- Published on
Pathology - Hepatorenal Syndrome
Pathophysiology
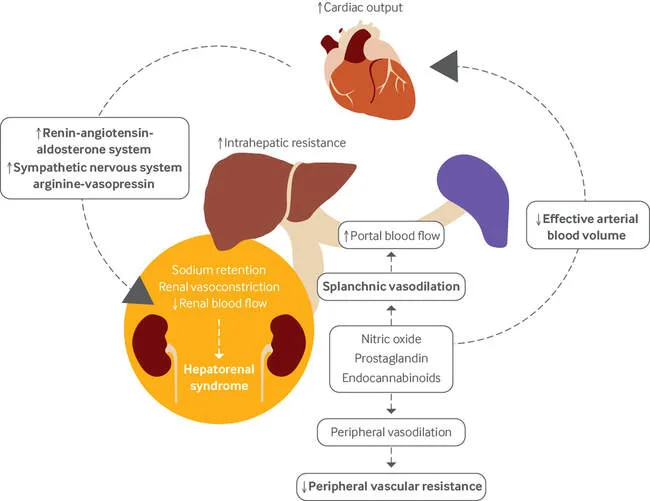
Arterial underfilling lowers renal perfusion pressure, which compromises renal function. Renal blood flow and glomerular filtration are reduced when renal vasoconstriction and renal blood flow occur together. Because of elevated amounts of vasodilators such nitric oxide, liver cirrhosis results in broad systemic vasodilation and blood pooling in the splanchnic circulation. Reduced diastolic blood pressure results in hyperdynamic circulation, tachycardia, and a broad pulse pressure (also observe the systolic flow murmur). Vasopressin secretion and the renin-angiotensin-aldosterone axis are stimulated by a decrease in the effective circulation volume. Renal vasoconstriction and sodium retention (urinary Na <10 mEq/L) follow as a result. Renal sympathetic efferent nerves and hepatic afferent nerves are also activated, causing a hepatorenal reflex that intensifies renal vasoconstriction.
Peritonitis, GI hemorrhage, over-diuresis, or, in this case, large-volume paracentesis are examples of second insults to the circulation that frequently set off the hepatorenal syndrome's progressive and fatal renal failure. Other organic kidney diseases must be ruled out in order to make a diagnosis (notice the normal renal ultrasonography and inactive renal sediment). The only long-term, effective treatment is a liver transplant, and the prognosis is quite bad.
Pathophysiology
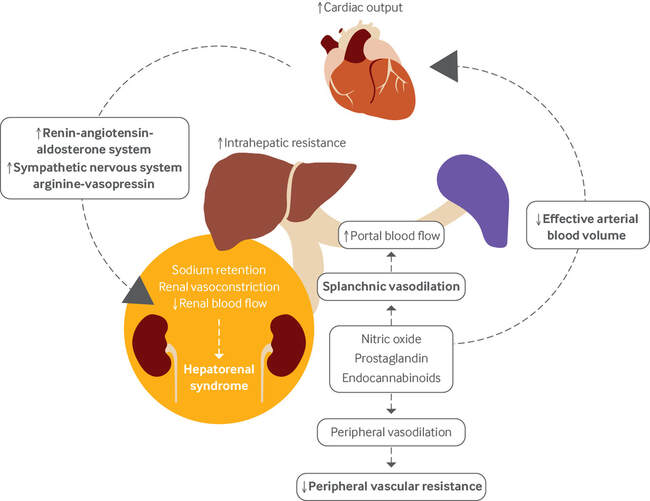
Arterial underfilling lowers renal perfusion pressure, which compromises renal function. Renal blood flow and glomerular filtration are reduced when renal vasoconstriction and renal blood flow occur together. Because of elevated amounts of vasodilators such nitric oxide, liver cirrhosis results in broad systemic vasodilation and blood pooling in the splanchnic circulation. Reduced diastolic blood pressure results in hyperdynamic circulation, tachycardia, and a broad pulse pressure (also observe the systolic flow murmur). Vasopressin secretion and the renin-angiotensin-aldosterone axis are stimulated by a decrease in the effective circulation volume. Renal vasoconstriction and sodium retention (urinary Na <10 mEq/L) follow as a result. Renal sympathetic efferent nerves and hepatic afferent nerves are also activated, causing a hepatorenal reflex that intensifies renal vasoconstriction.
Peritonitis, GI hemorrhage, over-diuresis, or, in this case, large-volume paracentesis are examples of second insults to the circulation that frequently set off the hepatorenal syndrome's progressive and fatal renal failure. Other organic kidney diseases must be ruled out in order to make a diagnosis (notice the normal renal ultrasonography and inactive renal sediment). The only long-term, effective treatment is a liver transplant, and the prognosis is quite bad.
0 Comments
