- Published on
Surgery - Aortic Dissection
Introduction
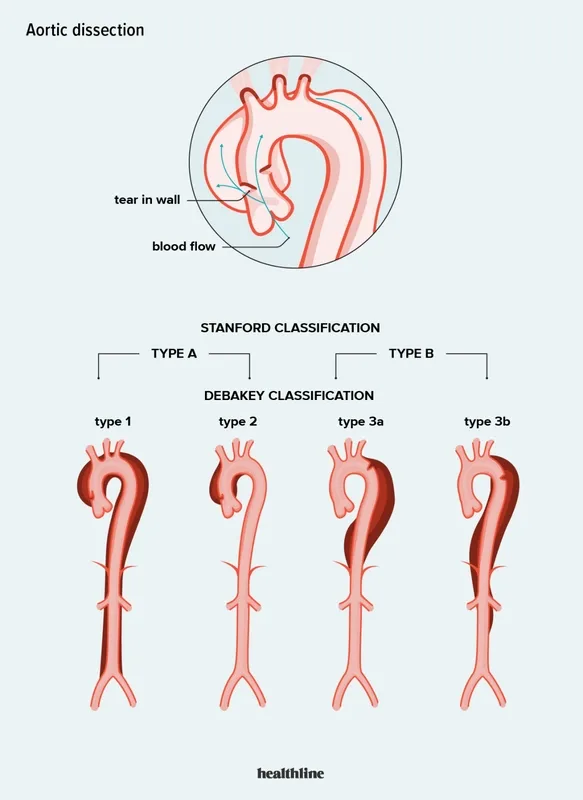
A disorder where blood can enter the aorta wall through a rupture in the aortic intima, splitting the inner and outer tunica media and forming a false lumen.
Etiology
The predisposing event is degenerative alterations in the aortic media's smooth muscle.
Aortic atherosclerosis, hypertension, connective tissue diseases (SLE, Marfan's, Ehlers-Danlos), congenital cardiac abnormalities (aortic coarctation, for example), aortitis (Takayasu's aortitis, tertiary syphilis), iatrogenic (during angiography or angioplasty, for example), trauma, and crack cocaine are common causes and predisposing factors.
Aortic Dissection is divided by Stanford categorization into:
Type A: Aorta tears that ascend (most common); Type B: Aorta tears that descend, extending away from the left subclavian artery.
False aneurysm expansion can block the renal, celiac, subclavian, or carotid arteries.
Epidemiology
most typical in the age range of 40 to 60. Men outnumber women.
History
An MI may seem like an abrupt core tearing pain that radiates to the back.
The aorta and its branches may become occluded as a result of aortic dissection.
Blackout, dysphasia, and hemiparesis due to carotid blockage.
Chest pain due to coronary artery blockage (angina or MI).
Ataxia and loss of consciousness due to subclavian blockage.
Paraplegia: anterior spinal artery.
Severe abdominal pain due to a celiac blockage (ischaemic bowel).
Renal failure and anuria due to renal artery blockage.
Examination
A murmur on the back that descends to the belly below the left scapula.
Blood pressure: Wide pulse pressure, hypertension (BP difference between arms of >20 mmHg). In case hypotension indicates tamponade, make sure to look for pulsus paradoxus.
An insufficient aorta Early diastolic murmur across the aortic region, collapsing pulse.
Arm pulses that aren't equal.
Investigational studies
Blood: coagulation, U&E (renal function), FBC, and cross-match.
CXR: Localized aortic arch bulging and widened mediastinum.
ECG: Usually normal. indicators of inferior MI or left ventricular hypertrophy if the right coronary artery's ostia is compromised by dissection.
False lumen of dissection visible in CT thorax abdomen.
Trans-oesophageal echocardiography is quite specific.
Vascular angiography and cardiac catheterization.
Management
Acute: In the event that resuscitation is suspected, an immediate CT scan should be carried out. Restart the heart and keep an eye on your blood pressure, pulse, and urine catheter. Idealized for ITU management.
Surgery is used to treat type A dissection. A surgical emergency due to the possibility of cardiac tamponade. A tube graft is used to repair the damaged aorta. Replaced aortic valves are another option.
Treatment options for type B dissection include medication, surgery, and endovascular stenting. take IV nitroprusside and/or IV labetalol to control blood pressure and stop additional dissection (take a calcium channel blocker if b-blockers are contraindicated). Patients with end-organ ischemia, aortic enlargement, intractable or recurrent pain, or dissection advancement may benefit from surgery. Some centers offer endovascular repair, a more recent procedure that uses endovascular stents (ADSORB trial results awaited).
Complications
cardiac tamponade, syncope, cerebrovascular, renal, mesenteric, or spinal ischaemia; aortic rupture.
Prognosis
30% in 24 hours and 75% at 2 weeks of untreated mortality.
5–10% operational mortality. 10% more suffer from neurological aftereffects.
Type B has a better prognosis than type A.
Introduction
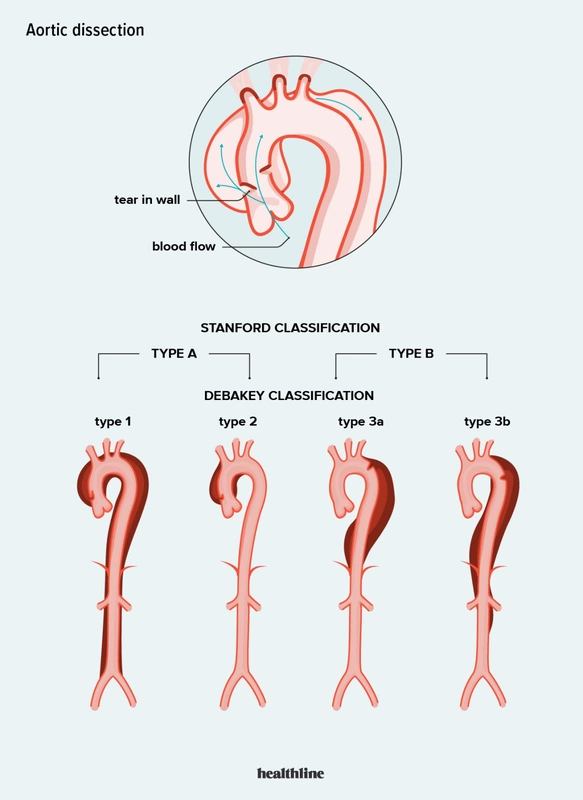
A disorder where blood can enter the aorta wall through a rupture in the aortic intima, splitting the inner and outer tunica media and forming a false lumen.
Etiology
The predisposing event is degenerative alterations in the aortic media's smooth muscle.
Aortic atherosclerosis, hypertension, connective tissue diseases (SLE, Marfan's, Ehlers-Danlos), congenital cardiac abnormalities (aortic coarctation, for example), aortitis (Takayasu's aortitis, tertiary syphilis), iatrogenic (during angiography or angioplasty, for example), trauma, and crack cocaine are common causes and predisposing factors.
Aortic Dissection is divided by Stanford categorization into:
Type A: Aorta tears that ascend (most common); Type B: Aorta tears that descend, extending away from the left subclavian artery.
False aneurysm expansion can block the renal, celiac, subclavian, or carotid arteries.
Epidemiology
most typical in the age range of 40 to 60. Men outnumber women.
History
An MI may seem like an abrupt core tearing pain that radiates to the back.
The aorta and its branches may become occluded as a result of aortic dissection.
Blackout, dysphasia, and hemiparesis due to carotid blockage.
Chest pain due to coronary artery blockage (angina or MI).
Ataxia and loss of consciousness due to subclavian blockage.
Paraplegia: anterior spinal artery.
Severe abdominal pain due to a celiac blockage (ischaemic bowel).
Renal failure and anuria due to renal artery blockage.
Examination
A murmur on the back that descends to the belly below the left scapula.
Blood pressure: Wide pulse pressure, hypertension (BP difference between arms of >20 mmHg). In case hypotension indicates tamponade, make sure to look for pulsus paradoxus.
An insufficient aorta Early diastolic murmur across the aortic region, collapsing pulse.
Arm pulses that aren't equal.
Investigational studies
Blood: coagulation, U&E (renal function), FBC, and cross-match.
CXR: Localized aortic arch bulging and widened mediastinum.
ECG: Usually normal. indicators of inferior MI or left ventricular hypertrophy if the right coronary artery's ostia is compromised by dissection.
False lumen of dissection visible in CT thorax abdomen.
Trans-oesophageal echocardiography is quite specific.
Vascular angiography and cardiac catheterization.
Management
Acute: In the event that resuscitation is suspected, an immediate CT scan should be carried out. Restart the heart and keep an eye on your blood pressure, pulse, and urine catheter. Idealized for ITU management.
Surgery is used to treat type A dissection. A surgical emergency due to the possibility of cardiac tamponade. A tube graft is used to repair the damaged aorta. Replaced aortic valves are another option.
Treatment options for type B dissection include medication, surgery, and endovascular stenting. take IV nitroprusside and/or IV labetalol to control blood pressure and stop additional dissection (take a calcium channel blocker if b-blockers are contraindicated). Patients with end-organ ischemia, aortic enlargement, intractable or recurrent pain, or dissection advancement may benefit from surgery. Some centers offer endovascular repair, a more recent procedure that uses endovascular stents (ADSORB trial results awaited).
Complications
cardiac tamponade, syncope, cerebrovascular, renal, mesenteric, or spinal ischaemia; aortic rupture.
Prognosis
30% in 24 hours and 75% at 2 weeks of untreated mortality.
5–10% operational mortality. 10% more suffer from neurological aftereffects.
Type B has a better prognosis than type A.
0 Comments
