and B12 are involved in the production of deoxythymidine monophosphate. Without production of the nucleic acid thymine, DNA synthesis is impaired, resulting in persistent cell proliferation without division, producing macrocytosis. Thus, RBCs are larger than normal (high MCV) and neutrophils have an increased number of nuclear lobes (hypersegmented neutrophils). Populations at risk for folate-deficiency anemia include those with diets lacking in green vegetables and animal protein, including indigent, elderly (tea and toast diet), and alcoholic patients in particular.
Alcohol also hinders the release of folate from the liver, further contributing to the shortfall. Symptoms include those of anemia including fatigue, weakness, headaches, and irritability as well as aphthous ulcers, poor growth, and a swollen tongue. This patient likely has not eaten adequately since the death of his wife. Folate stores normally only last 2 to 3 months. Other indications of self-neglect include absence of appropriate medical care for hypertension and indicators of dehydration (dry mucous membranes and delayed capillary refill).
0 Comments
