- Published on
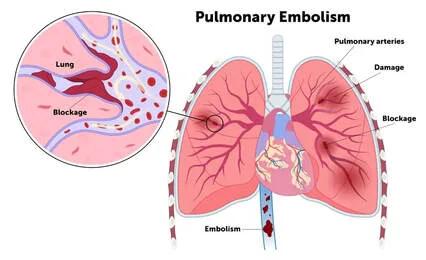
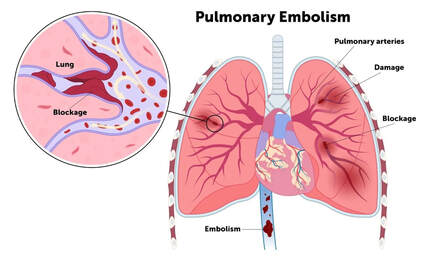
Pathology - Pulmonary embolism
Emboli may consist of air, amniotic fluid, fat, foreign substances, or malignant cells. Thromboemboli, which typically arise from deep vein thrombosis (DVT) in the leg, account for the majority (93%) of emboli.
Gross: Hemorrhage or infarction of the lung typically occurs in the lower lobes. Infarction only happens in individuals with insufficient blood flow due to lung or heart disease. In such cases, it is possible to observe a venous thrombus, which appears dark red with pale-gray fibrin strands and has a hard consistency, stuck in a pulmonary conduit.
The individual may experience tachycardia, dyspnea, pain upon inspiration, and potential symptoms of deep vein thrombosis such as a sore and swollen calf. Additionally, there is a possibility of syncope and tachyarrhythmias. or hypotension in the case of a major pulmonary embolism (PE)
Imaging: An inconsistency was observed on the ventilation-perfusion scan, and a region with incomplete filling was observed on the high-resolution CT scan of the chest.
Laboratory results: The presence of hypoxia and increased levels of D-dimer are observed in cases of thromboembolism.
Anticoagulation should be administered. If the patient is not eligible for anticoagulation, an IVC filter should be considered. Thrombolysis may be appropriate if the patient is experiencing hypotension or showing signs of right ventricular strain. In cases of extensive PE, surgical thrombectomy should be contemplated.
Hospitalized patients rank PE as the third most common cause of mortality.
The presence of Virchow triad, which consists of venous stasis, hypercoagulable condition, and vascular wall damage, increases the likelihood of developing deep vein thrombosis (DVT) and consequently pulmonary embolism (PE).
Emboli may consist of air, amniotic fluid, fat, foreign substances, or malignant cells. Thromboemboli, which typically arise from deep vein thrombosis (DVT) in the leg, account for the majority (93%) of emboli.
Gross: Hemorrhage or infarction of the lung typically occurs in the lower lobes. Infarction only happens in individuals with insufficient blood flow due to lung or heart disease. In such cases, it is possible to observe a venous thrombus, which appears dark red with pale-gray fibrin strands and has a hard consistency, stuck in a pulmonary conduit.
The individual may experience tachycardia, dyspnea, pain upon inspiration, and potential symptoms of deep vein thrombosis such as a sore and swollen calf. Additionally, there is a possibility of syncope and tachyarrhythmias. or hypotension in the case of a major pulmonary embolism (PE)
Imaging: An inconsistency was observed on the ventilation-perfusion scan, and a region with incomplete filling was observed on the high-resolution CT scan of the chest.
Laboratory results: The presence of hypoxia and increased levels of D-dimer are observed in cases of thromboembolism.
Anticoagulation should be administered. If the patient is not eligible for anticoagulation, an IVC filter should be considered. Thrombolysis may be appropriate if the patient is experiencing hypotension or showing signs of right ventricular strain. In cases of extensive PE, surgical thrombectomy should be contemplated.
Hospitalized patients rank PE as the third most common cause of mortality.
The presence of Virchow triad, which consists of venous stasis, hypercoagulable condition, and vascular wall damage, increases the likelihood of developing deep vein thrombosis (DVT) and consequently pulmonary embolism (PE).
0 Comments
