- Published on
Surgery - Chronic Lower Limb Ischemia
Introduction
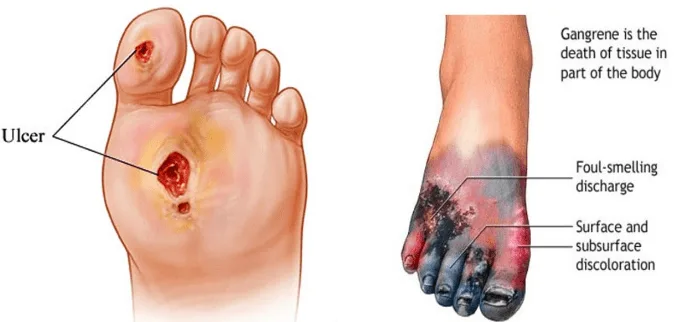
Chronic vascular insufficiency of the lower extremities can cause ulcers or gangrene, as well as pain during exercise known as intermittent claudication.
Etiology
Atherosclerosis in the leg arteries (femoral, iliac, and lower aorta).
Risk Factors
Diabetes, high blood pressure, smoking, high cholesterol, and family history.
Epidemiology
Common, occurrence 7–15% of senior citizens; male to female ratio is 2:1. In the UK, the yearly incidence of critical limb ischaemia is 50–100/100,000.
History
La Fontaine's severity classification system:
I. Lack of symptoms.
II. Claudication that is intermittent. Calf cramps that occur during exercise after a continuous distance (claudication distance) and go away a few minutes after the exercise is stopped.
III. Pain while rest. severe aching pain in the foot or lower limb that usually goes away at night when the leg is draped over the edge of the bed.
IV. Gangrene or ulceration of the leg.
Critical ischaemia: Severe arterial insufficiency endangering the limb's survival when there is rest pain lasting more than two weeks, ulceration, or gangrene.
The Leriche syndrome: when lower aortoiliac blockage causes impotence and claudication in the buttocks and thighs.
Examination
Check for evidence of hyperlipidemia, abdominal aortic aneurysm, carotid bruits, and signs of ischemic heart disease in the cardiovascular system.
Severe lower limb ischaemia is characterized by shining atrophic skin, atrophic nails, hair loss, and painful, punched-out ulcers (under toes, for example, or traditionally over the lateral malleolus). With weak or nonexistent pulses and a protracted capillary return time, the peripheries are chilly to the touch.
Keep an ear out for bruits.
Buerger's examination: Pallor and venous guttering are the first signs of elevation of the leg, and dependent rubor follows.
The index of ankle-brachial pressure (ABPI): calculated by dividing the brachial pressure by the systolic ankle pressure, using a portable Doppler device. 0.8–0.6 for claudication; normal >0.9.
<0.5 or ankle systolic <50mmHg or toe systolic <30mmHg is considered critical ischaemia (numbers may be erroneously high in diabetics due to weakly compressible arteries).
Investigations
Imaging: CT, MR, or arterial duplex angiography. Those receiving intervention can use digital subtraction angiography.
Bloods: FBC, lipids, glucose, coagulation, and preintervention group and save.
Management
Medical: It has been demonstrated that supervised programs are beneficial; quit smoking and promote exercise. Treatment of other cardiovascular risk factors, such as aspirin, statins, and antihypertensives (avoid b-blockers). Patients with serious ischemia who are not responding to previous treatments may occasionally receive prostacyclin infusions.
Endovascular surgery includes arterial stenoses stenting and/or balloon angioplasty.
Surgical: For severe ischaemia or intermittent claudication that is incapacitating.
Revascularization: The technique varies according on the occlusion site.
Aortoiliac occlusive disease: unilateral iliac disease (femoro-femoral or ilio-femoral bypass), aorto-bifemoral bypass, or occasionally axillo-bifemoral bypass.
The term "femoropopliteal disease" refers to conditions involving the grafting of autogenous tissue, such as saphenous vein (either reversed or in situ with valves damaged with a valvulotome), or synthetic tissue, such as PTFE, for bypass purposes. In the case of the latter, longer-term patency rates are considerably increased by a vein patch (Millar cuff) at the distal anastomosis.
observation of the graft with duplex scanning after surgery.
In cases of end-stage atherosclerotic disease, amputation is recommended if revascularization is not feasible, there is a substantial amount of necrosis, or sepsis is spreading. Revascularization may make it possible to amputate below the knee as opposed to above; the former is linked to improved mobility and the usage of prosthetic limbs after surgery.
Complications
If wet, there is a danger of systemic sepsis, multiorgan failure, pain, ulceration, and gangrene.
3–4% risk with angioplasty, including thrombosis, embolism, dissection, flap, and failure.
From bypass grafting: . Early: Edema, infection, lymphocoele, hemorrhage, cardiac events, and graft thrombosis. Late: Graft stenosis, anastomotic false aneurysm, and thrombosis. Overall, patency rates above the knee (70–80% at 3 years) are higher than those below.
Prognosis
Patients with lower limb ischaemia have an elevated risk of MI and stroke because it is a sign of atherosclerosis throughout the arterial tree. About 40% of people with intermittent claudication get better, 40% stay stable, and 20% worsen over the course of five years and need medical attention.
Introduction
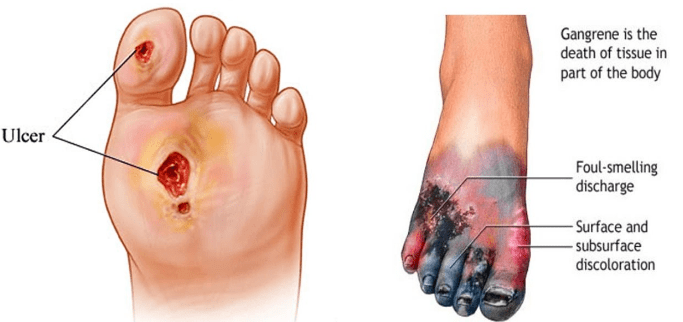
Chronic vascular insufficiency of the lower extremities can cause ulcers or gangrene, as well as pain during exercise known as intermittent claudication.
Etiology
Atherosclerosis in the leg arteries (femoral, iliac, and lower aorta).
Risk Factors
Diabetes, high blood pressure, smoking, high cholesterol, and family history.
Epidemiology
Common, occurrence 7–15% of senior citizens; male to female ratio is 2:1. In the UK, the yearly incidence of critical limb ischaemia is 50–100/100,000.
History
La Fontaine's severity classification system:
I. Lack of symptoms.
II. Claudication that is intermittent. Calf cramps that occur during exercise after a continuous distance (claudication distance) and go away a few minutes after the exercise is stopped.
III. Pain while rest. severe aching pain in the foot or lower limb that usually goes away at night when the leg is draped over the edge of the bed.
IV. Gangrene or ulceration of the leg.
Critical ischaemia: Severe arterial insufficiency endangering the limb's survival when there is rest pain lasting more than two weeks, ulceration, or gangrene.
The Leriche syndrome: when lower aortoiliac blockage causes impotence and claudication in the buttocks and thighs.
Examination
Check for evidence of hyperlipidemia, abdominal aortic aneurysm, carotid bruits, and signs of ischemic heart disease in the cardiovascular system.
Severe lower limb ischaemia is characterized by shining atrophic skin, atrophic nails, hair loss, and painful, punched-out ulcers (under toes, for example, or traditionally over the lateral malleolus). With weak or nonexistent pulses and a protracted capillary return time, the peripheries are chilly to the touch.
Keep an ear out for bruits.
Buerger's examination: Pallor and venous guttering are the first signs of elevation of the leg, and dependent rubor follows.
The index of ankle-brachial pressure (ABPI): calculated by dividing the brachial pressure by the systolic ankle pressure, using a portable Doppler device. 0.8–0.6 for claudication; normal >0.9.
<0.5 or ankle systolic <50mmHg or toe systolic <30mmHg is considered critical ischaemia (numbers may be erroneously high in diabetics due to weakly compressible arteries).
Investigations
Imaging: CT, MR, or arterial duplex angiography. Those receiving intervention can use digital subtraction angiography.
Bloods: FBC, lipids, glucose, coagulation, and preintervention group and save.
Management
Medical: It has been demonstrated that supervised programs are beneficial; quit smoking and promote exercise. Treatment of other cardiovascular risk factors, such as aspirin, statins, and antihypertensives (avoid b-blockers). Patients with serious ischemia who are not responding to previous treatments may occasionally receive prostacyclin infusions.
Endovascular surgery includes arterial stenoses stenting and/or balloon angioplasty.
Surgical: For severe ischaemia or intermittent claudication that is incapacitating.
Revascularization: The technique varies according on the occlusion site.
Aortoiliac occlusive disease: unilateral iliac disease (femoro-femoral or ilio-femoral bypass), aorto-bifemoral bypass, or occasionally axillo-bifemoral bypass.
The term "femoropopliteal disease" refers to conditions involving the grafting of autogenous tissue, such as saphenous vein (either reversed or in situ with valves damaged with a valvulotome), or synthetic tissue, such as PTFE, for bypass purposes. In the case of the latter, longer-term patency rates are considerably increased by a vein patch (Millar cuff) at the distal anastomosis.
observation of the graft with duplex scanning after surgery.
In cases of end-stage atherosclerotic disease, amputation is recommended if revascularization is not feasible, there is a substantial amount of necrosis, or sepsis is spreading. Revascularization may make it possible to amputate below the knee as opposed to above; the former is linked to improved mobility and the usage of prosthetic limbs after surgery.
Complications
If wet, there is a danger of systemic sepsis, multiorgan failure, pain, ulceration, and gangrene.
3–4% risk with angioplasty, including thrombosis, embolism, dissection, flap, and failure.
From bypass grafting: . Early: Edema, infection, lymphocoele, hemorrhage, cardiac events, and graft thrombosis. Late: Graft stenosis, anastomotic false aneurysm, and thrombosis. Overall, patency rates above the knee (70–80% at 3 years) are higher than those below.
Prognosis
Patients with lower limb ischaemia have an elevated risk of MI and stroke because it is a sign of atherosclerosis throughout the arterial tree. About 40% of people with intermittent claudication get better, 40% stay stable, and 20% worsen over the course of five years and need medical attention.
0 Comments
