- Published on
Surgery - Advanced Traumatic Life Support (ATLS)
Indications
Early trauma management that prioritizes addressing the condition that poses the biggest risk to life.
Procedure
Pre-hospital phase: The trauma patient is promptly assessed. Treatment of shock, hypoxemia, and prompt transfer to a suitable hospital.
Hospital phase: A trauma team, which typically consists of a general surgeon, an orthopaedic surgeon, an anesthetist, and nursing support, conducts the primary survey. The team leader leads the team. Every team member should have a predetermined job, and the team leader should oversee a methodical approach to the primary and secondary surveys.
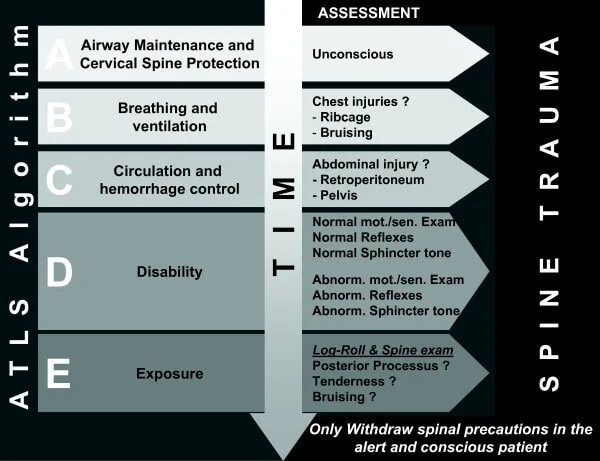
Control of the airways and the c-spine: suction and oral examination for foreign bodies. Assess the patient's (conscious or unconscious) capacity to maintain their own airway. Chin lift/jaw push, suitable cricothyroidotomy or intubation, orally or nasopharyngeally (not in cases of head trauma) as needed.
Breathing: Use a non-rebreather mask to provide 100% oxygen. Examine the respiratory rate, bilateral breath sounds, symmetrical chest expansion, and tracheal deviation. oximetry of the pulse.
In the event of a tension pneumothorax, decompress the needle on the affected side. Look for emphysema under the skin. A chest drain and a dressing with a seal on three sides are necessary for an open sucking pneumothorax. Seek out the flail chest.
Circulation: Measure blood pressure, pulse pressure, capillary return, and pulse in addition to performing intravenous access (using two large-bore peripheral cannulae) and drawing blood for cross-matching FBC, U&E, and G&S.
Assessing the major bodily cavities, the belly, the pelvis for evidence of pelvic fractures, the chest for hemothorax, and the management of external bleeding are all important aspects of treating shock and hemodynamic instability as well as internal bleeding.
Fluid resuscitation (crystallin, collloid, or blood); nonetheless, "permissive hypotension" of systolic blood pressure may be necessary if intracavity bleeding is not yet under control (not in severe head injury where cerebral perfusion pressure should be optimized). If stable, get a CT scan or a FAST (focused abdominal sonogram for trauma).
Disability: Gross neurologic damage assessed using the Glasgow Coma Score (GCS) or an AVPU (Alert, Voice elicits response, Pain elicits response, Unresponsive) score. Verify your blood sugar.
Exposure: Examine the patient for more injuries, undress them entirely to avoid hypothermia, logroll them, and check for spinal or posterior injuries. Treat and prevent hypothermia by using heated IV fluids, blankets, etc.
Regular evaluation is essential. Any decline necessitates a quick reassessment of the ABC.
A large portion of the ABC may be completed in simultaneously when a team is doing the assessment and resuscitation.
Secondary survey: Does not start until after the completion of the primary survey and the start of resuscitation. comprehensive assessment. MANY history (drugs, allergies, past medical conditions, pregnancy, last meal, and incidents connected to the accident). Regular evaluation is essential! comprehensive neurological assessment. Radiology as well as further recommended testing, including as ABG, FAST scan, and radiographic imaging for any fractures. stomach tube or urinary catheter. Injuries determine whether to pursue more decisive management. Sometimes a transfer to a tertiary trauma or neurosurgical center is required.
Investigational studies
Blood: FBC, suitable crossmatch, U&E, LFTs, clotting, and blood grouping.
Urinalysis: b-HCG if pregnancy risk, urine dipstick for haematuria.
Radiographs of the pelvis, chest, and cervical spine are included in the primary survey. An upright chest X-ray can be used to assess a penetrating abdominal injury.
FAST scanning is now the go-to non-invasive quick assessment method for trauma patients' hemoperitoneum.
CT scanning: When the patient is stable, as needed. An urgent laparotomy is required if there is any suspicion of an intra-abdominal bleed (hypotension, enlarged belly, etc.).
Radiographs: Should there be a possible bone fracture.
Death distribution in three dimensions. caused by a large-vessel, brain, or spinal cord injury early (within minutes). The golden hour, which is the second peak (within hours) of hemorrhage, is the time when there is the highest chance that receiving medical attention quickly can avert death. Sepsis-related third peak (within days to weeks).
Indications
Early trauma management that prioritizes addressing the condition that poses the biggest risk to life.
Procedure
Pre-hospital phase: The trauma patient is promptly assessed. Treatment of shock, hypoxemia, and prompt transfer to a suitable hospital.
Hospital phase: A trauma team, which typically consists of a general surgeon, an orthopaedic surgeon, an anesthetist, and nursing support, conducts the primary survey. The team leader leads the team. Every team member should have a predetermined job, and the team leader should oversee a methodical approach to the primary and secondary surveys.
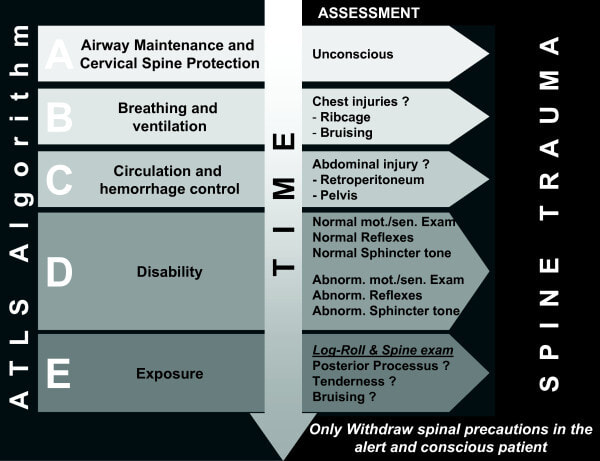
Control of the airways and the c-spine: suction and oral examination for foreign bodies. Assess the patient's (conscious or unconscious) capacity to maintain their own airway. Chin lift/jaw push, suitable cricothyroidotomy or intubation, orally or nasopharyngeally (not in cases of head trauma) as needed.
Breathing: Use a non-rebreather mask to provide 100% oxygen. Examine the respiratory rate, bilateral breath sounds, symmetrical chest expansion, and tracheal deviation. oximetry of the pulse.
In the event of a tension pneumothorax, decompress the needle on the affected side. Look for emphysema under the skin. A chest drain and a dressing with a seal on three sides are necessary for an open sucking pneumothorax. Seek out the flail chest.
Circulation: Measure blood pressure, pulse pressure, capillary return, and pulse in addition to performing intravenous access (using two large-bore peripheral cannulae) and drawing blood for cross-matching FBC, U&E, and G&S.
Assessing the major bodily cavities, the belly, the pelvis for evidence of pelvic fractures, the chest for hemothorax, and the management of external bleeding are all important aspects of treating shock and hemodynamic instability as well as internal bleeding.
Fluid resuscitation (crystallin, collloid, or blood); nonetheless, "permissive hypotension" of systolic blood pressure may be necessary if intracavity bleeding is not yet under control (not in severe head injury where cerebral perfusion pressure should be optimized). If stable, get a CT scan or a FAST (focused abdominal sonogram for trauma).
Disability: Gross neurologic damage assessed using the Glasgow Coma Score (GCS) or an AVPU (Alert, Voice elicits response, Pain elicits response, Unresponsive) score. Verify your blood sugar.
Exposure: Examine the patient for more injuries, undress them entirely to avoid hypothermia, logroll them, and check for spinal or posterior injuries. Treat and prevent hypothermia by using heated IV fluids, blankets, etc.
Regular evaluation is essential. Any decline necessitates a quick reassessment of the ABC.
A large portion of the ABC may be completed in simultaneously when a team is doing the assessment and resuscitation.
Secondary survey: Does not start until after the completion of the primary survey and the start of resuscitation. comprehensive assessment. MANY history (drugs, allergies, past medical conditions, pregnancy, last meal, and incidents connected to the accident). Regular evaluation is essential! comprehensive neurological assessment. Radiology as well as further recommended testing, including as ABG, FAST scan, and radiographic imaging for any fractures. stomach tube or urinary catheter. Injuries determine whether to pursue more decisive management. Sometimes a transfer to a tertiary trauma or neurosurgical center is required.
Investigational studies
Blood: FBC, suitable crossmatch, U&E, LFTs, clotting, and blood grouping.
Urinalysis: b-HCG if pregnancy risk, urine dipstick for haematuria.
Radiographs of the pelvis, chest, and cervical spine are included in the primary survey. An upright chest X-ray can be used to assess a penetrating abdominal injury.
FAST scanning is now the go-to non-invasive quick assessment method for trauma patients' hemoperitoneum.
CT scanning: When the patient is stable, as needed. An urgent laparotomy is required if there is any suspicion of an intra-abdominal bleed (hypotension, enlarged belly, etc.).
Radiographs: Should there be a possible bone fracture.
Death distribution in three dimensions. caused by a large-vessel, brain, or spinal cord injury early (within minutes). The golden hour, which is the second peak (within hours) of hemorrhage, is the time when there is the highest chance that receiving medical attention quickly can avert death. Sepsis-related third peak (within days to weeks).
0 Comments
