- Published on
Surgery - Bladder Cancer
Introduction
Urinary bladder epithelial cancer.
The majority are bladder epithelium-changing transitional cell carcinomas.
Others include adenocarcinomas that originate in the urachal remnant or squamous cell carcinomas linked to long-term inflammation (such as inschistosomiasis). Less common are leiomyosarcomas, carcinosarcomas, and small cell carcinomas (neuroendocrine).
Etiology
A number of genetic anomalies are linked to superficial tumors, such as chromosome 9 mutations in p15 and p16. Mutations in p53, p21, ras, c-myc, and c-jun are among the others.
Risk Factors
Smoking, exposure to benzidine and naphthylamines in the rubber, leather, and dye industries, treatment with cyclophosphamide (10% risk after 12 years of exposure), pelvic irradiation (for example, cervical cancer), persistent urinary tract infections, and schistosomiasis—early menopause has been demonstrated to raise risk by 50%. Adenocarcinoma is linked to patent urachus.
Epidemiology
2% of malignancies, the second most prevalent genitourinary system cancer; men are affected 2-3 times more frequently than women; rare <50 years; mean age at diagnosis in the sixties.
History
most frequently, macroscopic haematuria without discomfort. Urgency or nocturia, frequent urination, and recurrent UTIs are other symptoms. Pain from ureteral blockage, clot retention, or pelvic extension is infrequent.
Examination
Not many signs.
Palpable lymphadenopathy or bulk may indicate an advanced stage.
Investigational studies
Urine: Microscopy and culture in cytology.
Cystoscopy: Enables the tumor to be seen and removed or biopsied.
As tumors might have several locations, USS and IVU are used to evaluate the upper and lower urinary tracts.
MRI or CT scan: To stage.
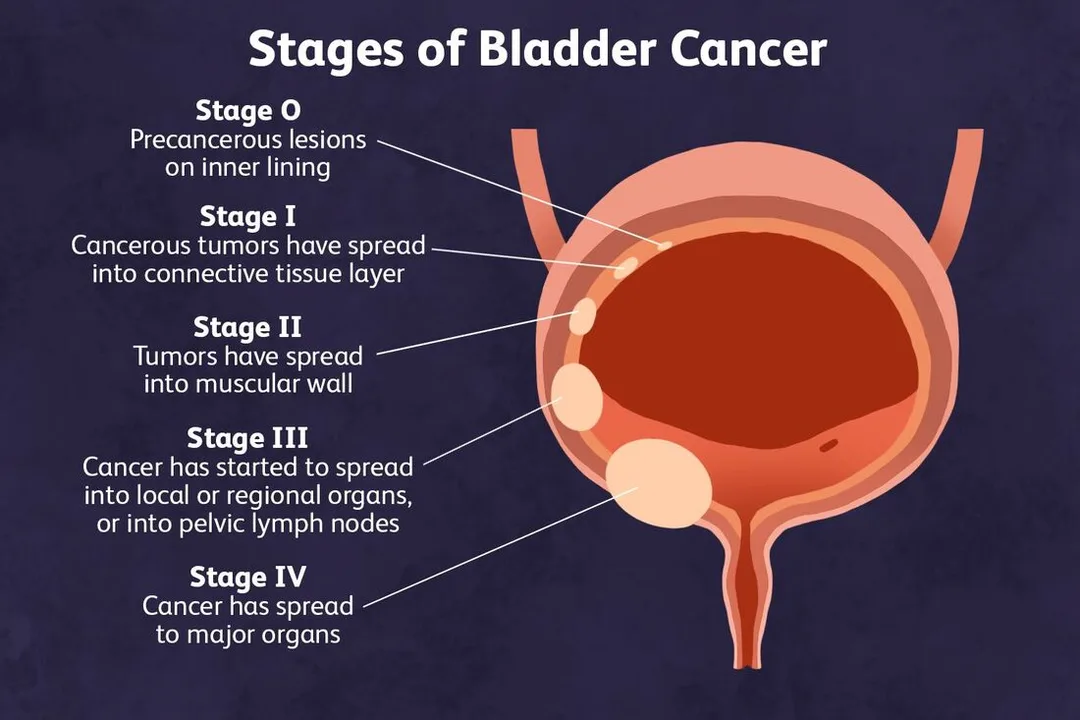
TNM setting: That is, in situ flat cancer; T1, submucosal invasion of lamina propria; T2, muscle invasion; T3, perivesical tissue invasion; T4, invasion of neighboring organs or pelvic wall; N, nodal involvement; and M, metastases. T1a is a papillary tumor above the lamina propria.
70% are only superficial when they are first diagnosed.
G1, well-differentiated; G2, moderately-differentiated; and G3, poorly-differentiated are the three classifications.
Management
Depending on the tumor's grade and stage.
Tumors on the surface (Tis, T1): Bladder tumor transurethral resection (TURBT).
To lower recurrence rates, provide BCG injections as part of intravesical immunotherapy or mitomycin C-based intravenous chemotherapy. close monitoring using recurrent cystoscopy and bladder cytology every three months for two years, then every six months for another two years, and finally once a year. The optimum treatment for high grade T1 tumors might be a cystectomy. Nephro-ureterectomy may be necessary due to upper tract illness.
T2 and higher invasive tumors: radical cystectomy if localized (this involves bilateral salpingo-oopherectomy and hysterectomy in females, and cystoprostatectomy in males with ileal conduit urine diversion, orthoptic reconstruction, and pelvic lymph node dissection).
Robotic-assisted or laparoscopic surgeries can be performed by specialised centres.
Chemotherapy or radiation therapy: If surgery is not an option, radical radiation therapy with salvage cystectomy is an alternative for post-radiation relapse. In cases of metastatic disease, palliative radiotherapy and chemotherapy are utilized, such as M-VAC (methotrexate, vinblastine, doxorubicin, and cisplatin).
Complications
hydronephrosis brought on by blockage of the ureteric orifice, haematuria, and clot retention.
Surgery: Early: rectal damage, ileus, intestinal blockage, infection, and bleeding.
Late: fistula, hernia, nephrolithiasis, pyelonephritis, and bowel obstruction.
Radiation therapy: hemorrhage, bladder contraction, and post-radiation cystitis.
Prognosis
Of those who undergo TURBT, 75% will develop further tumors, although only 10% will advance to an invasive illness. T1 90–100%, T2 70–70%, T3 30–65%, and T4 10–20% five-year survival rates. 5 year survival with distant metastases is 6%.
Introduction
Urinary bladder epithelial cancer.
The majority are bladder epithelium-changing transitional cell carcinomas.
Others include adenocarcinomas that originate in the urachal remnant or squamous cell carcinomas linked to long-term inflammation (such as inschistosomiasis). Less common are leiomyosarcomas, carcinosarcomas, and small cell carcinomas (neuroendocrine).
Etiology
A number of genetic anomalies are linked to superficial tumors, such as chromosome 9 mutations in p15 and p16. Mutations in p53, p21, ras, c-myc, and c-jun are among the others.
Risk Factors
Smoking, exposure to benzidine and naphthylamines in the rubber, leather, and dye industries, treatment with cyclophosphamide (10% risk after 12 years of exposure), pelvic irradiation (for example, cervical cancer), persistent urinary tract infections, and schistosomiasis—early menopause has been demonstrated to raise risk by 50%. Adenocarcinoma is linked to patent urachus.
Epidemiology
2% of malignancies, the second most prevalent genitourinary system cancer; men are affected 2-3 times more frequently than women; rare <50 years; mean age at diagnosis in the sixties.
History
most frequently, macroscopic haematuria without discomfort. Urgency or nocturia, frequent urination, and recurrent UTIs are other symptoms. Pain from ureteral blockage, clot retention, or pelvic extension is infrequent.
Examination
Not many signs.
Palpable lymphadenopathy or bulk may indicate an advanced stage.
Investigational studies
Urine: Microscopy and culture in cytology.
Cystoscopy: Enables the tumor to be seen and removed or biopsied.
As tumors might have several locations, USS and IVU are used to evaluate the upper and lower urinary tracts.
MRI or CT scan: To stage.
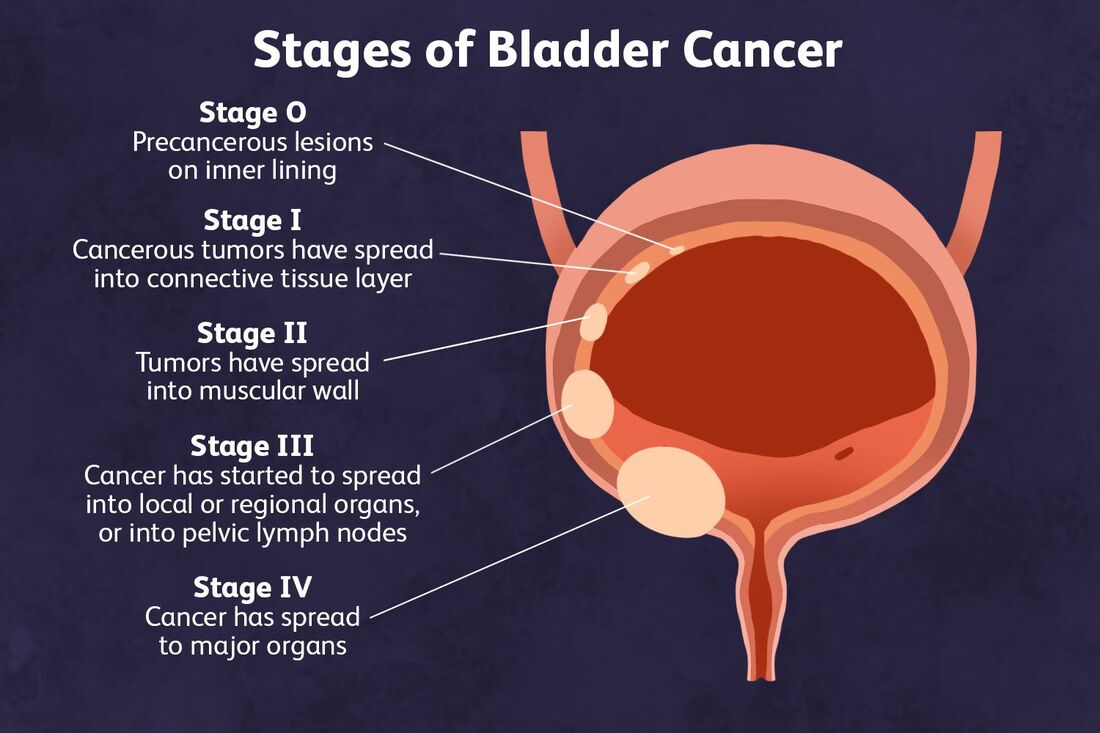
TNM setting: That is, in situ flat cancer; T1, submucosal invasion of lamina propria; T2, muscle invasion; T3, perivesical tissue invasion; T4, invasion of neighboring organs or pelvic wall; N, nodal involvement; and M, metastases. T1a is a papillary tumor above the lamina propria.
70% are only superficial when they are first diagnosed.
G1, well-differentiated; G2, moderately-differentiated; and G3, poorly-differentiated are the three classifications.
Management
Depending on the tumor's grade and stage.
Tumors on the surface (Tis, T1): Bladder tumor transurethral resection (TURBT).
To lower recurrence rates, provide BCG injections as part of intravesical immunotherapy or mitomycin C-based intravenous chemotherapy. close monitoring using recurrent cystoscopy and bladder cytology every three months for two years, then every six months for another two years, and finally once a year. The optimum treatment for high grade T1 tumors might be a cystectomy. Nephro-ureterectomy may be necessary due to upper tract illness.
T2 and higher invasive tumors: radical cystectomy if localized (this involves bilateral salpingo-oopherectomy and hysterectomy in females, and cystoprostatectomy in males with ileal conduit urine diversion, orthoptic reconstruction, and pelvic lymph node dissection).
Robotic-assisted or laparoscopic surgeries can be performed by specialised centres.
Chemotherapy or radiation therapy: If surgery is not an option, radical radiation therapy with salvage cystectomy is an alternative for post-radiation relapse. In cases of metastatic disease, palliative radiotherapy and chemotherapy are utilized, such as M-VAC (methotrexate, vinblastine, doxorubicin, and cisplatin).
Complications
hydronephrosis brought on by blockage of the ureteric orifice, haematuria, and clot retention.
Surgery: Early: rectal damage, ileus, intestinal blockage, infection, and bleeding.
Late: fistula, hernia, nephrolithiasis, pyelonephritis, and bowel obstruction.
Radiation therapy: hemorrhage, bladder contraction, and post-radiation cystitis.
Prognosis
Of those who undergo TURBT, 75% will develop further tumors, although only 10% will advance to an invasive illness. T1 90–100%, T2 70–70%, T3 30–65%, and T4 10–20% five-year survival rates. 5 year survival with distant metastases is 6%.
0 Comments
