- Published on
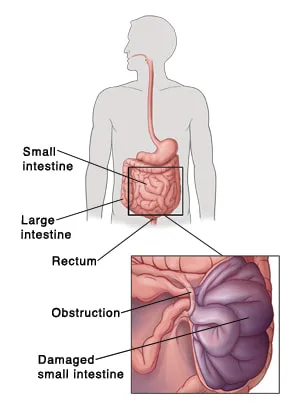
Pathology - Small Bowel Obstruction (SBO)
Pathophysiology
In 75% of cases, the cause is either hernias or, in this instance, adhesions from prior abdominal surgery.
Because the obstruction opposes peristaltic waves, obstruction-related pain is frequently paroxysmal. Peristalstic waves have the potential to cause loud bowel sounds, or borerygmi, which will occur simultaneously with the pain. Edema of the intestinal wall and gas and fluid buildup in the gut close to the obstruction are the causes of distention of the abdomen. In an upright abdominal film, air-fluid levels can be detected proximal to the blockage as progressive black-white horizontal interfaces within the intestine; the absence of colonic gas is pathognomonic of SBO and suggests a total obstruction.
Following many hours of blockage, fluid moves into the intestinal lumen, resulting in hypovolemia, which is shown as tachycardia and low blood pressure.
Vomiting due to visceral discomfort occurs in hypovolemia and hypokalemia. In the intestine, high intraluminal pressure reduces blood flow, which results in ischemia and damage to the intestinal wall. In this instance, a fever and leukocytosis indicate a possible breach of the intestinal barrier and peritonitis.
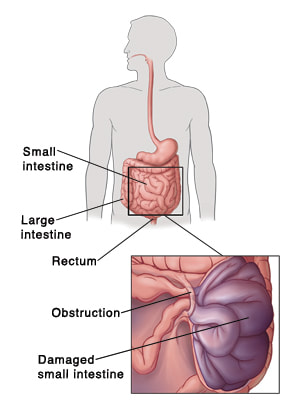
Pathophysiology
In 75% of cases, the cause is either hernias or, in this instance, adhesions from prior abdominal surgery.
Because the obstruction opposes peristaltic waves, obstruction-related pain is frequently paroxysmal. Peristalstic waves have the potential to cause loud bowel sounds, or borerygmi, which will occur simultaneously with the pain. Edema of the intestinal wall and gas and fluid buildup in the gut close to the obstruction are the causes of distention of the abdomen. In an upright abdominal film, air-fluid levels can be detected proximal to the blockage as progressive black-white horizontal interfaces within the intestine; the absence of colonic gas is pathognomonic of SBO and suggests a total obstruction.
Following many hours of blockage, fluid moves into the intestinal lumen, resulting in hypovolemia, which is shown as tachycardia and low blood pressure.
Vomiting due to visceral discomfort occurs in hypovolemia and hypokalemia. In the intestine, high intraluminal pressure reduces blood flow, which results in ischemia and damage to the intestinal wall. In this instance, a fever and leukocytosis indicate a possible breach of the intestinal barrier and peritonitis.
0 Comments
