- Published on
Pathology - Rheumatoid Arthritis
The etiology is uncertain, although it is thought that in individuals who are genetically vulnerable (HLA-DR4), an acute inflammatory response sets off a chronic autoimmune reaction.
most prevalent in females aged 30 to 50.
Joint: Initially, there is edema and lymphocytic infiltration in the synovium, which results in the formation of villi made of synovial lining cells and neutrophils in the synovial fluid. Later, the cartilage is destroyed and replaced with fibrocellular granulation tissue, or pannus, and joint deformity is caused by scarring following inflammation.
Rheumatoid nodule: firm, nontender, subcutaneous nodule; palisade of macrophages, lymphocytes, and fibroblasts encircling core of fibrinoid necrosis.
Clinical Signs and Symptoms
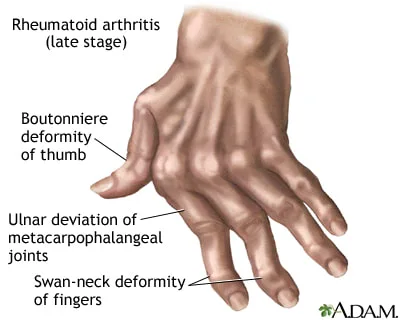
A rheumatoid nodule usually over bony prominences; a swan-neck deformity (flexion of DIP with extension of PIP joint); a boutonniere deformity (extension of DIP with flexion of PIP joint); ulnar deviation of fingers; joint deformities; fatigue; fever; symmetric joint swelling with stiffness and pain that often involves PIP and MCP joints of the fingers, wrists, knees, and ankles that is most severe in the morning and improves with activity.
Pericarditis, pleuritis, vasculitis, pulmonary fibrosis, and secondary amyloidosis are among the complications.
Imaging: narrowing of the joint space; osteopenja; bone degradation at the joints.
Results from the lab included elevated ESR, anemia, positive anti-CCP antibody, and positive rheumatoid factor (IgM antibody against IgG Fe fragment).
Treatments include NSAIDs, glucocorticoids, and immunomodulators (e.g., etanercept for severe disease; methotrexate or leflunomide for mild disease).
The etiology is uncertain, although it is thought that in individuals who are genetically vulnerable (HLA-DR4), an acute inflammatory response sets off a chronic autoimmune reaction.
most prevalent in females aged 30 to 50.
Joint: Initially, there is edema and lymphocytic infiltration in the synovium, which results in the formation of villi made of synovial lining cells and neutrophils in the synovial fluid. Later, the cartilage is destroyed and replaced with fibrocellular granulation tissue, or pannus, and joint deformity is caused by scarring following inflammation.
Rheumatoid nodule: firm, nontender, subcutaneous nodule; palisade of macrophages, lymphocytes, and fibroblasts encircling core of fibrinoid necrosis.
Clinical Signs and Symptoms
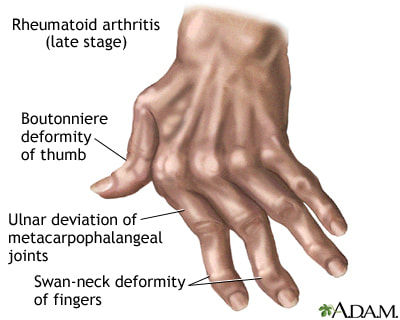
A rheumatoid nodule usually over bony prominences; a swan-neck deformity (flexion of DIP with extension of PIP joint); a boutonniere deformity (extension of DIP with flexion of PIP joint); ulnar deviation of fingers; joint deformities; fatigue; fever; symmetric joint swelling with stiffness and pain that often involves PIP and MCP joints of the fingers, wrists, knees, and ankles that is most severe in the morning and improves with activity.
Pericarditis, pleuritis, vasculitis, pulmonary fibrosis, and secondary amyloidosis are among the complications.
Imaging: narrowing of the joint space; osteopenja; bone degradation at the joints.
Results from the lab included elevated ESR, anemia, positive anti-CCP antibody, and positive rheumatoid factor (IgM antibody against IgG Fe fragment).
Treatments include NSAIDs, glucocorticoids, and immunomodulators (e.g., etanercept for severe disease; methotrexate or leflunomide for mild disease).
0 Comments
