- Published on
Surgery - Acute Ischemic Lower Limb
Introduction
abrupt blockage of the supplying artery resulting in limb ischaemia.
Etiology
Pathophysiology: Abrupt stoppage of blood flow. Emboli typically settle in the locations where vessels split. Cell injury occurs in two stages: ischemic injury, which occurs when tissues are cut off from blood flow, and reperfusion injury, which occurs when blood flow is restored.
Thrombosis: Low flow conditions, such as hypovolemia, aneurysm, graft stenosis, atherosclerosis, and thrombotic states.
Heart: 90%, great vessels: 9%, and other: 1% are the sources of embolism. Atrial fibrillation, myxoma of the atrium, aneurysms, valvular heart disease, and recent MI.
Trauma or dissection are two examples of vascular damage.
Epidemiology
14 cases out of 100,000 are estimated.
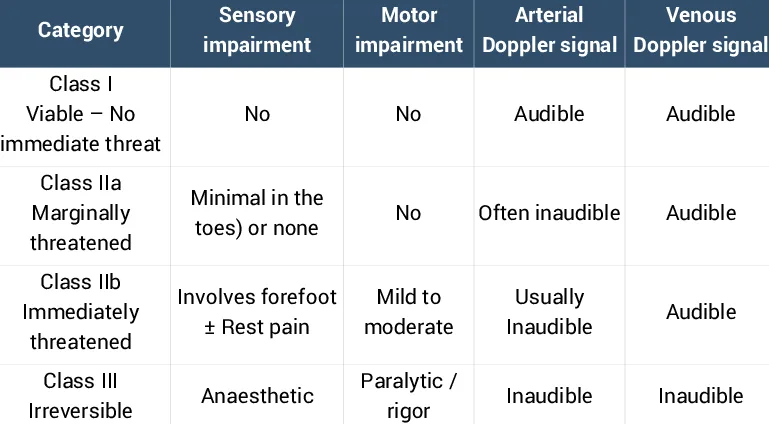
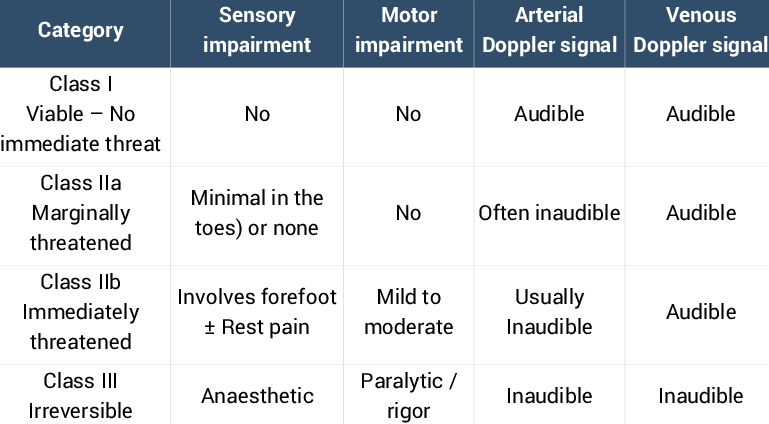
Pallor, pain, paraesthesia, pulselessness, paralysis, and a perishingly cold limb are the six Ps.The location of occlusion, length of ischaemia, and level of collateral circulation all affect the symptoms and signs.
Embolus is more likely to occur in cases of severe, abrupt onset, and recognizable possible cause, such as atrial fibrillation.
Thrombosis is typically less severe if collaterals are present, there is a history of peripheral vascular disease or claudication, and there isn't an identifiable embolus source.
Examination
Pale limb with no pulse; capillary return is slow.
After a few hours, there is capillary rupture-related venous stagnation, which causes a mottled appearance and, in later stages, permanent staining. There are changes in sensation, and if the ischemia is severe, there may be muscle paralysis and anesthesia, indicating that the limb may not be viable.
Investigations
Blood tests: thrombophilia screen, coagulation profile, G&S, FBC, and U&Es.
Imaging: CXR, Doppler or duplex blood flow scans, arteriography to show the occlusion site and, if the limb is still viable, to arrange an operation.
ECG: Checking for irregular heartbeat.
Management
Immediate: Heparin anticoagulation, analgesics, and ABCs to stop the spread of thrombus.
Surgery: Revascularization in six hours to save the limb. When cardiac disease is present, there is frequently a substantial operational risk. Anticoagulation after surgery is crucial.
If an embolus is found, an embolectomy will be performed, which entails artery isolation, arteriotomy, and the insertion of a Fogarty balloon-tipped catheter that will be inserted past the embolus and then withdrawn to recover the embolus.
If the thrombosis is acute or chronic, collateral development may allow the limb to survive longer. In this case, percutaneous intervention such as suction, intraarterial thrombolysis with local infusion of t-PA, and angioplasty of underlying stenoses are viable options.
In the event that thrombosis is required for this treatment but the limb is not expected to survive for 12 to 24 hours: If physically feasible, urgent reconstructive surgery using synthetic (PTFE or Dacron) or autogenous (saphenous vein) bypass grafting is needed.
Fasciotomy is necessary if compartment syndrome is a concern.
Amputation of the limb in question.
Complications
From disease: death, limb loss, and gangrene.
From intra-arterial thrombolysis: severe bleeding, CVA, and mortality (1-2%).
Reperfusion syndrome, compartment syndrome, rhabdomyolysis, and rethrombosis are post-treatment complications.
Prognosis
There is a 30% chance of losing a limb; 10% of people die from it, with heart disease being the main cause of death.
Introduction
abrupt blockage of the supplying artery resulting in limb ischaemia.
Etiology
Pathophysiology: Abrupt stoppage of blood flow. Emboli typically settle in the locations where vessels split. Cell injury occurs in two stages: ischemic injury, which occurs when tissues are cut off from blood flow, and reperfusion injury, which occurs when blood flow is restored.
Thrombosis: Low flow conditions, such as hypovolemia, aneurysm, graft stenosis, atherosclerosis, and thrombotic states.
Heart: 90%, great vessels: 9%, and other: 1% are the sources of embolism. Atrial fibrillation, myxoma of the atrium, aneurysms, valvular heart disease, and recent MI.
Trauma or dissection are two examples of vascular damage.
Epidemiology
14 cases out of 100,000 are estimated.
Pallor, pain, paraesthesia, pulselessness, paralysis, and a perishingly cold limb are the six Ps.The location of occlusion, length of ischaemia, and level of collateral circulation all affect the symptoms and signs.
Embolus is more likely to occur in cases of severe, abrupt onset, and recognizable possible cause, such as atrial fibrillation.
Thrombosis is typically less severe if collaterals are present, there is a history of peripheral vascular disease or claudication, and there isn't an identifiable embolus source.
Examination
Pale limb with no pulse; capillary return is slow.
After a few hours, there is capillary rupture-related venous stagnation, which causes a mottled appearance and, in later stages, permanent staining. There are changes in sensation, and if the ischemia is severe, there may be muscle paralysis and anesthesia, indicating that the limb may not be viable.
Investigations
Blood tests: thrombophilia screen, coagulation profile, G&S, FBC, and U&Es.
Imaging: CXR, Doppler or duplex blood flow scans, arteriography to show the occlusion site and, if the limb is still viable, to arrange an operation.
ECG: Checking for irregular heartbeat.
Management
Immediate: Heparin anticoagulation, analgesics, and ABCs to stop the spread of thrombus.
Surgery: Revascularization in six hours to save the limb. When cardiac disease is present, there is frequently a substantial operational risk. Anticoagulation after surgery is crucial.
If an embolus is found, an embolectomy will be performed, which entails artery isolation, arteriotomy, and the insertion of a Fogarty balloon-tipped catheter that will be inserted past the embolus and then withdrawn to recover the embolus.
If the thrombosis is acute or chronic, collateral development may allow the limb to survive longer. In this case, percutaneous intervention such as suction, intraarterial thrombolysis with local infusion of t-PA, and angioplasty of underlying stenoses are viable options.
In the event that thrombosis is required for this treatment but the limb is not expected to survive for 12 to 24 hours: If physically feasible, urgent reconstructive surgery using synthetic (PTFE or Dacron) or autogenous (saphenous vein) bypass grafting is needed.
Fasciotomy is necessary if compartment syndrome is a concern.
Amputation of the limb in question.
Complications
From disease: death, limb loss, and gangrene.
From intra-arterial thrombolysis: severe bleeding, CVA, and mortality (1-2%).
Reperfusion syndrome, compartment syndrome, rhabdomyolysis, and rethrombosis are post-treatment complications.
Prognosis
There is a 30% chance of losing a limb; 10% of people die from it, with heart disease being the main cause of death.


0 Comments
