- Published on
Pathology - Membranous Nephropathy
An immunological complex illness of unclear origin.
Secondary disease observed in 10% of systemic lupus erythematosus (SLE) patients, known as type V lupus nephritis, and is occasionally linked to infections (such as hepatitis B and C, syphilis, malaria), medications (such gold salts, penicillamine, NSAIDs), or solid-organ cancer.
The highest incidence occurs in adulthood.
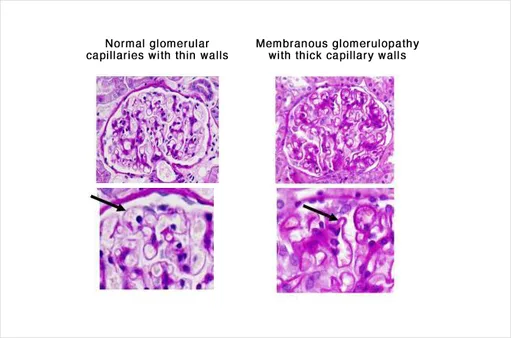
Light microscopy shows diffuse thickening of capillary walls and basement membranes.
Immunofluorescence shows a granular pattern of IgG or C3 deposits, sometimes known as lumpy-bumpy.
Electron microscopy reveals the presence of electron-dense immune complexes deposited in subepithelial areas within the basement membrane of glomerular capillary walls.
The silver methenamine stain shows a spike-and-dome pattern caused by the basement membrane extending between and around the immune deposits. Spikes represent the basement membrane, while domes represent the immune complex deposits.
Clinical presentation of nephrotic syndrome includes edema, proteinuria, anorexia, and commonly azotemia.
Symptoms and signs
Hematuria is present in 50% of patients.
Complications involve renal vein thrombosis and an increased occurrence of hidden tumors in the lung, stomach, and colon.
Treatment
Approximately 70% of patients may undergo spontaneous remission. If not, cyclosporine or other immunomodulators can be utilized. ACE inhibitors can help minimize urine protein loss. Severe instances may require a kidney transplant.
The prognosis is favorable, particularly in those who have spontaneous remission or respond well to medicines.
Membranous nephropathy frequently leads to adult nephrotic syndrome.
An immunological complex illness of unclear origin.
Secondary disease observed in 10% of systemic lupus erythematosus (SLE) patients, known as type V lupus nephritis, and is occasionally linked to infections (such as hepatitis B and C, syphilis, malaria), medications (such gold salts, penicillamine, NSAIDs), or solid-organ cancer.
The highest incidence occurs in adulthood.
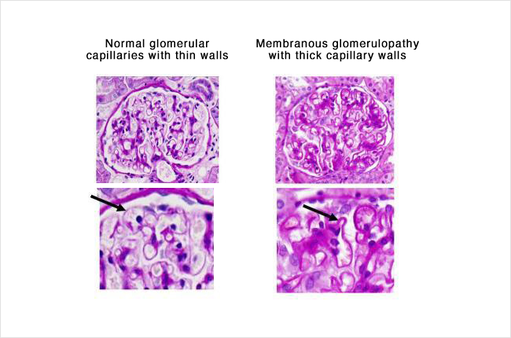
Light microscopy shows diffuse thickening of capillary walls and basement membranes.
Immunofluorescence shows a granular pattern of IgG or C3 deposits, sometimes known as lumpy-bumpy.
Electron microscopy reveals the presence of electron-dense immune complexes deposited in subepithelial areas within the basement membrane of glomerular capillary walls.
The silver methenamine stain shows a spike-and-dome pattern caused by the basement membrane extending between and around the immune deposits. Spikes represent the basement membrane, while domes represent the immune complex deposits.
Clinical presentation of nephrotic syndrome includes edema, proteinuria, anorexia, and commonly azotemia.
Symptoms and signs
Hematuria is present in 50% of patients.
Complications involve renal vein thrombosis and an increased occurrence of hidden tumors in the lung, stomach, and colon.
Treatment
Approximately 70% of patients may undergo spontaneous remission. If not, cyclosporine or other immunomodulators can be utilized. ACE inhibitors can help minimize urine protein loss. Severe instances may require a kidney transplant.
The prognosis is favorable, particularly in those who have spontaneous remission or respond well to medicines.
Membranous nephropathy frequently leads to adult nephrotic syndrome.
0 Comments
