- Published on
Surgery - Appendicitis
Introduction
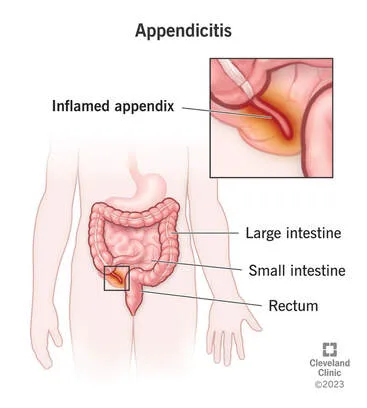
acute vermiform appendix infection and inflammation.
AE T IOLOGY
initiated by lymphoid hyperplasia, oedema, or luminal blockage caused by a faecolith (inspissated feces). The less common causes of luminal blockage are caecal cancer and helminth infections.
Epidemiology
One of the most prevalent emergency surgical diagnoses in the UK, with a 7% lifetime risk, can occur at any age, with a peak prevalence in the second and third decades.
H HISTORY
Typical presentation (less than 50% of cases): Pain in the abdomen (typically subsiding after 72 hours), diffuse at first, periumbilical, and colicky (visceral pain subsiding after a few hours). Sharp pain that is restricted to the RIF develops (somatic pain as parietal peritoneum involvement). The most prevalent symptoms are nausea and anorexia. It's possible to throw up.
Other possible manifestations include pain in the lower abdomen (pelvic appendix), right upper quadrant (long appendix), or right flank (retrocaecal appendix). may be linked to frequent urination or loose stools as a result of the inflamed appendix irritating the bladder or colon.
Examination
Facial flush, tachycardia, and mild pyrexia.
Often, rebound tenderness (visible on percussion) and guarding are present along a line that runs from the umbilicus to the anterior superior iliac spine, or McBurney's point, where the intensity of the abdominal pain is greatest.
Pressure applied over the left iliac fossa causes pain in the right iliac fossa, which is known as Rovsing's sign.
Pathogenesis
Transmurally propagating intestinal flora and inflammation are caused by luminal blockage. The swelling causes end artery blockage and thrombosis, resulting in gangrene and necrosis of the appendix. If treatment is not received, the inflammation may become localized by omentumor bowel loops, resulting in an appendix mass or abscess, or it may rupture with peritonitis. Histology may occasionally reveal a carcinoid tumor; if this is larger than 1-2 cm, a right hemicolectomy is recommended.
Investigational studies
A clinical diagnosis of appendicitis is common.
Blood: "WCC and CRP, LFTs, amylase (to check for pancreatitis and biliary pathology), U&Es."
Urine: For pregnancy tests in women of childbearing age, microscopy, culture, and sensitivity.
Imaging: Ultrasound (helpful in skilled hands, frequently difficult to visualize appendix; can reveal other pathology, such as ovarian cysts). CT requires a large amount of radiation exposure but has a 94% sensitivity and 95% specificity. It is particularly helpful if additional disease, such as diverticulitis, is a concern.
Accurate diagnosis and therapy are made possible by diagnostic laparoscopy.
Management
General: intravenous fluids, broad-spectrum antibiotics before and after surgery in the event of severe sepsis symptoms. If there are any unclear symptoms or indications, keep an eye on them and check them frequently.
Surgery: Laparoscopic or open appendicectomies (see Procedures).
After surgery: Antibiotics may be continued, particularly if the appendix is punctured or gangrenous.
Appendiceal abscess: Drainage can be done intraoperatively (with appendicectomy if safe) or percutaneously (with ultrasound or CT guidance, for example). In the event of a clinical deterioration, management of an appendiceal mass may involve periodic reassessment, parenteral fluids, antibiotics, and non-operative treatment. Weeks after the initial procedure, an interval appendicectomy may be done (Ochsner–Sherren method). If an adult does not undergo this, a barium enema or colonoscopy ought to be carried out in order to rule out a right colon malignancy.
Complications
Appendix abscess, perforation, peritonitis, inflammatory mass, and infrequently, portal pyaemia.
Following surgery, there may be an appendix stump faecal fistula, an abscess, an ileus, and wound infection.
Prognosis
An appendixectomy can be cured. It may be fatal if left untreated. The extremely young, the elderly, and pregnant women have greater rates of morbidity and mortality, making diagnosis more challenging in these situations.
Introduction
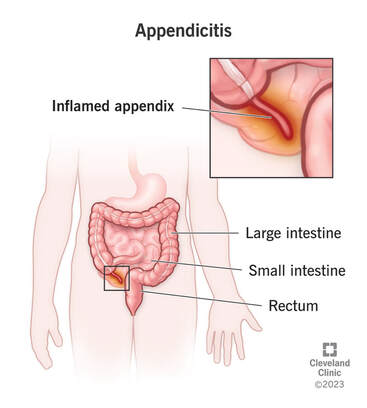
acute vermiform appendix infection and inflammation.
AE T IOLOGY
initiated by lymphoid hyperplasia, oedema, or luminal blockage caused by a faecolith (inspissated feces). The less common causes of luminal blockage are caecal cancer and helminth infections.
Epidemiology
One of the most prevalent emergency surgical diagnoses in the UK, with a 7% lifetime risk, can occur at any age, with a peak prevalence in the second and third decades.
H HISTORY
Typical presentation (less than 50% of cases): Pain in the abdomen (typically subsiding after 72 hours), diffuse at first, periumbilical, and colicky (visceral pain subsiding after a few hours). Sharp pain that is restricted to the RIF develops (somatic pain as parietal peritoneum involvement). The most prevalent symptoms are nausea and anorexia. It's possible to throw up.
Other possible manifestations include pain in the lower abdomen (pelvic appendix), right upper quadrant (long appendix), or right flank (retrocaecal appendix). may be linked to frequent urination or loose stools as a result of the inflamed appendix irritating the bladder or colon.
Examination
Facial flush, tachycardia, and mild pyrexia.
Often, rebound tenderness (visible on percussion) and guarding are present along a line that runs from the umbilicus to the anterior superior iliac spine, or McBurney's point, where the intensity of the abdominal pain is greatest.
Pressure applied over the left iliac fossa causes pain in the right iliac fossa, which is known as Rovsing's sign.
Pathogenesis
Transmurally propagating intestinal flora and inflammation are caused by luminal blockage. The swelling causes end artery blockage and thrombosis, resulting in gangrene and necrosis of the appendix. If treatment is not received, the inflammation may become localized by omentumor bowel loops, resulting in an appendix mass or abscess, or it may rupture with peritonitis. Histology may occasionally reveal a carcinoid tumor; if this is larger than 1-2 cm, a right hemicolectomy is recommended.
Investigational studies
A clinical diagnosis of appendicitis is common.
Blood: "WCC and CRP, LFTs, amylase (to check for pancreatitis and biliary pathology), U&Es."
Urine: For pregnancy tests in women of childbearing age, microscopy, culture, and sensitivity.
Imaging: Ultrasound (helpful in skilled hands, frequently difficult to visualize appendix; can reveal other pathology, such as ovarian cysts). CT requires a large amount of radiation exposure but has a 94% sensitivity and 95% specificity. It is particularly helpful if additional disease, such as diverticulitis, is a concern.
Accurate diagnosis and therapy are made possible by diagnostic laparoscopy.
Management
General: intravenous fluids, broad-spectrum antibiotics before and after surgery in the event of severe sepsis symptoms. If there are any unclear symptoms or indications, keep an eye on them and check them frequently.
Surgery: Laparoscopic or open appendicectomies (see Procedures).
After surgery: Antibiotics may be continued, particularly if the appendix is punctured or gangrenous.
Appendiceal abscess: Drainage can be done intraoperatively (with appendicectomy if safe) or percutaneously (with ultrasound or CT guidance, for example). In the event of a clinical deterioration, management of an appendiceal mass may involve periodic reassessment, parenteral fluids, antibiotics, and non-operative treatment. Weeks after the initial procedure, an interval appendicectomy may be done (Ochsner–Sherren method). If an adult does not undergo this, a barium enema or colonoscopy ought to be carried out in order to rule out a right colon malignancy.
Complications
Appendix abscess, perforation, peritonitis, inflammatory mass, and infrequently, portal pyaemia.
Following surgery, there may be an appendix stump faecal fistula, an abscess, an ileus, and wound infection.
Prognosis
An appendixectomy can be cured. It may be fatal if left untreated. The extremely young, the elderly, and pregnant women have greater rates of morbidity and mortality, making diagnosis more challenging in these situations.
0 Comments
