- Published on
Pathology - Hypovolemic Shock
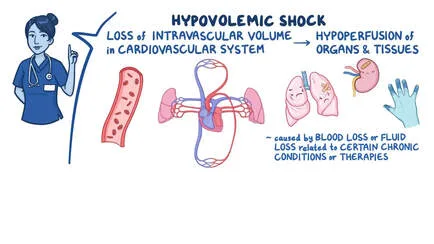
Pathophysiology
When there is not enough vascular volume to give tissues and organs perfusion, this kind of shock happens. When blood is moved preferentially to internal organs, there are physical signs of diminished peripheral perfusion, such as a weak pulse and chilly skin.
This kind of shock frequently happens in situations involving severe injuries where a significant volume of blood is lost quickly.
Large volumes of lactic acid are produced as a result of enhanced anaerobic glycolysis brought on by inadequate tissue perfusion. This lactic acidosis can reduce peripheral vascular reactivity to catecholamines and impair cardiac function.
Reduced pulse pressure is one of the body's compensatory responses, which causes widespread vasoconstriction. Vital blood pressure is maintained by the tachycardia's early cardiac reaction. Bradycardia may occur in cases of severe hypovolemia in order to reduce blood loss. Vasoconstriction lowers glomerular filtration in the kidney, but if hypotension persists for an extended period of time, it can cause acute tubular injury and renal failure. Increased levels of the pressor hormones vasopressin, norepinephrine, and angiotensin II are among the hormonal alterations. Angiotensin II and ACTH levels cause an increase in aldosterone, which causes sodium retention and an increase in the volume of the ECF. Vasoactive drugs and intravenous fluid therapy are desperately needed to increase peripheral resistance and vascular volume in order to eventually restore central perfusion.
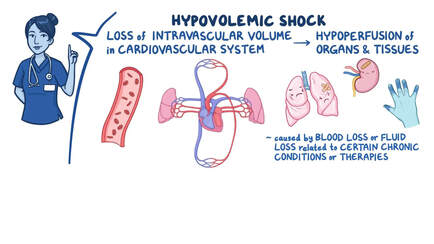
Pathophysiology
When there is not enough vascular volume to give tissues and organs perfusion, this kind of shock happens. When blood is moved preferentially to internal organs, there are physical signs of diminished peripheral perfusion, such as a weak pulse and chilly skin.
This kind of shock frequently happens in situations involving severe injuries where a significant volume of blood is lost quickly.
Large volumes of lactic acid are produced as a result of enhanced anaerobic glycolysis brought on by inadequate tissue perfusion. This lactic acidosis can reduce peripheral vascular reactivity to catecholamines and impair cardiac function.
Reduced pulse pressure is one of the body's compensatory responses, which causes widespread vasoconstriction. Vital blood pressure is maintained by the tachycardia's early cardiac reaction. Bradycardia may occur in cases of severe hypovolemia in order to reduce blood loss. Vasoconstriction lowers glomerular filtration in the kidney, but if hypotension persists for an extended period of time, it can cause acute tubular injury and renal failure. Increased levels of the pressor hormones vasopressin, norepinephrine, and angiotensin II are among the hormonal alterations. Angiotensin II and ACTH levels cause an increase in aldosterone, which causes sodium retention and an increase in the volume of the ECF. Vasoactive drugs and intravenous fluid therapy are desperately needed to increase peripheral resistance and vascular volume in order to eventually restore central perfusion.
0 Comments
