- Published on
Surgery - Abdominal Aortic Aneurysm
Defintion
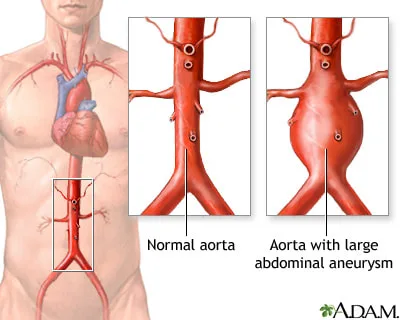
a deviation of >3 cm, or 50% over the normal diameter, in the abdominal aorta's localized dilatation. mostly affects the infrarenal aorta (95%) and the iliac arteries (30%).
Etiology
Degeneration of collagen and elastin in the artery wall is most likely the cause. frequently connected to atherosclerosis. Other conditions include connective tissue illnesses including Marfan's syndrome and Ehlers-Danlos type IV, traumatic injuries, infectious (mycotic), inflammatory (chronic inflammatory infiltration in the artery wall), and arthritis.
Risk Factors
Hypertension, smoking, coronary artery disease, popliteal artery aneurysms, smoking, and family history (10-fold "risk if first-degree relative affected). According to Laplace's law (tension as a radius, pressure), the diameter affects the likelihood of rupture. The risk for AAAs is 3.3% annually for 5–5.9 cm, 9.4% annually for 6–6.9 cm, and 24% annually for 7–7.9 cm.
Epidemiology
15% of people over 80 years old and 5% of people over 60 will have a AAA. Four to six times more common in men; in England and Wales, there are 6000 deaths annually.
History
Often asymptomatic, it can be discovered by accident during testing, imaging, or inspection.
Symptoms: The most typical presentation is collapse or epigastric or back pain due to the rupture of an unidentified AAA. Most patients who are admitted to the hospital have a retroperitoneal leak.
Perhaps mistaken as diverticulitis, muscular back pain, or renal colic. Because of distal embolization or vertebral erosion, intact aneurysms might result in lower limb ischaemia or back pain. Occasionally, exhibit severe gastrointestinal bleeding from erosion into the duodenum or high-output heart failure from an aortocaval fistula.
Examination
One feels a pulsating mass over the umbilicus. If there is leakage or rupture, pallor in the abdomen and back, tachycardia, hypotension, hypovolaemic shock, sporadic bruises on the flanks, and indications of emboli to the feet.
Investigational studies
Sharp presentation Bloods: coagulation, ECG, CXR, U&Es, FBC, and urgent blood cross-matching.
Bedside ultrasonography: To verify the aneurysm's size and presence.
In stable or diagnostic uncertainty: If stable or diagnostic doubt.
CT scan: Not if unstable; instead, proceed directly to the operating room or endovascular suite for repair.
Numerous facilities provide emergency EVAR.
Examining: Research, like the Multicentre Aneurysm Screening Study (MASS), has demonstrated that screening males 65 years of age and older with ultrasound reduces the mortality associated with aneurysms, is economical, and will, over the course of 20 years, minimize the need for emergency surgery by more than two-thirds.
To determine the morphology of an aneurysm before therapy, use CT or MR angiography.
Conservative management of asymptomatic aneurysms (less than 5.5 cm) involves regular follow-up ultrasound scanning (every 3.4 cm annually, or every 6 months if enlargement exceeds 10% annually), as well as managing cardiovascular risk factors. This was shown by the UK Small Aneurysm Study.
Radiological: There are ongoing research comparing endovascular treatment with stent placement (EVAR) against open repairs. EVAR is becoming more common. Between 40 and 60 percent of AAAs are acceptable, meaning they have a neck and landing sites that are ideal for the endograft. When EVAR and open surgery were compared in individuals deemed surgically capable, EVAR1 had a 3% advantage in aneurysm-related survival after 4 years. When EVAR2 was applied to unfit patients, it did not find any differences in all-cause mortality between EVAR and no intervention.
Surgical: Using tube or bifurcation grafts (see to Procedures) is recommended for: asymptomatic aneurysms larger than 5.5 cm in diameter; symptomatic or quickly increasing aneurysms; emergency treatment (e.g., suspected leaking or ruptured aneurysm).
Complications
The most common include rupture, distal embolus, abrupt total thrombosis, gram-negative or staphylococcal infection, persistent consumptive coagulopathy, ischaemia of the gut, aortic-intestinal fistula, and arteriovenous fistula resulting from aneurysm eroding into the inferior venous catheter.
following surgery: bleeding, thrombosis, embolism, colonic ischaemia, renal failure, problems related to the heart and lungs, and death.
Of EVAR: As mentioned before; also, migration, endoleak, kinking/distortion, fracture of the stent, renal infarction, and limb/pelvic ischaemia.
Prognosis
Only roughly 50% of patients with a ruptured AAA survive once they get at the hospital, accounting for the remaining 80% of deaths.
Mortality from elective open surgery is less than 5% in specialized centers. EVAR has a 2% death rate, however re-intervention rates are greater and observation is necessary.
Defintion
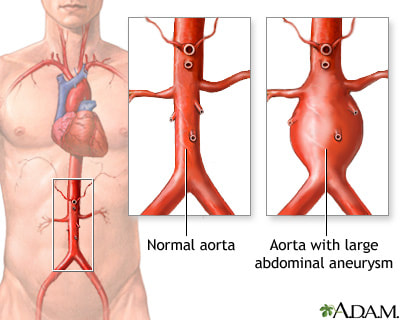
a deviation of >3 cm, or 50% over the normal diameter, in the abdominal aorta's localized dilatation. mostly affects the infrarenal aorta (95%) and the iliac arteries (30%).
Etiology
Degeneration of collagen and elastin in the artery wall is most likely the cause. frequently connected to atherosclerosis. Other conditions include connective tissue illnesses including Marfan's syndrome and Ehlers-Danlos type IV, traumatic injuries, infectious (mycotic), inflammatory (chronic inflammatory infiltration in the artery wall), and arthritis.
Risk Factors
Hypertension, smoking, coronary artery disease, popliteal artery aneurysms, smoking, and family history (10-fold "risk if first-degree relative affected). According to Laplace's law (tension as a radius, pressure), the diameter affects the likelihood of rupture. The risk for AAAs is 3.3% annually for 5–5.9 cm, 9.4% annually for 6–6.9 cm, and 24% annually for 7–7.9 cm.
Epidemiology
15% of people over 80 years old and 5% of people over 60 will have a AAA. Four to six times more common in men; in England and Wales, there are 6000 deaths annually.
History
Often asymptomatic, it can be discovered by accident during testing, imaging, or inspection.
Symptoms: The most typical presentation is collapse or epigastric or back pain due to the rupture of an unidentified AAA. Most patients who are admitted to the hospital have a retroperitoneal leak.
Perhaps mistaken as diverticulitis, muscular back pain, or renal colic. Because of distal embolization or vertebral erosion, intact aneurysms might result in lower limb ischaemia or back pain. Occasionally, exhibit severe gastrointestinal bleeding from erosion into the duodenum or high-output heart failure from an aortocaval fistula.
Examination
One feels a pulsating mass over the umbilicus. If there is leakage or rupture, pallor in the abdomen and back, tachycardia, hypotension, hypovolaemic shock, sporadic bruises on the flanks, and indications of emboli to the feet.
Investigational studies
Sharp presentation Bloods: coagulation, ECG, CXR, U&Es, FBC, and urgent blood cross-matching.
Bedside ultrasonography: To verify the aneurysm's size and presence.
In stable or diagnostic uncertainty: If stable or diagnostic doubt.
CT scan: Not if unstable; instead, proceed directly to the operating room or endovascular suite for repair.
Numerous facilities provide emergency EVAR.
Examining: Research, like the Multicentre Aneurysm Screening Study (MASS), has demonstrated that screening males 65 years of age and older with ultrasound reduces the mortality associated with aneurysms, is economical, and will, over the course of 20 years, minimize the need for emergency surgery by more than two-thirds.
To determine the morphology of an aneurysm before therapy, use CT or MR angiography.
Conservative management of asymptomatic aneurysms (less than 5.5 cm) involves regular follow-up ultrasound scanning (every 3.4 cm annually, or every 6 months if enlargement exceeds 10% annually), as well as managing cardiovascular risk factors. This was shown by the UK Small Aneurysm Study.
Radiological: There are ongoing research comparing endovascular treatment with stent placement (EVAR) against open repairs. EVAR is becoming more common. Between 40 and 60 percent of AAAs are acceptable, meaning they have a neck and landing sites that are ideal for the endograft. When EVAR and open surgery were compared in individuals deemed surgically capable, EVAR1 had a 3% advantage in aneurysm-related survival after 4 years. When EVAR2 was applied to unfit patients, it did not find any differences in all-cause mortality between EVAR and no intervention.
Surgical: Using tube or bifurcation grafts (see to Procedures) is recommended for: asymptomatic aneurysms larger than 5.5 cm in diameter; symptomatic or quickly increasing aneurysms; emergency treatment (e.g., suspected leaking or ruptured aneurysm).
Complications
The most common include rupture, distal embolus, abrupt total thrombosis, gram-negative or staphylococcal infection, persistent consumptive coagulopathy, ischaemia of the gut, aortic-intestinal fistula, and arteriovenous fistula resulting from aneurysm eroding into the inferior venous catheter.
following surgery: bleeding, thrombosis, embolism, colonic ischaemia, renal failure, problems related to the heart and lungs, and death.
Of EVAR: As mentioned before; also, migration, endoleak, kinking/distortion, fracture of the stent, renal infarction, and limb/pelvic ischaemia.
Prognosis
Only roughly 50% of patients with a ruptured AAA survive once they get at the hospital, accounting for the remaining 80% of deaths.
Mortality from elective open surgery is less than 5% in specialized centers. EVAR has a 2% death rate, however re-intervention rates are greater and observation is necessary.
0 Comments
