- Published on
Pathology - Pancreatic Carcinoma
Risk factors comprise chronic pancreatitis, smoking, alcohol consumption, high-fat diet, chronic gallbladder disease, and diabetes.
Linked to mutation of the K-ras oncogene and the p53 tumor suppressor gene.
More frequently observed in patients over the age of 60 and in those of African descent.
Pathology
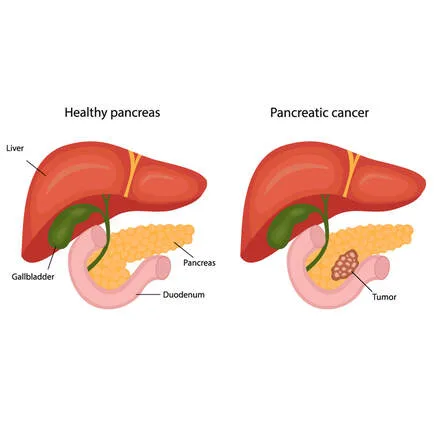
Gross: Can occur in several parts of the pancreas - head (60%), body (15%), tail (5%), or involve the entire organ (20%); characterized by a grayish mass that can impede the ampullary area, causing bile duct blockage and dilation of intrahepatic channels.
Microscopic examination reveals adenocarcinoma with varying levels of differentiation. Tumor cells are observed forming clusters or tubular formations with an invasive growth pattern. Malignant glands may develop from rapidly growing cuboidal epithelial cells with loss of differentiation; accompanied by fibrosis in the surrounding tissue.
Typically asymptomatic until extensive spread to the lungs or bones. Symptoms include upper abdomen pain spreading to the back, weight loss, loss of appetite, migratory thrombophlebitis (Trousseau syndrome), painless obstructive jaundice, and a palpable gallbladder due to common bile duct blockage.
Laboratory results: Elevated levels of direct bilirubin, amylase, ALP, and CEA. elevated CA 19-9 levels.
Treatment involves performing a radical pancreaticoduodenal resection (Whipple surgery) in patients with confined illness, followed by adjuvant radiation and chemotherapy.
The overall 3-year survival rate is less than 4%.
Risk factors comprise chronic pancreatitis, smoking, alcohol consumption, high-fat diet, chronic gallbladder disease, and diabetes.
Linked to mutation of the K-ras oncogene and the p53 tumor suppressor gene.
More frequently observed in patients over the age of 60 and in those of African descent.
Pathology
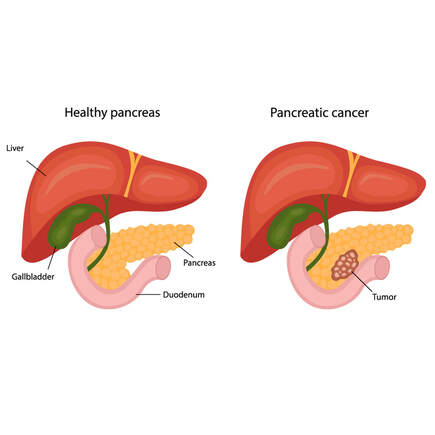
Gross: Can occur in several parts of the pancreas - head (60%), body (15%), tail (5%), or involve the entire organ (20%); characterized by a grayish mass that can impede the ampullary area, causing bile duct blockage and dilation of intrahepatic channels.
Microscopic examination reveals adenocarcinoma with varying levels of differentiation. Tumor cells are observed forming clusters or tubular formations with an invasive growth pattern. Malignant glands may develop from rapidly growing cuboidal epithelial cells with loss of differentiation; accompanied by fibrosis in the surrounding tissue.
Typically asymptomatic until extensive spread to the lungs or bones. Symptoms include upper abdomen pain spreading to the back, weight loss, loss of appetite, migratory thrombophlebitis (Trousseau syndrome), painless obstructive jaundice, and a palpable gallbladder due to common bile duct blockage.
Laboratory results: Elevated levels of direct bilirubin, amylase, ALP, and CEA. elevated CA 19-9 levels.
Treatment involves performing a radical pancreaticoduodenal resection (Whipple surgery) in patients with confined illness, followed by adjuvant radiation and chemotherapy.
The overall 3-year survival rate is less than 4%.
0 Comments
