- Published on
Pathology - Jaundice
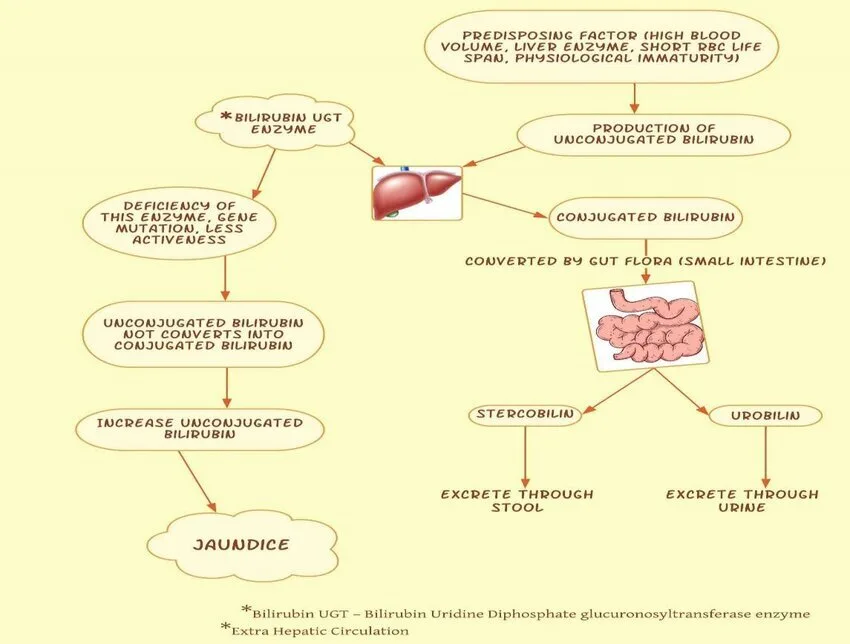
Resulting from hepatic illness, biliary blockage, hemolytic anemia, and congenital hyperbilirubinemias.
Bilirubin is produced by the breakdown of heme. After heme is broken down outside the liver, unconjugated bilirubin binds to albumin and is carried to the liver for further processing. Hepatocytes typically convert bilirubin into conjugated bilirubin and release it into bile. Bile is transformed into urobilinogen by intestinal bacteria in the gastrointestinal system, then reabsorbed and eliminated through urine. Conjugated bilirubin is the only form that is soluble and can be reabsorbed from the intestine.
Pathological mechanisms lead to elevated bilirubin synthesis, reduced hepatic uptake or outflow of bilirubin, inadequate conjugation, or hindered bile flow, resulting in bilirubin buildup. All of these factors result in jaundice.
Jaundice is characterized by yellowing of the skin, sclera, and tissues, as well as black urine.
Laboratory results: It depends on the cause of jaundice. (1) Hepatocellular disease jaundice presents with both conjugated and unconjugated hyperbilirubinemia, elevated urine bilirubin, normal or reduced urine urobilinogen, increased levels of ALT and AST, and elevated ALP. (2) Biliary obstructive jaundice is characterized by conjugated hyperbilirubinemia, increased urine bilirubin, decreased urine urobilinogen, elevated ALP, and hypercholesterolemia. (3) Hemolytic anemia jaundice is identified by unconjugated hyperbilirubinemia and the absence of urine bilirubin (acholuria). elevated urinary urobilinogen levels.
Treat the underlying cause.
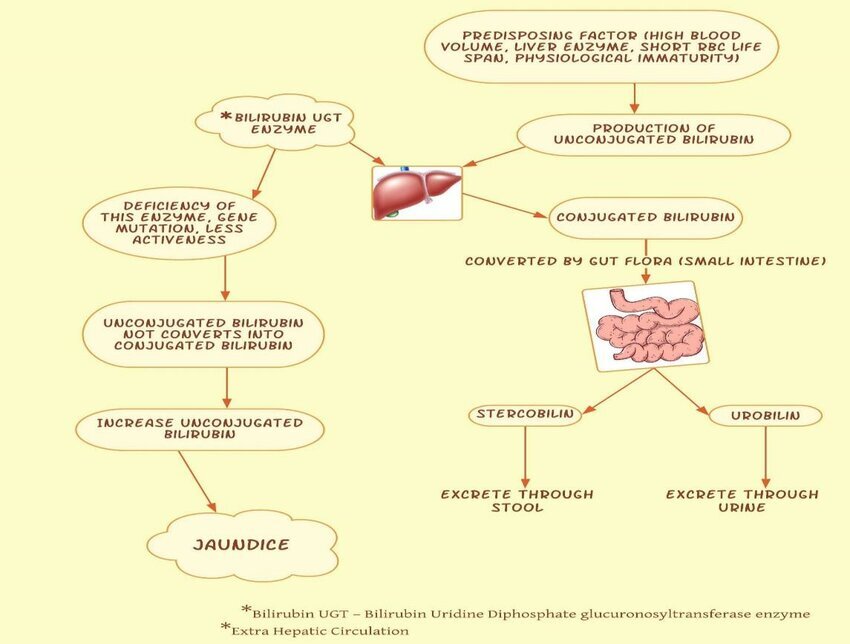
Resulting from hepatic illness, biliary blockage, hemolytic anemia, and congenital hyperbilirubinemias.
Bilirubin is produced by the breakdown of heme. After heme is broken down outside the liver, unconjugated bilirubin binds to albumin and is carried to the liver for further processing. Hepatocytes typically convert bilirubin into conjugated bilirubin and release it into bile. Bile is transformed into urobilinogen by intestinal bacteria in the gastrointestinal system, then reabsorbed and eliminated through urine. Conjugated bilirubin is the only form that is soluble and can be reabsorbed from the intestine.
Pathological mechanisms lead to elevated bilirubin synthesis, reduced hepatic uptake or outflow of bilirubin, inadequate conjugation, or hindered bile flow, resulting in bilirubin buildup. All of these factors result in jaundice.
Jaundice is characterized by yellowing of the skin, sclera, and tissues, as well as black urine.
Laboratory results: It depends on the cause of jaundice. (1) Hepatocellular disease jaundice presents with both conjugated and unconjugated hyperbilirubinemia, elevated urine bilirubin, normal or reduced urine urobilinogen, increased levels of ALT and AST, and elevated ALP. (2) Biliary obstructive jaundice is characterized by conjugated hyperbilirubinemia, increased urine bilirubin, decreased urine urobilinogen, elevated ALP, and hypercholesterolemia. (3) Hemolytic anemia jaundice is identified by unconjugated hyperbilirubinemia and the absence of urine bilirubin (acholuria). elevated urinary urobilinogen levels.
Treat the underlying cause.

0 Comments
